
Abstract
Keywords
Introduction
More than half a million people worldwide have been diagnosed with dementia (World Health Organisation, 2024a). It is estimated that over 11 million Americans (Alzheimer’s Association, 2023) and between 34,200 and 137,600 Australians (Australian Institute of Health and Welfare, 2023) are providing informal care for people living with dementia. Informal carers are people who provide unpaid care for their family members or friends on a regular basis (Carers Australia, 2024). Informal carers are an integral part of the health care system as they enable care recipients to continue living in their community (Carers Australia, 2024).
Informal carers of people with dementia face a variety of challenges not least due to the inevitable decline in the care recipient’s functional, cognitive, and emotional status (Kim et al., 2021) and disrupted sleep (Smyth et al., 2020). The provision and complexity of care significantly depends on the care recipient’s physical functions, mental health, end-of-life health, advanced age or disability (Australian Institute of Health and Welfare, 2023). In addition to declining health, there may also be acute events or illnesses including falls (Ang et al., 2020). It has been recognised that informal carers may face financial challenges, as the continuous demands of caregiving could prevent them from engaging in paid work (Australian Institute of Health and Welfare, 2023), creating a significant financial impact and preventing them from engaging in social activities that can in turn, lead to social isolation (Brown et al., 2017). Informal carers have less availability or time for family or work pursuits (Brown et al., 2016), which can negatively affect their quality of life, the quality of care they provide, relationships with the care recipient, and personal independence (Farina et al., 2017).
Informal carers of people with dementia are reported to experience significantly higher levels of stress which impact on their well-being than those who care for people who do not have cognitive impairment, and can present with severe psychological and physical symptoms (Feast et al., 2016; Gilhooly et al., 2016). Psychological well-being is defined as the state of wellbeing that the individual has the capacity to realise his/her own abilities, able to cope with the everyday life stressors, can contribute to the community while working productively and fruitfully (World Health Organisation, 2005). Increasing the wellbeing of informal carers could improve provision of care to older adults with dementia and delay early admission to nursing homes or admission to hospital (Vandepitte et al., 2016). The perspectives of informal carers of people with dementia are important to enhance their positive experience of caregiving and improve wellbeing (Lindeza et al., 2024).
Mindfulness-based interventions (MBI) have been shown to enhance the psychological health of a range of populations including university students, healthcare workers and patients (Gal et al., 2021; Jayawardene et al., 2017; Sommers-Spijkerman et al., 2021; Witarto et al., 2022; Zhang et al., 2020). However, adherence and retention in MBI programs have been shown to be poor due to the intensity of the program and need to participate in training. Recent studies have explored online delivery methods of MBI including smart phone applications (Torous et al., 2020), and other web-based interventions (Yadav et al., 2022), but have also identified similar challenges as in-person MBI programs. A range of enablers and barriers that informal carers experience when participating in online MBI, have been identified in a mixed-method systematic review (Abeysinghe Mudiyanselage et al., 2024). While online delivery is suggested as a better option due to the flexibility and accessibility of the programs, additional strategies are required to better support informal carers to enhance uptake and reduce drop-out rates (Abeysinghe Mudiyanselage et al., 2024).
The use of a co-design approach is the optimal method for developing an online MBI that is fit for purpose, promotes and retains participant engagement and importantly engages end-users to inform the planning and designing of the intervention (Slattery et al., 2020). Co-design is defined as a process of joint inquiry and imagination where diverse stakeholders share and combine their knowledge to improve service delivery (Steen, 2013; Steen et al., 2011). Empowering participants with lived experience and stakeholders to engage in the development of programs aimed for end users, enabling programs to be tailored to address their specific needs (Santana et al., 2018).
This paper describes a study that is part of a larger study to develop and implement an online mindfulness-based intervention program for informal carers of older people with dementia. This component of the study aimed to collaborate with the co-designers in the modification and design of the online mindfulness program: “Mindful Practice for Family Carers of People with Dementia Program” (MiPCaP).
Methods
Ethical Approval
The Edith Cowan University Human Research Ethics Committee approved this study (2022-03416-ABEYSIGNHE MUDIYANSELAGE). The chief investigator submitted the project proposal explaining the purpose of the study, risks, and benefits of obtaining the research approval. No personal identifiers were collected or identified in the focus group/one-to-one interview transcripts to preserve anonymity and confidentiality. Informed consent was obtained directly from all participants and was provided in written format.
Study Design
A qualitative interpretive descriptive approach was used for this component of the project in order to gain an in-depth understanding (Schneider et al., 2016) of the co-designers’ experiences of MiPCaP, grounded in their experiences as experts in the field. Interpretive descriptive methodology was developed from a combination of ethnography, grounded theory and phenomenology (Thorne, 2016), and is widely used in the health care arena. An interpretive approach within the constructive paradigm relies more on pure description of participants’ experiences including constructing stories, observation in their natural context, rather than being reliant on theory, in order to provide a comprehensive summary of events (Schneider et al., 2016).
The nature of interpretive descriptive studies is aligned with this study in various ways. Interpretive descriptive studies are conducted in the participants’ natural setting that are comfortable and ethically aligned for research participants (Thorne, 2016). The method also clearly acknowledges the value of subjective and experiential knowledge as one of the fundamental sources (Thorne, 2016). Interpretive descriptive methodology focuses on shared human experience as well as individual differences within the shared focus of interest (Thorne, 2016). Socially constructed elements to human experiences are also acknowledged, naturally embedded and cannot be meaningfully separated (Thorne, 2016). The interpretive descriptive approach also recognises that human experience is based on multiple constructed realities which may be opposing at times (Thorne, 2016). Interpretive descriptive approaches acknowledge an inseparable interaction between the researcher and participant that influences the research outcomes (Thorne, 2016) while providing a theoretically flexible approach to analyse data.
Development of MiPCaP
A co-design approach was used in the development of the MiPCaP, as it is imperative to collaboratively work with the end users to develop any interventions aimed at them; otherwise, interventions might not meet their actual needs and preferences (Allemann et al., 2023). The success of any program also is dependent on attrition rate, recruitment and participant engagement. Co-designing has been successful in increasing the engagement of informal carers in the development of mHealth applications (Rathnayake et al., 2021), supportive online resources (Perera et al., 2021), and carer readiness tools (White et al., 2021). The co-design approaches can be varied depending on the intervention, consumers and stakeholders. For this study, the co-design approach described by Steen (2013) was followed.
The co-design approach included a three stage process: (1) exploring and defining the problem, (2) perceiving the problem and conserving possible solutions, and (3) trying out and evaluating solutions (Steen, 2013). Firstly, relevant literature was systematically reviewed to inform potential solutions, to barriers of online MBI (Abeysinghe Mudiyanselage et al., 2024). The findings from this review were incorporated as a component of the development of the MiPCaP. The program consisted of an online platform, workbook, and audio recordings. We also adapted mindfulness activities from the workbook “RELAX The Mindful Way” by the Southwestern Sydney Local Health District (SWSLHD) Carers Program (South Western Sydney Local Health District, 2018), to better tailor the program to the Australian context. A dedicated Facebook page was created to house the program which comprised recordings of mindfulness activities, a chat function to enable participants to connect with each other during the program and promote social interaction with the potential to reduce social isolation. After obtaining consent to participate, information about the MiPCaP was emailed to potential members of the co-designers. The co-designers were asked to review the content of the MiPCaP which included the program booklet, recordings and the Facebook page, and provide their feedback during the interviews. Data were collected through one-to-one virtual interviews and a virtual focus group. Finally, MiPCaP was updated based on the co-designers feedback and recruitment of informal carers of people with dementia to undertake MiPCaP is underway. The tailored approach to co-design used to design MiPCaP is depicted in Figure 1. Tailored Approach to Co-design Used to Develop MiPCaP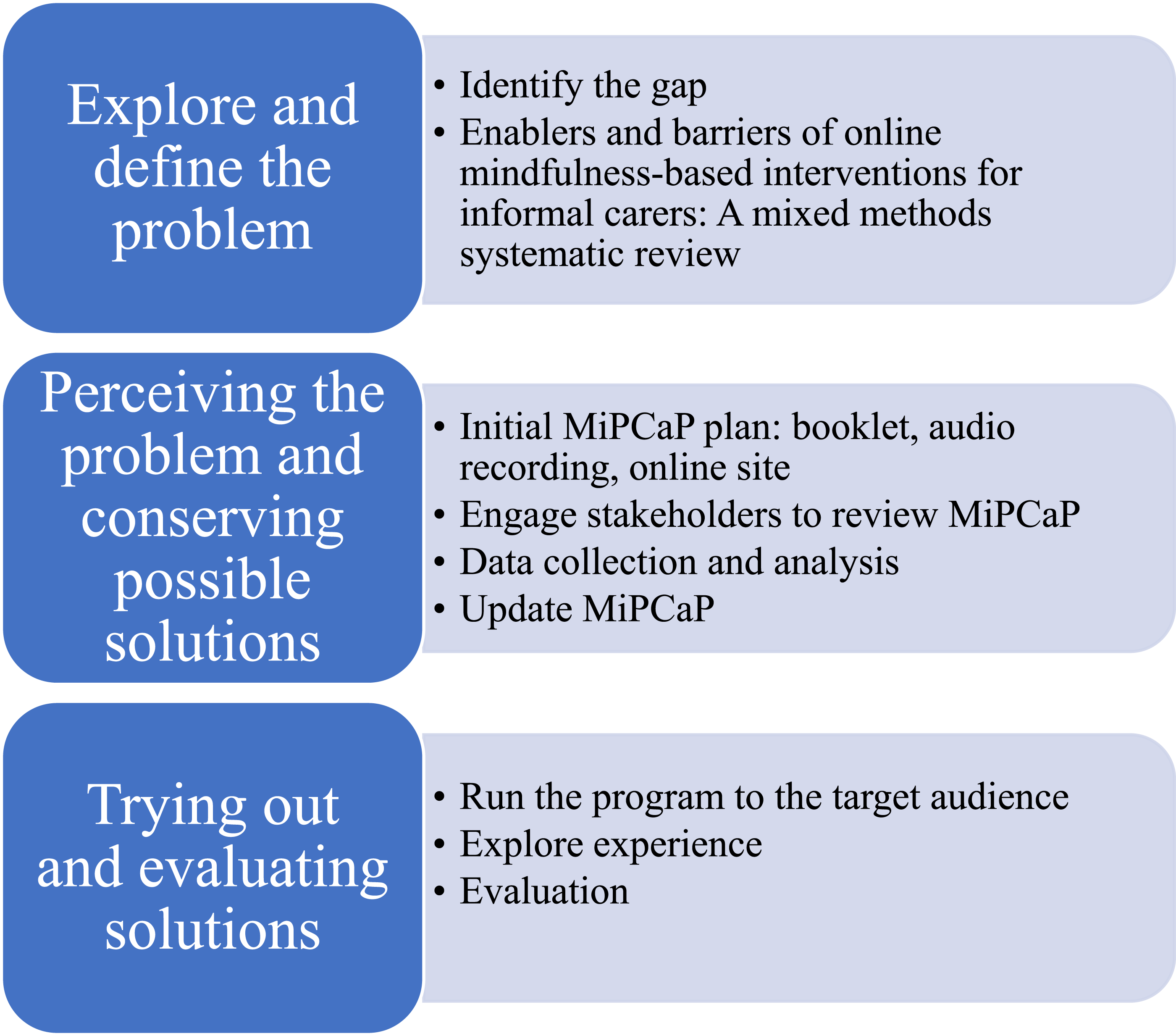
Sample and Setting
Purposive sampling was used to recruit the members of the co-designers (Figure 3). The co-designers were recruited from: the university’s staff wellbeing program, and snowballing from both the participants’ and researchers’ networks. The setting was within each participant’s natural setting, providing them with convenience, comfort and flexibility to complete the study, which in turn allowed the researcher to gather rich and thick data (Schneider et al., 2016).
Data Collection
Data were collected by the researcher via a focus group or one-to-one interviews. Initially, a virtual focus group was planned to enable participants to discuss and expand on each other’s ideas, and to arrive at a collective understanding about the program. However, not all participants were able to attend the focus group, so one-to-one virtual semi-structured interviews were conducted for those who were not able to attend. Both the focus group and one-to-one interviews were conducted using Microsoft Teams. All interviews were guided by a semi-structured interview guide (Appendix 2) which was developed by the researcher based on the recommendations of Galletta and Cross (2013), audio recorded, and transcribed verbatim.
The researcher ensured that the interview questions were aligned with the purpose of the research to explore the co-designers experiences to further develop and refine MiPCaP. The research team considered the arrangement of the questions to progress towards an in-depth exploration of the phenomena. For example, questions were planned to explore the ideas of overall program delivery. The interviews consisted of three segments. In the first segment, a level of comfort was established by explaining the research purpose, participants’ rights, and a mutual understanding of the process. Then, broad questions were utilised to create openings for participants to speak about their experiences related to MiPCaP. In the middle segment of the interview, researchers moved into more specific information related to the research questions focused on the booklet, recordings and Facebook page and looped back to participants’ descriptions of their experiences, which merged into the main focus of the research. The researcher also used probing questions to gain more information related to the research topic, including questions which explored navigation of the Facebook site and their thoughts on the chat forum. In the last segment of the interview, questions were asked in relation to theoretical considerations, offering participants the opportunity to explore opening narratives in relation to the research objectives of exploring the co-designers experience of MiPCaP and identifying barriers and enablers. The researcher also found opportunities to create a culturally safe environment for all participants. Then, the researcher concluded the interview by thanking the participants and emphasising their contribution to the research.
The focus group schedule was based on recommendations from Krueger and Casey (2015). First, all participants were welcomed, the researcher shared the purpose of the focus group, ground rules, and approximate duration; participants were given the opportunity to introduce themselves. The focus group commenced with an open question about the program booklet, and each participant was then given the opportunity to share. Whilst the researcher asked the questions according to the semi-structured interview guide (Appendix 2), sometimes the discussion revealed answers that prompted another question. For example, when asked about the program booklet, the navigation of the Facebook page was raised. After giving some time to discuss the navigation of the Facebook page, the moderator brought the topic back to the booklet to focus more on the booklet’s content and structure. Participants were encouraged to express different points of view, and the moderator used ‘pause and probe’ techniques to draw additional information such as pausing for a few seconds and asking how they experienced it. The chief investigator recorded notes and memos during and after the focus group to record relevant data. Participants were invited to ask questions at the end of the focus group interview and asked about suggestions for future program implementation.
Data Analysis
As cited by Krippendorff (2018), content analysis is a research method that enables the creation of replicable and valid inferences from data to their context to provide knowledge, new insights, a representation of facts, and a practical guide to action (Elo & Kyngas, 2008). In inductive content analysis, categories are derived from the data, whereas in deductive content analysis, previous knowledge guides the data categorisation to check the theory (Elo & Kyngas, 2008). Inductive content analysis process which was described by Elo and Kyngas (2008) was selected for this study based on the research purpose of exploring feedback from the co-designers in the adaptation of an online mindfulness program called MiPCaP.
Inductive content analysis includes open coding, creating categories and abstraction (Elo & Kyngas, 2008). During the open coding process, the research team read and re-read the transcriptions, highlighting and creating headings in the margins to describe all aspects of the content. For example, in one transcript, training the mind, providing examples, and nature of the mind were written in the margin as they appeared as headings. Following this, the headings were collected from the coding sheets and categories generated freely. The category of “provide guidance to enhance practice” was created after collecting all the similar headings. To create categories to describe the phenomena, similar categories were grouped under higher order headings. For example, “may incorporate formal practice beyond the program” and “provide guidance to enhance practice” were grouped under the higher-order heading of providing support beyond the program. Lastly, for abstraction, general descriptions of the topic were formulated through generating categories and naming content-characteristic words. For example, support for participants was created considering the “recognition of participants’ roles, promoting self-care and acceptance through mindfulness, accounting for participants’ limitations, developing a virtual social support network and providing support beyond the program”. The data analysis process is represented in Figure 2. Example of the Abstraction Process
Trustworthiness
Trustworthiness of this study was established in several ways by following Lincoln and Guba (1985)’s definition of trustworthiness. To ensure credibility, the first author participated in weekly debriefing sessions with her supervision team; used thick verbatim descriptions to support the findings; and maintained accurate record keeping. To ensure dependability, every step, including participant recruitment, was described in detail in the results section of this study. Peer debriefing, as well as a declaration of the chief investigator’s beliefs and assumptions were applied during the data analysis process in order to increase confirmability. To ensure transferability, the researcher provided thick descriptive data with direct quotes for readers to be able to evaluate the applicability of the findings to other settings. The researcher also provided a clear and transparent processes that were undertaken during the of co-design of the MiPCaP. To protect authenticity, the researchers included descriptions of participant experiences, while at the same time protecting participant privacy, in order to provide readers with further knowledge and context about the participants’ lives.
Results
The co-designers comprised six members, three of whom were interviewed and three who participated in the focus group and shared their experiences of MiPCaP. Characteristics of the co-designers are detailed in Figure 3. Pseudonyms were used to protect participants’ identity and their cultural background (Wang et al., 2024). Participant Characteristics Table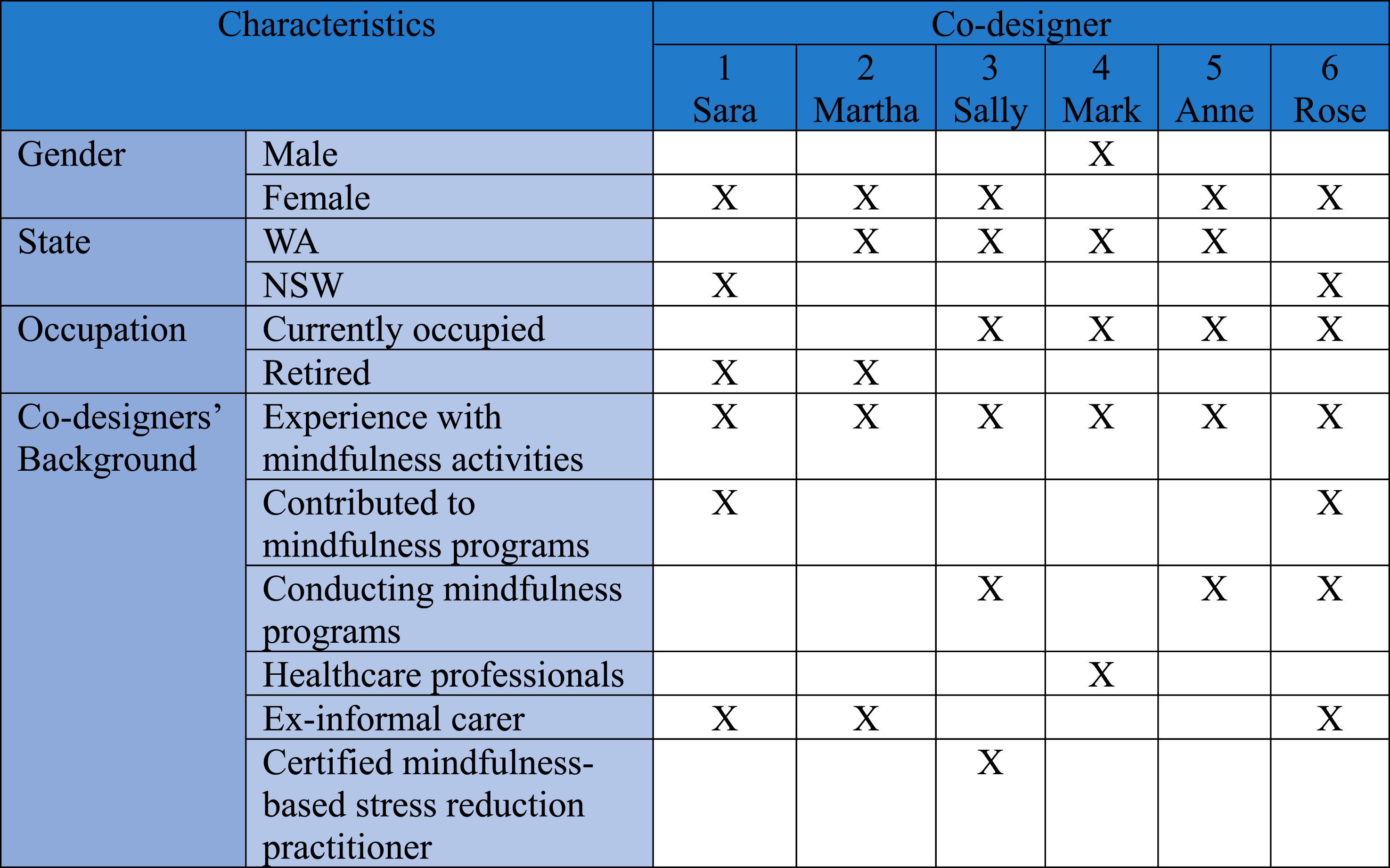
Two main categories were formulated (Appendix 1): support for participants and program delivery and content.
Support for Participants
For support for participants, there were five sub-categories: recognition of participants’ roles, promoting self-care and acceptance through mindfulness, accounting for participants’ limitations, developing a virtual social support network and providing support beyond the program.
Recognition of Program Participants’ Roles
The co-designers recommended providing recognition for the informal carers’ roles by acknowledging their contribution to the care and considering potential challenges they might face when participating in MiPCaP. The Co-designers recognised the contribution made by informal carers of people with dementia and suggested acknowledging them. “You are devoting part of your life to a big job. Caring is a big job. So let's be honest with it and say that and accept that's good you're doing something really good and it's recognised. It's a nice experience” (Rose).
Another suggestion was to recognise challenges faced by informal carers of people with dementia with time limitations, where “The first thing that comes to mind when it comes to carers, particularly with people with dementia, which can be many years. That people say, oh my God, I don't have time to go do anything new. I don't want to learn. I don't want this, I already have too much to do” (Rose).
Promoting Self-Care and Acceptance through Mindfulness
Co-designers suggested incorporating loving kindness as an activity and emphasising the importance of the reflection section. Most co-designers suggested that the reflection section was important: “I like these reflections that you got here. Not everybody would do it, but I think it's good to reflect on how you feel after a while doing it. And also, what was the challenge, and now, like, what stopped you from doing it?” (Rose).
The co-designers also emphasised the importance of adding loving kindness as an activity as it provides space to self-care and acknowledge the informal carers of people with dementia feelings to promote others’ wellbeing: “Unless we treat ourselves with love and compassion, we cannot reflect the same on others. Once we begin to experience self -love and self-compassion for ourselves, we can extend the same to others too” (Martha).
Account for Participants’ Limitations
The co-designers recommended considering participants’ limitations, including physical and caregiving needs, by giving clear instructions, providing larger and less complex images to colour, improving the quality of recordings, and reducing the content within the useful resources section. The co-designers appraised the clear instructions, where one noted its practicality and easy to understand nature while Anne stated, “I really liked the way that they were. The instructions went step by step. I thought they were really easy to follow.”
Including larger and simpler pictures and the process of colouring were suggested, considering participant health issues that could limit their ability to move their hands freely or due to their impaired vision. Sara expressed her experience with colouring: “I do the colouring. I still do it, but you need, especially as you get older with reduced eyesight, you actually need a bigger picture. You need to see the lines and you need the space to do it.”
Co-designers shared their view about the recording and the importance of high-quality recording in considering the target population, noting: “...could not hear very well. I had it. I couldn't try to adjust” and “I felt like you were too far away from the microphone… I think just letting it flow a little bit better” (Anne).
They also emphasised the importance of the flow and reducing pauses. Beyond suggestions by members of the importance of quality recording, they also discussed reducing the useful resource section, in particular to “cut it down to like one mindfulness link just the best one” (Mark) and shrinking the information.
Developing a Virtual Social Support Network
The co-designers discussed the importance of developing a virtual social support network as online access connects the participants and can form a supporting community. Anne suggested the chat forum as a supportive system, noting: “it’s good for those people to feel like they have a community because the community is so important for the carer and for the person who's going through who’s participating”.
Some co-designers identified the online forum to be an ideal way to improve connection, as informal carers of people with dementia might be at risk of social isolation, whereby: “it might be good for them to connect. Might be good for them to share...to help people strengthen the concept and also to encourage them to continue” (Rose, x-informal carer).
Providing Support Beyond the Program
The co-designers discussed the importance of providing support beyond the program by incorporating informal practice beyond the program and providing guidance to enhance practice. The co-designers talked about integrating mindfulness beyond the program during daily activities as it becomes more practical, noting: “Choose a daily activity where you could do every day as you walk to the car, as you put your clothes on, as you clean your teeth” (Sally).
The co-designers also emphasise providing guidance to enhance practice. The expert panel suggested starting with an activity that “will be easy” to do without extra effort. Acknowledgment of a wandering mind was also described by the co-designers, where it was noted to be: “in fact, very normal, to lose focus during practice. The mind is distractible by default, and part of the benefit of mindfulness is actually about refocusing and training our attention.” (Mark)
Gradually training the mind was emphasised, considering aspects of human nature, where they suggested the strategy in response was, “what you do is without getting annoyed or upset, you gently bring it back to being aware again, present moment” (Martha).
Further to this, the structural approach for commencement was highlighted, after which “people will eventually adjust it to them to their own way of doing it” (Rose). It was acknowledged that informal carers of people with dementia might feel tired during mindful activities and fall asleep, where it was suggested, “if they want to, they can have a little short nap” (Martha, x-informal carer).
Co-designers also emphasised the importance of daily practice for success, noting “because we have never done this before, you tend to say oh no, I'll do it later and you don't continue. But if you persist at the beginning… then your mind also will go along with it…”(Martha).
Program Delivery and Content
Three sub-categories emerged related to the delivery method: tailor the program to the practical needs of the participants, provide options for program delivery and ensure a culturally safe program.
Tailor the Program to the Practical Needs of the Participants
The co-designers recommended tailoring the program to the practical needs of the participants ensuring easy access and navigation, limiting the duration of each activity, continually emphasising the benefits of mindfulness and including distress protocol. The co-designers appraised the easy access of the platform and its information, “making it as easy as possible for the carers and the participants to actually access that” (Mark).
Further, it was suggested that having a maximum 10 minutes of duration for each activity was appropriate due to caregiving demands. Co-designers also agreed that the MiPCaP was consistent with mainstream mindfulness programs. Emphasising the benefits of mindfulness was discussed to encourage participants to continue practising mindfulness, as mindfulness is a freely available empowering tool, “This should be something that feels enjoyable and free to. It should be like a safety point for me where I can go when there is nowhere else to go” (Rose).
Co-designers also discussed mindfulness helping to understand the nature of the mind, “It can also support us to better understand the nature of the mind and the nature of emotions and the nature of the interaction between the mind, the body, thoughts, reactions, all of those kinds of things” (Sally).
The co-designers expressed how mindfulness was advantageous for informal carers of people with dementia as these carers face unique problems including repetitive questioning and behavioural challenges, where they noted “it might be useful to actually include how mindfulness might actually even help somebody who is caring for somebody to dementia” (Mark).
Beyond discussing the continual emphasis on the benefits of mindfulness, the co-designers also discussed the importance of including a protocol for managing distress. Mark emphasised having a protocol to direct participants, “if they do start saying quite distressing things that there might kind of disclose thoughts of suicide”.
Co-designers also suggested to screen participants for their vulnerability, considering “a person with a trauma history or other mental health vulnerabilities needs to have additional specialised support if they undertake a program involving meditation” (Sally).
Co-designers further suggested the “acknowledgement of the potential difficulties, depending on the vulnerability of the person coming in” (Sally). Co-designers also spoke about the normal concept, “the problem with our world is that we are never taught about our emotions” (Rose).
Further, they discussed how emotions often go unacknowledged and often people do not know how to deal with it, “We go to school and we learn so many different skills, but we don't learn the management of emotions and life will bring you so much that” (Rose).
In addition, co-designers talked about importance of acknowledging our emotions, whereby “they could definitely acknowledge, like if they're feeling angry and things like that” (Rose). Co-designers reflected and applied their expertise by suggesting the normalisation of emotions, noting “I’d definitely put something around normalising the range of emotions that carers will have and acknowledging. That this is a normal human reaction to the stresses of being in that situation” (Sally).
Provide Options for Program Delivery
The co-designers discussed providing options for program delivery including choices of platform and incorporating diverse presentation of content. The co-designers raised concerns with Facebook and technology, noting that: “some of them are not registered with Facebook or use technology that way. I think you need to give them options. Some people will be comfortable with that, so that's an option. But other people might not be comfortable with that, so they need the booklet” (Sara, x-informal carer).
Co-designers also suggested to incorporate diverse presentation of content, but noted that “this is the kind of the tricky part cause…some like music, some don't like music, some prefer a male voice, others like a female voice…The kind of best way of giving those options but not overwhelming people with too many options” (Mark).
Ensure a Culturally Safe Program
The co-designers emphasised cultural safety, including the culturally safe approach, compelling introduction and reducing useful resources. The culturally safe approach was a code that emerged, where co-designers expressed their experience working with clients from different cultures and how culture shaped their lives and actions. Further, they were also curious to phrase loving kindness in a different way due to cultural consideration. Co-designers also emphasise the importance of a compelling introduction welcoming all cultures. Mark stated, “The introduction could be a little more compelling and relatable, perhaps by including a fictional story of a carer or just mentioning the real stressors carers experience and the impact on them”.
Discussion
The aim of this study was to explore the experiences of co-designers to seek their feedback in modifying MiPCaP. Six co-designers reviewed MiPCaP. In our study, the co-designers suggested tailoring the program to the practical needs of the participants considering flexibility of delivery, as well as potential impairments of participants such as impaired vision and hearing and health conditions including arthritis. Previous studies also identified flexibility as an enabler to participate, as participants were able to access the program whenever they wanted using smartphones, computers or tablets (Stjernsward & Hansson, 2020). The co-designers also suggested to consider potential impairments of participants such as impaired vision and hearing and health conditions including arthritis when tailoring the program to their practical needs. They suggested to include bigger and less complex pictures to colour and including clear voice recording. Health-related issues are equally important to consider when planning programs which may include older adult populations, as certain health conditions including hearing loss, cataracts, and osteoarthritis are common in aging (World Health Organisation, 2024b). It is therefore important to identify factors that predict attrition for successful future program developments (Steele et al., 2007). Additionally, it is equally important to protect participants’ rights by giving them options and choices while including everyone regardless of their disability and health issues.
Aligning with the co-designers suggestions in this study, previous studies have also highlighted the importance of a protocol for managing distress (Britton et al., 2021; Stjernsward & Hansson, 2018, 2020; Taylor et al., 2022). A systematic review identified commonly reported distress as mental and somatic distress (Taylor et al., 2022), whilst another study identified MBI practices as associated with transient distress, mild to severe depression and persistently high levels of negative effects (Britton et al., 2021). Thus it is important to inform participants to seek help immediately if they experience any discomfort (Stjernsward & Hansson, 2018, 2020). Facilitators also need to be well equipped to identify potentially vulnerable participants and monitoring them to maximise the safety and efficacy of the MBI (Stjernsward & Hansson, 2018, 2020). The creation of clear protocols for managing distress and a strategic approach, are vital to ensure safe collaboration of participants with online MBI (Taylor et al., 2022).
One of the suggestions from this study’s co-designers was to include loving kindness as an activity considering the nature of dementia, including repetitive questioning and behavioural challenges, which can be frustrating for informal carers. Loving kindness can be defined as a mental state of unselfish and unconditional kindness to all beings (Hopkins, 2001), involving sending feelings of kindness and care to oneself, loved ones, strangers and all beings (Petrovic et al., 2024). Loving kindness and compassion are generally overlapping concepts (Gilbert & Choden, 2013), where it has been documented that people who are high in self-compassion treat themselves with kindness when they are in stressful life situations (Allen & Leary, 2010). Several systematic reviews and meta-analyses have identified loving kindness and compassion-based interventions to be beneficial when facing negative life events (Galante et al., 2014; Gu et al., 2022; Petrovic et al., 2024), where both interventions are also associate with reducing caregiver burden in the long-term (Hofmann et al., 2011). Both interventions can also be used as an alternative strategy for reducing stress and easing empathic distress (Watson et al., 2023). Therefore, introducing loving kindness to informal carers can help to reduce caregiver burden and improve psychological wellbeing.
Together with the study’s co-designers suggestions, it is important to develop culturally responsive interventions (Hall et al., 2016) to overcome the barriers of applicability, replicability and generalisability (Roll et al., 2019). A recent systematic review conducted by McDermott et al. (2024) suggested that high-quality culturally adapted interventions are yet to be developed for marginal people, including refugees and asylum seekers. Interventions can be adapted considering the end users’ preferred language, personal values, simplifying the method to achieve goals and including culturally relevant materials, concepts and goals (Bernal & Saez-Santiago, 2006). It is also imperative to consider end users’ social, economic, and political context and knowledge, values, customs and traditions of cultural context (Bernal & Saez-Santiago, 2006). For example, certain types of interventions may be less effective for Asian cultures than Western cultures, such as the intervention developed focusing individual perspective, focusing on the goals of promoting positivity and self-enhancement (Ng & Ong, 2022). Researchers can implement culturally accepted interventions, where for example, Eastern culture is inherently more aligned to acceptance of negative emotions and experiences (Ng & Ong, 2022).
Our co-designers suggested considering potential challenges and providing guidance to enhance participation. It is well-documented that informal carers have poor engagement and higher attrition rates participating in in-person and online programs (Hartley et al., 2022; Joshi et al., 2023). A study that was conducted to evaluate the feasibility of a self-guided mindfulness app for family carers and individuals with autism, had difficulty finding participants to complete the program (Hartley et al., 2022). One qualitative study identified the reasons and motivations for carers of people with dementia including moral, religious, and spiritual aspects (Zahed et al., 2019). These carers in particular require greater incentives to participate in research (Joshi et al., 2023). As in this study, retention rates can be enhanced by integrating a theoretical framework such as the Theoretical Domain Framework (TDF), which comprises 12 key constructs relevant to changing the behaviour of consumers (Michie et al., 2005). Understanding key constructs in behaviour change processes is imperative for successful program implementation. Health professionals have widely used the TDF and have investigated this for further applications and key developments of interventions and programs (Francis et al., 2012; Phillips et al., 2015; Sarmast et al., 2014). It is suggested to incorporate TDF when planning and implementing interventions for informal carers.
Adherence to a program can also be a challenge, as shown in previous studies, where informal carers had difficulty adhering to training schedules (Hudson et al., 2020; Stjernsward & Hansson, 2018, 2020). This could include not having enough time to complete the program due to competing caregiving responsibilities and priorities (Hudson et al., 2020), trouble remembering the training schedule and creating a routine (Hudson et al., 2020) and viewing unable to participation as a personal failure (Stjernsward & Hansson, 2020). In our previous systematic review, we identified that program structure and delivery could both positively and negatively relate to barriers and enablers of online mindfulness-based interventions of informal carers (Abeysinghe Mudiyanselage et al., 2024). Lack of self-motivation and external factors preventing participation can be interrelated and act as barriers while self-motivation and positive experience of mindfulness can act as enablers of participating in online mindfulness-based interventions (Abeysinghe Mudiyanselage et al., 2024). Therefore, well planned strategies are crucial for attracting participants and ensuring the program is ‘fit for purpose’ ensures a higher retention rate, such as creating an online community with similar experiences, sending reminders for participants who are willing to receive weekly reminders, creating a flexible program schedule and being available to help participants who have challenges connecting in online program.
It is well documented that co-designing creates positive outcomes for a project (Slattery et al., 2020; Talevski et al., 2023), even if the process is complex, as it involves several interactions: researchers, software developers, users including people with lived experiences and expertise (Thabrew et al., 2018). These interactions provide equal opportunity for end users to collaboratively participate in program design, minimising the power imbalance between designers and the end users (Iniesto et al., 2022), empowering the end users for sharing their lived experiences (Martinez Escobedo et al., 2024). One study designed self-compassion interventions with a co-design approach for family carers of people with dementia to prioritise their perspectives and lived experiences and highlighted the value of incorporating end-user experience to development of interventions (Murfield et al., 2022). Previous studies have incorporated co-design to improve program structures and the development of online interventions for informal cares of colorectal cancer patients, where these studies had only 20% and 29% attrition rates respectively (Atreya et al., 2018; Dragomanovich et al., 2021). Therefore, co-designing online MBI may increase informal carers adherence with a program as most potential causes for dropout rate are already being addressed when attracting participants.
Strengths and Limitations
Those who participated in the co-designers shared their view of MiPCaP and contributed to the adaptation and further extension of the program. However, the study had many strengths, including diversity of co-designers, their expertise and lived experience. Further, connecting with participants virtually allowed them to participate in the interview at a convenient location and time. We also adapted commonly used mindfulness activities to the program ensuring previously tested, simple and easy activities. We utilised an authenticated co-design approach to refine and re-develop the MiPCaP and considered all potential barriers to further enhancing MiPCaP’s usability. Our study also highlighted the importance of recognising participants’ challenges, limitation and cultural awareness to enhance program retention. Findings also revealed the importance of a user-friendly online platform for increasing participant retention.
There were some limitations to our study. This was a small sample of participants, and we only included participants from within Australia. We also only included English-speaking participants and co-designers only had past experience of informal caring. Despite some limitations to this study, we gathered rich and meaningful data and analysed these in alignment with the methodology. The chief investigator has significant experience with caring for people with dementia, and as such, she regularly discussed her perceptions and assumptions with the supervisory panel to avoid any potential bias.
Conclusion
Our study highlights potential strategies and challenges for online mindfulness programs. We followed a co-design approach to engage end-users in the adaptation and further extension of MiPCaP. Based on co-designers’ feedback for the provided materials, two main categories emerged: support for participants and program delivery and content. Those emerged categories were linked with previous findings and provided valuable feedback for future project implementation. Program developers should consider end-user feedback prior developing customer focus programs to better adapt programs to the community.
Supplemental Material
Supplemental Material - Co-design of an Online Mindfulness Program for Informal Carers of People Living With Dementia: A Qualitative Study of Co-designers’ Experience
Supplemental Material for Co-design of an Online Mindfulness Program for Informal Carers of People Living With Dementia: A Qualitative Study of Co-designers’ Experience by Charunya A. K. R. Abeysinghe Mudiyanselage, Beverley Ewens, Aisling Smyth, Joanne M. Dickson, and Seng Giap Marcus Ang in Dementia.
Footnotes
Acknowledgement
We would like to acknowledge the contribution and support of the South Western Sydney Local Health District (SWSLHD) Carers Program. We also extend our sincere thanks to the co-designers. We also thankful for Dr. Michael Stein of Edith Cowan University Higher Degree Research Communication Advisor, SOAR peer advisors of Edith Cowan University.
ORCID iDs
Ethical Approval
The Edith Cowan University Human Research Ethics Committee approved this study (2022-03416-ABEYSIGNHE MUDIYANSELAGE). The chief investigator submitted the project proposal explaining the purpose of the study, risks, and benefits of obtaining the research approval. No personal identifiers were collected or identified in the focus group/ one-to-one interview transcripts to preserve anonymity and confidentiality. Informed consent was obtained directly from all participants, and was provided in written format.
Funding
The author(s) received no financial support for the research, project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.