
Abstract
There are significant challenges in creating and maintaining positive care cultures for people with dementia. My Home Life is a UK initiative that provides staff with frameworks and tools to facilitate the development and implementation of strategies that support compassionate, relationship-centred care. Staff at a neurobehavioral unit used one of these tools, ‘A Way with Words', and developed this into a language intervention, flipping language, which was grounded by the principles of My Home Life. This qualitative study explored how flipping language impacted on care provision and culture in a neurobehavioral unit. Five focus groups were held with staff (n = 23) and family members (n = 3) to understand their experiences of the flipping language intervention which involved staff and families exploring everyday clinical communication with individuals living with dementia. Using reflexive thematic analysis, seven themes were identified from the data. Flipping language resulted in staff having a better understanding of the person which facilitated tailored support. Conversely, families believed that knowing a person fosters language about them being flipped. The power of language was highlighted by all participants. Families spoke about the impact that clinical language had on their care journey. Staff spoke about their experiences of the playful and curious approach to flipping language fostered a culture of openness and connectedness. In summary, flipping language was perceived to promote a care environment that was enabling for staff to connect with residents, families and other staff, facilitating personalised and relational care. Flipping language has the potential to be implemented in any care setting seeking to challenge and improve care practices and culture. Unique components of this study include the intervention being led by a lived-experience staff member.
Keywords
Introduction
There are significant challenges in creating and maintaining positive care cultures for people with dementia (Handley et al., 2017). Poor care standards for older people continue to be reported internationally, with policy emphasising the need to implement care that is person-centred and promotes personal dignity (Dewar & MacBride, 2017; Koh et al., 2022). Ageism is recognised as a major social issue affecting people’s health and wellbeing (WHO, 2021). Ageism pervades society and institutions, and in healthcare is evident in policies, organisational culture, and social interactions (Sao Jose et al., 2019; WHO, 2021). Compounding negative stereotypes associated with advancing age, for people living with dementia, stigma is prevalent within health services and in the community (Swaffer, 2014). Furthermore, the dominant biomedical approach in healthcare is situated within a deficit discourse that focuses on disease and symptoms and locates the problem as within the person. The medical discourse separates normal (successful) aging from abnormal (unsuccessful) aging (Libert & Higgs, 2022). The “othering” and subsequent discrimination that occurs to those who are “stigmatised” has been well documented over decades (Link & Phelan, 2001; Rewerska-Juśko & Rejdak, 2020).
The role that language has in contributing to stigma, and mitigating it, is well acknowledged (Fforde et al., 2013; Swaffer, 2014). Kate Swaffer (2014), an academic with lived-experience of early onset dementia, advocates that the language used about people with dementia should be normal, inclusive and focus on the person rather than the disease and/or care system. Kitwood (1997) explored how biomedical language is used to define and position people with dementia as a challenge or problem; a process that legitimates structural relationships of dominance, discrimination, power and control. This manifests in language as an objective stance, using de-personalising deficit discourses to reinforce the pathological features of disease and behaviour, whilst reducing the subjective and intersubjective experiences of the person. In arguing that dementia care should be centred in personhood, Kitwood (1997) identified the necessity to situate care relationally and within each person’s social world, implying mutual recognition, respect and trust for and between individuals. This requires health practice that identifies the status bestowed upon humans, with interactions that situate and seek to understand the rich individual histories and attributes of people, and in doing so, changes reductionist discourses of power and domination that are common to the language of medicine and healthcare (Kitwood, 1997; Koh et al., 2022). Issues related to deficit discourses extend beyond dementia care into the range of healthcare settings. Deficit discourses are particularly common about people living with a mental illness (Dawson et al., 2021), those identifying as gender diverse (Ferfolja & Ullman, 2021) and/or individuals with Aboriginal and Torres Strait Islander identities (Fogarty et al., 2018). Approaches to addressing deficit discourses and how these legitimise structural power imbalance in healthcare settings are urgently needed.
One such approach is My Home Life which is an international movement that promotes innovation in social and health care to improve the quality of life for those living, dying, visiting and working in care settings for older people (My homelife, ND; Sharp et al., 2018). The foundational principles of My Home Life are relational practice, appreciation, and collaboration (Sharp et al., 2018) and are analogous with person-centred behaviours that enable personhood and wellbeing for people with dementia (Kitwood & Brooker, 2019). My Home Life frameworks underpinning these principles include the Caring Conversations framework and Appreciative Inquiry (My Home Life England, 2020). The Caring Conversation framework centres practice in conversations that are courageous, emotionally connected, curious, collaborative, considerate of other’s perspectives, compromising and celebratory (Dewar & MacBride, 2017; Dewar & Nolan, 2013). Such conversations, underpinned by theory of Appreciative Inquiry, enable staff to develop curiosity and discovery about a person’s strengths and motivations (Sharp et al., 2018) and provide scaffolding for building positive culture.
This study is situated in the context of recent organizational cultural reform that occurred in South Australia after a failure of care for older people living with serious mental illness and dementia. In 2017, an external review was conducted of a 64 extended-stay place of care for older persons with complex mental health needs (Groves et al., 2017). The review was prompted by complaints from families and staff about the conduct of staff and care provision at the Oakden Older Persons Mental Health Facility (ICAC, 2019). The final report highlighted significant failures in governance, clinical care and organisational culture, including reports of use of pejorative language to describe behaviours and using language to imply the person had acted deliberately (Groves et al., 2017). Subsequently, Oakden was closed, and an oversight committee was formed with responsibilities regarding development of a model of care, infrastructure, staffing, clinical governance, organisational culture and reducing restrictive practices (McGrath, 2022). The Culture Reform Working group, including people with lived-experience, clinical, community and advocacy representatives and industry, co-designed a culture framework that placed compassionate relationship-centred care at its core (McKellar & Hanson, 2020).
Person-centredness has been associated with improved quality of life for people living with dementia (Sjögren et al., 2013). Relationship-centred care, however, extends person-centred care principles and acknowledges the role of all relationships in care delivery and has been shown to improve care quality and staff satisfaction (Soklaridis et al., 2016). Although relationship-centred care is identified as key to transforming care and outcomes for people with dementia (Kitwood & Brooker, 2019; McKellar & Hanson, 2020), this requires substantial change to structures that direct care, service provision and communication with people with dementia (Koh et al., 2022). In response to the reform following the Oakden Report, My Home Life was selected to inform the model of care for a new state-wide specialist dementia care unit in South Australia. To support practice change, My Home Life includes a range of tools which have been created to facilitate the development and implementation of strategies that support compassionate, relationship-centred care (My Home Life England, 2020).
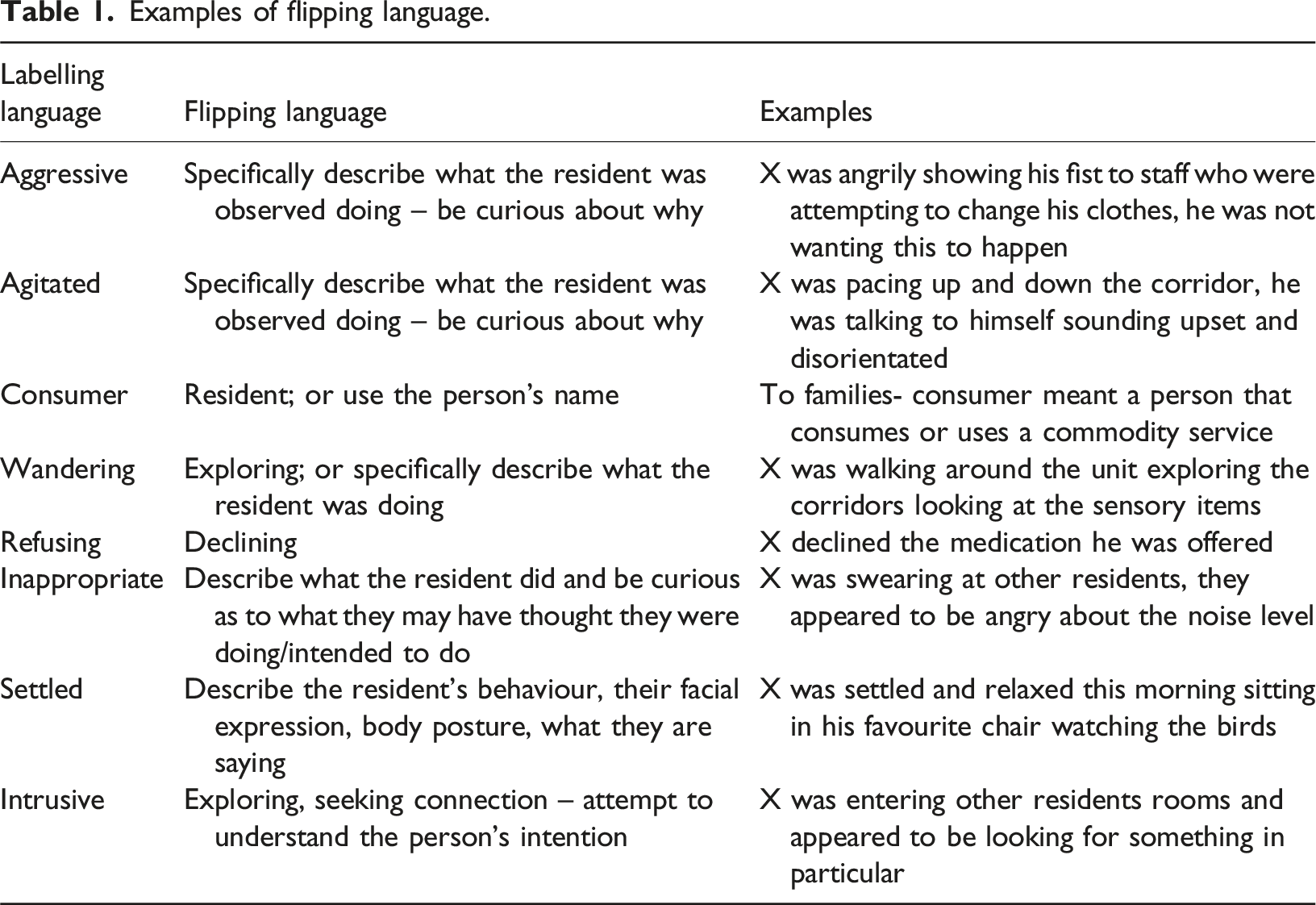
This study investigates the application of one of these tools, ‘A Way with Words', which was selected by the carer consultant to explore language used on the unit. ‘A Way with Words’ Tool, (see A Way with Words - My Home Life Charity, 2022) provides suggestions of how to collaboratively explore alternatives to words or phrases that are perceived as negative. An example is changing the label intrusive to a descriptive phrase, such as a man who likes to seek connection and company from others (My Home Life England, 2020). This tool was adapted into a whole-of unit intervention named flipping language, which facilitated the exploration of frequently used language in a specialised high dependency unit for people with behavioural and psychological symptoms of dementia (which refers to mood and behaviour changes). Flipping Language is a deliberate process that involved staff pausing, noting language that is being used, reflecting on the meaning and impact of language, and modifying language. The research aimed to understand how examining everyday clinical language used in communication regarding individuals living with dementia may contribute to building a positive culture to improve care practices, experiences and outcomes. Specifically, we sought to answer the following questions: (1) What is the impact of flipping language on care practices? (2) What are staff and carer experiences of flipping language?
Methods
Methodology
This qualitative study applied a social constructionist framework and Appreciative Inquiry to inform the research process. Social constructionism facilitates an understanding of how and why individuals make meaning and apply knowledge and how their behaviours and practices might be adaptive to this knowledge within a particular setting (Thomas et al., 2014). Appreciative Inquiry is both a theory and a method that relates to social constructionism in fostering meaning-making through a collaborative and strengths-based approach to change (Sharp et al., 2018; Whitney & Cooperrider, 2011). Flipping language used Appreciative Inquiry as a method to inquire about people’s perspectives and understandings of language and co-create new understandings. Appreciative Inquiry assumes that people and organisations have capacities, resources and strengths that can be drawn upon to facilitate change (Dewar & MacBride, 2017). Caring Conversations was the facilitator of these discussions, with the research members applying the six attributes of the framework (being courageous, connecting emotionally, being curious, considering other perspectives, collaborating, compromising and celebrating) in their explorations during staff focus groups (Dewar & MacBride, 2017). As such, these two frameworks were used by the research team to inform the development of the focus group questions, facilitation of focus groups and analysis of these discussions.
The research team included clinicians (medical and nursing), a carer consultant (with lived-experience of caring for a family member with dementia) and clinician researchers (occupational therapist, speech-language pathologist and provisional psychologist). The investigators acknowledge a collective commitment to improving care practices and culture in dementia and mental health and aged care settings.
Setting
The study took place at the neuro-behavioural unit, a specialised, purpose-built, high dependency unit for people with the most severe presentations of behavioural and psychological symptoms of dementia. The neuro-behavioural unit houses 18 rooms, across 3 pods of 6 beds each and is staffed by a multi-disciplinary team of nursing, allied health, medical, and lived-experience (carer consultant). The Carer Consultant is a member of the leadership team and is a key conduit in the development of family friendly practices and service delivery. The neuro-behavioural unit opened in February 2021 with a new model of care, informed by contemporary evidence for individuals with extreme behavioural and psychological symptoms of dementia and drawing heavily on My Home Life approaches (South Australia Health, 2020). This included a de-emphasis on a clinical model and the promotion of psychosocial and non-pharmacological interventions. To support implementation, key staff from the neuro-behavioural unit attended training in My Home Life with the South Australian Innovation Hub between 2020 and 2021. This included several members of the research team (JA, MP, KM).
Intervention
Examples of flipping language.
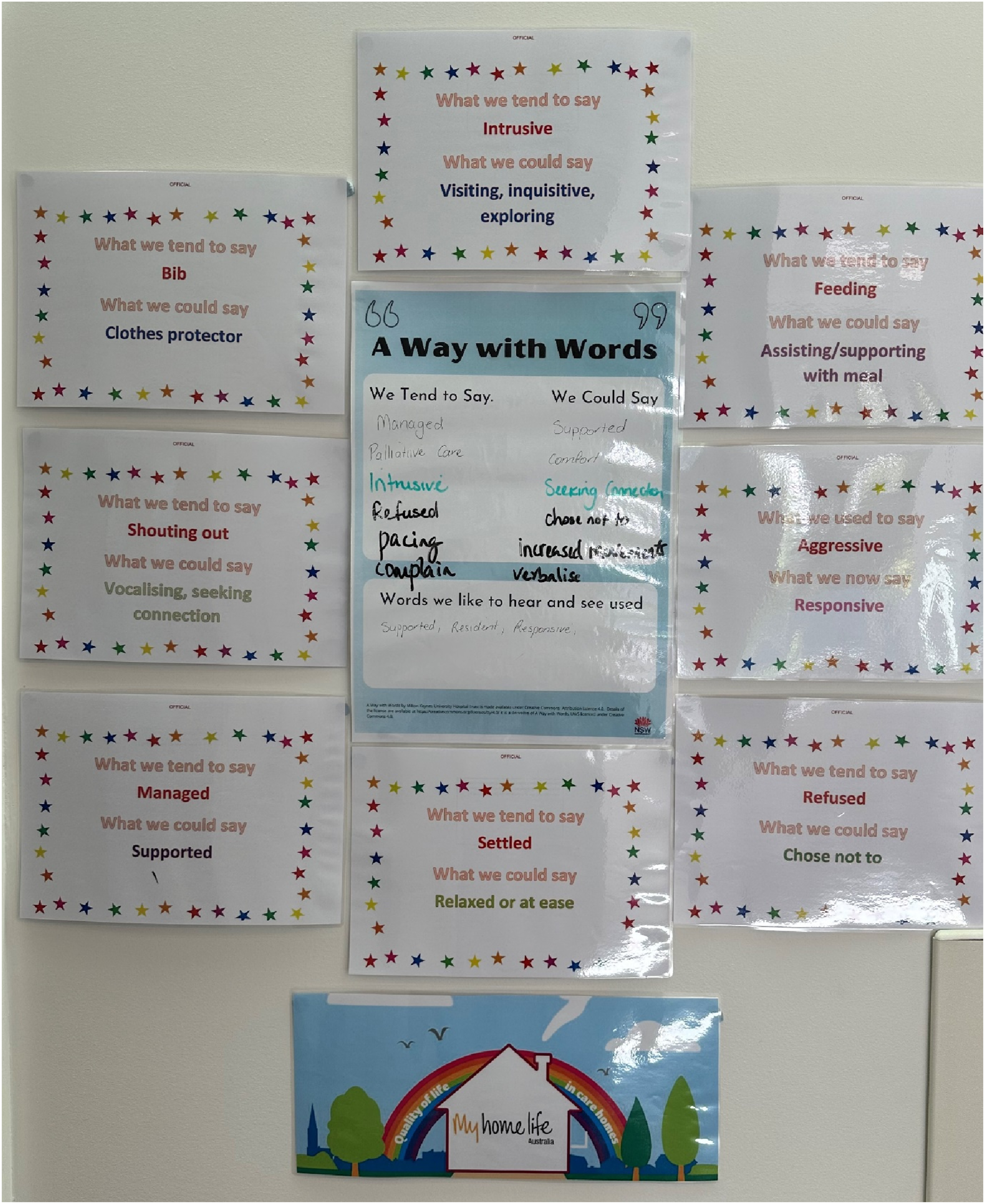
Flipping language board.
The above image illustrates how posters with examples of flipping language were shared with staff and families on the unit.
Participants
Two groups of participants were recruited from the neuro-behavioural unit: 1) staff from a range of disciplines; and 2) family members of current residents. Participation was voluntary with no exclusion criteria. Staff and families were invited to attend a focus group of up to eight participants to discuss their experiences of flipping language. Information about the project was presented at staff meetings and huddles. Families were contacted in person while attending the neuro-behavioural unit, or by letter. Potential participants were provided with an information sheet outlining the project, and a consent form. Information about the study was displayed on the unit information board. Staff researchers known to the families personally engaged with them to explain the ethics process and their choice regarding participation. To minimise the risk of participants feeling obliged to participate, people’s understanding of consent was rechecked at the beginning of each focus group.
As involvement in this study required an ability to articulate understanding of language comprehension and expression, in addition to recalling interactions on the unit, it was not possible to include residents with dementia at the neuro-behavioural unit due to the nature of their dementia being at an advanced stage.
Data collection
Focus group participants.
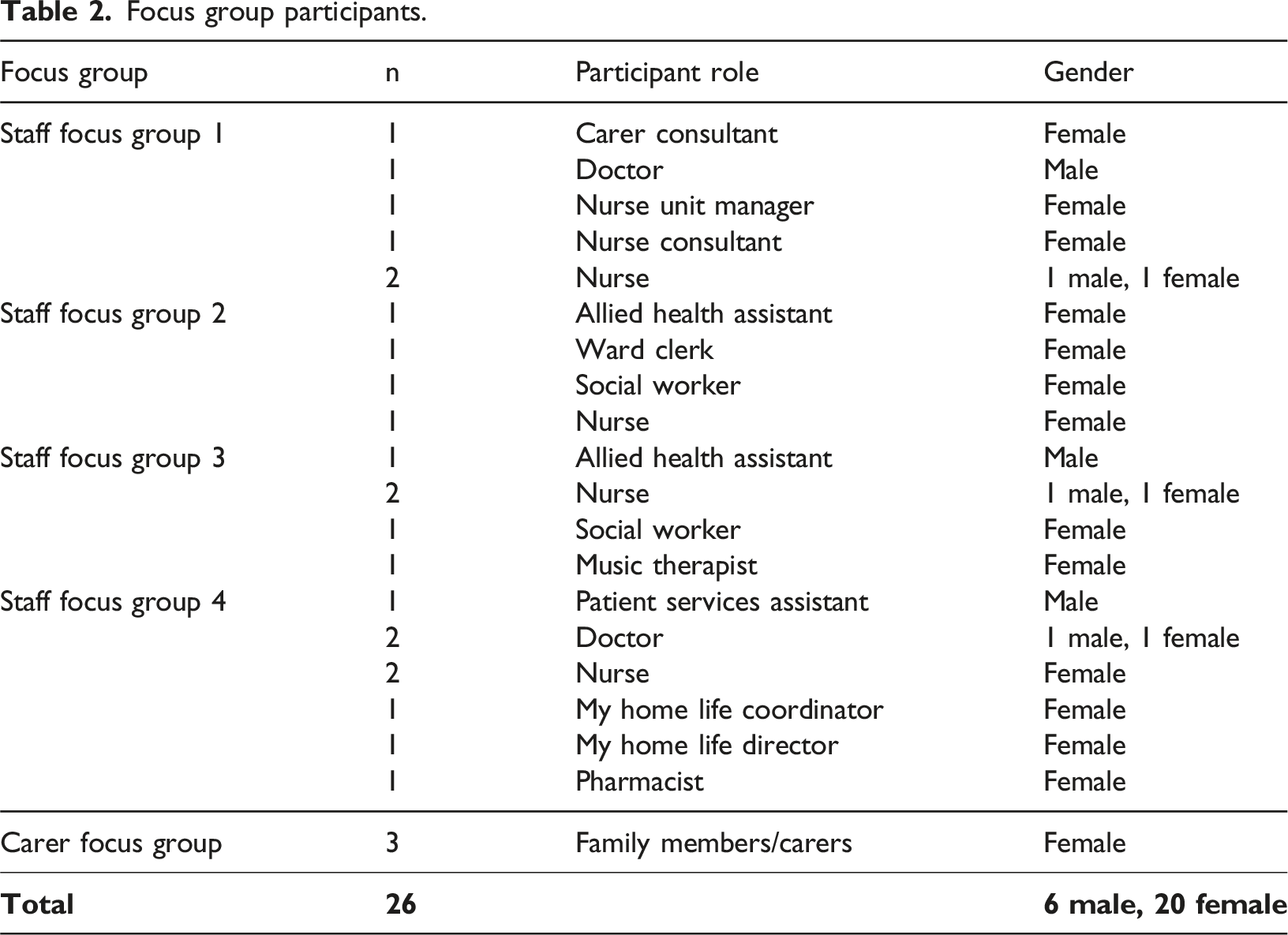
An additional focus group was held with one family member and 22 staff to present the preliminary findings and receive feedback on these.
Data analysis
Guided by the research questions, Braun and Clarke’s (2022) (Dawson et al., 2021) approach to reflexive thematic analysis was applied. This included familiarisation with the data through reading and rereading transcripts, coding (descriptively labelling data extracts relevant to the research questions), reflecting on the coding and generating themes, defining and naming themes, reviewing and reflecting on the relationships between themes, and constructing a narrative with illustrative data to answer the research questions. Each transcript was coded by several members of the research team providing diverse perspectives from lived-experience, clinicians and clinician researchers. [SC] led the write-up of the analysis which was discussed and agreed by all authors. Data was organised using NViVO 1.7.1 (QSR International).
Rigour
The facilitators met at the conclusion of each focus group to reflect on the content and process of the group. Through this process data saturation was reached. During the analysis and write-up, the research team met regularly to reflect on the process of coding and development of themes, discuss themes and generate consensus.
Ethical considerations
Ethics for this project was granted by the Southern Adelaide Clinical Human Research Ethics Committee [LNR/22/SAC/74].
Findings
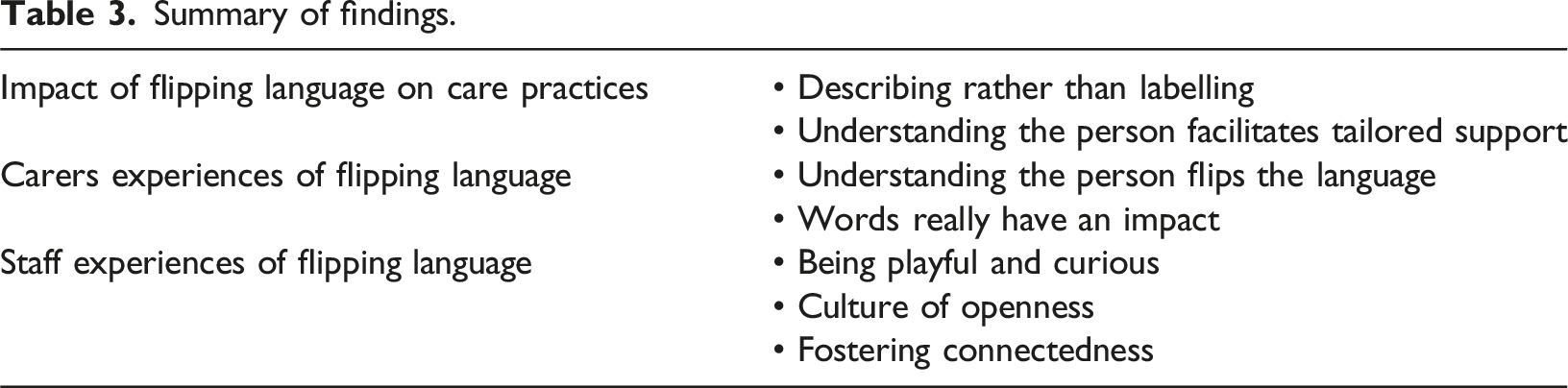
Summary of findings.
The impact of flipping language on care practices
Describing behaviour rather than labelling
Staff described moving away from using labels typical of traditional clinical language, and “the more negative words historically used” (Staff focus group 2) in similar clinical settings (e.g., aggressive, intrusive, agitated), to using ‘person-first’ language that was perceived by staff to be “probably a more accurate description of what is happening for that person” (Staff focus group 2). “We’re trying not to label, not to box them into a specific behaviour but we’re describing what they may be doing … I guess trying to reframe it in a more positive way or in a less damaging way or less labelling way” (Staff focus group 2)
Staff reflected that clinical language was generally considered a quick and efficient way to communicate essential information in a busy clinical environment. “Everyone’s trained to go with … the shortcut because that’s only gonna take you 5 seconds to read it” (Staff focus group 2)
However, staff noted that despite the perceived efficiency and precision of clinical language, it was ‘superficial’, and failed to convey depth of meaning or assist staff in fully understanding an individual’s experiences and care needs. “The old way of doing it is efficient and when you're busy and when you're under the pump, you're looking for shortcuts, and these are very short sharp ways of describing something, and then just leaving … You've done your job! It’s at a very superficial level” (Staff focus group 1) “In actual fact it’s not really precise. If people are ‘intrusive’ there’s like a range of, of reasons” (Staff focus group 3)
Staff acknowledged that documenting and verbally communicating using a more descriptive approach took longer than using traditional clinical labels. “In the handover when you have to think about how you’re going to say it, it will take you longer probably to say what you want to say rather than using one word like ‘agitation’” (Staff focus group 2)
However, this time requirement wasn’t perceived as a barrier - “I wouldn’t necessarily say it’s a barrier” (Staff focus group 2). Staff reflected that by taking the time to describe a resident’s behaviour, other staff were able to better understand residents’ behaviour and care needs. “If you really spell it out in handover, then everyone will understand what you’re talking about rather than just one word. So, it takes the thinking and the time and the writing will take longer” (Staff focus group 2)
Staff reported being mindful of the need to balance the aims of flipping language with concerns about risk for both residents and staff, alongside the requirements regarding observations and documentation about residents to translate to settings beyond the neuro-behavioural unit. “We’re still clinicians and have to record what we’re doing, professionally” (Staff focus group 4) “And that’s when we have discussions as well with them, the clinical team, going ‘well, how would this hold up in a coroner’s court that they were exploring the garden’? … We have those discussions of how we can still make it clinically sound.” (Staff focus group 4)
Understanding the person facilitates tailored support
Flipping Language helped staff better understand and contextualise residents’ behaviour. Staff reported that ‘seeing’ residents through this process positively changed the way they perceived residents and encouraged them to “look at things at a deep level” ( Staff focus group 1) and “from the resident’s perspective” (Staff focus group 2). Through this process of discovery, alongside communication with families, it became apparent that some residents demonstrated behaviours that were traceable to work or hobbies they had performed prior to being diagnosed with dementia. “I think it's because we looked at the person rather than the disease. And this was a person that was an athlete, and this was a person that was very affectionate and was known to pick people up and give them big hugs and shake them. And so, … putting that into your mind when looking at what you were seeing and making up that bigger picture assessment” (Staff focus group 1) “So, if we’re saying a resident is walking, is wandering because that’s always how they did it, they always went out for a Saturday wander” (Staff focus group 4)
Staff reported that through developing a deeper understanding of residents and their behaviour, they were able to provide care that was better tailored to residents’ needs. “For someone else it’s like physical activity is really important for them, and so… we might be thinking ‘how else will we incorporate physical activity?’” (Staff focus group 4) “If you know exactly what it is they are doing, you can work to strategies around that” (Staff focus group 2)
Carer experiences of flipping language
Understanding the person flips the language
Through sharing stories and photos of their loved ones, carers played a key role in helping staff to build a “more personal” (Carer focus group 1) and integrated understanding of residents. Carers themselves perceived their lifetime understanding and relationship with their loved one as contributing unique and valuable knowledge, adding meaningful context that informed the staff’s approach to care. “Our perspective on who they are as people is different” (Carer focus group). “Photos would make a huge difference, especially for staff. You see photos of people before dementia, and then actually to see them while they’re with the service, it just makes a huge impact yeah (Carer focus group)
Subsequently, carers perceived that staff developed a deeper connectedness and understanding of resident’s individual needs and perspectives, and that this had a positive impact on how staff provided care. “I think that’s where it flips things, and it changes things, and it turns things around. So they start to then look from the person’s perspective, because they know a lot more about their history” (Carer focus group) “Then they understand that from your point of view, and the patient’s point of view…” (Carer focus group)
In turn, carers perceived that by deepening staff understanding and knowledge about the lives of each resident, the language staff used around care provision grew more personal and empathic. “I wonder if something like that that actually helps flip language as well, because it just broadens our awareness straight away. And you would just naturally expect language to change a little” (Carer focus group)
Words really have an impact
Carers reported that the language used by staff to describe their loved ones was important and impactful. They reflected on their own vulnerability during what was a stressful time in their lives and the lives of their loved ones, as they faced the progressive cognitive and physical decline associated with dementia. “There’s a lot for you to process when the partner, husband whatever is going through this...you do become much more vulnerable, and sensitive to what’s being said to you” (Carer focus group) “Hearing things – words that describe your partner, they’re heart breaking, so there’s other ways of doing it” (Carer focus group)
Carers spoke of the ‘negative’ words and phrases used by other health services regarding their loved ones’, such as their loved one being “managed”…“aggressive”, [or] “behaving inappropriately” (Carer focus group). In contrast, carers perceived the language used at the neuro-behavioural unit as humanising their loved ones, using words that positioned residents positively, rather than as a problem. “There’s a big barrier when you say the traditional word ‘he is…rude, aggressive, intrusive’. It suddenly becomes negative. So the flipping language, that always invites you to the positive things” (Carer focus group)
Flipping language was perceived by carers to create an environment and care culture that was “very different” (Carer focus group) from other health services they had encountered. “Certainly different from hospital… it’s softer and more positive here” (Carer focus group) “I haven’t come across a lot of negative energy in neuro-behavioural unit” (Carer focus group)
Staff experiences of flipping language
Culture of openness
Staff perceived the positive culture of the neuro-behavioural unit to be an essential ingredient in facilitating flipping language. They reported feeling that it was a “psychologically safe space” (Staff focus group 2) to question, explore, experiment with language, and to encourage and learn from each other. “We’re all pretty open with each other, and we do share it, and when someone does something well, they go, ‘well that was really good’. Or if you see someone else do it, … you might see it and go, ‘actually that does sound nicer’, or ‘that does capture what happened in that moment a bit better, and maybe I can’ – you know, we share our learning.” (Staff focus group 4)
This culture of openness extended to documentation, as staff read each other’s notes and reflected on how other staff described residents’ behaviour. “You’re looking at each other’s notes and things you write, and saying, ‘oh, I like the way you’ve done that’” (Staff focus group 4)
Staff also reported feeling safe to communicate openly with family members, even if that meant communicating uncertainty, which staff indicated was not the case in other health settings where they had worked. “So, it is quite amazing to sit with someone and just see that impact …I feel lucky that we can have those conversations with family here” (Staff focus group 3) “I know certainly I’ve had conversations with family members, and it’s felt incredibly heated and I’ve just – instead of doing the usual clinician 'wall up' thing and I’ve kind of gone, “this isn’t feeling comfortable. I don’t know what to say. I’m not sure this is going to help you out”, and then just saying that and having that honesty in itself…which I think comes from the way we use the language as well has, you know, helped the conversation rather than kind of completely disengaging” (Staff focus group 3)
Being playful and curious
Staff reflected on using playfulness and curiosity rather than criticism to encourage each other to explore language and develop new ways of communicating that moved away from labelling and towards a deeper understanding of residents’ needs. Rather than imposing rules around ‘right’ or ‘wrong’ language, staff worked together, playfully exploring language use and being curious about residents’ behaviours. Staff discussed and demonstrated an ongoing curiosity about language and its meaning, unpacking the meaning of words and phrases, and playfully examining them to discover what was the most useful, helpful, and accurate way of describing behaviours. “Nothing being absolute mandated that you’ve got to say it this way…it’s a curiosity about language, rather than necessarily having to get it perfectly right all the time” (Staff focus group 4) “It’s not to say there’s a right or a wrong way, but it’s to play with it and just be curious” (Staff focus group 1)
Staff encouraged each other “to be kind…to be curious” (Staff focus group 1) about residents’ behaviour and to explore different ways of describing what they observed. Throughout staff focus group discussions there was often laughter as staff members discussed flipping language, and a sense of playfulness and curiosity was tangible. “Flipping language opens conversations because you find us laughing for half an hour in handover not because you’re handing over the clinical thing, but you’re just talking about the language” (Staff focus group 1). “Maybe just to go back to the flipping language and the point of being playful, the outcome with that is, again about connection, but about engagement and energising” (Staff focus group 4)
Fostering connectedness
Through openness, curiosity, and playful exploration, staff reported experiencing a greater sense of connectedness with each other, and with residents and their families. “We try to understand, that makes us really connect with the residents and carers and also our staff” (Staff focus group 1) “Just knowing there's something deeper, the just knowing “Let's flip this to see sort of what else we might see”, isn't just an academic exercise, it's actually an individual exercise and you have to connect with someone to get the answers because one person's aggression and somebody else's are different reasons. And so it just invites that opportunity to look at things at a deep level” (Staff focus group 1)
Staff perceived that through the exploration of language, they developed a deeper understanding of residents, which facilitated emotional connections with residents’ families and carers. “It connects people emotionally. We’re talking about language connecting emotionally. You talk clinically, it’s a barrier. And I think that’s where it’s huge. That’s where the impact comes from, is you’re emotionally connecting with people on a very different level because you’re talking about their loved one” (Staff focus group 1) “I notice how much [the language] benefits families, think it simplifies things for them too, when you talk more, more connecting emotionally” (Staff focus group 4)
Staff also reported feeling a greater sense of connection with their work colleagues. “It can be a case of – especially if busy, like, thinking that people aren’t caring or anything like that. But if you see that everyone’s doing things, … person centred notes, I think you then have a bit more of a connection with your … co-workers as well” (Staff focus group 3)
Staff conveyed satisfaction in being able to work in a way that was congruent with the values that had initially led them to pursue a career in healthcare. “I came to be a nurse because I wanted to care for people, and I wanted to talk to people, and I wanted to connect with people. Like, sometimes the system takes that away, but I think this is where that helps me have that moment to reflect and sit in the moment with people” (Staff focus group 3) “That’s why you come into nursing was to connect with people, to build relationships, to help people. And I feel like this is a good way to do it” (Staff focus group 1)
This greater sense of connection was perceived by staff to have a beneficial effect on the quality of care they provided. “We are really connected each other, we are giving good support” (Staff focus group 1)
Discussion
Findings from this study highlight the impact of language on care and service culture and demonstrate the power that language adjustment as an intervention can have in creating and sustaining positive culture. Flipping language explored the intent behind words used in everyday clinical practice in a dementia care setting. This exploration changed staff use of language, and subsequently, positioned both the resident and the relationship between the resident and the practitioner more positively, thus reducing the power imbalance between them. Practice-change initiatives in clinical settings can be challenging to implement and maintain (Powell et al., 2015). However, the flipping language intervention has been successfully implemented and maintained at the neuro-behavioural unit over a three-year period. The closure of Oakden due to severe failure in care, led to the development of models of care that prioritised the implementation of a cultural framework to support staff to provide care meaningfully and safely for people living with severe dementia (McKellar & Hanson, 2020; South Australia Health, 2020). This was an opportunity to do things differently. Central to the older persons’ mental health culture framework is compassionate relationship-centred care (McKellar & Hanson, 2020). Our study findings show that flipping language is an approach that can effectively change care practices, promote connection (between staff, residents and families) and positively influence the culture of care. We suggest that this method of facilitation of a three-way connection between staff, residents and families, fosters the context for relationship-centred care.
Staff commented that although medical language creates distance, flipping language reduces distance, and fosters emotional connection. Biomedical language conventions are often justified as producing an objective, measured stance, and in people with dementia, facilitates a quantitative approach to describing behaviours that infers an equal, reasoned approach to care. However, critical analysis reveals this use of language as “the medium of domination and social force…to legitimise relations of organised power” (Habermas and McCarthy, 1977, p. 259). Language produces meaning for users and recipients that become stable and routinised. Over time, these meanings are rarely critiqued and come to be seen as ‘given’ (Wodak, 2001). In identifying how flipping language related to their emotional connectedness with residents, staff made visible their interconnectedness with the residents. Upon further exploring how the flipping of their language facilitated their understanding and individualisation of the resident’s care and support, they captured the relational practice that is key to honouring personhood (Kitwood & Brooker, 2019). It is reasonable to surmise that this use of language that centres the person and enables a relational, meaning-based approach to care will also reduce power differences between staff, patients and families. However, this requires further research. In particular, studies are needed to explore the impact of flipping language on the care relationships and outcomes from the perspectives of patients and families.
Although staff identified that flipping language could improve their understanding of a person, family members approached this in reverse, highlighting that understanding the person led to a change in language. There are other methods that are used in clinical practice to gain a greater understanding of the person. One such method is building life stories which involve developing detailed accounts of the person’s life through interview with the person and their family members (Kindell et al., 2014; Rey et al., 2024). Life stories are rich in context, however developing a meaningful narrative requires significant staff investment. Flipping language when embedded into daily practice, can be applied immediately and broadly. As such, flipping language has the potential to be sustained in practice across a range of settings (including short stay acute settings where staff may have less time to get to know patients).
The power of flipping language is underpinned by the combined application of Appreciative Inquiry and the Caring Conversations framework. Dewar and Nolan (2013) found that combining these approaches/frameworks enables the development of ‘person and relational knowledge’ (p.1247). In a study where Appreciative Inquiry was used as an approach to develop Caring Conversations in a care home in Scotland, staff reported improved individual and team morale, new learnings and changes in practice (Dewar & MacBride, 2017). These findings closely align with our study outcomes, where clinical staff reflected that new learnings about the person resulted in an improved understanding and thus change in their care approach. Although the facilitators of flipping language had an in-depth understanding of Appreciative Inquiry and the Caring Conversations framework, the broader team had not been socialised to these frameworks beyond the process of participating in the flipping language intervention. This suggests that a few key champions with an in-depth understanding of the frameworks can facilitate uptake of My Home Life principles into practice. Playful provocation has been highlighted as a key feature of successful implementation of the frameworks/approach (Sharp et al., 2018), with this playfulness evident in the focus group discussions. Playful provocation appeared to be a useful approach that should be used in future implementation, as highlighted by staff who reported feeling safe to be exploratory with language. Furthermore, a study using Appreciative Inquiry alone as an approach to co-develop knowledge and practice in a hospital setting, found that staff reported the approach to be empowering, safe, and leading to possible alternative ways of doing things in practice (Hung et al., 2018). We propose that future facilitators of flipping language require an understanding of the Caring Conversations framework and/or Appreciative Inquiry to effectively promote positive and sustained cultural change.
Alongside the many positive experiences, staff also reported challenges associated with flipping language. A staff member, reflecting on the findings from this analysis, stated that “change needs to occur in the community [general public] so that changes in language [about care] is acceptable and safer”. This reflection aligns with a recent international review of healthcare workers’ understandings of dementia, in which the authors suggested expanding relationship-centred care to include the broader community, could support culturally inclusive care approaches (Jenkins & Smythe, 2024). Broader change may enable staff to feel more empowered in using language differently within medical care settings by ensuring that it is valid, acceptable and understood in other health and aged care contexts, and importantly, could also empower the recipients of care across their care journey. Whilst flipping language was broadly implemented in the neuro-behavioural unit, staff highlighted the challenges that they encountered with other services and organisations (e.g., when making referrals to residential aged care homes). A unique component of our study was that flipping language was led by a carer consultant on the unit with lived-experience of caring for a close family member with dementia. The lived-experience workforce is evolving in mental health care, although there are concerns that workers may be co-opted to the dominant system/practice models which continue to position clinicians as experts in the provision of care and treatment (Roennfeldt & Byrne, 2021). Flipping language challenged the dominant language used for people with dementia, and thus fits well with lived-experience workforce values, which is inclusive of contributing to and advocating for system change (Gagne et al., 2018).
Study limitations and future research
This study reports on findings from one setting and thus caution should be applied regarding generalisation of the findings. The inability to include the residents (due to the advanced stage of their dementia) and the small number of family participants are limitations to this study. Additionally, there are contextual factors that may have had an impact on the success of the intervention. Specifically, flipping language was commenced several months after the unit opened, and staff were employed through a values-based recruitment process. Future research could examine the flipping language intervention in established teams in a range of settings where language is identified as being problematic/stigmatising (e.g., mental health care settings). Additionally, the application of Appreciative Inquiry alone in the flipping language intervention warrants further exploration.
Conclusion
Flipping language, the examination of everyday language used in the care of people living with dementia involving staff and families, has been sustained over several years at the neuro-behavioural unit. Key effects of flipping language reported by staff and families are an improved understanding of residents and their needs, and more personalised care responses. Staff and families reported that the flipping language contributed to a culture of openness and connectedness, highlighting the potential for this intervention to positively influence care culture. Flipping language has the potential to be implemented in any care setting. However, its power lies in the application of Appreciative Inquiry and Caring Conversations. These frameworks enable staff to examine the impact of day-to-day clinical language playfully and inquisitively and co-create a positive service culture that positively influences care practices.
Footnotes
Acknowledgements
The authors would like to acknowledge the carers and staff at the RNBU for their participation in the flipping language intervention and focus groups to discuss their experiences.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Southern Adelaide Local Health Network (SALHN) Enquiry Grant funded by Flinders Foundation and The Hospital Research Foundation Group.
Ethical statement
Data Availability Statement
The data that support the findings of this study are included in the text of the manuscript as participant quotes.
Appendix
![]() and clinicians’ experiences, aims to enhance consumer care outcomes and experiences. Suzanne was awarded an Aged Care Research & Industry Innovation Australia (ARIIA) Grant in 2023 and Hazel Hawke Research Grant in Dementia Care, Dementia Australia Research Foundation in 2022. Suzanne is in a joint position with SALHN mental health services and Flinders University.
and clinicians’ experiences, aims to enhance consumer care outcomes and experiences. Suzanne was awarded an Aged Care Research & Industry Innovation Australia (ARIIA) Grant in 2023 and Hazel Hawke Research Grant in Dementia Care, Dementia Australia Research Foundation in 2022. Suzanne is in a joint position with SALHN mental health services and Flinders University.