
Abstract
It is important to understand the range of transitional care models that support people with dementia who have complex health needs. This is to avoid unnecessary hospitalisations, to maximise any benefits in care transfers and, may increase access to higher quality care and reduce the incidence of low value care. A scoping review of peer-reviewed literature was conducted to investigate and summarise nurse or allied health-led models of transitional dementia care in Australia. Nurse and allied health-led transitional care models for older people and people with dementia included models that emphasised community services, hospital avoidance, out-reach to residential care, emergency department streamlining, intensive dementia support, or a combination (n = 14). Health outcomes reported included decreased presentations, length of stay and costs in emergency departments; reduction in hospital admissions and in medication use and increase in non-pharmacological interventions. Future models of nurse or allied health-led care should emphasise the need for localised relational approaches by the transitional staff to support continuity of care as crucial aspects for behavioural and gerontological transitional care.
Keywords
Introduction
Dementia is a significant health care issue in Australia, compounded by a growing aging population (Australian Institute of Health and Welfare, 2024). In 2023, an estimated 15 people are living with dementia per 1,000 people in Australia, with the majority living within the community (Dementia Australia, 2023). Dementia is a progressive brain disorder resulting in progressive decline (Dementia Australia, 2024), with symptoms affecting memory, speech, cognition, behaviour and mobility (Australian Institute of Health and Welfare, 2024). People with dementia receive care across settings (home, post-acute facilities, hospitals and in residential aged care (RAC)), with support needs increasing with disease progression, and care typically provided by family, healthcare workers, healthcare practitioners and paid carers (Australian Institute of Health and Welfare, 2024; Bail et al., 2018).
People with dementia are commonly admitted to hospital for circumstances other than dementia itself, however, due to dementia, often require a greater number of nursing care hours, longer length of stay and delayed discharge (Bail et al., 2013; Bail & Grealish, 2016). Compared to people without dementia, they experience higher risk of iatrogenic complications (e.g., 1.8 times higher to develop a pressure ulcer and 2.8 times higher to develop a urinary tract infection) and have more complex health needs (Bail et al., 2013). However, despite older people with complex needs (including dementia) being the largest users of beds and care within hospitals, the current hospital system is not well suited to meeting the complex needs of this population cohort (Bail et al., 2013, 2018; Yates et al., 2018).
Furthermore, dementia services in the community have been reported to be fragmented, with poor intersectoral communication (Robinson et al., 2009). Access to general practitioners in the current primary care model is difficult for people with dementia and their carers due to limited appointment time allocation and Medicare rebates (Gibson et al., 2024; Fetherstonhaugh et al., 2021). Within the acute setting, limited clinician knowledge, skills and experience in providing care for people with dementia and complex needs is a current challenge (Evripidou et al., 2019; Schneider et al., 2020; Surr et al., 2016). Poor communication within and between hospitals, community services and residential care (i.e., intersectoral) remains a challenge, contributing to sub-optimal transfer of care (Bail et al., 2009). Within residential care, inconsistent documentation (Yates et al., 2018), declining nursing staff (Rayner & Fetherstonhaugh, 2022), and poor communication between health care professionals and carers (Rayner & Fetherstonhaugh, 2022) are commonly reported challenges.
Nurse-led or allied health-led interventions are valued due to their integrated, multidisciplinary and holistic approach to care (Bail et al., 2009; Ye et al., 2024). This is in contrast to a traditional medical paradigm of curative over preventative, whereby care becomes medicalised based on symptomology (Bail et al., 2009; Ye et al., 2024). In providing care for people with dementia, nurse-led community programs have been shown to reduce stress and improve quality of life for caregivers (Ma et al., 2023; Yamakawa et al., 2022). More information is needed to understand the characteristics, descriptors and evaluation of these models. Previous literature reviews in this area include a focus on hospital discharge for people with dementia (Stockwell-Smith et al., 2018), models of home and community care services for older people (Low et al., 2011), case management/health navigators (Stretton et al., 2023), NPs in aged care (Peters et al., 2024), complex interventions for improving independent living (Ho et al., 2023), management of behavioural and psychological symptoms of dementia in the community (Trivedi et al., 2019), and effectiveness of the Severe Behaviour Response Team (Westera et al., 2020). However, these did not examine transitional models of care, nor effectiveness for people with dementia, specific to the Australian setting.
This scoping review aims to identify and summarise the literature relating to nurse or allied health-led models of transitional dementia care in Australia over the past twenty years. The overarching research question is “What are nurse or allied health-led models of transitional dementia care in Australia?”.
Materials & Method
A scoping review of peer-reviewed academic literature was conducted between July and August 2024, guided by an established methodological framework (Colquhoun et al., 2014) and was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) statement (Figure 1). The scoping review protocol was registered on Open Science Framework (Open Science Framework, 2024). PRISMA Flow Chart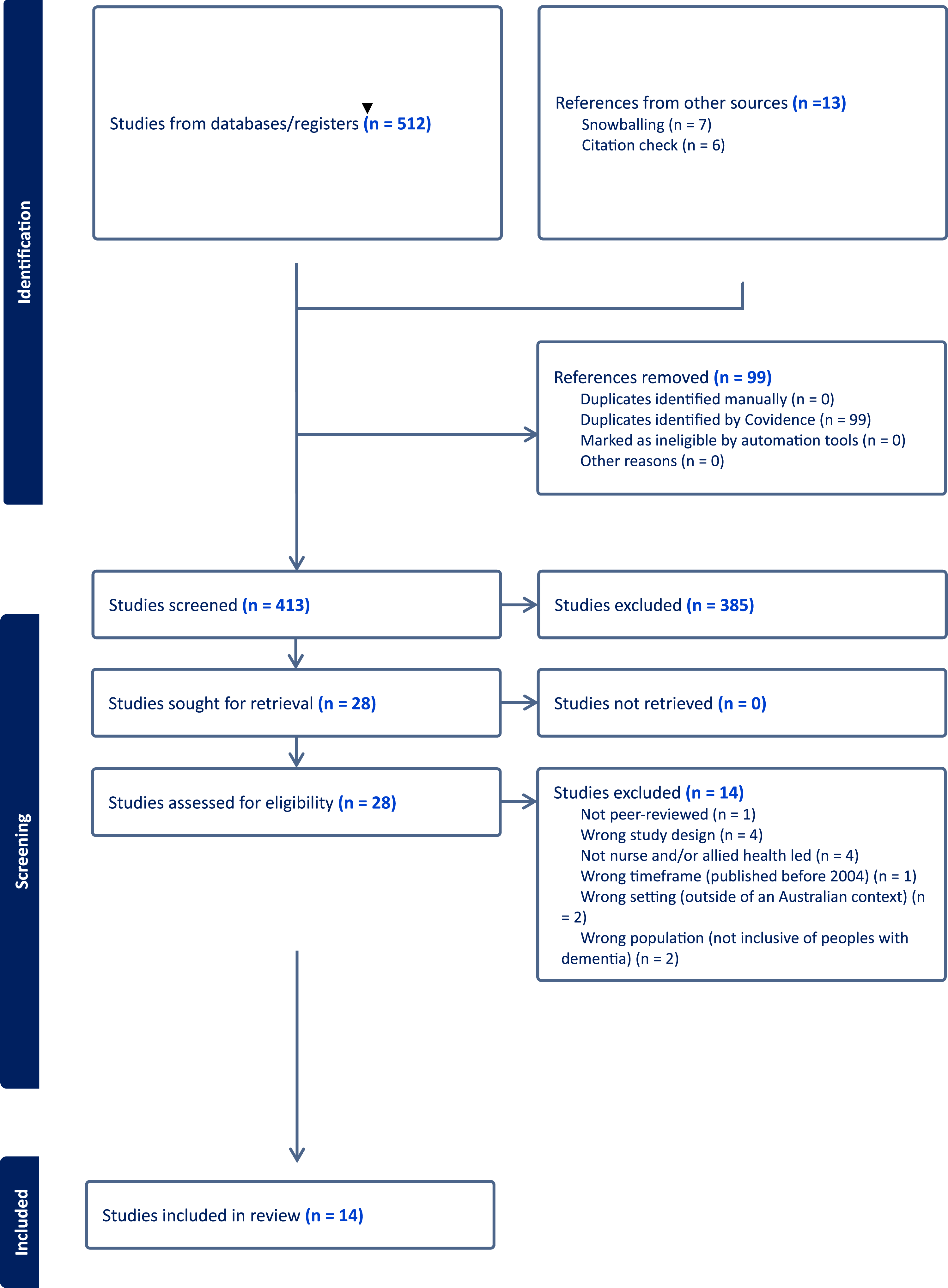
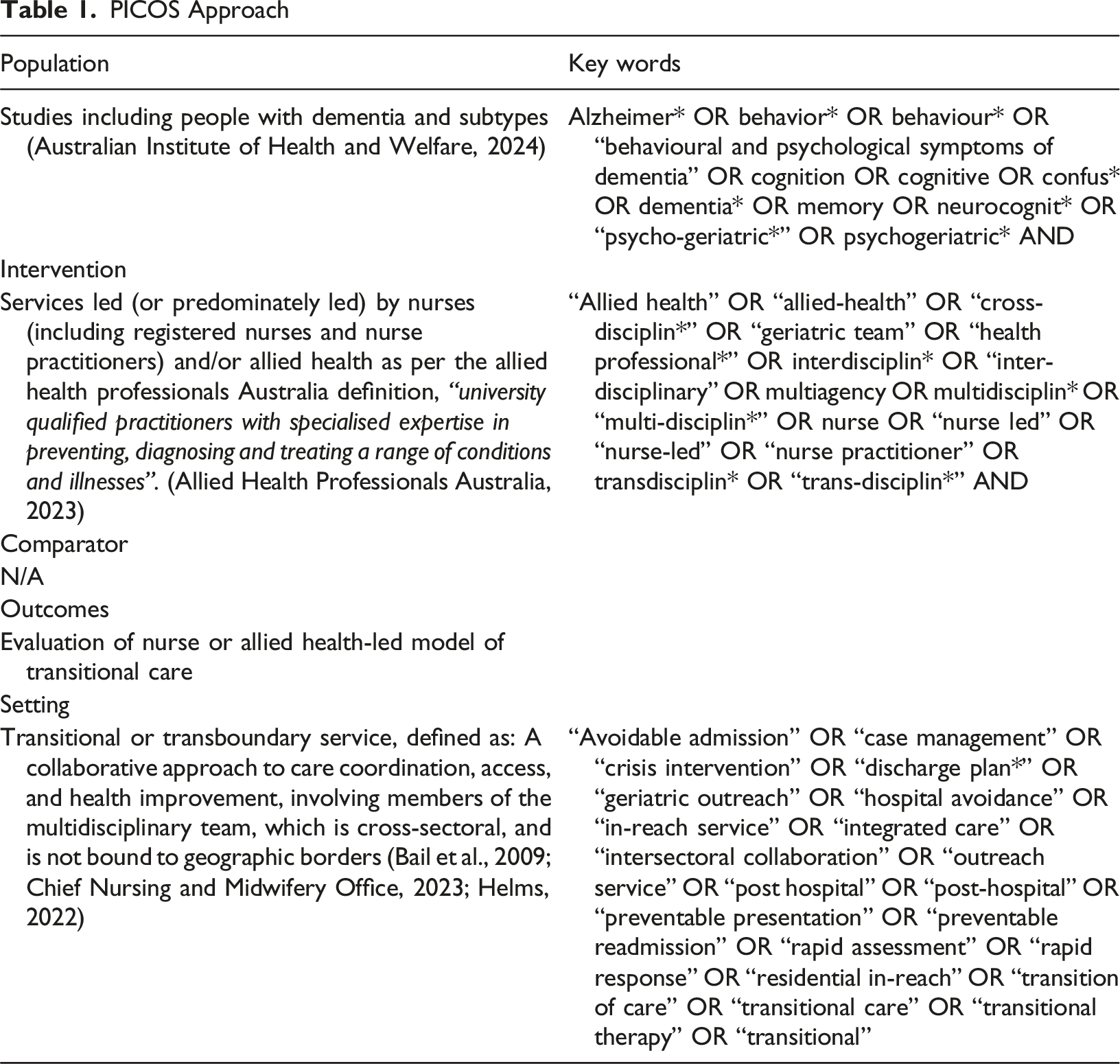
PICOS Approach
Search Strategy
An initial search of MEDLINE and CINAHL was undertaken in consultation with a Research and Information Services Librarian to ensure appropriate use of keywords and search terms. A full search strategy was then developed through the review of titles, index terms and abstracts of relevant articles identified. The search strategy included all identified key words for each database which included, MEDLINE, CINAHL, Web of Science, PsychINFO and Cochrane. These databases were selected as they included important journals across nursing and allied-health disciplines. Manual screening of reference lists of included articles was also undertaken. Studies published between 2004-2024, written in the English language, inclusive of people with dementia, based within an Australian context, peer-reviewed and including an evaluation of a nurse or allied-health-led model with clear multidisciplinary involvement; were included into the review. The search was restricted to articles published within the past twenty years to include articles most clinically relevant to current practice. All study designs were considered if they met all eligibility criteria, however, review articles were excluded.
Screening and Selection of Studies
Following the search, citations were collated using EndNote (Clarivate, Philadelphia, PA, USA) and duplicates were removed. Studies were then uploaded onto Covidence (Veritas Health Innovation), to assist in the management and organisation of study selection and screening. Following a pilot test of 21 studies between four reviewers (SI, ND, KB, RM), all titles and abstracts were screened by one reviewer (RM) for assessment against the inclusion criteria (Ghalibaf et al., 2017). Results were cross-checked by three reviewers (SI, ND, KB). If uncertainty arose regarding eligibility, the study was progressed to full-text screening. Feedback on inclusion and/or exclusion were discussed between the reviewers (SI, ND, KB, RM), with outcomes agreed upon if any deviations occurred. All four reviewers (RM, SI, ND, KB) independently completed full-text reviews against the inclusion and exclusion criteria, with two authors independently reviewing each paper at random. The process was repeated, and any deviations were collaboratively discussed with outcomes agreed upon.
Data Extraction and Presentation
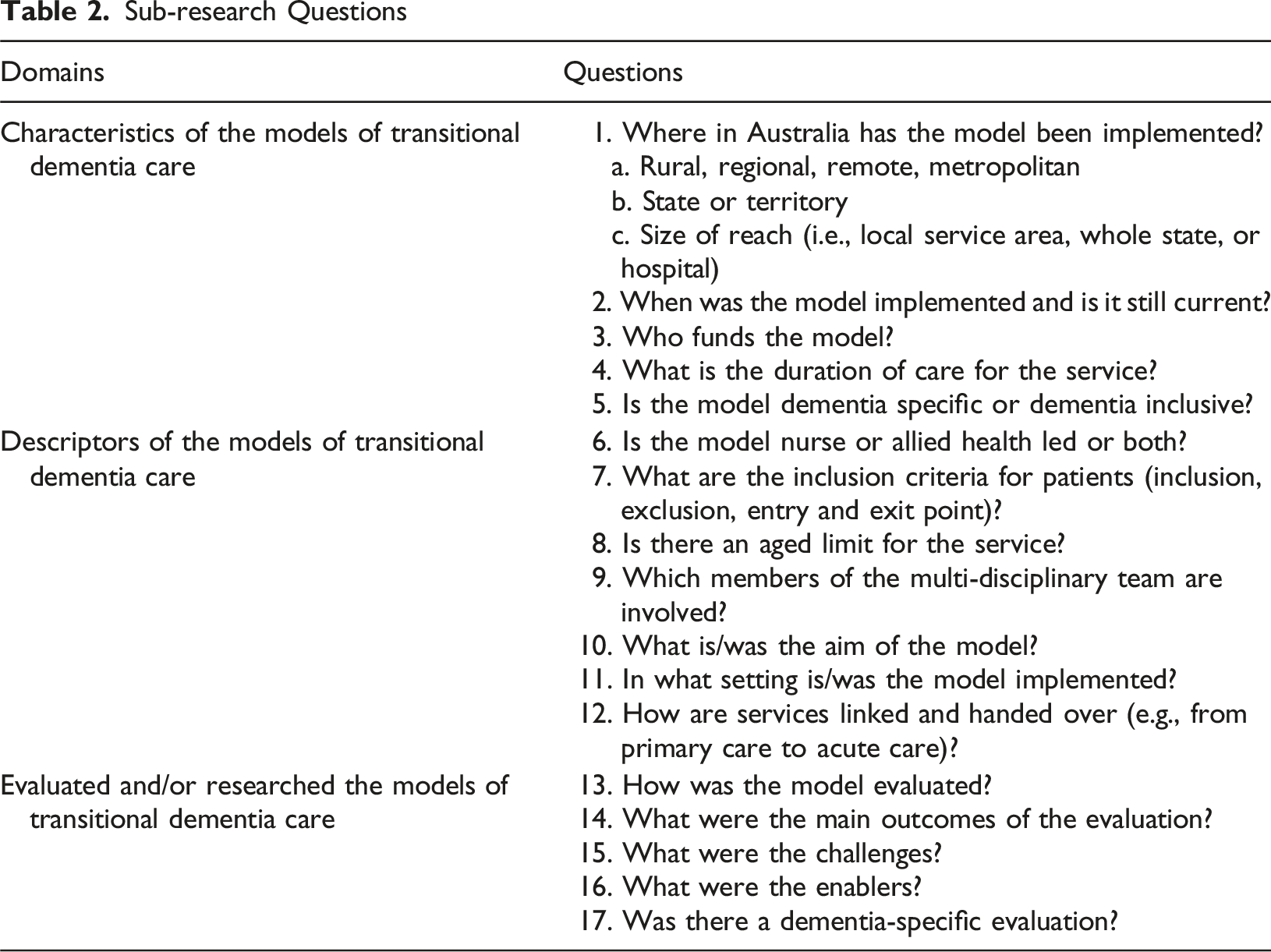
Sub-research Questions
Quality Appraisal
The Mixed Methods Assessment Tool (MMAT) (Hong et al., 2018) was used to evaluate the quality of the studies selected. Two authors (RM and AS) independently appraised papers with disagreements on any criteria discussed until a consensus was reached. No studies were excluded based on the quality appraisal. The results of the quality appraisal are presented using a star rating system based on the percentage of quality criteria met: 100% = five stars; 80% = four stars; 60% = three stars; 40% = two stars; and 20% = one star (Supplemental Table 1).
Results
The search and review process are outlined in the PRISMA flow diagram (Figure 1). The search resulted in identifying 512 studies. After removing duplicates (n = 99), a total of 413 studies were included for abstract and title screening. The title and abstract review identified a total of 28 studies for full-text review. Studies were primarily excluded because they were studies conducted outside of Australia or did not explicitly mention people with dementia (or confusion, behaviours, cognitive impairment, or behavioural and psychological symptoms of dementia). Following full-text review, 14 studies were included (see Figure 1).
Quality Appraisal
Seven studies received a score of five stars (Brooks et al., 2024; Clancy, 2015; Craswell et al., 2020; Dwyer, Craswell, et al., 2017; Hullick et al., 2016; Kable et al., 2015; Kwa et al., 2021), two studies received a score of four (Pond et al., 2021; Waugh, 2009), and five studies were identified to have a score of three or below (Anderson et al., 2020; Borbasi et al., 2010, 2011; Elias et al., 2021; Marsden et al., 2018). Results of the quality appraisal can be found in the Supplemental Table 1.
Study Characteristics
Characteristics of the Transitional Dementia Care Models
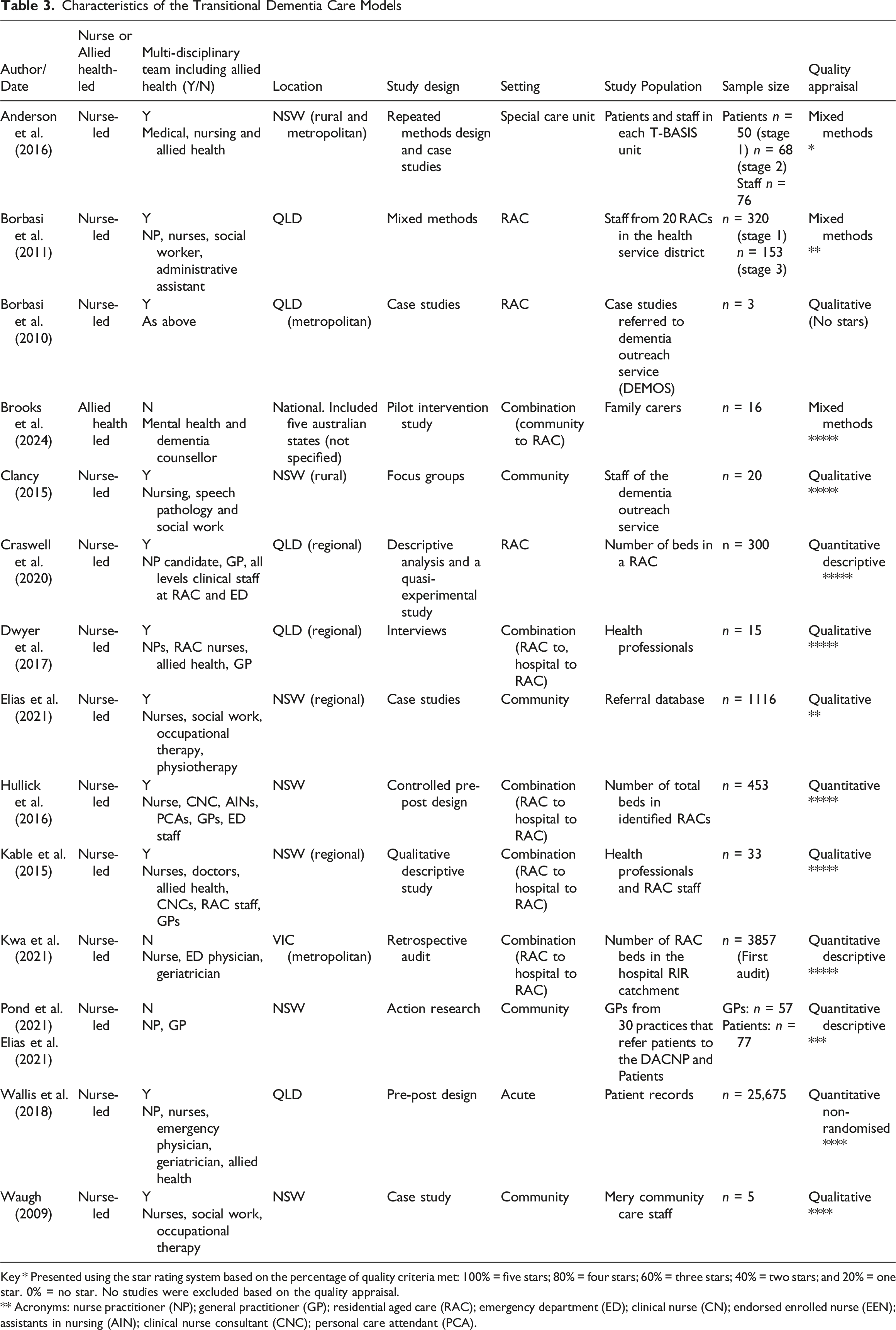
Key * Presented using the star rating system based on the percentage of quality criteria met: 100% = five stars; 80% = four stars; 60% = three stars; 40% = two stars; and 20% = one star. 0% = no star. No studies were excluded based on the quality appraisal.
** Acronyms: nurse practitioner (NP); general practitioner (GP); residential aged care (RAC); emergency department (ED); clinical nurse (CN); endorsed enrolled nurse (EEN); assistants in nursing (AIN); clinical nurse consultant (CNC); personal care attendant (PCA).
Model Characteristics
A total of 14 models of transitional dementia care models were identified (Table 3). The majority of models were nurse-led (n = 13) (Anderson et al., 2016; Borbasi et al., 2010, 2011; Clancy, 2015; Craswell et al., 2020; Dwyer, Craswell, et al., 2017; Elias et al., 2021; Hullick et al., 2016; Kable et al., 2015; Kwa et al., 2021; Pond et al., 2021; Wallis et al., 2018; Waugh, 2009), with only one model being allied health-led (Brooks et al., 2024). Multidisciplinary involvement and composition of the team varied between models. For example, the multidisciplinary team was described as including a NP, Clinical Nurse (CN), Endorsed Enrolled Nurse (EEN), Assistants in Nursing (AIN), clinical facilitator, social worker and administrative assistant (Borbasi et al., 2010, 2011). In comparison, Clancy (2015) described the following professions as part of the multidisciplinary team: nursing, speech pathology and social work (Clancy, 2015). The multidisciplinary team, as outlined by Elias et al. (2021), described a more varied team containing nursing, social work, occupational therapy and physiotherapy. This model also integrated services from dietetics, speech pathology, clinical psychology and, where required, a health justice lawyer (Elias et al., 2021).
Models were implemented across a range of different settings, including within the community (Elias et al., 2021; Pond et al., 2021; Waugh, 2009); RAC (Borbasi et al., 2010, 2011; Clancy, 2015); acute settings (i.e., emergency department (ED), special care unit, hospital) (Anderson et al., 2016; Wallis et al., 2018) and across settings (Brooks et al., 2024; Craswell et al., 2020; Dwyer, Alison, et al., 2017; Hullick et al., 2016; Kable et al., 2015; Kwa et al., 2021) (Figure 2). The Different Settings of the Transitional Dementia Care Models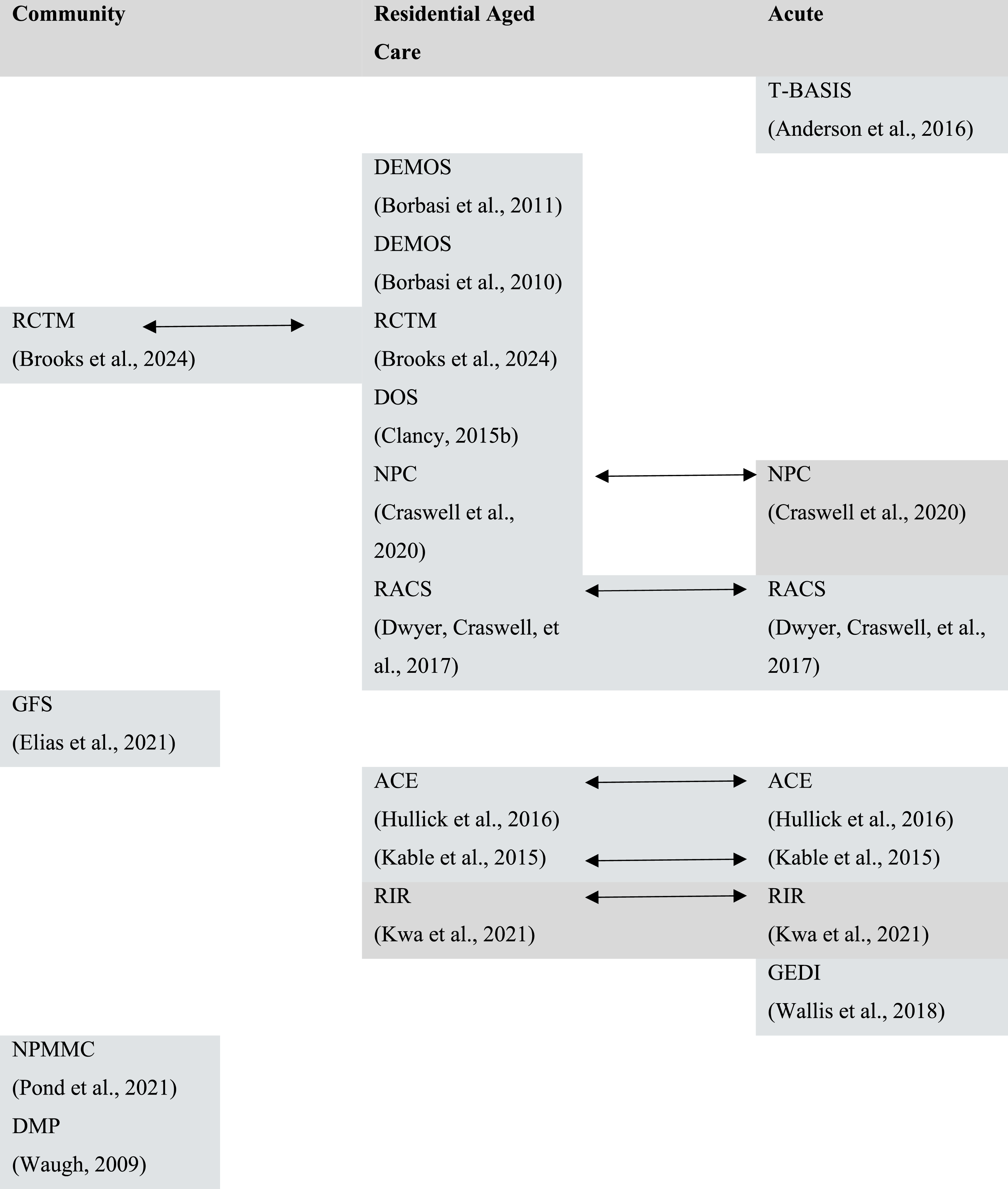
The Geriatric Flying Squad (GFS) model was a community-based model, with an aim to improve access for vulnerable, frail older people to a multidisciplinary service (Elias et al., 2021). Through reciprocal referral pathways, emergency responders (NSW Ambulance, Police and Fire and Rescue) were able to assess the individual and provide care as an alternative to a hospital admission (Elias et al., 2021). Also aligning with improving community access to health services, the Mobile Memory Clinic (MMC), provided assessment and care for a patient in their own home by an NP (Pond et al., 2021). The Dementia Monitoring Program (DMP) was another community-based model, aimed at providing a specialist service for individuals living alone with dementia (Waugh, 2009). One model that primarily provided support for the RAC was the Dementia Outreach Service (DEMOS) model (Borbasi et al., 2010, 2011). This model provided specialist support to RACs within the Metro South Health Service District of Queensland (Borbasi et al., 2010, 2011). The Residential Care Transition Model (RCTM), provided support for people with dementia and their families in the community by assisting prior to permanent residential care (Brooks et al., 2024).
Two models were positioned within the acute setting (Anderson et al., 2016; Wallis et al., 2018). The Transitional Behaviour Assessment and Intervention Service model (T-BASIS) emerged from a NSW Health commissioned review of existing CADE units (Confused and Disturbed Elderly) with an aim to provide a service between acute inpatient care and long-stay residential care (Anderson et al., 2016). The T-BASIS model delivered care both within a hospital’s special care unit and in the RACs where the patient was initially referred (Anderson et al., 2016). Coordinating care through the ED of a hospital, the Residential Aged Care and Primary Health Collaboration (CEDRiC) project is a model that facilitates response communication and collaboration between the Health Intervention Program for Seniors (HIPs) and Geriatric Emergency Department Intervention (GEDI) services (Marsden et al., 2018). The GEDI service aims to where possible, avoid hospital admission, and if not, ensure faster admission and medical management for the person with dementia (Wallis et al., 2018).
In contrast, most of the models used services that moved across settings in a bi-directional manner, from one to another (Brooks et al., 2024; Craswell et al., 2020; Dwyer, Craswell, et al., 2017; Hullick et al., 2016; Kable et al., 2015). These models primarily encouraged communication between RAC and the acute setting, with the aim of reducing avoidable hospitalisations (Craswell et al., 2020; Dwyer, Craswell, et al., 2017; Hullick et al., 2016; Kwa et al., 2021). The Residential Acute Care Service (RACS) model used a NP to provide early intervention to a deteriorating resident within the RAC, or, if admitted to hospital, to coordinate care and early discharge back to the RAC (Dwyer, Craswell, et al., 2017). The Aged Care Emergency Service (ACE) model aimed to also avoid hospital admissions of residents from the RAC by providing clinical support to nurses to provide care in situ (Hullick et al., 2016). Additionally, the Residential in Reach (RIR) model also aimed to reduce avoidable hospital admissions for acute conditions for residents of the RAC (Kwa et al., 2021).
Summary of the Models of Transitional Dementia Care
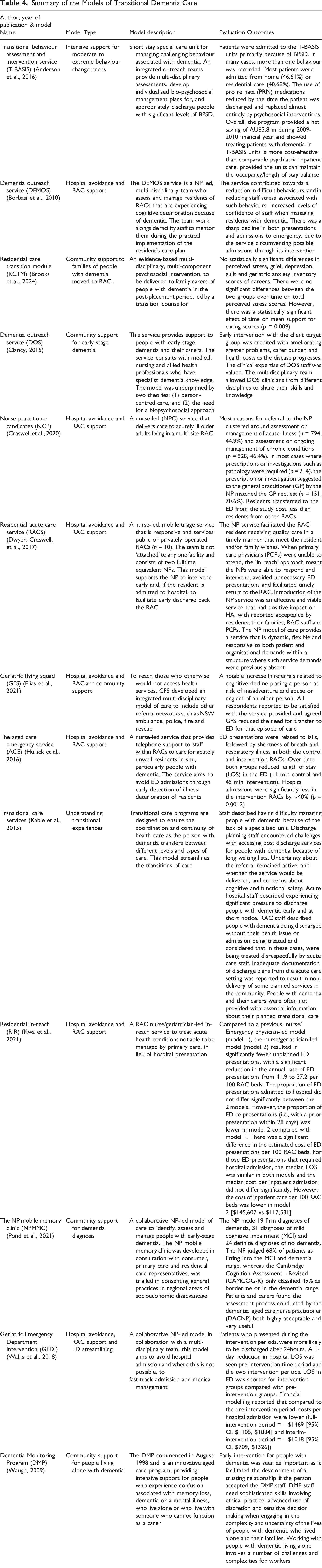
Other models were community focused, providing support for people living in the community with dementia and their families/carers (Brooks et al., 2024; Clancy, 2015; Elias et al., 2021). These models identified that the families and carers of people with dementia need support, especially pertaining to decisions around transitioning from home to RAC placement (Brooks et al., 2024). In addition, information about managing early-stage dementia was also given to support carers and families through access to specialist health professionals with dementia knowledge (Clancy, 2015). Similarly, transitional support was also given to staff within the acute setting and in RAC. This support aimed to streamline the admission and discharge process and improve communication between the two settings (Kable et al., 2015) and to empower staff through upskilling to enable ethical decision making when engaging in complex situations with family/carers of people with dementia (Waugh, 2009). Alternatively, the T-BASIS model provided intensive support for people with moderate to extreme behaviour change needs within a special care unit (Anderson et al., 2016). Patients admitted into the T-BASIS special care unit often displayed more than one changed behaviour, including wandering, verbal aggression, sexual disinhibition and physical aggression, typically during personal care (Anderson et al., 2016).
Enabling Components of Models of Transitional Dementia Care
Supporting Quotes From Models of Dementia Care - Enablers
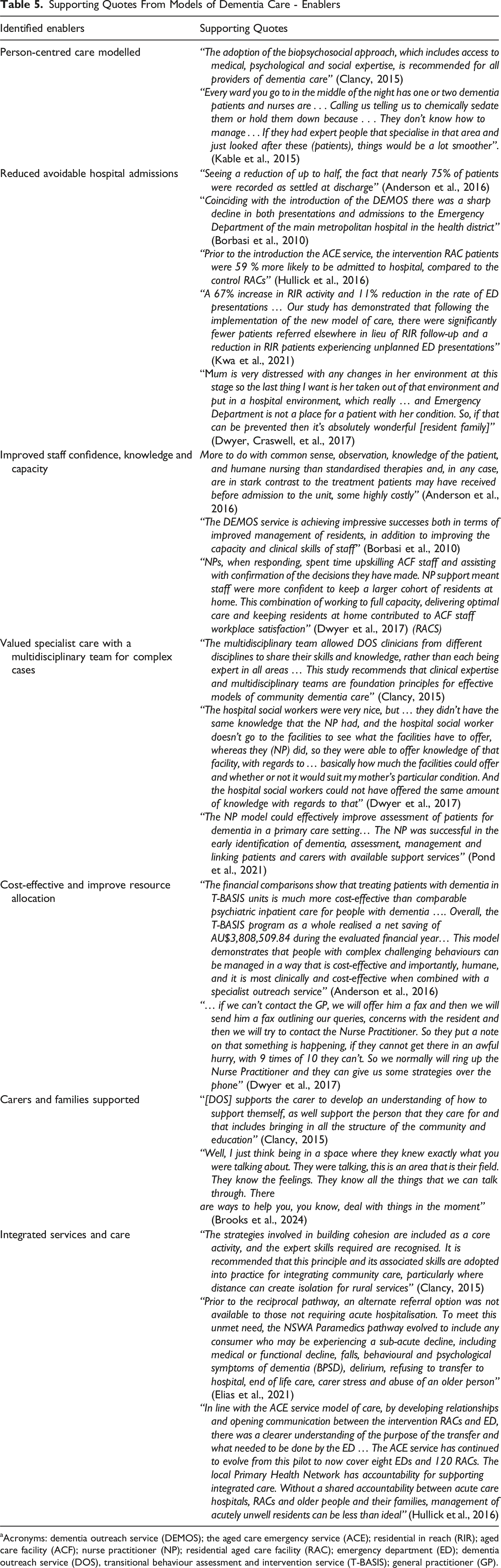
aAcronyms: dementia outreach service (DEMOS); the aged care emergency service (ACE); residential in reach (RIR); aged care facility (ACF); nurse practitioner (NP); residential aged care facility (RAC); emergency department (ED); dementia outreach service (DOS), transitional behaviour assessment and intervention service (T-BASIS); general practitioner (GP).
Patient/resident-centred care was at the forefront of models (Anderson et al., 2016; Clancy, 2015; Craswell et al., 2020; Kable et al., 2015; Waugh, 2009). Applying this lens improved the quality of life of people with dementia and/or with challenging behaviours as it highlighted the person rather than a medical diagnosis. Typically guided and supported by an NP, alternative case management, and strategies that employed psychosocial principles rather than a reliance on pharmaceutical interventions were suggested and implemented in collaboration with the RAC nursing and residential care staff (Anderson et al., 2016; Clancy, 2015; Craswell et al., 2020; Kable et al., 2015; Waugh, 2009). The DEMOS model highlighted this underpinning philosophy as using, “ minimal medication with maximal nursing interventions” (Borbasi et al., 2011). The NPs of the T-BASIS service encouraged the implementation of psychosocial interventions by RAC nursing staff, resulting in improved quality of care for residents. Without the T-BASIS service, 40.7% of nurses stated they would have used sedation to manage patients, 18.5% would have asked for a GP medical review, 7.4% would have sent the patient to ED, another 7.4% would have referred the patient to local mental health team and 7.4% would have used one-to-one special care (Anderson et al., 2016).
A reduction in the number of avoidable hospital admissions were reported by services which integrated a NP to coordinate supportive care and guide clinical and behaviour management plans for residents/patients across RAC and acute settings (Anderson et al., 2016; Borbasi et al., 2010, 2011; Craswell et al., 2020; Hullick et al., 2016; Kwa et al., 2021). While the hospitalisation rates of residents from RACs varied between models, the involvement of a NP consistently resulted in fewer admissions (Anderson et al., 2016; Borbasi et al., 2010, 2011; Craswell et al., 2020; Hullick et al., 2016; Kwa et al., 2021). For example Craswell et al. (2020) reported that 61.8% of transfers to the emergency department occurred when the NP was not on duty, compared with 21.5% when the NP was present (Craswell et al., 2020). Avoiding unnecessary hospital admissions not only ensured the continuity of care for the residents within a familiar environment but was also highly valued by carers and family members.
Models that invested NP time to provide training to staff across different settings resulted in an increase in confidence, knowledge and capacity to provide care for residents and people with dementia and/or with changed behaviours (Anderson et al., 2016; Borbasi et al., 2010, 2011; Clancy, 2015; Dwyer, Craswell, et al., 2017; Hullick et al., 2016; Kable et al., 2015; Pond et al., 2021; Wallis et al., 2018). This in turn also contributed to avoiding hospital admissions of residents as RAC nursing staff were better equipped to identify, treat and manage the complex needs of residents (Anderson et al., 2016; Craswell et al., 2020; Elias et al., 2021; Kwa et al., 2021). NPs provided reassurance and guidance about the severity of symptoms of residents in relation to whether immediate admission to hospital was required (Dwyer, Craswell, et al., 2017). This form of support from NPs to RAC nursing staff was highly valued, considering limited access to GPs (Clancy, 2015; Dwyer, Craswell, et al., 2017).
It was reported that the complexity of care for people with dementia and/or with changed behaviours was often exacerbated by multiple co-morbidities (Anderson et al., 2016). Thus, the need for specialist gerontological care was not only recommended but commonly emphasised in many of the studies (Anderson et al., 2016; Clancy, 2015; Dwyer, Craswell, et al., 2017; Elias et al., 2021). For example, the T-BASIS study reported that residents are “often admitted to the units because the resources of their RAC are insufficient to provide appropriate management where they are” (Anderson et al., 2016). In most studies, this specialist care was NP-led, who has the knowledge and expertise to fulfil this care need with support from a multidisciplinary team (Anderson et al., 2016; Clancy, 2015; Dwyer, Craswell, et al., 2017; Elias et al., 2021). Confirming the expertise of the NP, it was recognised and reported that the identification, diagnosis and care management plan devised were similar to that of the residing GP at the RAC (Craswell et al., 2020). This was further supported by findings from the NPMMC model which indicated that the NP had the clinical knowledge and expertise to effectively identify, assess and manage people with dementia (Pond et al., 2021).
Additionally, it was reported that nurse-led models of care have the potential to be more cost-effective because hospital admissions, re-admissions and hospital length of stays are reduced, compared to non-nurse-led models (Anderson et al., 2016; Craswell et al., 2020). Dwyer et al. (2017) highlighted that the NP intervention kept residents at home and saved other healthcare services such as ambulance, emergency and inpatient care time. The T-BASIS model evaluation reported a net saving of AU$3,808,509.84 (Anderson et al., 2016), while the RIR model reported significant cost savings, with a 9% reduction in the estimated cost of emergency presentations and a 19% reduction in actual inpatient costs (Kwa et al., 2021). The cost-effectiveness of avoidable admissions, in addition to improved quality of care, was also emphasised.
Collaboration and integration of services and care across all settings (i.e., home, community and acute) was recommended, especially for rural and remote health districts (Clancy, 2015; Dwyer, Craswell, et al., 2017; Elias et al., 2021; Hullick et al., 2016; Kable et al., 2015; Kwa et al., 2021; Waugh, 2009). NPs were identified as playing a crucial role in ensuring an integrated system of care and were commonly described as being the communication ‘bridge’ between settings and services” (Dwyer, Craswell, et al., 2017).
Barriers to Model Sustainability and Effectiveness
Supporting Quotes From Models of Dementia Care - Barriers
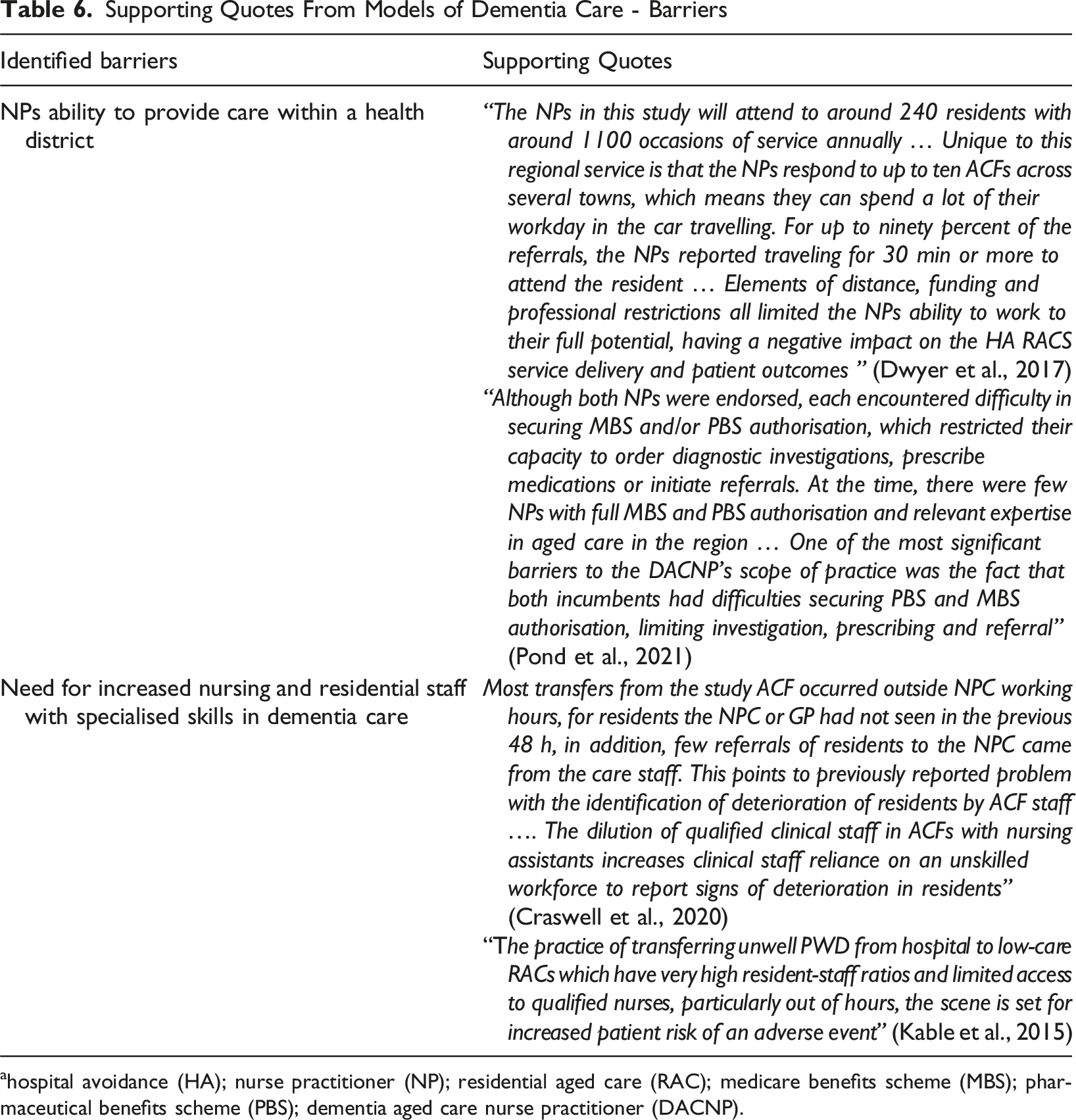
ahospital avoidance (HA); nurse practitioner (NP); residential aged care (RAC); medicare benefits scheme (MBS); pharmaceutical benefits scheme (PBS); dementia aged care nurse practitioner (DACNP).
Studies identified that due to a high case load associated with providing care within the community and in RACs across multiple health districts or over large geographical distances, NPs often reported conflicting priorities that were exacerbated by time lost due to travel (Anderson et al., 2016; Clancy, 2015; Dwyer, Craswell, et al., 2017). While GPs, nursing and residential staff endorsed the role of NPs in providing care for residents, professional restrictions were also noted as barriers to care and included: ability to prescribe medication, services not eligible for Medicare rebates and tensions in determining the NP is working to their full scope of practice (Dwyer, Craswell, et al., 2017; Pond et al., 2021).
Additionally, another barrier was current nursing and residential staff knowledge, skills and workload capacity to manage residents with dementia and/or with challenging behaviours (Anderson et al., 2016; Craswell et al., 2020)
Discussion
The review found published evidence of a range of transitional nurse-led models and a single allied-health-led model in Australia, including community support, hospital avoidance (which often included a form of residential aged care in-reach), and intensive support by way of standalone units. The studies were predominantly qualitative evaluations, with some quantitative measures that were not consistent and, therefore, not comparable.
The community support approach ranged from home visits by a NP for dementia diagnosis to follow-up support for carers when a person with dementia has transitioned to residential aged care. Diagnosis of dementia is a key gap in service provision (Cappetta et al., 2020), and effective pathways to develop NPs are needed to enhance care delivery for this population (Peters et al., 2024). The finding that trainee NPs can fill this gap while working towards endorsement warrants further implementation investigation. NPs/Advanced Practice nurse-led models of care have also shown promise internationally (Callaghan, 2008; Naylor & Kurtzman, 2010). The in-reach service approach is common in multiple hospital models, with a recent survey of geriatric medicine departments showing that 59% of those surveyed have such a service to RAC, but that one of the most frequent suggestions to manage gaps is to increase staff numbers and policy for sufficient reach and impact of in-reach/outreach care (Azarias et al., 2024). Intensive support was only reported in one identified model (Anderson et al., 2016). Purpose-built behavioural management units are highlighted as a need in the recent geriatric survey (Azarias et al., 2024).
Underlying all the models is a response to gaps in workforce related to specialised gerontological knowledge and pathways to support clinicians to choose aged care as a career (Peters et al., 2024; Traynor et al., 2024). The lack of clinical functionality of residential aged care has been problematic for some time as highlighted by the Australian Royal Commission into Aged Care Quality and Safety (2021), and the resultant changes to bolster the workforce, policies and practices, and sustain the retention of high quality clinicians in residential care will take time (Traynor et al., 2024). Hospitals, health services and governments have long recognised that hospital avoidance is an important service pathway that can be served by in-reach to residential aged care in order to positively affect hospital length of stays (Australian Institute of Health and Welfare, 2024), as demonstrated by the high rates of out-reach services from geriatric departments (Azarias et al., 2024).
In a 2,023 review of complex care models for older people internationally, most included holistic assessment (94%) and care planning (90%), half involved multidisciplinary care (54%), most were delivered mainly by primary care teams without geriatricians (30%) (Ho et al., 2023). Ho highlights that nurses were the most frequent care coordinators, and this is reinforced by our review. Complex interventions increased the likelihood of living at home, reduced mortality, enhanced cognitive function, and improved instrumental activities of daily living (Ho et al., 2023). This highlights the need for transitional models to provide complex interventions to sustain independence and delay acute and residential interventions.
The modelling of care behaviours by experienced staff with clinical credibility, additional staff to improve ratios in order to add responsiveness, and the concomitant support network for nurses, were crucial to success in a number of programs in this review Borbasi et al. (2011); Clancy (2015); Dwyer, Craswell, et al., 2017; Elias et al. (2021); Hullick et al. (2016); Kwa et al. (2021); Westera et al. (2020) rapid evidence assessment examined localised rapid response services targeting people with changed behaviours related to dementia, highlighting the Severe Behaviour Response Team (SRBT) as a large-scale intervention (Westera et al., 2020). Operational attributes key to responding were: clearly defined parameters and processes; provision of clinical expertise and knowledge translation activities; person-centred philosophy; relationship-oriented approach to stakeholders (Westera et al., 2020). Differences between large, centeralised responses like SRBT and local programs that build community and workforces show warrants further study. Clinician leadership of residential care staff can leave staff feeling empowered and supported as a primary outcome, even where the behaviours remain ‘unsolved’ (Anderson et al., 2020). Specialised training and education are key components in delivering effective transboundary transitional care in previous studies (Naylor & Kurtzman, 2010, Callaghan, 2008; Boltz, 2015; Renehan, 2013); this review emphasises the localised and relational nature of transitional support services as key to successful outcomes in staff education as well as resident care. Future models or embellishments should emphasise these relational approaches in conjunction with continuity of care as crucial aspects for behavioural and gerontological transitional care.
A key issue revealed in the review was the need to decrease the separation of community and acute services, with nurses frequently providing a bridge between services and a rapid response to prevent deterioration of the older person and decrease magnitude of health issues. These transitional nursing (or allied health) roles are arguably particularly important in a climate of nurse dissatisfaction with role and burnout, and ongoing calls for maximising nursing capacity (Peters et al., 2024) and recognition that nurses are often not able to work to their full scope of practice. In particular, endorsed NPs, can encounter barriers in ordering subsided diagnostic testing and prescription medication. These are important avenues for investigation and development to ensure models of care are maximised for greatest impact on patient experiences.
It is also important to note often registered nurses in RAC are unable to work to their full scope of practice due to RAC workforce training, skills and capacity Royal Commission into Aged Care Quality and Safety (2021). It was only after the Australian Royal Commission that dementia care training became mandatory for personal care workers. When RAC staff are underperforming, nurses must fill these gaps, limiting their capacity to focus on higher-level care. Additionally, staffing numbers and ratios required a Royal Commission to even be recognised as key to adequately respond to complex behavioural care needs Royal Commission into Aged Care Quality and Safety (2021). While the increase in staffing ratios have likely improved since the studies in this review were conducted, the models of care reported in this review highlight the variation between services and the uneven nature of advancement in skills, knowledge and capacity across sectors and locales. It is important to recognise that both quality of knowledge and skills as well as quantity of staffing will impact older person health outcomes. The studies in this review highlighted the responsiveness of transitional gerontological NP roles to adapt to service and workforce needs in situ.
There are known alternative models that were not revealed in the review. These include nurse navigators, which are well established in managing complex care such as people with cancer and transitioning to self-management, so there may be scope for pivoting to dementia and gerontological care (Byrne et al., 2024). GP-led models of collaborative dementia care management have also been found to be associated with fewer BPSD symptoms, better mental health and lower caregiver burden (Byrne et al., 2024). Advanced practice nurses are found to support the management of geriatric conditions all over the world, including cognitive decline and delaying or averting the development of disability (Fougère et al., 2018). These models may also provide important insights for further research and development.
The strength of this review is that it provides an overview of the last twenty years of peer-reviewed literature related to transitional care in Australia, inclusive of people with dementia. Limitations included identification of keywords due to the variation in nomenclature and unique nature of the models. Many papers focused on gerontological populations without explicit mentions of dementia, behaviours or cognition, though likely included conditions with cognitive impairment. This invisibility of dementia and changed behaviours within the gerontological models may be partly due to the difficulty in accessing accurate and reliable diagnosis and documentation of dementia (Cummings et al., 2011).
Conclusion
Nurse and allied health-led transitional care models for older people and people with dementia were any one of (or a combination of) community bolstering, hospital avoidance and in-reach to residential care, or intensive dementia support focused. These models were associated with some improved health outcomes including decreased presentations, length of stay and cost in emergency departments, reduction in hospital admissions, reduction in medication use, increase in non-pharmacological interventions, decrease in carer time burden, and increase in documented diagnosis of dementia. Staff impacts included gains in confidence, knowledge and capacity of staff across settings and satisfaction with care models trialled. Key enablers of transitional models were effective integration of multidisciplinary team collaboration, and support for carers. Key barriers included restrictions to nurse (and in particular NP) scope of practice, and the need for more specialised dementia care nurses and residential staff. Integration of specialised NPs can provide further support in upskilling and educating ‘insitu’ staff and thus contributing to improved confidence, skills and knowledge in dementia care provision. However, it is worth noting that currently within Australia, there is a small pool of highly skilled dementia care nurse practitioners and ongoing issues with recruitment and retention within these roles. Further support for multidisciplinary workforce mix in dementia services, and education for all clinicians regarding collaborative skills and training were implicated by this review. Future models or embellishments of nurse or allied health-led care should emphasise the need for localised relational approaches by the transitional staff to support continuity of care as crucial aspects for behavioural and gerontological transitional care.
Relevance for Clinical Practice
This review found that nurse-led in-reach services to aged care, emergency department streamlining for people experiencing changed behaviours, and intensive behaviour support units were associated with positive health and service outcomes for dementia care. The clinical credibility and expertise of the nurse or allied health professional leading the services were found to be important for providing relational approaches to health staff education as well as continuity of care for residents/patients.
Supplemental Material
Supplemental material - Nurse or Allied Health-Led Models of Transitional Dementia Care in Australia: A Scoping Review
Supplemental material for Nurse or Allied Health-Led Models of Transitional Dementia Care in Australia: A Scoping Review by Rebecca Mete, Aisling Smyth, Nathan D’cunha, Diane Gibson, Stephen Isbel and Kasia Bail in Dementia
Footnotes
Acknowledgements
The papers authors appreciate the members of the Centre of Ageing Research and Translation and the Dementia Health Experts Network feedback and contributions to the development of this work. Acknowledging the evolving nature of language, the authors have endeavoured to use respectful language throughout this report as guided by the Dementia Australia Language Guidelines (Dementia Australia, 2023). As a scoping review, oftentimes the language of the source material was used which may not be consistent with the current guidelines. The University of Canberra acknowledges the Ngunnawal people, traditional custodians of the lands where Bruce Campus is situated. We wish to acknowledge and respect their continuing culture and the contribution they make to the life of Canberra and the region. We also acknowledge all other First Nations Peoples on whose lands this report was prepared.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report about nurse or allied health-led models of transboundary dementia care in Australia was partially funded by the ACT Health Directorate. This is a second of two reports commissioned by ACT Health Directorate from Centre for Ageing Research and Translation related to dementia, with the first report relating to health professional interviews and recommendations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.