
Abstract
As the prevalence of dementia rises exponentially globally, instituting practices to support the dying process of people affected by dementia is a public health priority. However, end-of-life quality indicators such as place of death provide limited information about the totality of the dying process. Hence, this study’s aim was to identify factors affecting the relatively understudied concept of final place of care (where care was received in the last three days of life i.e. home/inpatient hospice/hospital) and its concordance with previously stated preferences (goal-concordance). A retrospective cohort study was conducted using secondary data (electronic medical records) from 284 individuals enrolled in a home-based palliative care service for people with advanced dementia in Singapore. Despite demonstrating positive impacts, the service was unable to meet some individuals’ end-of-life preferences. Analysis used multivariate binomial logistic regression, concordance and sensitivity analyses. Results found home to be the most common final place of care (81.7%). Better biological and functional status, and inconsistent preferences for place of care and death predicted hospital admission for care (9.2%). Discomfort, oral feeding, psychosocial challenges, and family unemployment predicted inpatient hospice admissions (9.2%); these were often late and unplanned, suggesting a preference for home until death was imminent. Better prognosis, infection two weeks before death/admission, higher caregiver burden and psychosocial challenges predicted non-concordance with preferences (14.4%). The results highlight the unpredictable, protracted trajectory of people with advanced dementia and the multifaceted challenges of end-of-life care and death. Unlike place of death, relatively stable factors (sociodemographic, chronic comorbidities) had no effect on final place of care. These fresh insights, supported by findings about end-of-life transitions in international literature, have implications for policies and practices to advance the global health goal of facilitating people with advanced dementia not just to die but to spend their final days at their place of choice.
Background
Dementia is a global public health priority (Nichols et al., 2022; World Health Organization, 2023). As a multifactorial condition, people with dementia experience progressive cognitive and functional decline, and become completely dependent on others for all aspects of care and decision-making in the advanced stage (Eisenmann et al., 2020; Emmady et al., 2024). Family caregivers of people with advanced dementia take on a particularly wide range of responsibilities (Chiao et al., 2015). Besides providing physical assistance and care, they often have to make decisions on their relatives’ behalf, despite feeling ill-equipped, uncomfortable and stressed doing so (Nakanishi et al., 2024; van der Steen et al., 2024). Because of the high care needs, they are often unable to take on formal paid work nor participate in social/leisure activities, resulting in social isolation (Broady et al., 2018; Brodaty & Donkin, 2009). The high rates of multimorbidity and susceptibility to infections for the person with advanced dementia may also incur high healthcare costs (Bunn et al., 2014; Phelan et al., 2012). Associated frequent hospitalisations increase the risks of delirium, distress and confusion (Mitchell et al., 2009; Sadak et al., 2017), thereby compounding caregiver burden and healthcare system strains (Nichols et al., 2022; Sadak et al., 2017). In 2019, dementia cost the global economy US$1.3 trillion, 50% of which was attributable to informal care by families/friends, who provide on average 5 hours of care per day (World Health Organization, 2023). The health, social and economic impacts of dementia are therefore substantial (Nichols et al., 2022).
As a care approach that addresses the physical, psychological, social and spiritual needs of individuals with life-limiting illnesses (World Health Organization, 2020), palliative care could potentially mitigate some of the negative implications of dementia (Eisenmann et al., 2020). Studies have found palliative care to be associated with improved symptoms and quality of life (Eisenmann et al., 2020; Hum et al., 2019; Sampson, 2010), enhanced caregivers’ satisfaction with care (Tay et al., 2020), and reduced healthcare utilisation and costs in advanced dementia (Pereira et al., 2020), although more robust evidence is still needed (Walsh et al., 2021). A palliative care approach for people with dementia is also recommended by the European Association for Palliative Care (van der Steen et al., 2014). However, despite being a life-limiting illness with no known effective disease-modifying treatment and high, complicated care needs (Eisenmann et al., 2020; van der Steen et al., 2014), inequity in access to palliative care persists for people with advanced dementia (Nichols et al., 2022). They also often do not have the same opportunity to die at home, which is the preference of the general population of people surveyed (Mogan et al., 2018).
As with most other developed nations, Singapore faces a number of challenges in dementia care because of its ageing population (Nichols et al., 2022). The number of people with dementia increased by more than 40% over 10 years from 51,934 to 73,918 in 2023 (Subramaniam et al., 2025). In anticipation of the increase, an inpatient and home hospice provider collaborated with a hospital’s palliative medicine department in 2014 to establish a home-based palliative care programme to support families and their domestic helpers in their care of people with advanced dementia at home (Hum et al., 2018, 2019). Domestic helpers provide informal live-in paid help and are often women without formal care qualifications from neighbouring developing countries such as the Philippines, Indonesia and Myanmar who are employed to assist with physical caregiving (Woo et al., 2017). Available 24 hours a day, seven days a week, this programme involves a multidisciplinary team that works closely with the inpatient hospice unit and collaborating hospital (refer to Appendix 1 for details of the care model). Although the programme has demonstrated health and health system benefits (Hum et al., 2019; Pereira et al., 2020), anecdotal evidence suggested that not all individuals were able to die at the place of their choosing. Identifying factors associated with place of death and its concordance with preferences could lead to recommendations to improve the care model and inform policies and practices.
In helping to understand the potential predictors, a recent systematic review with meta-analysis was used as a guide. In the review, 10 individual, illness-related and environmental factors were identified as determinants of place of death for people with advanced dementia (Tay et al., 2024). Being younger, male, from an ethnic minority, having pneumonia, chronic obstructive pulmonary disease (COPD), and city living were associated with dying in hospital, while worse functional status, cancer, and capitation-based funding were associated with long-term care setting death (Tay et al., 2024). Being married was associated with dying at home or in hospital as opposed to long-term care (Tay et al., 2024).
Although place of death is a widely used and recognised international end-of-life care quality indicator (Bhadelia et al., 2022), this indicator has been criticised for providing information of severely limited utility as it gives no indication of the individual’s care quality or dying experience (Hoare et al., 2024). Examining where individuals receive care for a period before death – final place of care – may provide greater insights into the care received over the end-of-life trajectory (Sun et al., 2020). However, studies examining this relatively novel concept in advanced dementia are limited at present, including how the period should be defined.
In addition, to achieve person-centred care, it is important for what actually happened to concord with preferences. Despite the increasing recognition of goal-concordance as an important end-of-life quality indicator (Finkelstein et al., 2022), evidence is nascent (Badrakalimuthu & Barclay, 2014; Tay et al., 2024). The limited studies examining preferences in people with advanced dementia found being in receipt of home hospice, functional impairment and comfort goals of care to be associated with dying at the preferred location, while having a cancer comorbidity and the wish for full resuscitation predicted non-concordance (Badrakalimuthu & Barclay, 2014; Shega et al., 2008; Wiggins et al., 2019). As advanced dementia prevalence rises exponentially with global population ageing, identifying factors affecting final place of care and its concordance with preferences is imperative. The results could inform policies and practices for progressing the global public health goal of facilitating people with advanced dementia not just to die but to spend their final days at the place of their choosing.
Aim
To identify factors affecting final place of care and goal-concordance in people with advanced dementia receiving home-based palliative care in Singapore.
Methods
Study Design and Ethics
This was a retrospective cohort study using secondary data analysis. A theory-informed conceptual model classifying place of death determinants into three categories - individual, illness-related and environmental - was used to underpin the study (Gomes & Higginson, 2006) (Appendix 2). This model was informed by health research theories, such as the ecological theory of health behaviour, and refined based on a systematic review of 58 quantitative studies examining place of death mainly in people with cancer. Though not dementia-specific, the model’s use is not restricted by diagnosis, with applications in studies of people with different life-limiting conditions or chronic diseases (Costa et al., 2016; Harding et al., 2018; Tan et al., 2019).
Ethics approval was obtained from the Singapore National Healthcare Group (DSRB reference number: 2022/00782) and the authors’ affiliated University Research Ethics Committees (FHM-2023-3564-ExRev-1). The requirement for informed consent was waived as only routinely collected data of deceased individuals were used, and in previous analyses evaluating the effectiveness and cost-effectiveness of the programme, consent to collect data was already in place.
Setting and Study Population
Individuals consecutively enrolled in the service, from October 2014 to September 2017, who had died by 31/3/2020 (before COVID-19), were included in the study. Service enrolment criteria included being at Functional Assessment Staging Test (FAST) Stage 7 (i.e., having severe dementia) (Sclan & Reisberg, 1992), and feeding via an enteral tube, or having a serum albumin level <35 g/L (a biological marker indicating inflammation which is a risk factor for malnutrition) or pneumonia in the past year (Alvarez-Fernández et al., 2005). These mortality risk factors of community-based people with advanced dementia appropriately identify only people with less than one-year prognosis for palliative care. In addition, only home-dwelling individuals were eligible for the service (Hum et al., 2018, 2019).
Individuals enrolled from October 2017 to December 2019, when co-payment was trialled by the health ministry were excluded to prevent selection bias as home-based palliative care in Singapore has traditionally been and is at present fully subsidised (Jones & Rice, 2011). The study cohort was also restricted to before COVID-19; the significant impact of public health measures on service integrity and healthcare institution visitation policies that could potentially affect the outcomes were atypical of the usual health and social care contexts (Government of Singapore, 2023).
In addition, as the outcome was not just place of death, but where individuals received care for a period before death, individuals had to be at the place of death for minimally three days to be eligible for study inclusion. As this period is not well-defined in literature at present, three days was chosen based on stakeholder engagement and a study examining the minimum window period for quality end-of-life care to be delivered (Wright et al., 2016); the high frequency of end-of-life care setting transitions (Hanratty et al., 2014; Leniz et al., 2019) could result in the exclusion of too many individuals from the study if an unnecessarily long duration was defined. Individuals discharged to other services or not deceased by 31/3/2020 were excluded as the outcomes were unknown.
Data Source and Collection
All the data required were extracted from the service’s electronic medical records which included administrative and clinical data routinely collected during healthcare professionals’ phone contacts or home visits (Hanratty et al., 2008; Saunders et al., 2015).
Independent Variables
As indicated earlier, independent variables to be collected were informed by a systematic review of place of death determinants in advanced dementia (Tay et al., 2024), as well as stakeholder engagement to incorporate relevance to the Singapore context and data availability (Gilbert, 2008). The variables were classified according to the three categories of the conceptual model used to guide this study (Gomes & Higginson, 2006).
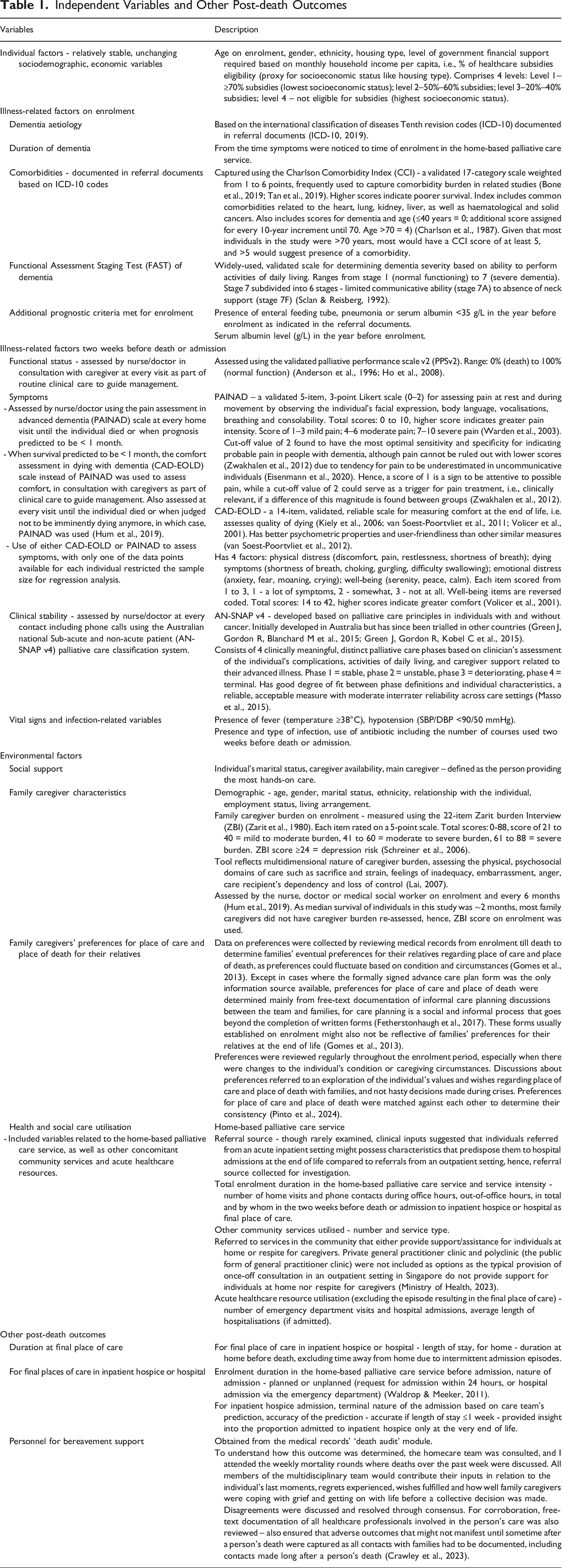
Independent Variables and Other Post-death Outcomes
Outcomes
The primary outcome was the final place of care (defined as last three days of care) – i.e., home, inpatient hospice or hospital. Pairwise comparisons of these settings were performed to facilitate comparison with a systematic review (Tay et al., 2024), and for corroboration of results (Wooldridge, 2012).
The secondary outcome was goal-concordance – a binary variable indicating preferences achieved (concordance) or not achieved (non-concordance). As an indicator encompassing both the place of care and death, goal-concordance was only considered achieved when the final place of care matched the preferences for both. As the number of undecided/undiscussed preferences for place of death was small (n = 3), their preferences were considered as not achieved and grouped with the non-concordant group for analysis. This was on the assumption that families who were not ready to discuss care plans or were undecided were likely to want aggressive treatment, which was found to be associated with non-concordance (Wiggins et al., 2019). Moreover, as meeting preferences made based on pragmatic considerations may not be a true reflection of end-of-life care quality (Smith et al., 2024), goal-concordance was defined as the final place of care matching what individuals and/or families would have wanted. This was determined based on discussions exploring the individual’s values and wishes between the homecare team and families during home visits, recorded as free-text in the electronic medical records, and not hasty decisions made during crises. This mitigated the insufficiency of examining goal-concordance without examining preferences per se (Smith et al., 2024).
Other post-death outcomes collected are described in Table 1.
Data Analysis
Data were summarised using descriptive statistics. Due to non-normal data distribution (assessed using the Kolmogorov-Smirnov test), non-parametric tests were used for comparing continuous variables between groups (Kruskal-Wallis for final place of care, Mann Whitney U for goal-concordance) (Pallant, 2013). Chi-square test was used for comparing categorical variables (Pallant, 2013). The Kappa measure of agreement was used to determine the degree of consistency in preferences for place of care and place of death and their concordance with final place of care (Landis & Koch, 1977).
Independent variables which differed at p < .1 in the between-group comparisons were shortlisted for multivariate regression analysis (MacNeil Vroomen et al., 2015). The usual p-value – p < .05 – for determining statistical significance was not used, as the objective was to shortlist variables for further analysis and not to determine the variables associated with the outcomes yet. Using an overly stringent criterion at the initial stage of variable selection could result in omitted variable bias in subsequent regression analysis which would affect validity (Wooldridge, 2012). After shortlisting, highly correlated and/or conceptually similar variables were excluded based on sample size and statistical strength considerations, as well as the indicator’s breadth and accuracy in reflecting the variable, to ensure the independence of variable for regression analysis (Wooldridge, 2012). Tests of multicollinearity were then performed to confirm the absence of multiple high correlations among the selected variables (Neergaard et al., 2019). To reduce the risk of Type 1 error due to multiple comparisons among the three final places of care (Bowling, 2014), post hoc univariate regression analyses were performed prior to multivariate analysis to identify the variables that were significantly different at p < .1 for each pair of final places of care. Again, p < .05 was not used to mitigate the risk of omitted variable bias.
All shortlisted variables were then entered simultaneously for multivariate binomial logistic regression analysis to evaluate the unique effect each variable had on the outcome that was over and above that offered by the other variables at the same time (Pallant, 2013). Model performance was assessed using predictive accuracy, R-square value and the Hosmer-Lemeshow goodness-of-fit test (Hosmer Jr. et al., 2013).
Sensitivity Analyses and Missing Data
As individuals with less than two-week survival after enrolment had a shorter look-back period for the service intensity indicators, and more acute healthcare resources could be utilised with a longer enrolment duration, correlation analyses were performed to check the strengths of the relationships. The effects of enrolment duration were also controlled in multivariate analysis, with sensitivity analyses performed to determine its exclusion’s impact on the results.
As there were minimal missing data, they were not replaced/imputed (Allison, 2002; Shrive et al., 2006). For variables with greater proportion of missing data that were not significant in regression analysis, they were excluded from the model to increase the sample size available for regression, with sensitivity analysis performed to determine the impact of their exclusion on the results.
A sensitivity post hoc power analysis was also performed to determine if the sample size obtained had 80% power to detect a clinically relevant effect size at 5% level of significance, using a formula for calculating the sample size needed for binary outcomes with effect size expressed as odds ratio (Suresh & Chandrashekara, 2012) (refer to Appendix 9 footnote for details of the formula).
All statistical analyses were performed using SPSS (version 25.0, IBM Corporation, New York). All tests were two-tailed with statistical significance defined as p < .05.
Results
From October 2014 to September 2017, 390 individuals were enrolled into the service. After excluding those who did not fulfil study eligibility criteria, 284 individuals were included for analysis (Appendix 3).
Background Characteristics
The median age of the 284 individuals was 88 (IQR 84-94) years; 66.9% were females. The majority were Chinese, lived in public housing, and required financial support.
Many were quite advanced in their disease trajectory on enrolment - half were at the most severe FAST 7E stage (Sclan & Reisberg, 1992), 75.3% met >1 prognostic enrolment criterion. The median duration of living with dementia was 6 (IQR 4-9) years; mixed dementia was the most common. Comorbidities such as stroke, diabetes, and moderate-severe chronic kidney disease were prevalent, with a median comorbidity score of 8 (IQR 7-10).
Two weeks before death or admission, most were confused/drowsy, experienced some pain (Mdn PAINAD 1 IQR 0-3) or discomfort (Mdn CAD-EOLD 38 IQR 35-40), and were in the terminal phase. Infection, especially pneumonia was also prevalent. Most were treated with antibiotics with a median of 1 (IQR 0-1) course administered.
Given the advanced age, most were widowed, with the majority of family caregivers being children. Family caregivers had a median age of 59 (IQR 53-64.5) years; 65.8% were females, 58.5% were married, and 72.5% lived with their relatives with advanced dementia. Although most had informal caregiving support from domestic helpers, caregiver burden was mild-moderate (Mdn ZBI 25 IQR 15-36), predisposing them to risk of depression (Schreiner et al., 2006). Despite being still of statutory working age (Ministry of Manpower, 2024), more than a third were not in paid employment.
The higher than usual service intensity in the two weeks before death or admission reflected the high care needs during this period. Although most were enrolled in the service for about two months with few acute healthcare resources utilised, a median of 2 (IQR 1-4) home visits and 5 (IQR 3-8) phone calls made in the two weeks indicated one contact made every other day. More than half also utilised other community services concomitantly (Appendix 4).
Outcomes
Comparison of Background Characteristics and Outcomes Among the Three Final Places of Care - Variables With p < .1
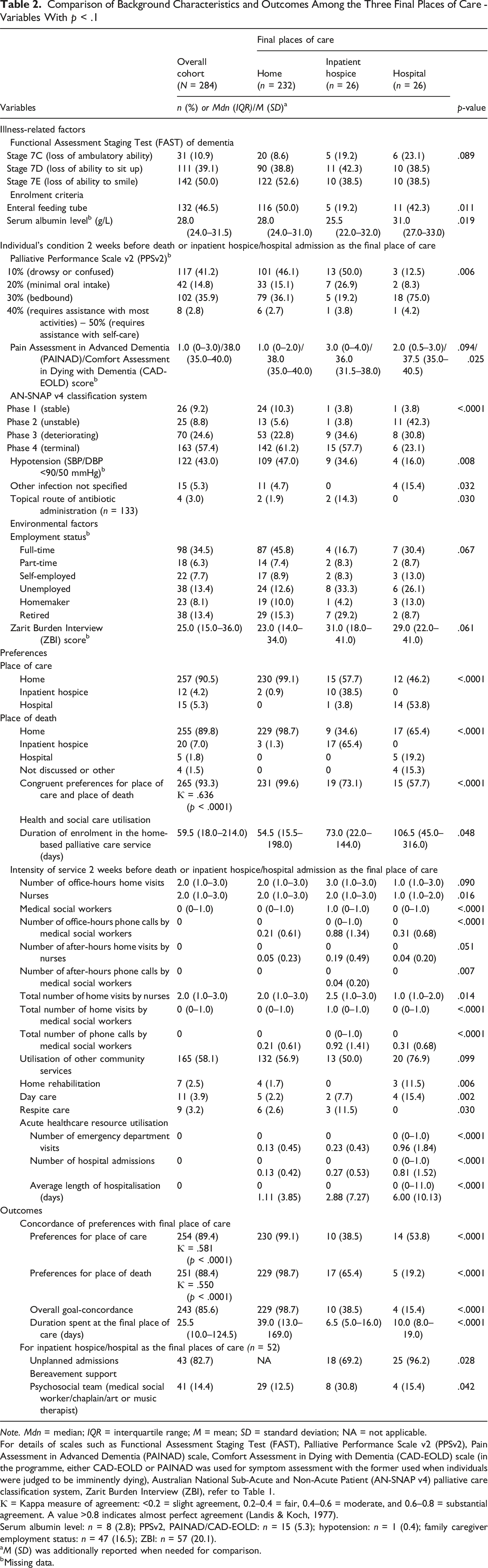
Note. Mdn = median; IQR = interquartile range; M = mean; SD = standard deviation; NA = not applicable.
For details of scales such as Functional Assessment Staging Test (FAST), Palliative Performance Scale v2 (PPSv2), Pain Assessment in Advanced Dementia (PAINAD) scale, Comfort Assessment in Dying with Dementia (CAD-EOLD) scale (in the programme, either CAD-EOLD or PAINAD was used for symptom assessment with the former used when individuals were judged to be imminently dying), Australian National Sub-Acute and Non-Acute Patient (AN-SNAP v4) palliative care classification system, Zarit Burden Interview (ZBI), refer to Table 1.
Ƙ = Kappa measure of agreement: <0.2 = slight agreement, 0.2–0.4 = fair, 0.4–0.6 = moderate, and 0.6–0.8 = substantial agreement. A value >0.8 indicates almost perfect agreement (Landis & Koch, 1977).
Serum albumin level: n = 8 (2.8); PPSv2, PAINAD/CAD-EOLD: n = 15 (5.3); hypotension: n = 1 (0.4); family caregiver employment status: n = 47 (16.5); ZBI: n = 57 (20.1).
aM (SD) was additionally reported when needed for comparison.
bMissing data.
Comparison Between Individuals Who Achieved and did Not Achieve Goal-Concordance – Variables With p < .1
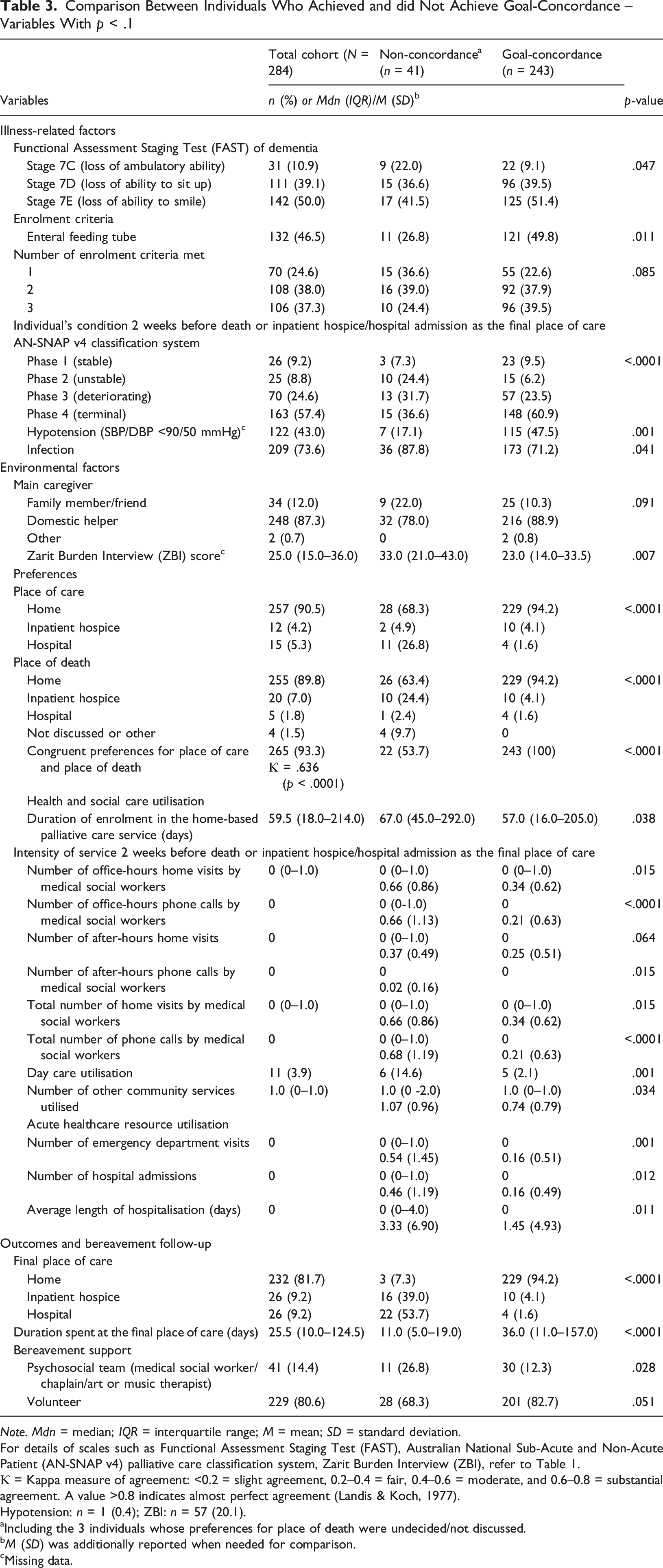
Note. Mdn = median; IQR = interquartile range; M = mean; SD = standard deviation.
For details of scales such as Functional Assessment Staging Test (FAST), Australian National Sub-Acute and Non-Acute Patient (AN-SNAP v4) palliative care classification system, Zarit Burden Interview (ZBI), refer to Table 1.
Ƙ = Kappa measure of agreement: <0.2 = slight agreement, 0.2–0.4 = fair, 0.4–0.6 = moderate, and 0.6–0.8 = substantial agreement. A value >0.8 indicates almost perfect agreement (Landis & Koch, 1977).
Hypotension: n = 1 (0.4); ZBI: n = 57 (20.1).
aIncluding the 3 individuals whose preferences for place of death were undecided/not discussed.
bM (SD) was additionally reported when needed for comparison.
cMissing data.
Comparison Between Groups
When all the independent variables were compared between groups, no individual factors were significantly different at p < .1 for both outcomes (Appendix 4 for final place of care; Appendix 5 for goal-concordance). Variables that were significant are in Tables 2 and 3. After excluding conceptually similar or highly correlated variables and those with small numbers, 15 illness-related and environmental factors were shortlisted for post hoc univariate (Appendix 6) and multivariate regression analyses. No multicollinearity was detected.
Multivariate Analyses
Only results of the final regression models are presented here. Models before sensitivity analyses are in Appendices 7 and 8. Model performance was assessed to be adequate.
Hospital versus Home
Multivariate Analyses of Factors
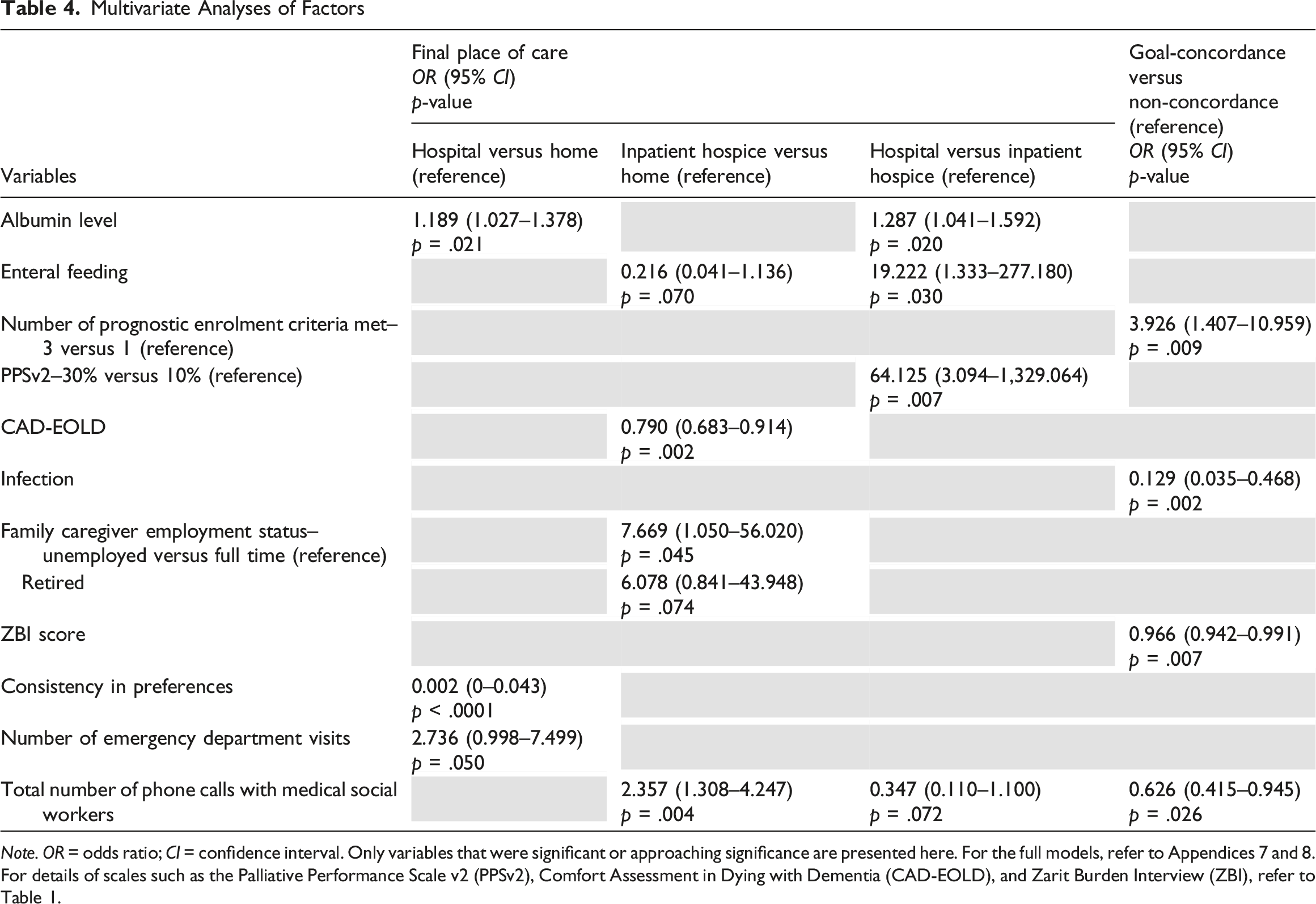
Note. OR = odds ratio; CI = confidence interval. Only variables that were significant or approaching significance are presented here. For the full models, refer to Appendices 7 and 8.
For details of scales such as the Palliative Performance Scale v2 (PPSv2), Comfort Assessment in Dying with Dementia (CAD-EOLD), and Zarit Burden Interview (ZBI), refer to Table 1.
Inpatient Hospice versus Home
Greater discomfort with lower CAD-EOLD scores (OR 0.790 95% CI 0.683–0.914), more phone contacts with medical social workers (OR 2.357 95% CI 1.308–4.247), and unemployed family caregivers predisposed one to inpatient hospice admission for care at the end of life (OR 7.669 95% CI 1.050–56.020). Though only approaching significance, the same directions of associations were observed for oral feeding (OR 0.216 95% CI 0.041–1.136), and retired family caregivers (OR 6.078 95% CI 0.841–43.948) (Table 4).
Hospital versus Inpatient Hospice
The results corroborated with the above comparisons to home. Individuals with higher serum albumin levels (OR 1.287 95% CI 1.041–1.592), and better functional status with PPSv2 30% compared to 10%, were more likely to be admitted to hospital for care (OR 64.125 95% CI 3.094–1,329.064). Oral feeding (OR 19.222 95% CI 1.333–277.180), and more phone contacts with medical social workers similarly predisposed one to inpatient hospice admission (OR 0.347 95% CI 0.110–1.100), although the latter’s effects were only approaching significance (Table 4).
Goal-Concordance versus Non-concordance
Poorer prognosis with all three enrolment criteria met (compared to one) predicted goal-concordance (OR 3.926 95% CI 1.407–10.959), while an infection episode two weeks before death or admission (OR 0.129 95% CI 0.035–0.468), higher family caregiver burden with higher ZBI score (OR 0.966 95% CI 0.942–0.991), and more phone contacts with medical social workers were associated with non-concordance (OR 0.626 95% CI 0.415–0.945) (Table 4).
Sensitivity Analyses
Sensitivity correlation analyses confirmed the absence of any strong positive relationships between enrolment duration and service intensity two weeks before death or admission, and with acute healthcare resource utilisation. Removing enrolment duration from the regression models did not change the direction and strengths of associations significantly. Notwithstanding the reduction in effect sizes for some variables, removing non-significant variables including those with high missing data from the models increased the estimates’ precision and statistical significance of some variables without affecting model performance. Post hoc sensitivity power analyses also confirmed that the sample size obtained was able to detect clinically-relevant odds ratios that had medium to large effect sizes for all the outcomes (Appendix 9).
Discussion
In this retrospective cohort study of people with advanced dementia receiving home-based palliative care in Singapore, most were at home for care for at least three days before death. An equal but small number were admitted to the inpatient hospice or hospital for care in their final days. Better biological and functional status, inconsistent preferences for place of care and place of death, as well as possibly more emergency department visits (effects approaching significance) predisposed individuals to hospital admission. Discomfort, oral feeding, more phone contacts with medical social workers, unemployed and possibly retired families predicted inpatient hospice admission for care. Although goal-concordance with preferences was high overall, the rates were lower for the inpatient hospice and hospital groups. Better prognosis, an infection episode two weeks before death/admission, higher family caregiver burden, and more phone contacts with medical social workers predicted non-concordance.
The factors associated with hospital as final place of care, and the associations of better prognosis and infection with non-concordance, exemplified the impact of the condition’s unpredictable trajectory on end-of-life care and death for people with advanced dementia (Lewis et al., 2023). With better health/physical status, families may perceive their relatives still to have a reasonable quality of life and prognosis, with infections viewed as being potentially amenable to treatment in hospital, especially if previous hospital interventions have been “successful” (Moore et al., 2017). The intention of an admission may have been for care/treatment, and not to die there. However, the diminished/limited reserves of people in the advanced stages of dementia could mean individuals may succumb unexpectedly/unpredictably to the infection (Murray et al., 2005), and not be discharged in time to die at the place of choice (Smith et al., 2024). Conversely, by recognising/acknowledging the limitations of hospital care at the advanced stages of the illness, and having a consistent, clear direction/focus or preference for home, home care and death could be facilitated (Mogan et al., 2018; Wiggins et al., 2019).
In addition, the results highlight the multifaceted, profound care challenges that people with advanced dementia and their caregivers face at the end of life, and the condition’s uncertain, protracted trajectory (Lewis et al., 2023). Symptom control, oral feeding, and psychosocial challenges such as family caregiver burden/stress, requiring medical social workers’ support, could make sustaining care at home difficult (Chiao et al., 2015; Lysaght Hurley et al., 2014; Malhotra et al., 2021). With a prolonged trajectory, this could take a significant physical, psychosocial, and financial toll on family caregivers, particularly those who gave up work or retired early to become a caregiver (Brodaty & Donkin, 2009; Woo et al., 2017), thereby necessitating inpatient hospice admission for care (Lysaght Hurley et al., 2014). Despite facing profound challenges, admissions to inpatient hospice were often late and unplanned, suggesting a preference for care at home until death was imminent. This could possibly be due to societal norms and cultural beliefs such as filial piety (Gao et al., 2024; Lien Foundation, 2014), which imbues children with the responsibility of caring for their elderly parents, particularly for the Chinese ethnic majority (Chan et al., 2019). The preference for care at home for as long as possible, with the admission viewed as dignifying if the person was not cognisant of it anymore by the time it happened has also been reported in international literature (Gomes et al., 2013; James et al., 2023). The results demonstrated that this could have potential psychosocial consequences post-death. A greater proportion of families whose relatives were admitted to inpatient hospice for care required professional psychosocial bereavement support, consistent with the findings of a systematic review examining bereavement outcomes in family caregivers of people with dementia (Crawley et al., 2023).
Compared to factors affecting place of death for people with advanced dementia (Tay et al., 2024), relatively unchanging individual sociodemographic (age, gender, ethnicity), and long-standing, chronic comorbidities (cancer, COPD) had no effect on final place of care and its concordance with preferences. Conversely, dynamically changing variables such as symptoms and caregiving challenges with the potential to disrupt the dying process did. This could be because death was viewed as not just an event but as a process with a period of time (three days) needed to assess the outcome (final place of care) (Krikorian et al., 2020). This has implications for the convention of using place of death as an end-of-life quality indicator that views death simply as an event; important modifiable risk factors that are more amenable than stable factors to interventions could be missed.
Informed by the results, a final place of care model for people with advanced dementia, which was adapted from the conceptual model introduced in the Methods section that was used to guide this study was developed (Gomes & Higginson, 2006). This new model highlights final place of care as a novel, distinct concept from place of death, albeit with some overlaps. In addition, illness-related factors in the original model could be split into relatively stable and dynamically changing factors, which form the overarching categories for the new model. In the context of advanced dementia, chronic comorbidities can also be relatively unchanging, in addition to individual factors. Factors associated with goal-concordance are also incorporated in the new model (Figure 1). Final Place of Care Conceptual Model for People With Advanced Dementia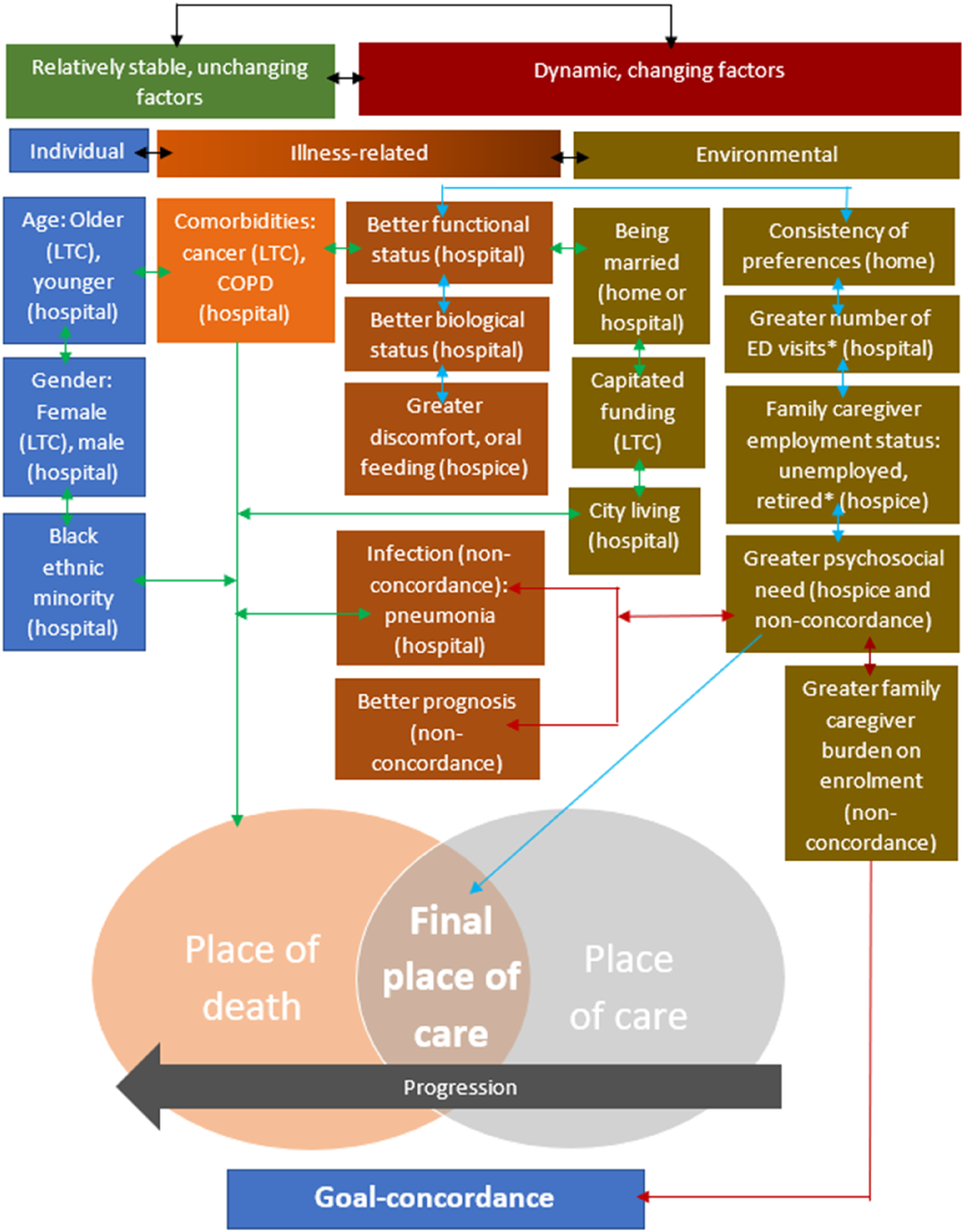
Implications for Practice and Policy
The unpredictable, protracted trajectory of dementia highlights the need for early, regular review of care plans and education of families about the condition’s trajectory as well as care that would be appropriate at the advanced stage. Otherwise, the inconsistency in preferences could result in individuals dying in hospital, which may not be concordant with their wishes. Predictors of final place of care that are available on enrolment could help healthcare professionals to identify individuals who prefer a comfort-directed approach to care but have difficulty remaining at home for care early. Psychosocial support helping families explore and accept alternative options for final place of care can then be provided, with inpatient hospice admissions planned and facilitated in a timelier manner before care quality and/or caregivers’ well-being are compromised.
To help families cope with the multifaceted end-of-life care challenges in advanced dementia at home, more caregiving, psychosocial and financial support are required, if both home care and home death is preferred. Alongside caregiver training on safe feeding techniques (van der Steen et al., 2014), psychosocial support could be provided to help families cope with the distress of not being able to feed their relatives orally - food being emblematic of care, concern and love in Asia (Ho et al., 2022) - and to embrace other ways of caring. As difficulty swallowing could also affect medication administration for symptom control (Wernli et al., 2022), empowering caregivers with skills/knowledge to administer medications via alternative routes to ensure comfort at the end of life is essential for sustaining care at home until death (Malhotra et al., 2021). In addition, policies catering to the condition’s unpredictable, protracted trajectory such as increasing the accessibility and affordability of home-based end-of-life caregiving services (Browne et al., 2021; Lewis et al., 2023), and recognising family caregiver as a social identity with their opportunity costs lost, compensated through financial incentives could be useful. These measures could potentially alleviate the significant physical, psychosocial, financial strains and stigma that families who give up work/retire early to care, face (Brodaty & Donkin, 2009; Woo et al., 2017). Even though most have domestic helpers, these initiatives could serve as additional layers of support for family caregivers who have decision-making, care coordination and management roles as well (Yuan et al., 2022).
Strengths and Limitations
This was the first study to examine the final place of care concept for people with advanced dementia. The fresh, clinically relevant insights into factors affecting care at the end of life contribute to knowledge and inform practices/policies. The final place of care model (developed from refining an existing model) could be externally validated in the general advanced dementia population and for underpinning future relevant studies. In addition, infrequently examined variables such as consistency in preferences were investigated. The use of eventual preferences and not those established on enrolment addressed previous studies’ limitations (Guerriere et al., 2015; Prioleau et al., 2016).
There were, however, a few limitations. Causation cannot be established from associations (Bowling, 2014; Wooldridge, 2012); consequently, caution is needed when considering the results’ implications for policies/practices. Additionally, the specific, temporal context and predominantly Chinese cohort limited generalisability/applicability (Bowling, 2014). Although restricting the study cohort to individuals enrolled before charging was implemented mitigated selection bias, individuals enrolled before implementation but chose to remain with the programme could also have been an able, willing-to-pay select group (Jones & Rice, 2011). Sensitivity analysis to determine their inclusion’s impact on the results could not be performed due to reidentification concerns by the Singapore ethics board with admission and death dates collected. However, the small number was unlikely to affect representativeness significantly.
The use of secondary data (medical records) not designed with the research objectives in mind could also affect data integrity and quality (completeness, accuracy), as healthcare professionals have their preconceptions and judgements of what was relevant/required to be documented (Saunders et al., 2015). Variables that could be examined were also limited by data availability, potentially resulting in omitted variable bias (Wooldridge, 2012). Reviewing free-text records to determine quantitative variables such as preferences without a second reviewer for inter-rater check could also introduce subjectivity/bias (Bowling, 2014). To mitigate this limitation, stakeholders were engaged, and different healthcare professionals’ records were reviewed for corroboration. Reflexivity was also exercised to challenge assumptions and biases (Tashakkori & Teddlie, 2010).
Although the small inpatient hospice/hospital sample sizes relative to the number of variables entered for regression analyses resulted in imprecise estimates with large confidence intervals (Wooldridge, 2012), the sample size obtained had sufficient power to detect medium to large effect sizes for all the outcomes in sensitivity analyses (Sullivan & Feinn, 2012). Lastly, the quantitative study design limited the examination of variables to their strengths of associations (Bowling, 2014). Further qualitative research exploring the context and nuanced decision-making processes underpinning end-of-life care choices is needed (Gomes et al., 2013).
Conclusion
The results highlighted the implications of people with advanced dementia’s unpredictable, protracted trajectory on end-of-life care and death. Despite the specific context, the results supported by international literature still have global applicability. As a concept distinct from place of death, these fresh perspectives contribute to knowledge, with the final place of care model developed having the potential to be used in future research. The results could also inform the policies and practices for addressing the multifaceted care challenges at the end of life. Early, regular education and review of the disease trajectory and care plans, as well as greater caregiving, psychosocial and financial support, could enhance the integrated ecosystem of care for individuals with advanced dementia and their families to be better supported in the dying process. These results could advance the prominent global public health goal of facilitating people with advanced dementia not just to die, but to spend their final days at the place of their choosing without compromising on care quality and family caregivers’ well-being. Place of death is important, but the final place of life should be equally so.
Supplemental Material
Supplemental Material - Predictors of Final Place of Care in People With Advanced Dementia Receiving Home-Based Palliative Care in Singapore: A Multivariate Regression Analysis
Supplemental Material for Predictors of Final Place of Care in People With Advanced Dementia Receiving Home-Based Palliative Care in Singapore: A Multivariate Regression Analysis by RiYin Tay, Allyn YinMei Hum, Mervyn YongHwang Koh, Jane Simpson, and Nancy Preston in Dementia.
Footnotes
Acknowledgements
The authors would like to thank the practitioners who gave their feedback, as well as individuals enrolled in the programme and their family caregivers - their data made this study possible.
Ethics Considerations
Ethics approval was obtained from the Singapore National Healthcare Group (DSRB reference number: 2022/00782) and Lancaster University Research Ethics Committees (FHM-2023-3564-ExRev-1).
Consent to Participate
The requirement for informed consent was waived as only routinely collected data of deceased individuals were used, and in previous analyses, consent to collect data was already in place. Contacting families just to obtain informed consent for this additional analysis was impracticable and ethically inappropriate.
Author Contributions
RYT, AYMH, JS, and NP conceptualised and designed the study, RYT acquired the data, RYT, JS, and NP analysed and interpreted the data, and RYT drafted the article. All authors revised the article critically for important intellectual context, and gave their final approval of the version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was done in partial fulfilment of the first author’s PhD study in Palliative Care at Lancaster University. Her studies are funded by Dover Park Hospice and The Palliative Care Centre for Excellence in Research and Education (PalC). The sponsors had no role in the design, execution, data collection, analysis and interpretation, or writing and preparation of the paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Request for data can be made to the corresponding author, which will be considered on a case-by-case basis.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.