
Abstract
Dementia is the second leading cause of disease burden in Australia, with regional populations facing limited access to multidisciplinary assessment, leading to delays and poorer outcomes. A hybrid virtual memory clinic (hVMC) combining in-person and virtual assessments is a possible solution. This study aimed to co-design a hVMC model for trialling in regional areas. This cross-sectional qualitative study included four co-design workshops (n = 56) and four interviews with people living with dementia, care partners, clinicians, and administrators. A hVMC model was iteratively developed and refined. Thematic analysis was conducted. The first theme, “we need the right service, right time,” describes regional challenges such as delays in assessment, limited specialist availability, and gaps in post-diagnostic support. The second theme, “the virtual memory clinic must be integrated with existing services,” highlights the need for a person-centred hybrid model involving in-person visits and collaboration with local providers, fostering relationships and reciprocal capacity building. The third theme, “clarity needed on who virtual assessment would suit,” reflects mixed views on eligibility, with general agreement on a cognitive threshold (e.g., Mini-Mental State Examination >20) but uncertainty around its application, suggesting a need for flexibility. Co-design participants also proposed practical features — shared intake, regular in-person assessments, post-diagnostic interventions (e.g., occupational therapy, cognitive programs), and local capacity building — which were iteratively integrated into the model. We present a co-designed hVMC model incorporating key features to support feasibility, access, and continuity of care. The model includes shared intake, quarterly in-person face-to-face assessments, structured post-diagnostic support, and collaboration with local services to build capacity. This model will be tailored to each region and is currently being piloted. Co-designed models must balance stakeholder priorities with implementation feasibility.
Introduction
The world’s population is ageing, the number of people living with dementia is increasing, and the demand for dementia-related services continues to grow. In Australia, dementia’s disease burden – a measure that captures both the impact of living with illness (years lived with disability) and premature death (years of life lost) – has risen from the 12th leading cause of total disease burden in 2003 to the leading cause in 2024 (Australian Institute of Health and Welfare, 2024). Current clinical guidelines recommend that dementia be diagnosed by a specialist (Laver et al., 2016), with multidisciplinary memory clinics representing the gold standard model for assessment and diagnosis (Naismith et al., 2022). In addition, people living with mild cognitive impairment, or dementia should be supported to access interventions and services to slow progression, maintain function, and preserve quality of life (Laver et al., 2016). Despite these recommendations, access to specialist memory clinics and post-diagnostic support remains inequitable in Australia, particularly for people living in rural and regional areas. Virtual dementia services offer a promising approach to bridging these gaps by supporting both diagnostic assessment and post-diagnostic care. The development and co-design of such a model is the focus of this paper.
Although 34% of older Australians live in rural and regional areas, fewer than 10% of memory clinic services are located there (Naismith et al., 2022). Limited specialist availability and workforce shortages further exacerbate access issues (Cortie et al., 2024). In the absence of specialist services, primary care physicians often provide the first point of contact for dementia assessment and coordinate ongoing management; however, limited consultation time, dementia-specific training, and multidisciplinary support constrain their capacity to do so effectively. Further, within Australia’s publicly funded healthcare system (Medicare), there are few financial incentives for primary care physicians to undertake dementia assessment (Dixit & Sambasivan, 2018). Key assessment services, such as neuropsychology, are not covered by Medicare, and rising out-of-pocket costs disproportionately affect people living outside metropolitan areas (Angeles et al., 2023). Fragmentation between federal and state funding structures further contributes to disjointed dementia care services (Low et al., 2021), and there is currently no dedicated or consistent funding model for memory clinics (Naismith et al., 2023). Our recent Delphi process to develop Australian Memory and Cognition Clinic Guidelines (https://www.australiandementianetwork.org.au/) highlighted the distinction between “ideal” and “feasible” services, identifying limited resources, staff training, and confidence as key barriers to delivering optimal care (Bundy et al., 2022).
These structural and financial limitations contribute to significant inequities in care. People living in regional and rural areas experience longer wait times – only 20% of public regional clinics can provide non-urgent assessments within two months, compared with 40% of metropolitan clinics (Naismith et al., 2022) – and are less likely to be diagnosed with dementia or receive high-quality dementia care (Arsenault-Lapierre et al., 2023; Rahman et al., 2021; Xu et al., 2022; Zilkens et al., 2014). Access to timely post-diagnostic support is limited, including non-skilled in-home services and carer support programs, which are inconsistently provided across regional areas (Garrett et al., 2024). Further, post-diagnostic care is typically limited to provision of information, referrals to other services, or medications for Alzheimer’s disease (Naismith et al., 2022; Pavković et al., 2024). Evidence-based cognitive interventions are rarely offered despite guideline recommendations (Pike et al., 2024; Woodward et al., 2022).
Given these systematic and geographical barriers, virtual dementia services offer a promising approach to improve access, support both diagnosis and post-diagnostic care, and build capacity in regional and rural areas. Videoconference-based dementia assessments have good diagnostic reliability compared to face-to-face assessments (Watt et al., 2021). There has also been ongoing development and validation of neuropsychological tests for reliable online administration (Owens et al., 2020). In the state of New South Wales, Australia, a virtual hospital model has been implemented to expand outreach services, including dementia care, to residential aged care facilities and remote communities. This model underscores the feasibility of delivering multidisciplinary dementia support via telehealth when integrated with appropriate local services and infrastructure (Sydney Local Health District, 2020).
However, there are challenges to virtual dementia assessment. Known barriers to virtual healthcare include the need to accommodate cognitive, sensory, and physical impairments; ensure appropriate physical environments, stable staffing, and reliable technology; and address low motivation and awareness among providers and low digital literacy among users (Savira et al., 2023). Additional barriers to dementia assessment via videoconference include limited technological access, literacy and confidence; challenges in building rapport and therapeutic alliance; needing to maintain patient privacy and confidentiality; and ensuring security of information. While prior studies have demonstrated generally good diagnostic accuracy for virtual cognitive assessments, concerns remain regarding the standardisation of assessment environments, applicability of normative data for some paper-based tests administered online, and limitations of teleneurological examination in certain clinical scenarios (Blane et al., 2021; Germine et al., 2019; Gosse et al., 2021).
A hybrid virtual memory clinic (hVMC) model – combining in-person and virtual assessments – may minimise some of the challenges with telehealth. International examples have demonstrated that hybrid models can improve access, provide support with technology, enhance privacy, and strengthen relationships between patients, their care partners, and clinicians (Bundy et al., 2022; Liu et al., 2022). Ideally, such a service would encompass good knowledge and working relationships with local services and may need to work with local services to build capacity.
It has been stressed that health systems should be co-designed to meet the needs of the person, rather than the needs of the system (Lachman et al., 2020). The Institute of Medicine framework for healthcare quality states that healthcare systems should be safe, effective, patient-centred, timely, efficient, and equitable (Institute of Medicine Committee on Quality of Health Care in America, 2001). Additionally, when developing a new healthcare model, it should be feasible (i.e., the model could be successfully delivered within a particular setting) (Karsh, 2004). This supports the notion that models of care need to be localised to the specific setting. To address these systemic and geographical barriers, innovative service models are needed to improve access to diagnostic and post-diagnostic dementia care in regional and rural areas.
This project aimed to co-design a hVMC model suitable for deployment across Australia. The current paper reports on the planning and co-design phase of the project, which will inform subsequent implementation in partnership with Australian local health districts and networks. This model will later be localised (i.e., adapted) and piloted in one regional site, prior to more widespread testing.
Methods
Design
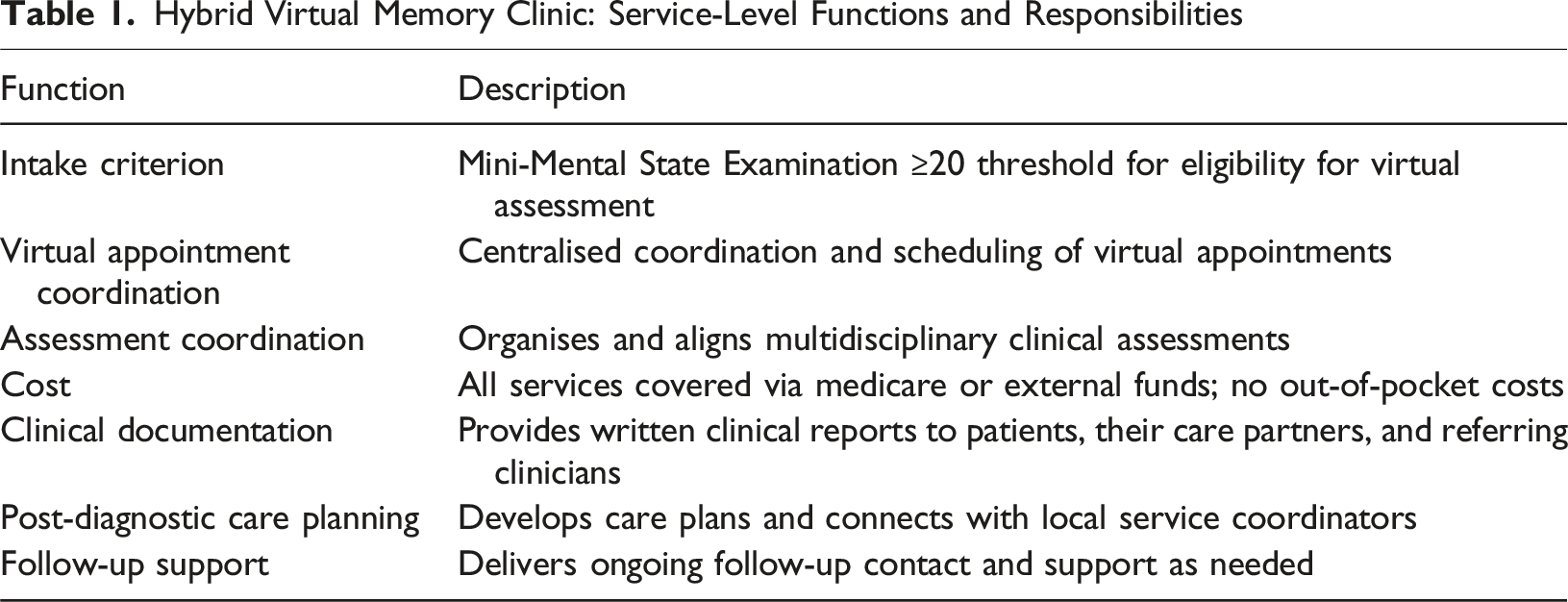
Hybrid Virtual Memory Clinic: Service-Level Functions and Responsibilities
Hybrid Virtual Memory Clinic (hVMC): Clinical Governance Structure and Team Roles
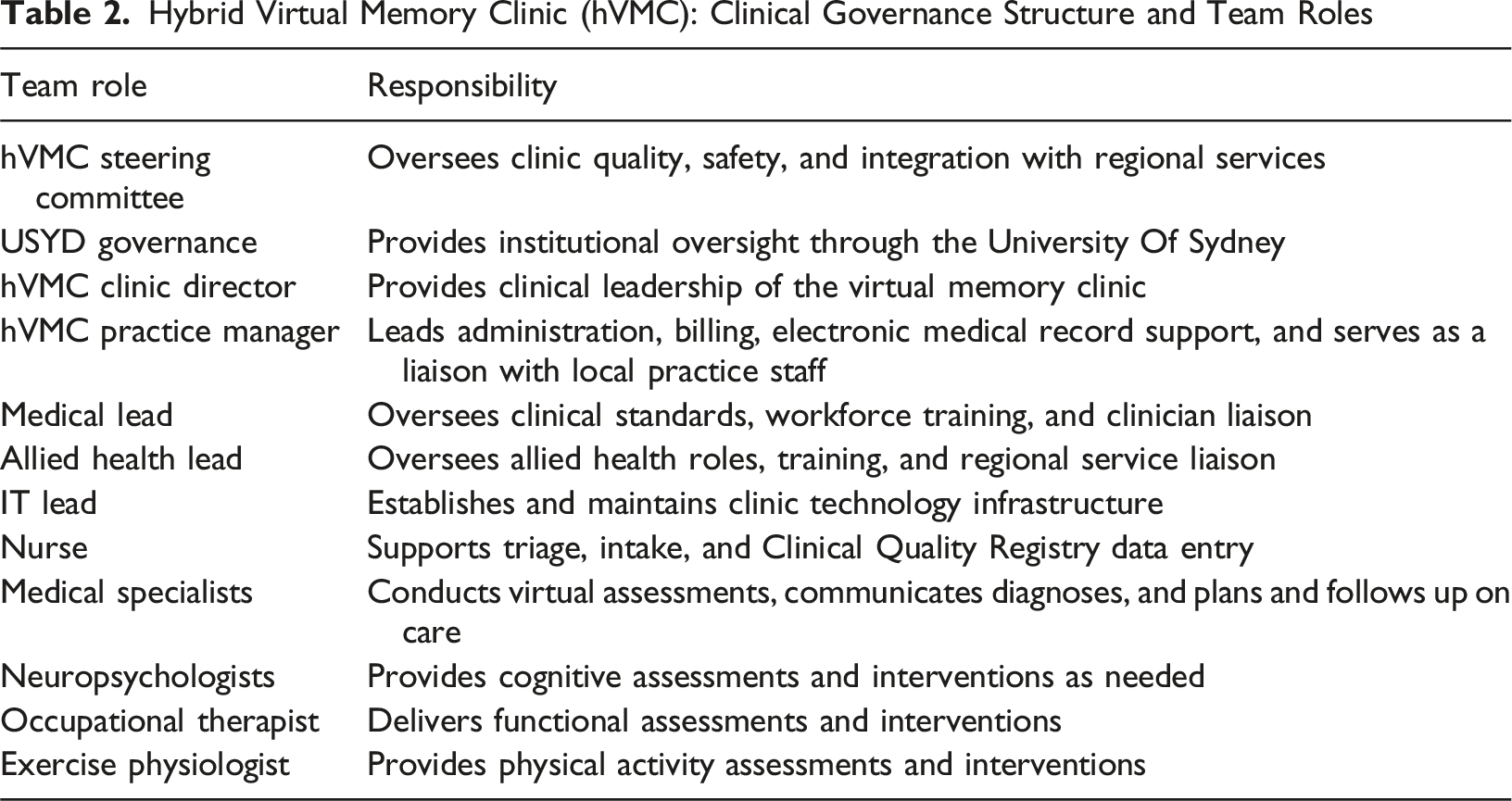
These components formed the basis for stakeholder discussions and were iteratively refined throughout the co-design workshops and interviews.
Ethics
Ethical approval was obtained from the University of Sydney Human Research Ethics Committee (HREC 2023/566). Written informed consent was obtained from all co-design participants.
Sample
Co-design participants were recruited by personal invitation, through the professional networks of the research team and by snowballing through the networks of the professionals and advocates.
Inclusion criteria - People living with dementia and their care partners who had experience with, or interest in, memory clinics and/or regional health services. - Health and aged care administrators, clinicians, and policy or system-level stakeholders (e.g., health planners, representatives from health agencies) with experience in memory clinics and/or regional or virtual assessments.
Data Collection
Workshops and interviews were conducted between 21 September and 6 December 2023. Three were conducted online and one was conducted in person. To facilitate the meaningful participation and inclusion of people living with dementia and their care partners, clear slides were prepared, speaking order prioritised contributions from people living with dementia, followed by care partners, and one team member was designated as their specific contact and support person during workshops. Co-design participants were asked a selection of the following questions depending on their expertise: 1. What needs to be changed about the model to achieve its aims? 2. Who would be suitable to use the virtual service? 3. How could the clinic responsibilities be shared between the local and virtual clinic service organisations and members? 4. How can the clinical governance and roles and responsibilities be improved? 5. What is the referral pathway in, and discharge pathway out of the service? 6. What is the need and feasibility of virtual occupational therapy and cognitive rehabilitation programs? 7. What local capacity building is required to support post-diagnostic services as part of care planning? 8. What are the technological considerations in delivering this model? 9. What are the perceived barriers or challenges around implementing the virtual clinic?
Workshops and interviews were audio recorded and transcribed. Zoom chat and field notes taken during workshops, interviews, and meetings were also used as data.
Analysis
Thematic analysis (Braun & Clarke, 2022) was undertaken to identify the desirable features of a virtual clinic model, and perceived concerns around the structure of these qualities in a virtual memory clinic model. We identified any healthcare system values (i.e., safe, effective, patient-centred, timely, efficient, and equitable) (Institute of Medicine Committee on Quality of Health Care in America, 2001) or feasibility issues, raised as part of these discussions. Two researchers (LV, TWB) independently identified codes using NVIVO software (Version 14) and then derived themes from those codes, in discussion with a third researcher (LFL).
The research team comprised a multidisciplinary group of clinician academics with backgrounds in psychology, neuropsychology, health services, public health, geriatrics, old age psychiatry, nursing, occupational therapy, and speech pathology. Team members have a range of experience in dementia research from a few months to decades. Members of the research team also ran memory clinics and have experience in working in regional areas and in conducting virtual assessments. We took a reflexive approach to developing this model, in which the co-design participants and different research team members challenged some of our initial assumptions and broadened our thinking. This process involved post-workshop debriefing sessions, where we worked on reorganising the information and iterating on the model for the next workshop.
Findings
Sample Description
The workshops involved a diverse group of attendees, including medical professionals, allied health professionals, people with lived experience of dementia, health services management personnel, and representatives from the aged care sector.
Workshop Co-Design Participants
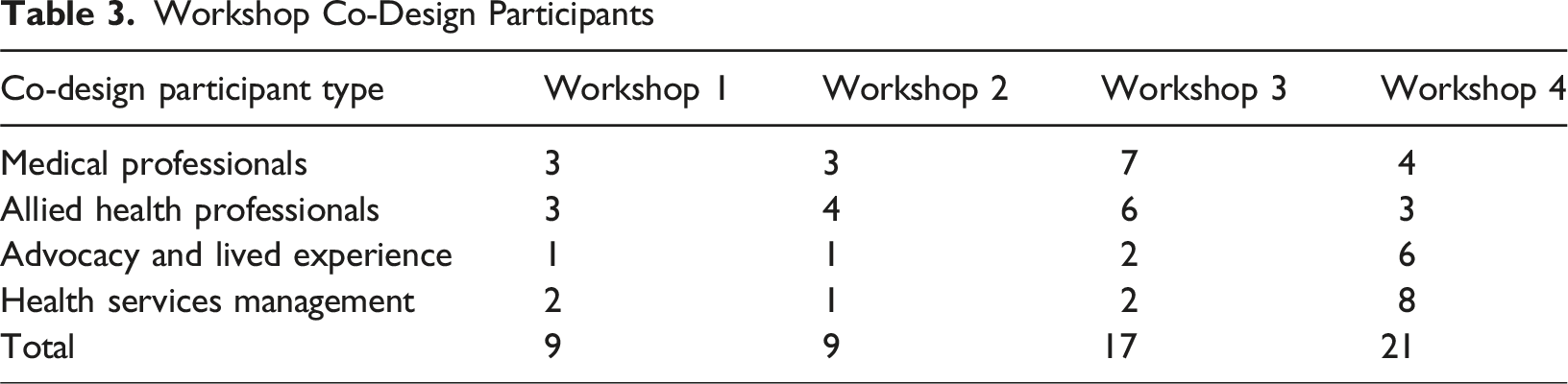
A total of four supplementary interviews were conducted by the same researcher, who also participated in the workshops. One interview was held with a person living with dementia, and three interviews were conducted with clinicians.
Key Themes
Key Themes Identified From the Co-Design Process
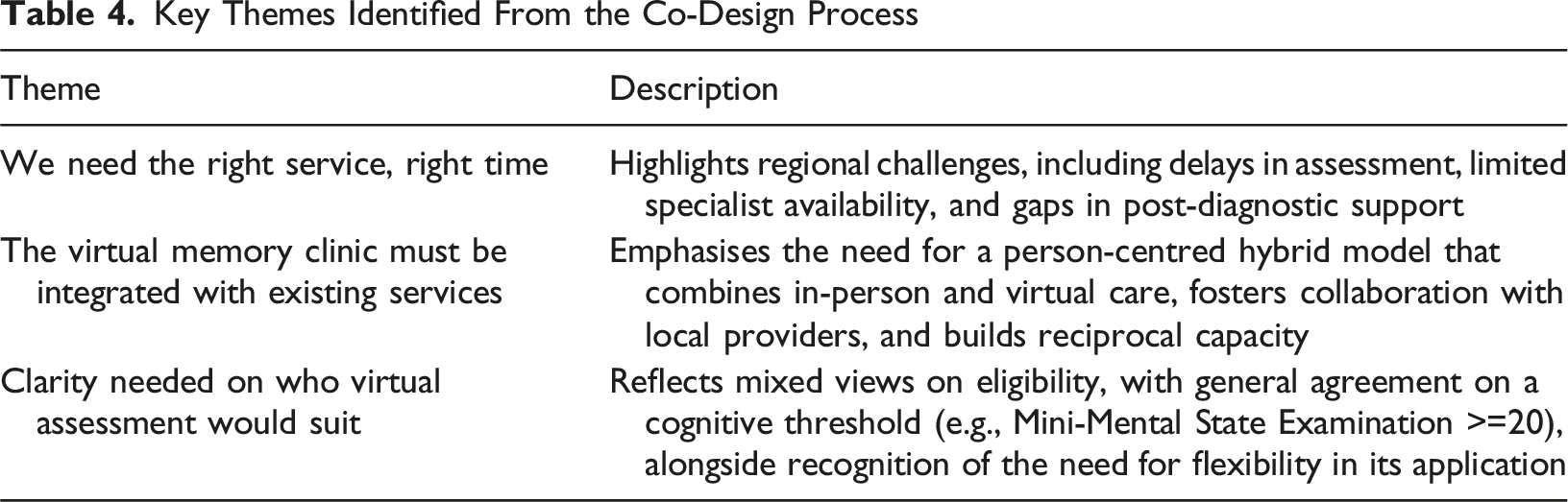
We Need the Right Service, Right Time
People living with dementia, their care partners, and clinicians all stressed the need for more dementia-related diagnostic services, and immediate, seamless post-diagnostic services. In regional areas, diagnosis was often protracted, with many co-design participants describing long journeys to diagnosis. This issue reflects both the limited access to appropriate services and the challenges posed by a fragmented system. Services or clinicians with specialised dementia expertise were not always well matched to the needs of people living with dementia. This theme reflects values raised by co-design participants that the service should be timely (minimise delay), effective (service has dementia expertise), and efficient (provided in an accessible and appropriate way).
Delays in provision of dementia assessments were raised as a shortcoming of the current health system. “Taking a year to get the full diagnosis is way too long” (care partner). Co-design participants shared experiences of lengthy waiting lists in some regional areas, and that timely assessment was needed.
They talked about the importance of the dementia diagnosis in facilitating management of dementia “I’ve got a friend down there who rings me every second day about what's happened with her brother … They had nothing, but there’s things in place now because they've been onto dementia care thank goodness” (care partner). “The regionally based CDAMS clinics in Victoria - Ballarat, Bendigo, Shepperton, Warrigal – all have long waiting lists post-COVID” (Geriatrician).
However, one clinician indicated that the wait time for regional assessment was not longer than in their own metropolitan clinic. Other clinicians commented that waiting lists were not a good indicator of the level of unmet need, as referrals might not continue to be made once referrers know there is a long waiting list. Clinicians and administrators were also concerned about the possible prevalence of undiagnosed mild cognitive impairment in the community, and that even with additional memory clinic services, the system would not be able to manage if people came forward for testing. If the new anti-amyloid therapies were available in Australia, they expressed concern that people seeking help for these drugs would lengthen waiting lists.
Co-design participants from regional areas discussed limited availability of clinicians with dementia expertise and of programs specifically for people living with dementia. “I’m also a member of a carers group which we set up here … And it’s still amazing 3 years after my wife died the stories about lack of services is still there” (care partner).
Clinicians and administrators talked about the low numbers of medical specialists (geriatricians and old age psychiatrists) working in regional services, as well as ongoing difficulty attracting specialists to the regions. Clinicians noted that people attending regional clinics often presented with diverse and complex needs (e.g., mild or inconsistent cognitive symptoms, psychiatric symptoms or complex physical co-morbidities) and these presentations required additional specialist assessment and treatment to ensure the right service at the right time.
Care partners and clinicians also noted insufficient public or private allied health services for people living with dementia, in particular, neuropsychologists and occupational therapists. “The local occupational therapist and speech pathologist rang me from the local hospital and said we’d love to be able to help you, but we don’t have the specialist expertise here” (care partner).
All stakeholders highlighted the need for seamless post-diagnostic supports as part of the virtual clinic model. People with dementia and care partners emphasised that they valued ongoing connection and follow-up after diagnosis, though this was not necessarily specifically a regional issue. People with dementia and their families expressed a desire for a case manager or navigator to work alongside them in navigating post-diagnostic support. “We went to see a geriatrician, and it was ‘You’ve got your diagnosis — go away and be happy’” (care partner). “You have that nurse practitioner role that guides people through post-cancer diagnosis. We don’t have that in dementia and I think it would be a really good thing if we did” (care partner).
Some clinicians also reported that their clinics faced constraints in providing comprehensive post-diagnostic follow-up services. “It’s a bit like ‘There’s your diagnoses off you go’. You know, that’s it. That’s what we can offer” (neurologist).
While there was general support for a virtual memory clinic model, some clinicians had reservations that it could be “done really badly, really superficially” and be a “second-rate” or “better than nothing” service. Regionally based clinicians expressed concern that directing funding and services into a virtual model may compound current regional inequities by decreasing the need for regionally based clinicians.
The Virtual Memory Clinic Must be Integrated With Existing Services
Clinicians and administrators felt strongly that the virtual memory clinic needed to be integrated with existing local in-person services. A hybrid virtual model would include an in-person location for videoconferencing and a local allied health professional to support the appointment. The model needed some flexibility in how it would integrate the virtual service with existing regional dementia diagnostic services and needed to include reciprocal capacity building and leverage existing relationships held by the regional service. The values of person-centredness (flexible depending on what the person’s needs), safety (emphasising the importance of an in-person clinician) and efficiency (minimising duplication of intake, using the same medical records) are reflected in this theme.
Co-design participants thought that, to operate effectively and efficiently, the assessment service had to be a hybrid virtual model. That is, it should have a physical site and face-to-face support person, or clinician as well as the virtual memory clinic team. This physical location requires a private space with a computer (a larger screen is preferable) and internet access for co-design participants who did not have these technologies at home. The local allied health professional support people by conducting ‘hands-on’ physical examinations and cognitive screens, coordinating assessments, and obtaining additional information from referrers (e.g., blood tests, brain scans). They would also need to enter information into the electronic medical record before the virtual assessments so that it is available for the virtual clinicians and be physically present to provide emotional support when a diagnosis is given.
People living with dementia and their care partners stressed the importance of having this in-person support with technology: “Having a human on the other end of that can facilitate getting that up and running” (care partner).
Administrators and clinicians emphasised the need for integration of the virtual clinic with pre-existing regional services, with the virtual clinic supplementing existing services, both face-to-face and other virtual services run by sole specialists. There were initial concerns that the virtual clinic might duplicate existing services or create confusion for referrers and patients, but these concerns were allayed as the model was iteratively refined throughout the co-design process to be more integrated. Patients would come under the care of the regional service, with the virtual team credentialed as visiting medical officers or allied health staff. “You may want to set up a virtual clinic that runs in parallel with [Clinician’s name] clinic because she’s doing the further end of the spectrum. And you start a virtual clinic at the earlier end of the spectrum … [an] improvement to the service, rather than trying to fit on the clinic that already exists and is overburdened into a structure that it’s not designed for” (clinician).
Because the virtual clinic was collaborating with and supplementing existing services, it was very important that there was flexibility in the model from the perspective of administrators and clinicians. This was to avoid duplication and increase efficiency (e.g., not having multiple intake processes). For instance, co-design participants from some potential sites were interested in combining existing in-person or geriatric services with virtual neuropsychology, consultant aged care psychiatry, and post-diagnostic services. That is, the virtual team could bring complementary skills that local services did not have and did not need to duplicate services already exist within the regional/rural area. For example, some local services expressed interest in additional training in cognitive rehabilitation, which the virtual team could offer to better support families: “The local services aren’t trained in cognitive rehabilitation, so they won’t necessarily be able to take that approach with families, to really provide them with the insights that are required” (clinician).
This offers a highly bespoke but flexible model, in partnership with local service needs.
The hybrid virtual clinic could leverage existing relationships that the regional service had with local referring doctors and other services. This would help ensure that the clinic receives timely and appropriate referrals. Local partnerships were also critical to maintain continuity of care after diagnosis as the regional clinics often provided diagnostic assessments and referred people to their GPs for ongoing care. The virtual clinic would need an aligned discharge process. Local clinics also had relationships with aged care and other services which might be used by people with dementia.
Clinicians and administrators said it was critical that reciprocal capacity building occurred between virtual clinic and regional clinic staff, with regional staff sharing local knowledge and relationships, and the virtual team bringing additional dementia expertise: “I think it’s a [two]-way street” (clinician). There were many suggestions regarding ways that the virtual clinic could support or upskill the dementia workforce – including running formal training sessions particularly for GPs, nurses, and allied health; weekly case conferences to discuss complex cases and; the development of a clinical peer support network. We incorporated formal training into the model; however, we decided that the other capacity-building components might be incorporated based on the context of the region in which it is being implemented. Where appropriate, training resources could be drawn from existing national programs such as Dementia Training Australia, a government-funded provider of dementia-specific education and training for the health and aged care workforce.
Diversity in electronic health platforms was identified by the project team as a challenge in delivering the model. Health services had separate, different electronic medical records systems and telehealth platforms.
Clarity Needed on Who Virtual Assessment Would Suit
There was general agreement that virtual assessment was not suitable or desirable for all people help-seeking for an assessment. There are people who “just don’t like technology”, and “don’t like the online platform, full stop”. Aside from agreeing that people with poor hearing should not be assessed virtually, there was no clear consensus on who should be selected for virtual assessment. In response to this, we proposed a preliminary threshold of Mini-Mental State Examination ≥20 for access to telehealth assessments, recognising that this may not be appropriate in all cases. Co-design participants agreed that case-by-case flexibility would be needed to accommodate individual needs. There was tension between values of non-maleficence (not increasing burden on patients or families), equity (not excluding people unnecessarily from virtual assessment), effectiveness (using virtual assessment only when this can be done well), and efficiency (using the virtual clinic’s expertise to assess more difficult-to-diagnose patients).
Our draft criteria excluded people with visual impairments from the virtual assessments – this generated different opinions. Some clinicians advocated that people with visual impairment could still be assessed virtually. A few co-design participants thought that virtual assessment may be more challenging for people who use interpreters, but also commented that this need would be lower in regional Australia. There was some discussion also about the typical use of informant/care partners during assessment for collateral history taking, and that this needed consideration, as some people do not have a care partner. However, this was not a specific issue for a virtual assessment. In fact, some co-design participants saw the virtual model as facilitating this. For example, a family member could join the assessment even if they were not based locally or in the ‘same place’ as the person with cognitive impairment for the assessment. Mental illness, drug, and alcohol use were discussed in deliberations about who would be suitable for the clinic. Ultimately, co-design participants agreed that many of these factors should be assessed collaboratively with local services, which are best placed to evaluate individual circumstances.
There were concerns that a service model that used a virtual clinic could have an unintended, increased burden for older people and their care partners/families. Regarding in-home virtual assessments, co-design participants raised concerns about accessibility to technology and the risk of burdening family to support the person with cognitive impairment accessing the technology. Somewhat contradictory, there were also some concerns about creating a service that required people to travel to a physical location to access the virtual service – e.g., to the local health centre with telehealth facilities, as this was essentially the same effort as attending an in-person assessment. Some co-design participants suggested offering links to local transport services could facilitate access to the local centre to attend the assessment, if required. A consensus was reached that on-site virtual assessments would be offered, with the possibility to trial at-home virtual assessments on a case-by-case basis.
Our draft model initially conceptualised the hVMC as focusing on assessments for people with milder cognitive symptoms, because this is the typical clientele seen by memory clinics, and we thought that this would be an efficient use of virtual team’s expertise. Some co-design participants agreed that virtual assessments were more suitable for people with milder impairments “I don’t think that we can assess people with more severe dementia well virtually” (clinician). However, other co-design participants thought that the clinic would provide a more equitable service if eligibility criteria were based on local needs (e.g., capacity of other assessment services in the region), and that there should be minimal criteria based on level of cognitive function. Again, the importance of the service being flexible was emphasised by both clinicians and people living with dementia and their care partners “You just need to be very sort of pragmatic – you do what you can, when you can, how you can” (geriatrician); “I think it’s about variety, so it covers all bases and [is] as simple and basic as possible” (care partner).
Final Hybrid Virtual Memory Clinic Model
The co-designed, hVMC features a shared intake/triage process across existing regional assessment services and a virtual specialist team (see Figure 1). The virtual team includes a nurse coordinator and specialists (primarily geriatrician with old age psychiatrist or neurologist when indicated) and supplementary neuropsychology or occupational therapy assessments as required. It includes quarterly face-to-face visits for individuals for whom a virtual service is not suitable or insufficient. These visits also help to build relationships and support collaboration between local health professionals and the virtual team. Final model of the hybrid virtual memory clinic*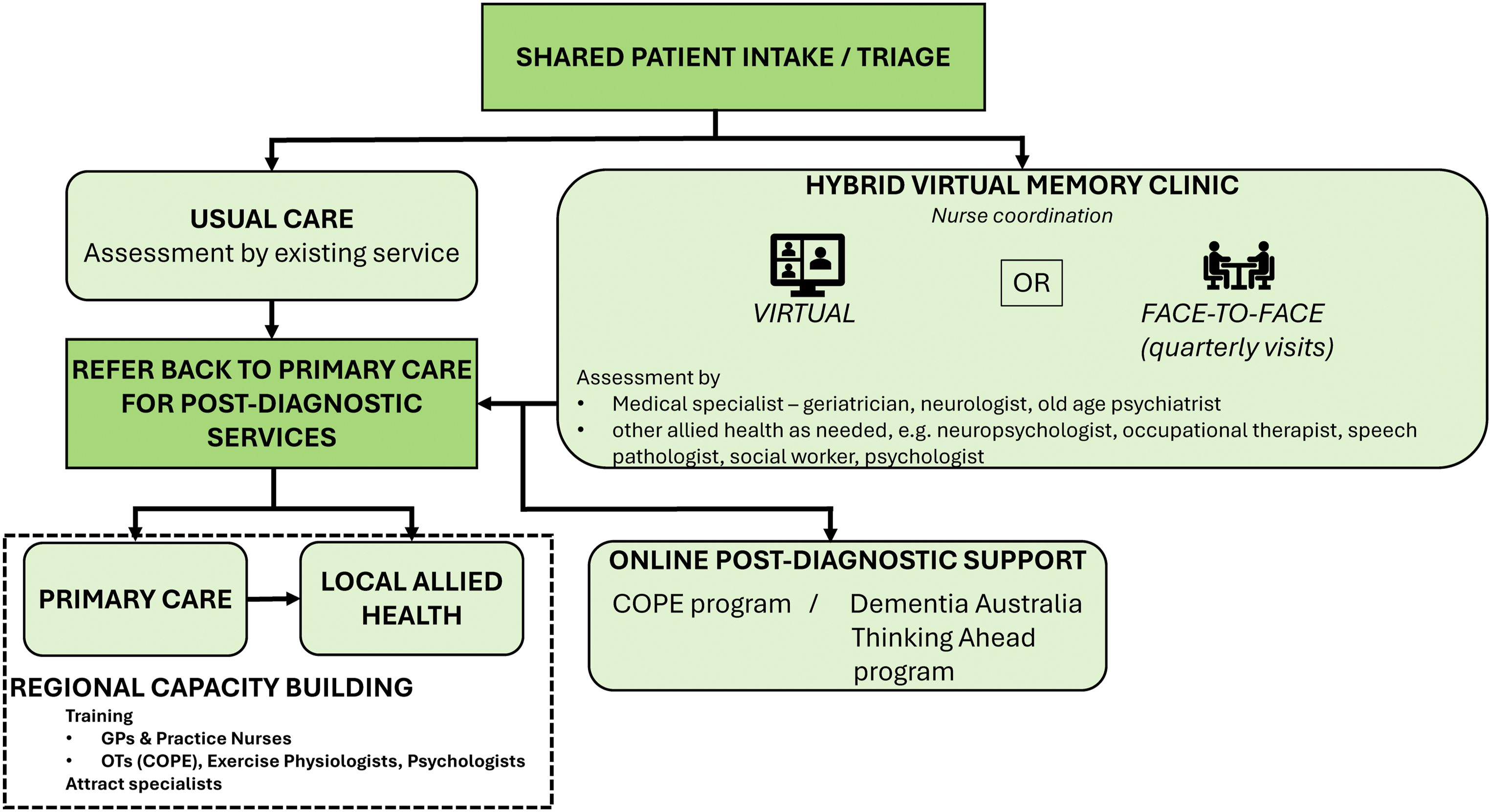
Patients enter via shared intake/triage and receive either usual care or a hybrid pathway with virtual and/or face-to-face assessments by specialists (e.g., geriatrician, neurologist, old-age psychiatrist) and allied health (e.g., occupational therapist, neuropsychology, social work, psychology). build regional capacity.
The final hVMC model includes post-diagnostic services including face-to-face delivery or virtual delivery of occupational therapy via the Care of Older Persons in their Environment program (Clemson et al., 2021; Laver et al., 2020), and cognitive interventions such as Thinking Ahead by Dementia Australia (based on the Healthy Brain Ageing program) (Diamond et al., 2015). The model also includes training and education for local GPs and practice nurses to enhance dementia care skills and build regional capacity.
The co-design process led to key refinements that strengthened the model’s integration and usability. It clarified roles – particularly that of the nurse coordinator – and established clear pathways for post-diagnostic support. The shared intake process was consolidated to improve efficiency, and formal scheduling of face-to-face clinics ensured consistent access for those with more complex needs. To address legal and privacy requirements, separate record-keeping protocols were established: regional clinicians document in their local electronic medical record, while the virtual team maintains parallel records. This dual system ensures compliance with both clinical and regulatory standards.
Some elements discussed during co-design could not be included in the final model due to feasibility and funding limitations. Providing transport for in-person appointments was out of scope; however, implementation planning includes exploring existing transport options to support attendance. Although the need for a dedicated navigator or case manager was strongly highlighted by people with dementia and their care partners, this role was not incorporated, but remains a priority for future planning. This decision was based on equity considerations — such a role should ideally be available to all individuals with dementia, not only those diagnosed through the memory clinic — and because the pilot funding did not cover ongoing post-diagnostic support.
Discussion
We co-designed a hVMC model suitable for tailoring and implementation at regional sites in different Australian states and territories. Our research team made decisions with co-design participants that balanced reported needs and characteristics of an ideal service, with feasibility, funding scope, and budget. There was no consensus on eligibility criteria for virtual assessment, largely because co-design participants felt the need to maintain some flexibility and evaluate suitability on a case-by-case basis, in collaboration with local services.
Our hVMC includes, as core, a local intake officer and a team of clinicians offering services locally, including at least one medical specialist, a neuropsychologist, an intake officer (nursing or allied health), as well as occupational therapists and other allied health as needed. The hVMC is integrated with existing services, with shared intake, and similar post-diagnostic referral to primary care and post-diagnostic care. The model includes face-to-face visits and training for regional GPs, practice nurses, occupational therapists, psychologists, and exercise physiologists in dementia and mild cognitive impairment assessment, post-diagnostic care, and delivery of interventions such as Care of People with dementia in their Environments program. Online post-diagnostic occupational therapy and cognitive intervention programs will also be offered and promoted as pivotal whenever possible.
Primary care professionals will be supported to assist their patients post-diagnosis through flexible follow-up mechanisms, including educational sessions, a letter outlining referrals to services, direct phone contact with hVMC clinicians, and participation in case conferencing. This approach seeks to enhance local workforce capability, improve care coordination, and strengthen integration between specialist and primary care services.
The desired features of a hVMC appear like those co-created for a physical memory clinic such as rapid referrals, diagnostic services, allied health, and ‘one-stop-shop’ with a navigator or key worker (Clemson et al., 2021). Our results were also consistent with a qualitative evaluation (n = 20) of a rural hybrid virtual clinic in North Carolina, USA where the regional sites were two primary care clinics (Steiner et al., 2020). They found that having a physical location for telehealth increased accessibility of the virtual service by providing patients with privacy, supporting older care partners less comfortable with telehealth, and having an in-person staff member to negotiate patient-care partner relationships (Bundy et al., 2022). Our findings were also consistent with an audit of UK memory clinics after the COVID-19 pandemic. It showed that virtual cognitive stimulation therapy services can improve access to services for some people living with dementia, but not for those without the ability to access technology or with sensory impairments, which restrict engagement (Fisher et al., 2023).
Limitations of our model are that the post-diagnostic support currently includes one scheduled follow-up appointment with the specialist, and optional short-term occupational therapy or cognitive intervention programs. Our model does not include case management or navigation as strongly suggested, but notably, these roles are also not part of mainstream memory clinic services in Australia. There are examples of such navigators working as part of virtual services (Liu et al., 2022). Post-diagnostic support will likely vary depending on services within the region.
Virtual neuropsychology is feasible and acceptable with older people, and early results suggest that virtual delivery is comparable to face-to-face neuropsychological assessment (Zeghari et al., 2022). However, further adaptation of some tests for online or local administration (e.g., supervised by neuropsychologist) would be worth considering. We did not work with Aboriginal or Torres Strait Islander Peoples, and hope to engage with them in the future around acceptability, feasibility, and co-design of a virtual memory clinic service to suit their preferences and needs. One challenge will be selection of standardised assessment measures (Hindman et al., 2024). We also have not catered for people whose preferred language is not English, but the use of interpreter services trained in dementia could be considered and trialled. Strengths of the model include its alignment with the needs and preferences of people living with dementia and their care partners, and its feasibility for regional implementation.
Via a face-to-face visit and localisation workshop, our team has further tailored the model to the region of Echuca, Victoria, Australia, where it is currently conducting a feasibility pilot study. The pilot will examine the capability of the hVMC to increase cases seen and provide services within stipulated wait times (Australian Dementia Network, 2021), as well as the accessibility to multidisciplinary assessment. It will also examine the quality of the service for people living with dementia and their care partners, and initial data on the costs of running the model will also be derived from the pilot. We plan to refine and further implement the model if the pilot trial is successful. We anticipate that, over time, the hVMC model will further evolve – such as the use of digital cognitive testing, novel blood-based biomarkers to improve diagnostic accuracy, and high-risk case identification using text mining of electronic records (Gramkow et al., 2024).
Limitations of this study are that we did not engage co-design participants broadly from many different areas, as we concentrated recruitment in regions where we had research partnerships. It is likely that the older people and care partners who participated may have particular familiarity with technology or prior engagement with healthcare services, which could influence their perspectives on virtual healthcare. Additionally, although the inclusion of GPs is acknowledged, it’s worth noting that only two GPs participated in the co-design process, which likely limited their perspective on the development of the model.
Strengths of the study include an experienced team with an extensive network and strong engagement from stakeholders and co-design participants.
Conclusion
We present a hVMC model suitable for regional and rural Australia. Co-designed models need to balance the priorities of the different stakeholders and feasibility of implementation. The next steps are to pilot and evaluate the model in partnership with local health services. Following implementation, we plan to develop a national strategy to scale the model, with implications for improving access to dementia care across Australia.
Footnotes
Acknowledgements
We thank all the co-design participants for their input and Cristian Valenzuela for formatting and paper submission. We thank the Australian Dementia Network for supporting the co-design initiative.
Ethical Considerations
This project was approved by the University of Sydney Human Research Ethics Committee (2023/566).
Consent to Participate
Written informed consent to participate in the study was obtained from all participants prior to their involvement. The study was approved by the University of Sydney Human Research Ethics Committee (HREC 2023/566).
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is part of the Australian Dementia Network (ADNeT) and is delivered in collaboration with the Australian Government Department of Health and Aged Care. It is led by the University of Sydney and supported by funding from the NHMRC National Institute for Dementia Research – Boosting Dementia Grant, Grant/Award Number: APP1152623. SLN is supported by an NHMRC Leadership Fellowship APP2008064.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated during the current study are not publicly available as consent was not obtained for participants for public analysis as some participants are potentially re-identifiable from the transcripts.