
Abstract
Despite an aging population and acknowledged importance of advance care planning (ACP) for persons living with cognitive impairment, few engage in ACP. Most existing tools to facilitate ACP discussions focus on medical outcomes, despite research documenting that persons with cognitive impairment often have quality of life outcomes as primary goals. A tool for ACP that incorporates a range of outcomes that are most important to persons with cognitive impairment and their carers is needed. This qualitative study engaged persons with mild cognitive impairment (MCI) or dementia and their carers to identify outcomes that are most important to inform development of a tool to guide ACP interventions with this population. We conducted interviews with 17 persons with MCI or dementia and 15 caregivers of persons with MCI or dementia. Interviews explored participants’ prior experiences with ACP and goals for care planning. Content analysis was used to generate a list of outcomes identified as most important to persons with MCI or dementia and their carers. The list of person-centered outcomes was refined/categorized by research team consensus. Most participants in the sample had not participated in a prior ACP conversation with a primary care provider. Participants identified 23 outcome categories for ACP interventions within the following six domains: social life, family involvement, current lifestyle, physical independence, financial independence and healthcare goals. Of the 23 outcome categories, the majority (86%) were quality of life goals and only a small fraction (14%) were healthcare specific. The outcomes identified as most important to persons with MCI or dementia and their caregivers can be used as a foundation for future work focused on developing an ACP tool to guide shared decision-making about healthcare. This tool can facilitate prioritization of goals that are most meaningful to persons with cognitive impairment and their carers as opposed to focusing only on medical aspects of care.
Introduction
Dementia is a leading cause of dependence and disability around the world and its prevalence is expected to increase given the rapidly aging population (Shin, 2022; World Health Organization (WHO), 2023). Approximately 7 million people age 65 and older are living with Alzheimer’s disease and other dementias in 2024, and the annual number of new cases of these dementias is expected to double by 2050 (Alzheimer's Association, 2024). The financial impact of Alzheimer’s Disease and Related Dementias on households and the economy is substantial (Bryant et al., 2019), with costs of caring for persons with dementia expected to reach $360 billion dollars in 2024 (Alzheimer’s Association, 2024). Advance care planning (ACP) is the process of making and communicating decisions about future care for circumstances in which patients are unable to express their wishes such as during medical crisis and end of life (Butler et al., 2014; Morrison et al., 2021). While ACP has been proposed as a solution to improve the quality of end-of-life care, with healthcare institutions being incentivized to document these discussions, a growing body of evidence suggests that ACP focused on end-of-life care has not achieved its intended goals (Morrison et al., 2021). The progressive course of dementia and inevitable impairment in participation in end-of-life conversations necessitate a call to action to re-evaluate ACP interventions for persons with cognitive impairment and their caregivers, particularly during the early stage of the disease (Clayton et al., 2024; Flaherty et al., 2025).
ACP discussions between persons with cognitive impairment and providers are not routinely taking place, (Poppe et al., 2013; Sampson et al., 2018; Schickedanz et al., 2009; Tetrault et al., 2022), with less than 40% of persons with cognitive impairment engaging in ACP (Sampson et al., 2018). Clinician barriers to ACP conversations have been well-documented and include personal discomfort, perceived time constraints, lack of knowledge about advance directives, and concerns that patients might not receive the conversations well (Bosisio et al., 2021; Flaherty et al., 2023; Morrison et al., 1994; Phenwan et al., 2020; Snyder et al., 2013; Tilburgs et al., 2018)). Tools have been developed to facilitate ACP discussions, yet most tools focus on medical outcomes, such as desire for cardiopulmonary resuscitation and intubation or hemodialysis, and do not consider quality of life, functioning, and other outcomes of care despite documented importance to patients (Hofmann et al., 1997; Jennings et al., 2017; McMahan et al., 2013; Poppe et al., 2013; Schickedanz et al., 2009; Wendrich-van Dael et al., 2020).
Decision aids such as video guides and images and dyadic interventions have helped persons with cognitive impairment in understanding the course of dementia and using that information for care planning (Einterz et al., 2014). However, these tools are outdated and none are standardized for use in routine practice. Additionally, technology has advanced at an unprecedented rate in the last decade. A shared-decision making web tool for persons with dementia and their caregivers has been developed in the Netherlands. However, the tool is in Dutch and the interface needs improvement for use by older adults with dementia (Span et al., 2015). A mixed-methods study in the U.S. guided the development of an end-of-life (EOL) planning tool called the Life-Planning in Early Alzheimer’s and Dementia (LEAD) guide for persons with dementia (Dassel et al., 2019). Limitations of this study include a small sample size comprised predominately of white, well-educated females. These factors suggest that both persons with mild cognitive impairment (MCI) or dementia and their caregivers and clinicians would benefit from a standardized approach to ACP that enables them to identify goals and outcomes of care that are most meaningful. Our work builds upon what is known about ACP conversations by providing specific guidance on topics to include in these discussions that are most important to persons living with cognitive impairment and their caregivers.
The purpose of this qualitative study is to understand the goals and outcomes that persons with MCI or dementia (referred to as persons living with cognitive impairment) and their caregivers identify as important to their healthcare to inform an ACP intervention that is most valuable to patients with dementia across all stages of the disease. Findings from this work can be used to inform development of an ACP intervention that focuses on both medical and broader life goals that more effectively engages patients with cognitive impairment and their caregivers in decision-making about care.
Methods
Design and Setting
We used a purposive sample to conduct semi-structured interviews via telephone with persons living with varying levels of cognitive impairment and carers of persons with cognitive impairment from August-November 2020. This research was approved by the Thomas Jefferson University Institutional Review Board.
Participants
Participants were identified through either a dementia registry, current enrollment in a study that screened for cognitive impairment, or by their primary care physicians (PCPs) as having cognitive impairment (PCPs at Thomas Jefferson University in Philadelphia, PA were asked to refer their potentially eligible patients). We included interested persons with MCI or dementia who were English speaking, above 18 years old, not currently taking antipsychotics, determined to have MCI or dementia, and able to provide informed consent, as assessed through answering teach-back questions as part of the informed consent process. We included all interested caregivers of patients with MCI or dementia who were English speaking, above 18 years old, and able to provide informed consent, including caregivers who cared for someone with dementia who had recently passed away. Recruitment letters were mailed to potential participants explaining the study with the ability to opt-out. We contacted persons with MCI or dementia and caregivers via telephone using the contact phone numbers listed in patient participants’ Electronic Medical Record (EMR). We attempted to contact 111 potential participants and ultimately engaged 25 participants in interviews (17 patients, 8 caregivers). Participants were excluded if they had a non-functioning number or did not pick up the telephone (n = 48), were unable to speak on the telephone (n = 11) or declined (n = 27). For those who agreed to participate in an interview, we obtained verbal consent, including use of teach-back questions to ensure capacity to consent. Recruitment continued until thematic saturation was reached (Boyatzis, 1998).
Data Collection
Interviews
We developed separate semi-structured interview guides for persons living with cognitive impairment and caregivers to explore prior experiences with and perceptions regarding ACP interventions, current goals and life values, and expectations for future care if health worsens. (Online Appendix A and B) Three trained research coordinators (NS, VJS, GA) conducted telephone interviews, with oversight from a researcher with extensive experience with qualitative methods (KLR). The average length of interviews was 48 minutes. Among participants, there was one patient-caregiver dyad with the rest being unrelated to each other. Interviews were audio-recorded, professionally transcribed, and de-identified We used the consolidated criteria for reporting qualitative studies (COREQ) checklist (Tong et al., 2007).
Measures
At the conclusion of the interviews, demographic characteristics were obtained via self-report, the PHQ-2 questionnaire was used to assess level of depression, and standardized tests of cognitive function were administered. First, we administered the Telephone Interview for Cognitive Status (TICS), which is a standardized objective test of cognitive functioning designed to be administered over the phone (Brandt et al., 1988). A question about the current president was omitted as data collection occurred during an election year. Therefore, scores on the TICS range from 0 to 39. Higher scores indicate better cognitive function, with 31 being the cut off for cognitive impairment and 27 or below consistent with dementia. Self-reported cognitive status was assessed with the Cognitive Function Instrument (CFI) (Li et al., 2017). Both the self-report and study partner report versions of the CFI were used for persons living with cognitive impairment and caregivers, respectively. Scores on this instrument range from 0 to 14, with higher scores indicating greater subjective cognitive complaints. TICS and CFI scores were used to describe the cognitive status of participants.
Data Analysis
We conducted conventional content analysis of interview transcripts to identify themes related to understanding participants’ prior experiences and perceptions of ACP interventions as well as goals for ACP planning (Hsieh & Shannon, 2005). The team first reviewed a subset of transcripts to develop an initial codebook for persons with cognitive impairment. Then two team members (VJS and GA) applied the codebook to a set of transcripts and reviewed coding with the team to inform revision of the codebook. This was done iteratively until a final codebook was established. The two coders applied the final codebook to all the transcripts, double coding a portion of the transcripts, with percent agreement and Kappa coefficient reviewed regularly. Reviewing the percentage agreement in conjunction with the Kappa coefficient is a commonly used practice to assess intercoder reliability of qualitative data. A mean kappa ranging from 0.61 to 0.80 is considered substantial intercoder agreement and this range was used as a guide for assessing sufficient intercoder agreement (Burla et al., 2008; Hemmler et al., 2020). An additional team member (ATG) met regularly with the coders to compare coding, resolve discrepancies, and refine the codebook as needed. After coding the transcripts of persons with cognitive impairment, a similar process was used for caregiver transcripts to identify themes and develop a codebook that could be applied to transcripts from caregivers.
As a primary objective of this work was to develop a list of person-centered goals related to care planning, the second stage of analysis was focused on extracting this list of goals from persons with cognitive impairment and caregiver transcripts. To do so, two team members reviewed all content in the “patient goals” code within both codebooks and individually extracted a list of specific person-centered goals. To ensure comprehensiveness of this list of goals, the team members then reread the entirety of all the transcripts to ensure that there were no missing goals in the list. After developing individual lists, they worked together to combine their lists into a master list, resolving language differences and combining similar goals.
The research team then went through a series of steps to collapse the comprehensive list of highly specific goals into a list of more general person-centered outcome categories. To do so, first the team worked together to create a preliminary list of person-centered outcomes that was representative across the full range of identified goals. Team members then tested this list of outcomes by independently categorizing each goal to one of the newly developed person-centered outcomes. For this exercise, each goal could only be assigned to one person-centered outcome, though multiple goals could be assigned to the same person-centered outcome. For example, person-centered goals such as ‘see granddaughter get married’, ‘stay healthy for future family events’, and ‘see a great-grandchild be born in the coming months’ were consolidated into the person-centered outcome ‘Be alive for important upcoming event (family or other).’ As necessary, each team member suggested a different person-centered outcome name or entirely new person-centered outcome categories to facilitate appropriate sorting. The entire team then reviewed all the categorized goals outcome lists together, specifically discussing: (1) wording of categories for person-centered outcomes and (2) decisions regarding the final sorting of goals to person-centered outcomes. Discrepancies were resolved with group consensus and a final draft list of person-centered outcomes for ACP was established. This process of goal extraction and sorting has been used by our team in prior work (Rising et al., 2021).
As a final check of data trustworthiness, a member of the research team (VJS) loaded the final list of person-centered outcomes into NVivo as a codebook and applied it to the “patient goals” node. Modifications were made by the team to the outcomes wording based on coding back to the original data. This ensured that the final list of person-centered outcomes was appropriately representative of the original participant language used.
Results
Participant Characteristics
Interview Participant Demographics (N = 25)
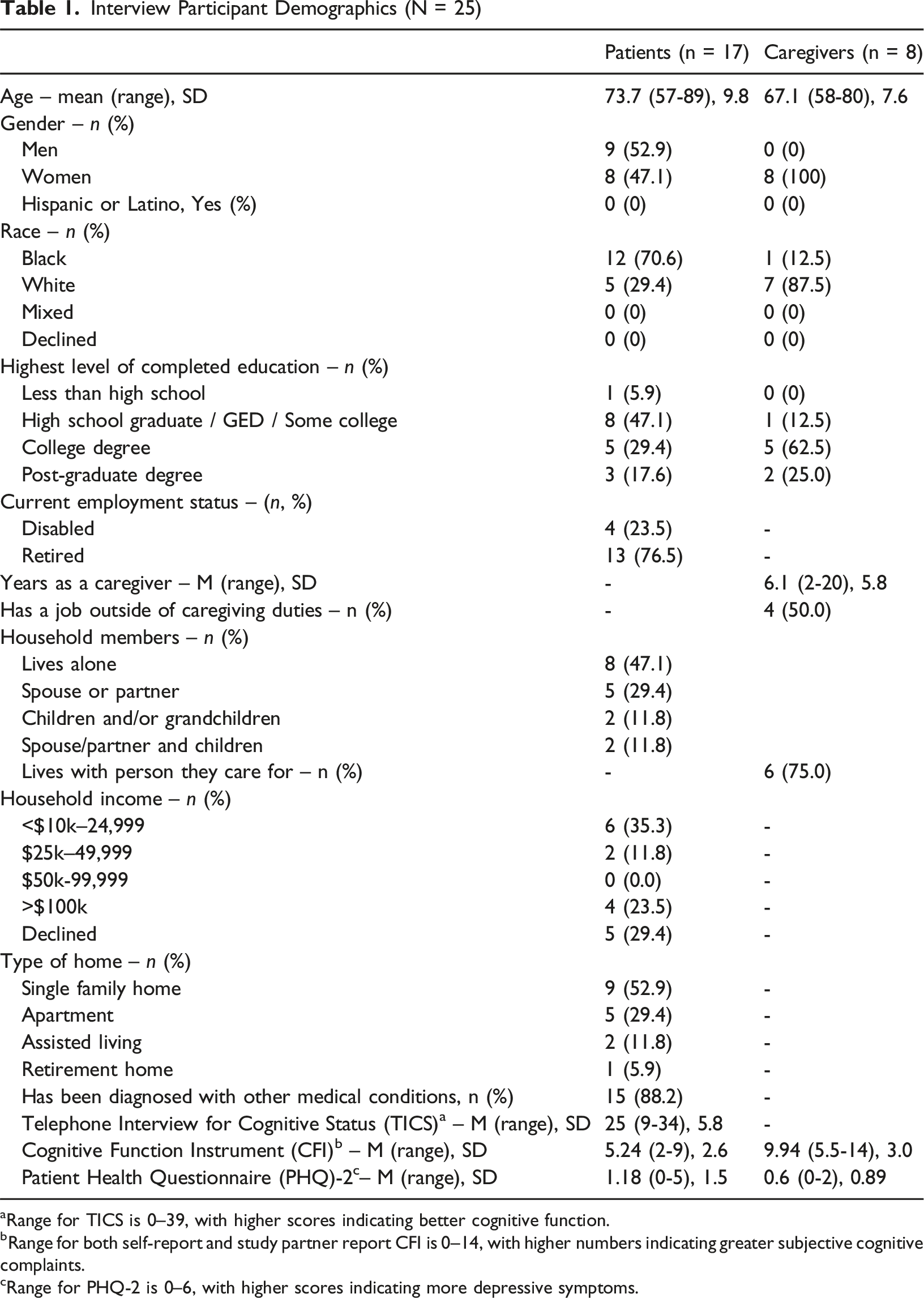
aRange for TICS is 0–39, with higher scores indicating better cognitive function.
bRange for both self-report and study partner report CFI is 0–14, with higher numbers indicating greater subjective cognitive complaints.
cRange for PHQ-2 is 0–6, with higher scores indicating more depressive symptoms.
Perceptions and Prior Experience with Advance Care Planning (ACP)
Of the 17 persons with cognitive impairment interviewed, 13 (76%) stated they did not recall a prior ACP discussion with their primary care provider or other provider, and several noted that this was needed. Of the four patients who reported having prior ACP discussions with a provider, three reported that specific goals were not discussed. When asked about their goals during the interviews, persons with cognitive impairment generally had difficulty thinking of specific goals. Most deferred to their caregivers/family members, with the sentiment of “whatever you guys (family) think is good for me, I have to live with that.” (PT 9)
Similar to reports of persons with cognitive impairment, six out of eight caregivers interviewed (75%) stated they had not had an ACP discussion with their loved one and primary care provider. Most reported that an advance care directive existed, however, there had not been intentional discussions about this with a primary care provider. Congruent with the perspectives from persons living with cognitive impairment, many caregivers explained how their loved ones relied on them to make decisions. One caregiver raised concern about how much her husband relied on her for his decisions: “My husband has always pretty much depended on me to make a lot of decisions, so I guess what would happen if it’s me [who has a medical problem] and not him? He will be in bad shape.” (CG 1) Many caregivers focused on their desire to include their loved ones in the decisions making process. They noted the heaviness of the responsibility: “… when you’re making decisions about other people’s lives, suppose after you’re riddled with guilt. That’s awful. I think the more the person is making those decisions themselves, the better.” (CG 1) A few caregivers identified being shut out from talking when trying to talk to their loved ones about ACP topics. In addition, some identified the desire for healthcare providers to have more proactive dialogue, both about ACP as well as about what to expect with progression of dementia generally. “A structured discussion with our doctors and people in the field, I could see a lot of benefit from that. Because it would help us then to have a set of goals.” (CG 8)
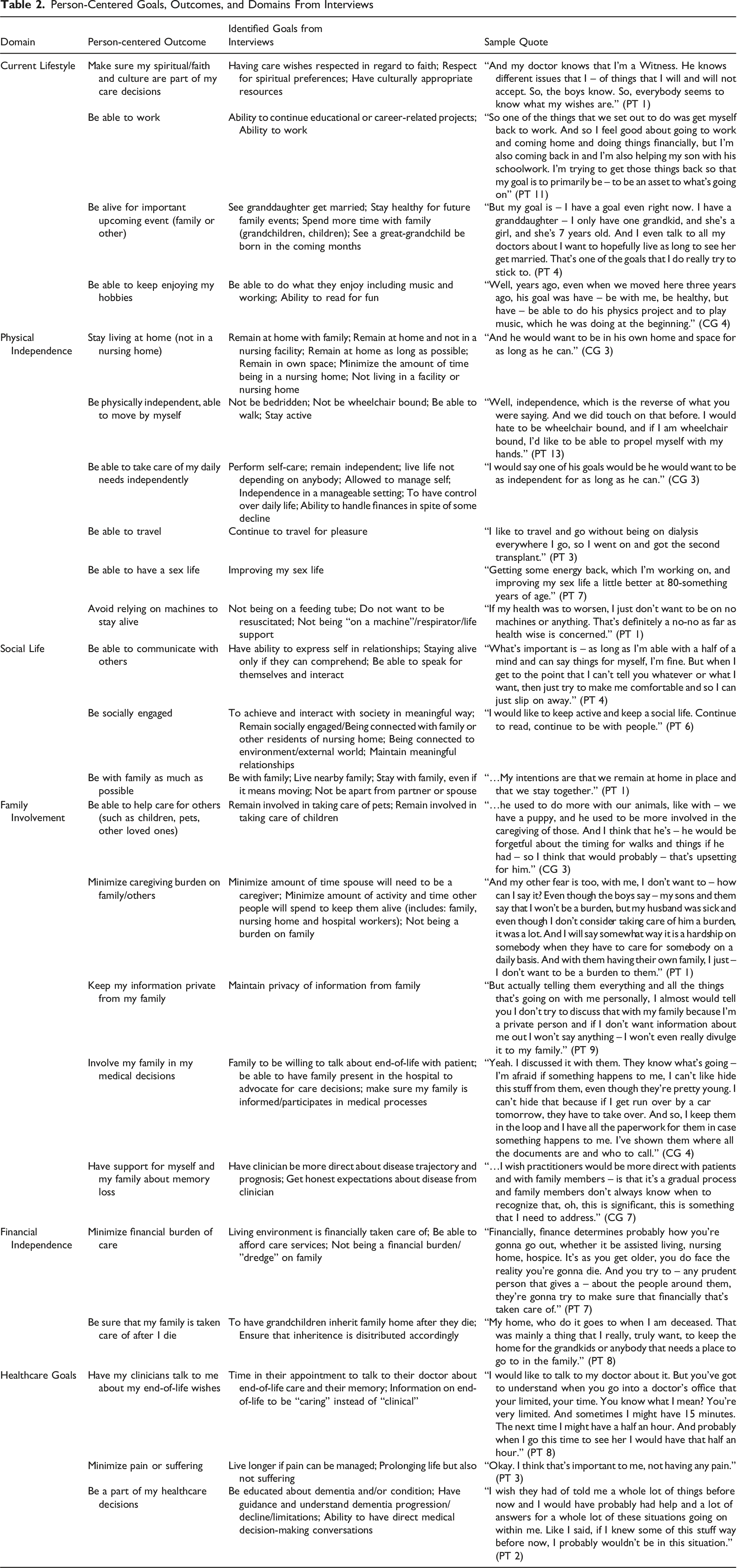
Person-Centered Outcomes and Domains
Person-Centered Goals, Outcomes, and Domains From Interviews
Discussion
Our findings suggest that persons with cognitive impairment and their caregivers are not routinely engaging in ACP discussions with primary care providers. Only 20% (5/25) of the patients and caregivers in this study reporting having had a prior ACP discussion with their primary care providers, which is less than persons with dementia and caregiver reports in other studies (Gabbard et al., 2020; Poppe et al., 2013). Further, findings highlight that persons living with cognitive impairment and caregivers are primarily focused on issues of quality of life when considering ACP priorities. Participants identified a list of goals that were ultimately sorted into 23 person-centered outcomes related to ACP for patients with cognitive impairment that were organized into six domains. Five of the six domains (physical independence, social life, family involvement, financial independence, current lifestyle) focused on quality of life socially and physically, with the other domain being medically focused (healthcare goals).
Our findings support prior work that has suggested the importance of focusing on quality of life goals and not solely medical outcomes (Flaherty et al., 2025; Hofmann et al., 1997; Jennings et al., 2017; McMahan et al., 2013; Poppe et al., 2013; Shafir et al., 2022). Our study identified 23 person-centered outcomes that can be used to guide ACP interventions for persons with cognitive impairment and their caregivers. The majority of the outcomes were not related to medical care, but rather reflected desires to preserve independence and maintain social connections. Further, most persons living with cognitive impairment in this study had difficulty responding to open-ended questions inquiring about goals, suggesting that a structured tool may be necessary in order to elicit their preferences. By providing the list of outcomes generated in this study to persons with cognitive impairment and their caregivers during ACP discussions, providers may better empower them to identify tangible priorities that they want incorporated into care plans currently and in the future, thus enabling personalized and efficient ACP (Hanson et al., 2017; Wendrich-van Dael et al., 2020). These person-centered outcomes can then be used by caregivers and clinicians to inform acceptable medical interventions as the diseases progress. Finally, in addition to facilitating more effective conversations with persons living with cognitive impairment and their caregivers, use of these person-centered outcomes to jumpstart a discussion can reduce some of the clinician-reported barriers associated with ACP such as lack of time and understanding of the care planning process or comfort in initiating the conversation (Bosisio et al., 2021; De Vleminck et al., 2014; Phenwan et al., 2020; Shafir et al., 2022; Snyder et al., 2013; Tilburgs et al., 2018).
To create a patient-responsive healthcare system, there is a critical need to involve persons living with cognitive impairment in the decision-making process in a way that is meaningful to them, however, persons with cognitive impairment have not been consistently included in ACP interventions (Tetrault et al., 2022). Given that most ACP discussions occur within one month of death, most persons with cognitive impairment are not able to engage in decision-making at this time given severity of disease progression (Clayton et al., 2024; Poppe et al., 2013). Having a set of person-centered outcomes can provide a framework for providers to facilitate conversations with patients with dementia related to the impact of their cognitive function (and associated medical interventions) on all relevant life domains. Focusing on the goals, values and preferences of persons with cognitive impairment earlier in their disease processes can facilitate better alignment of clinicians’ medical recommendations with what they identify as most important once their disease is more advanced and they are unable to directly participate in decision-making (Dening et al., 2013; Flaherty et al., 2025; Hirschman et al., 2008; Huang et al., 2022).
Limitations
This study took place at a single academic institution in an urban setting, with most patient participants being Black and most caregiver participants being White women. This potentially limits transferability of the findings to other settings. In addition, the study used a convenience sample of persons with varying levels cognitive impairment who were already participating in a research study or were identified by clinicians, thus biasing the sample to persons who are more engaged with the health system. Patients were also cognitively impaired, and thus some of their interview responses that rely on recall (such as whether or not a prior ACP discussion with their primary care provider had occurred) may have been factually incorrect. Also, one individual identified as having cognitive impairment had TICS scores that fell in the normal range. It is uncertain as to whether they were misclassified regarding having cognitive impairment. Finally, this work was conducted during the COVID-19 pandemic during which participants experienced changes to their daily routines, thus likely impacting their perspectives on goals and priorities. Despite these limitations, this work is novel in that it engages persons with cognitive impairment and caregivers to identify outcomes that are most meaningful for inclusion in ACP interventions.
Conclusion
Our study identified 23 person-centered outcomes that can be used to guide ACP interventions for persons with cognitive impairment and their caregivers. The majority of the outcomes centered on maintaining independence and social connections. These outcomes can be used to inform a tool designed to guide clinicians in ACP discussions that enable persons with cognitive impairment to identify and prioritize their desired outcomes. Most persons living with cognitive impairment in this study had difficulty responding to open-ended questions inquiring about goals, suggesting that a structured tool may be necessary in order to elicit patient-related preferences. Given the lack of consensus on the ideal components of ACP interventions for persons with cognitive impairment and outcome measures for evaluating effectiveness of these interventions (Wendrich-van Dael et al., 2020), our study has the potential to transform the way ACP interventions are implemented and evaluated in this vulnerable population.
Supplemental Material
Supplemental Material - Patient- and Caregiver-Identified Goals for Advance Care Planning in Patients With Dementia or Cognitive Impairment
Supplemental Material for Patient- and Caregiver-Identified Goals for Advance Care Planning in Patients With Dementia or Cognitive Impairment by Kristin L. Rising, Angela M. Gerolamo, Nazanin Sarpoulaki, Venise J. Salcedo, Grace Amadio, Robin Casten, Anna Marie Chang, Alexzandra T. Gentsch, C. Virginia O’Hayer, Barry Rovner, Brooke Worster in Dementia
Footnotes
ORCID iDs
Ethical Approval
This research was approved by the Institutional Review Board at Thomas Jefferson University.
Consent to Participate
All participants provided verbal consent to participate.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Pennsylvania Medical Society in a grant issued to Kristin L. Rising (2019-PAMED-00182). The funder did not have any role in the design of the study; collection, analysis, and interpretation of data; or writing of the manuscript. The statements in this article are solely the responsibility of the authors and do not necessarily represent the views of the Pennsylvania Medical Society.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.