
Abstract
This scoping review examined literature on dementia education programs (DEPs) for healthcare providers and students. The search was conducted using the Discover! search engine that includes 63 databases. The review included a total of 25 articles that met the eligibility criteria. There were numerous DEPs that varied by frequency and duration, mode of delivery, content, target population, program evaluation measures, and outcomes. Most involved nursing staff and students and took place in Canada, the US, and the UK. The most common delivery mode was a one-time in-person session and a wide variety of topics were covered, both general (e.g., understanding dementia) and specific (e.g., driving, delirium). Twenty different tools were used to measure primarily changes in knowledge and attitudes, with little attention paid to performance and care provision. Only three studies on DEPs focused on culture in terms of race and ethnicity. The implications of this scoping review for education are that DEPs need to meaningfully address culture and culturally safe care in order to respond to the increasing diversity of older adults and care providers. In terms of future research on DEPs, program evaluation must attend to the importance of consistent measures, translation of knowledge to practice, and sustainability.
Introduction
Over 55 million people across the globe are living with dementia currently and this is expected to more than triple by 2050 (Alzheimer Disease International [ADI], 2022; Gauthier et al., 2021), largely due to population aging. At the same time dementia is increasing, countries in the global North are becoming more ethnically and racially diverse, including older adult populations (Statistics Canada, 2016). Dementia rates vary by ethno-racial group, with most studies finding higher rates for Indigenous, Black/Caribbean, and Hispanic/Latinx people compared to (non-Latino) White and Asian people (ADI, 2022; Brewster et al., 2019; Kornblith et al., 2022; Public Health Agency of Canada [PHAC], 2019). Further, experiences of dementia diagnosis and care differ considerably by ethnicity and race, with the same aforementioned groups subjected to more disparities in both health and health care than White and Asian people (Centers for Disease Control & Prevention [CDC], 2021; Iroanyah et al., 2021; Roche et al., 2021; Tsoy & Possin, 2021). For example, through a meta-synthesis of qualitative research on Black, African and Caribbean people’s understanding and experiences of dementia and dementia care, Roche et al. (2021) determined that dementia diagnosis and services are seen as irrelevant and/or inappropriate, while religion and kinship relations are very important. Centers for Disease Control (2021) reported that Black, Native, Asian and Hispanic Americans experienced higher levels of discrimination in dementia healthcare than White Americans, at 50% of Black survey respondents and 42% for Native Americans compared to 9% for non-Hispanic Whites; recommendations include diversifying the dementia workforce and addressing implicit bias in dementia training. Additionally, Iroanyah et al. (2021) identified several cultural barriers for racially-diverse populations, including beliefs that dementia is normal aging, fear of shame and stigma, avoidance of healthcare due to systemic discrimination, and lack of information and services in the language of their choice or that are culturally appropriate. This makes culturally responsive and safe dementia care exceedingly important and compels educators and practitioners working with people with neurocognitive disorders like dementia to adapt their care and teaching practices accordingly (Gale et al., 2022; Gauthier et al., 2021; Hulko et al., 2021).
At the policy level, national dementia strategies and international reports adopt the language of equity, diversity and inclusion, and promote the education of health care providers 1 to address diversity and complexity (of care and health needs), yet their discussion of ethnic and cultural minority communities focuses mainly on risk factors, stigma reduction, and dementia inclusive communities, and overlooks specific ways health care providers could be educated to provide culturally safe and appropriate dementia care (see ADI, 2022; PHAC, 2019). In addition, at-risk groups, such as Indigenous people, are addressed in isolation and there is no deep engagement with terms such as diversity, equitable, and minority in dementia strategies (Wyndham-West, 2021), indicating a pro forma approach.
A number of knowledge syntheses have examined dementia education programs (DEPs) for regulated health professionals and health care aides (Eggenberger et al., 2013; Moehead et al., 2020; Riesch et al., 2018; Surr et al., 2017; Zhao et al., 2021) and undergraduate healthcare students (Williams & Daley, 2021). Eggenberger et al. (2013) included family caregivers and persons with dementia, along with professional caregivers, in their systematic review of dementia communication skills training; the majority of the 12 studies were in nursing homes and these interventions improved skills, competencies, and knowledge of both professional and family caregivers, and the quality of life and wellbeing of persons living with dementia. An influential systematic review of the effectiveness of DEPs for health and social care workers found the majority of studies published between 2000–2015 (n = 152) took place in the US and UK, involved nursing staff (71%), and most often used group face-to-face delivery, with teaching tools including video clips, discussions, exercises, and lectures (Surr et al., 2017). The most important elements of effective DEPs were found to be content relevant to the learner’s setting and role; interactive group work and blended learning; accessible and informative materials; and trainers with strong knowledge of dementia and experience in adult education (Surr et al., 2017).
Both Riesch et al. (2018) and Zhao et al. (2021) conducted systematic reviews on dementia training for nursing home staff and built on Surr et al. (2017) by focusing not only on the effectiveness and design of DEPs, but also on the content of DEPs. Riesch et al. (2018) determined the main topics to be person-centered care, communication strategies, and information about dementia; and identified missing elements as family dynamics, palliative care, and varied health care providers’ roles. Zhao and colleagues’ (2021) systematic review of nursing home staff’s preparedness, contrary to previous studies, determined DEPs did not significantly impact participants’ attitudes and competence, thus they called for high-quality studies and an increased focus on other cultures. Similarly, Mast et al. (2021) determined the need for more attention to culture, as did Resciniti et al. (2021) in their reviews of dementia evaluation instruments used with professional and informal caregivers to assess knowledge and care. Importantly, other reviews did not specifically focus on or address culture - at all or in a meaningful way. Eggenberger et al. (2013) list ethical and cultural knowledge in their table of the content of dementia communication skills training programs, yet do not discuss culture beyond a culture of feedback.
Moehead and colleagues’ (2020) integrative review of web-based DEPs considered a wide variety of research and non-research articles and identified self-paced, interactive, and measurability to be key features of the majority of effective and functional on-line DEPs, and also noted an overall inattention to translation to practice in 37% of them. Like Surr and colleagues’ (2017) earlier review, Moehead et al. (2020) used Kirkpatrick Partners’ (2022) four-level model for assessing the effectiveness of training and found that most DEP studies only consider levels one (reaction) and two (learning) and overlook levels three (behavior) and four (results). More than 25 different measurement tools have been used to evaluate DEPs (Mast et al., 2021), with results indicating DEPs are effective at increasing knowledge and skills of care providers (Resciniti et al., 2021) and confidence and attitudes of students (Williams & Daley, 2021).
While there have been a variety of reviews of DEPs published in the past ten years, two were restricted to nursing home staff and the rest to professional and informal caregivers or health and social care workers, with none focusing on both students and healthcare providers in a range of settings. Further, the majority of these reviews have focused on specific types or aspects of DEPs such as web-based programs, communication skills, and evaluation instruments. No review to date has analyzed the extent to which culture is addressed in DEPs. Thus, in order to depict the current educational landscape in dementia care more fulsomely, and determine the extent to which DEPs address culture, we report herein a scoping review of existing and emerging DEPs for healthcare providers and students working in a range of settings.
Methods
Scoping reviews are preliminary syntheses that allow researchers to examine the breadth of existing and emerging evidence and gaps in research pertaining to a particular subject area (Grimshaw, n.d; Levac, 2010). They generally follow a five-stage process: (1) Identifying the research question or purpose; (2) Identifying relevant studies; (3) Selecting the studies; (4) Charting the data; and (5) Collating, summarizing, and reporting the results (Arksey & O’Malley, 2005, pp. 22–23). To map the number of records included and excluded in the scoping review process, a flow diagram was developed (see Figure 1) guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (Moher et al., 2009). Also the PRISMA checklist was completed for this review, but the study protocol was not registered as neither of these steps are normally part of the scoping review process. Flow diagram of search strategy.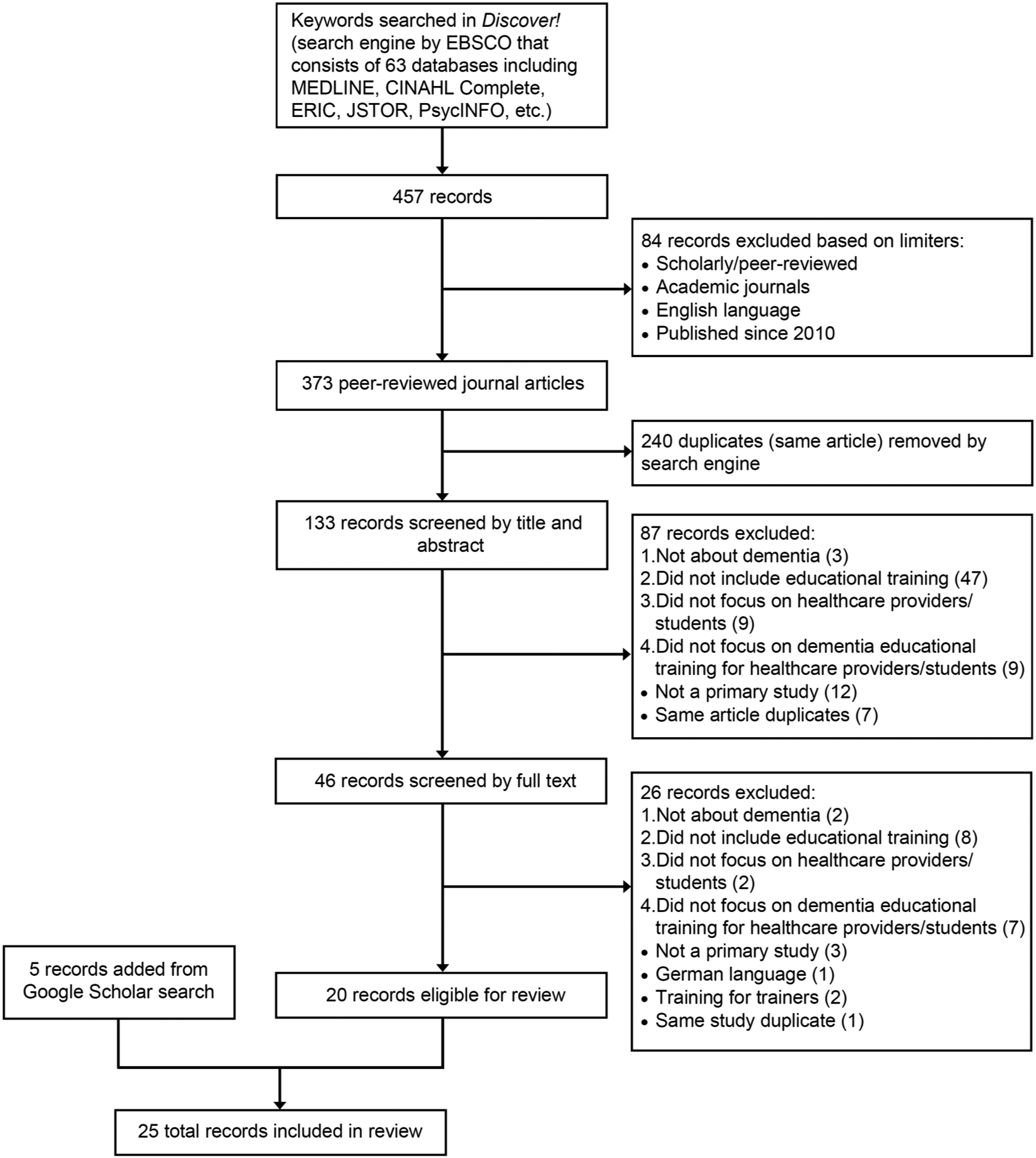
Stage 1: Identifying the research question or purpose
Identification of the research question or the purpose of the scoping review guides researchers in formulating a comprehensive search strategy (Arksey & O’Malley, 2005). The purpose of this scoping review was to synthesize evidence on DEPs for healthcare providers and students. Hence, the research question this scoping review addressed was: What is the existing and emerging evidence on dementia education programs (DEPs) for healthcare providers and students? A secondary question guiding our analysis was to what extent is culture addressed in DEPs for healthcare providers and students?
Stage 2: Identifying relevant studies
To identify relevant studies on DEPs for healthcare providers and students, the University librarian was consulted to develop a search strategy consisting of search terms, date range, and databases. As a result, the Discover! search engine was used in July 2021 to search 63 databases and results were found from the following: MEDLINE with Full Text, CINAHL Complete, Complementary Index, Academic Search Complete, APA PsycInfo, Biomedical Reference Collection: Comprehensive, ScienceDirect, Directory of Open Access Journals, ERIC, Teacher Reference Center, Business Source Complete, Digital Access to Scholarship at Harvard (DASH), SwePub, AGRIS, and IEEE Xplore Digital Library. Discover! automatically removes duplicates which is an important step in narrowing down results. Further, the automatic limiter to search only within the library holdings was removed to broaden the search further.
The search terms education or learning or teaching or training (as a Subject) were used and combined with dementia or Alzheimer’s (as a Subject) and “healthcare professionals” or “healthcare workers” or “healthcare providers” (in Abstract): SU (education or learning or teaching or training) AND SU (dementia or Alzheimer*) AND AB (“healthcare professional*” or “healthcare worker*” or “healthcare provider*”)
This search yielded 457 records. Then 84 records were excluded based on specific limiters: scholarly or peer-reviewed articles, peer-reviewed journals, English language, and published since 2010. This date range was chosen as scoping reviews focus on recent literature, that is, articles published within the past ten years. Applying these limiters resulted in 373 peer-reviewed journal articles. Through the duplicate (same article) feature of the search engine, 240 records were removed, yielding 133 records.
Stage 3: Selecting the studies
To select the studies related to the topic, inclusion and exclusion criteria were developed. The hierarchical inclusion criteria were: 1. Research study must be about dementia. 2. Research study must include educational training. 3. Research study must focus on healthcare providers and/or students. 4. Research must focus on DEPs for healthcare providers and/or students.
Exclusion criteria consisted of studies that were not primary studies (e.g., knowledge syntheses, abstracts, commentaries, letters, opinion papers, protocols, and frameworks) or not aimed at healthcare providers and/or students, or were the same article (i.e., duplicate) or a new article that reported on the same study already examined or included (i.e., same study duplicate).
The 133 records from title and abstract search were screened by one reviewer in consultation with two others. 87 records were excluded based on the inclusion and exclusion criteria: three were not about dementia; 47 did not include educational training; nine did not focus on healthcare providers or students; nine did not focus on DEPs; 12 were not primary studies (reviews, letter to editor, or preview of irrelevant articles); and seven were duplicates of the same article which the search engine did not remove in the previous step (e.g., author names not entered correctly in database). This yielded 46 records which were then screened by full text.
Full text screening of the 46 records by the first reviewer in consultation with the two additional reviewers, led to 26 additional records being excluded based on the inclusion and exclusion criteria: two were not about dementia; eight did not include educational training; two did not focus on healthcare providers or students; seven did not focus on DEPs for healthcare providers or students; three were not primary studies (protocol, reviews); one was in the German language; two focused on training the trainers; and one was a duplicate of a study already included. This resulted in 20 records eligible for the scoping review. A final search using Google Scholar in January 2023, yielded five additional articles that met the inclusion criteria and were either published after the initial search (4/5) or were excluded from the Discover! search as the journal is not fully indexed in major databases. As these records met the eligibility criteria, they were added, resulting in a total of 25 records for this scoping review. To ensure congruency, we also worked with the university librarian to run separate searches in Medline and CINAHL; the results for these databases in February 2024 using the same formula above were 109 and 87 respectively. The same search in Discover! resulted in 477 records from academic journals, providing assurance of its ability to identify relevant literature not only in Medline and CINAHL, but also in 61 others from which 24 of the 25 articles were drawn including ERIC, PsycInfo, Science Direct, Complementary Index, and Academic Search Complete.
Stage 4: Charting the data
Initially two reviewers read and extracted the data independently and then discussed and charted it. A third reviewer read and reviewed the chart, after which slight modifications were made. Finally, a fourth reviewer read and charted additional data alongside the third reviewer after it was decided to include more data on the evaluation procedures and tools. These final two reviewers also confirmed all earlier data in consultation with the initial two reviewers. After developing an initial data extraction table, the authors discussed the articles as a team to ensure the information for each study was complete and organized in a manner that would facilitate comparison. The information extracted for each study included the purpose, type of DEP, research design, major findings, and conclusions. This provided a comprehensive overview of the existing and emerging literature on DEPs for healthcare providers and students to analyze and categorize as a team.
Stage 5: Collating, summarizing, and reporting the results
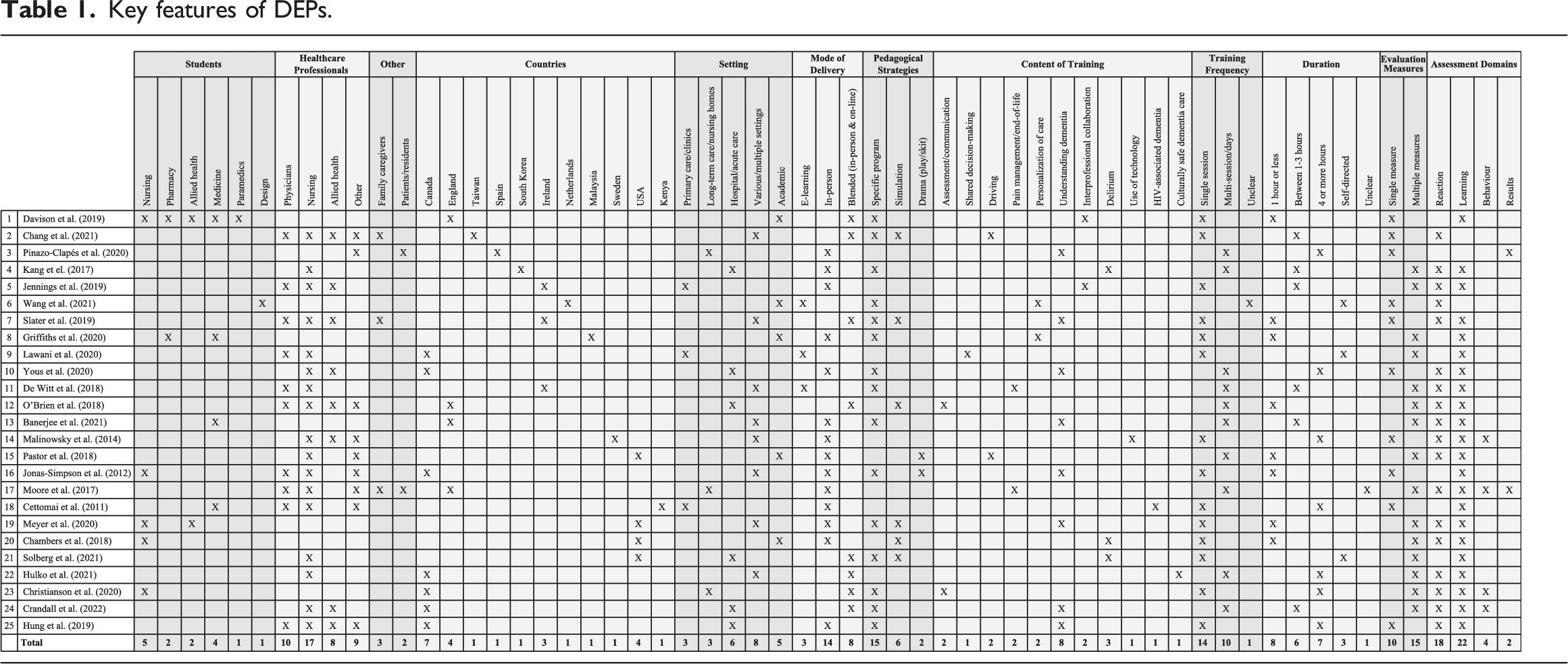
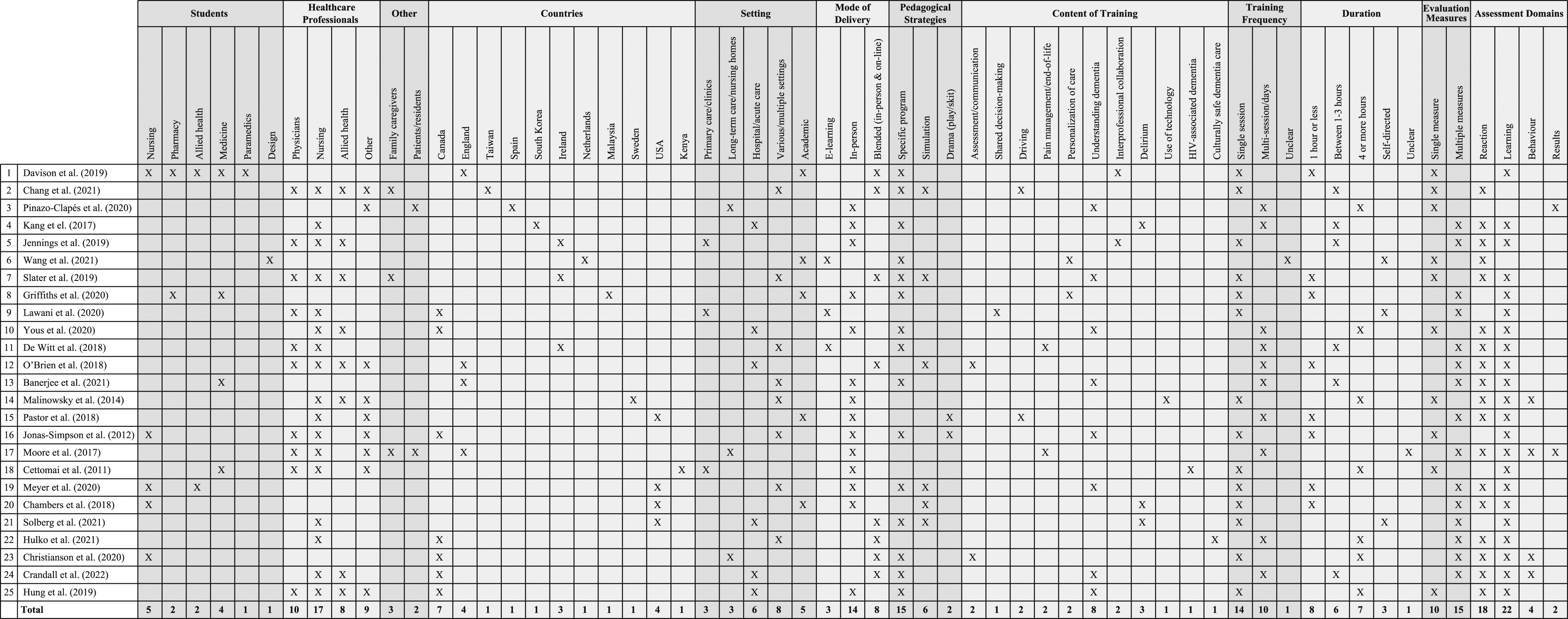
Key features of DEPs.
Results
Study characteristics
Of the 25 articles included in this scoping review, the majority (72%) were based on research conducted in one of four North American or British countries: Canada (28%), England (16%), the USA (16%), and Ireland (12%). The remainder (28%) were from: Kenya, Malaysia, The Netherlands, South Korea, Spain, Sweden, and Taiwan. The participants in DEPs were both healthcare students and providers, with many studies involving nursing students (16%), nursing staff (RN, LPN, HCA, NP) (64%) or both (Jonas-Simpson et al., 2012). The other healthcare professions represented amongst student participants in order of frequency were medicine, pharmacy and allied health (speech language pathology, occupational therapy, and physiotherapy), and paramedics. While nursing made up most provider participants, other disciplines in order of frequency were medicine (40%), other (e.g., activities/recreation coordinator, unspecified), and allied health (as above plus Social Work, Nutrition, and Music Therapy). Many studies had mixed samples of either health care students (12%) or health care providers (60%). The studies that did not have mixed populations (28%) involved only nursing staff (Hulko et al., 2021; Kang et al., 2017; Solberg et al., 2021), nursing students (Chambers et al., 2018; Christianson et al., 2021), medical students (Banerjee et al., 2021), and students studying design (Wang et al., 2021).
There were a range of work and/or educational settings represented in the literature, with acute care (24%) being more common than either primary care (12%) or long-term care (12%). It was more common for samples to include health care professionals working in a range of settings (32%) such as acute or long-term care and community care, rather than only one. Several studies reported on DEPs delivered to health care or other students in a university or other educational context (20%). Twelve percent of studies involved family care partners/‘befrienders’ and staff in their DEP intervention (Chang et al., 2021; Moore et al., 2017; Slater et al., 2019) and 8% assessed residents living in the care homes where the DEP was offered (Moore et al., 2017; Pinazo Clapés et al., 2020).
Characteristics of dementia education programs
More than half (56%) of the DEPs were one-off events such as an in-service or staff development session. The rest were multi-day sessions (40%), apart from one study that was unclear about the frequency (Wang et al., 2021). The Know-Me Toolkit was a 20-week design challenge to facilitate the personalization of dementia care; 16 Dutch students in a graduate design course each created toolkits for persons living with dementia in care homes with some of the students being able to test them remotely (Wang et al., 2021). Thirty-two percent of the single session DEPs were one hour or less in length, 24% were one to 3 hours in length, 28% lasted four or more hours, and others were self-directed (12%) or unclear (4%).
The multi-day sessions included a 20-hr. educational session offered in three weekly sessions of 4 hours each (Pinazo-Clapés et al., 2020), a 7-h delirium education program offered over three months with two 1.5-h workshops in the first month and a 50-min workshop in both months two and three (Kang et al., 2017), and Time for Dementia, a two-year long enhanced placement in which Medical students spent 2 hours every three months with a resident with dementia (Banerjee et al., 2021). One program – the Compassion Intervention - was a whole system intervention in two care homes with education sessions for formal and informal carers being one component; the sessions were developed by the Interdisciplinary Care Leader in consultation with staff and the total number and length varied based on identified learning needs (Moore et al., 2017).
In-person learning was the preferred method of instruction (56%), followed by a blend of in-person and on-line learning (32%), with solely e-learning (12%) being the least common. Specific programs were well represented in the literature (60%), including Gentle Persuasive Approaches (GPA) (Christianson et al., 2021; Crandall et al., 2022; Hung et al., 2019), Putting the PIECES Together (PIECES) (Yous et al., 2019), Dementia Friends (Davison et al., 2019), Dementia Detectives (Griffiths et al., 2020), and the Virtual Dementia Tour (Slater et al., 2019). More experiential or creative methods observed in the literature included simulations (24%) and plays (8%), with some being combined with specific programs and others being original productions (Jonas-Simpson et al., 2012).
Content of dementia education programs
The most common single topic overall was understanding (the experience of) dementia, including responsive behaviours (32%). Other general dementia care topics were inter-professional learning/collaboration (8%), assessment and communication (8%), and the personalization of dementia care (8%). There were a wide range of topics addressed in the DEPs, with seven specific ones being the focus of nearly half (44%) of the programs studied: the use of technology (Malinowsky et al., 2014), HIV-associated dementia (Cettomai et al., 2011), shared decision-making (Lawani et al., 2020), culturally safe dementia care (Hulko et al., 2021), pain management and end of life care (De Witt Jansen et al., 2018; Moore et al., 2017), dementia and driving (Chang et al., 2021; Pastor et al., 2018), and dementia and delirium (Chambers et al., 2018; Kang et al., 2017; Solberg et al., 2021). Only 8% of studies modified or developed educational materials to suit a particular cultural group (Chang et al., 2021; Hulko et al., 2021) and a further one determined the need for modifications to ensure cultural appropriateness (Griffiths et al., 2020). The other studies (88%) did not address culture at all.
Impact of dementia education programs
A wide variety of measurement tools and evaluation methods were used to assess the impact of the various DEPs with the focus being mainly on the health care provider and student participants. Exceptions were three studies involving family care partners or ‘befrienders’ in surveys, interviews, and/or assessments (Chang et al., 2021; Moore et al., 2017; Slater et al., 2019) and a fourth that assessed care home residents pre and post intervention to determine the DEP’s effectiveness (Pinazo Clapés et al., 2020), which Moore et al. (2017) also did along with their interviews and assessments of family care partners and staff.
Most of the measures were designed to assess the knowledge, attitudes, and skills related to dementia care that attendees possessed, with a total of 20 different tools being used and only five for more than one study. This includes the Sense of Confidence in Dementia Care Staff scale (SCIDs) (Schepers et al., 2012), the Knowledge Test or Multiple-Choice Questions (Advanced Gerontological Education [AGE] Inc., n.d) and the Self-Perceived Behavioural Management Self-Efficacy Profile (SBMSEP) (Schindel & Dupuis, 2005; Schindel et al., 2003) for two of the three evaluations of Gentle Persuasive Approaches (GPA) training for health care providers (Christianson et al., 2021; Crandall et al., 2022); and the Approaches to Dementia Questionnaire (ADQ) (Lintern & Woods, 1996) for two DEPs with health care providers (Banerjee et al., 2021; Hulko et al., 2021) that combined the ADQ with four to six additional tools. The three GPA studies made use of focus groups or interviews immediately after the training (Crandall et al., 2022; Hung et al., 2019) or six to eight weeks later (Christianson et al., 2021) and for Hung et al. (2019), this was their only measure. The Cummings Neuropsychiatric Inventory (NPI) was administered to care home residents in two studies in which the care home staff took part in DEPs (Moore et al., 2017; Pinazo-Clapes et al., 2020). These were the only two studies to assess the impact on residents/care provision.
Over half (60%) of the studies used multiple measures to assess the effectiveness of their DEP, ranging from 2 to 13 with a mean of 3.866 tools per study (median = 3, mode = 2). Moore et al. (2017) used assessment tools (three pre intervention and ten post), not to assess effectiveness of their Compassion Intervention, but to determine its feasibility. The study by Jennings and colleagues (2019) was a pilot of an interdisciplinary DEP. Time for Dementia (Banerjee et al., 2021) was evaluated through seven measures, six of which were administered pre-test, at 12 months, and at 24 months, and one (student satisfaction survey) that was completed after the placement. For the studies that employed only one measure (40%), the researchers administered a questionnaire (10%), feedback tool (20%), or individual or group interview (40%) following their educational session or used a pre- and post-test design and gathered data via questionnaires (Cettomai et al., 2011; Pinazo-Clapés et al., 2020) and focus groups (Jonas-Simpson et al., 2012).
More than half (60%) of the studies gathered data through focus groups and/or interviews. Of these, 60% also used standardized or self-developed questionnaires to assess knowledge, attitudes, and/or skills (Christianson et al., 2021; Crandall et al., 2022; De Witt Jansen et al., 2018; Hulko et al., 2021; Jennings et al., 2019; Kang et al., 2017; Lawani et al., 2020; Moore et al., 2017; Solberg et al., 2021), one used a feedback tool (Meyer et al., 2020), and 33.33% only used qualitative methods (Hung et al., 2019; Jonas-Simpson, 2012; Malinowski et al., 2014; Slater et al., 2019; Yous et al., 2019). Forty percent used only quantitative methods to measure outcomes of the DEP with half of these employing multiple measures, including more than one questionnaire (20%) or a combination of questionnaires and feedback tools (30%); and the rest used either a single feedback tool (20%) or questionnaire (30%). For example, O’Brien et al. (2018) paired the Confidence of Dementia Scale (CODE) with three additional measures they developed to assess their dementia communication skills course: Dementia Knowledge Test, ratings of video-taped simulations, and participant satisfaction survey. In terms of assessment domains, the overwhelming majority of studies on DEPs assessed reaction (72%) and/or learning (88%), with very few studies considering the domains of behaviour (16%) and results (8%).
Discussion
To understand the current educational landscape in dementia care and determine potential gaps, this scoping review explored the breadth of DEPs for healthcare providers and students, including attention to culture. Of the articles reviewed, it is clear there is importance placed on education and training related to appropriate dementia care; however, what and who to include/focus on for such education varies depending on the interests of the researchers.
Although the articles spanned 11 countries across both the Global North and Global South, North America and Europe featured prominently. This is similar to Surr and colleagues’ (2017) finding where the majority of the studies on DEPs they reviewed took place in the US and UK. While their sample was much larger, we found a wider breadth of countries and more Canadian content, as did Moehead et al. (2020) who reported 50% of their 46 studies as being from the US and UK, 17% from Australia, and 33% from a variety of other countries. There was a similar geographic spread for Williams and Daley’s (2021) scoping review of undergraduate DEPs though there were more DEPs in the US (56%) and Australia (22%) than in the UK (18.5%) and the only other country was Korea.
Both GPAR and P.I.E.C.E.S.TM are Canadian DEPs that are evidence-based and standardized (AGE Inc., 2021; Hamilton et al., 2020), while many other programs in this scoping review were created specifically for a research study or local population and very few were replicated. According to best practice for the delivery of DEPs, it is important they be offered in a consistent manner through accredited or certified trainers (Surr et al., 2017), involve persons living with dementia (Williams & Daley, 2021), and include ongoing coaching by interdisciplinary leaders or dementia champions to ensure sustainability in practice settings (Moehead et al., 2020; Moore et al., 2017).
While most of the DEP interventions included a variety of healthcare professionals and students, the majority involved nursing staff (RN, LPN, HCA), followed by Medicine, similar to the findings of previous knowledge syntheses (Surr et al., 2017; Williams & Daley, 2021). Nursing is the largest regulated health workforce (Boscart et al., 2019) and nursing staff provide most of the direct care for those who have dementia, regardless of practice setting (Office of the Seniors Advocate, 2020; Ontario Long Term Care Association, 2019). More than two-thirds of the studies in this review had mixed samples of health care providers and/or students, reflecting greater attention being paid to preparing students for the interdisciplinary nature of dementia care. Acute care featured more prominently than either long-term care or primary care which aligns with the spread of DEPs such as GPA and PIECES from long-term care to other practice sites along the care continuum.
The DEPs in our scoping review were split between single session events, mainly lasting 3 hours or less, and multi-day events. Best practice indicates that more sessions are better for consolidating knowledge, skills, and values (Surr et al., 2017). As most of the research in this review was conducted before the COVID-19 pandemic forced educators to switch to remote delivery, in-person delivery was found to be the preferred option. Blended learning options were described, with some noting flexible program delivery will be key for future DEPs. However, some programs are more amenable to this than others. For example, the GPA modules now can be separated into shorter sessions and delivered through a combination of on-line and in-person (AGE Inc., n.d; Crandall et al., 2022); DEPs using experiential or creative methods such as simulations and plays may be less amenable to flexibility in program delivery in terms of time and location, however.
Within this scoping review, the expansion of content beyond understanding dementia into other realms of life and experience reflects the growing awareness of persons with dementia as everyday citizens and neighbours (Nedlund et al., 2019; Ward et al., 2022), not only residents of long-term care homes. This includes bio-medical topics such as HIV-associated dementia and delirium, social aspects like driving and the use of technology, and concerted attention to family and culture in terms of dementia care and shared decision-making. Surprisingly though, very little cultural content was included in the DEPs developed, adapted and/or evaluated by the researchers. This supports other reviews focused specifically on DEP evaluation measures that identified the need for more attention to culture in future research (Mast et al., 2021; Resciniti et al., 2021).
We had hoped to learn more about the role of culture in DEPs given the breadth of countries represented and the considerable ethno-cultural and racial diversity in the UK, Canada, and the US where most of the research occurred. Only one study addressed culturally safe dementia care for Indigenous Elders (Hulko et al., 2021) and two focused on adapting educational materials or programs for Asian populations (Chang et al., 2021; Griffiths et al., 2020), with all being very recent. For example, Hulko and colleagues’ (2021) co-developed DEP with First Nation Elders was based on five indicators of cultural safety: (1) care must match the individual; (2) historical trauma; (3) understanding culture; (4) staying connected with family and community; and (5) relationship with the healthcare team. In contrast, the study by Chang et al. (2021) involved the translation of a DEP into Mandarin and they learned that adjusting the grammar, spelling, and terminology to be Taiwan-specific was needed to make it more culturally appropriate. Finally, Griffiths et al. (2020) made their DEP more culturally appropriate by including Malaysian family roles, names, and activities. All three studies showed positive impacts from their DEPs, while suggesting ways other DEPs could be more culturally appropriate and safe.
There was no research on DEPs focused on Black, Hispanic/Latinx or any other racialized or ethno-cultural minority groups, even though Black, Hispanic and Indigenous people have particularly high rates of dementia (ADI, 2022; Brewster et al., 2019; Kornblith et al., 2022; PHAC, 2019). This aligns with critiques of the suppression of Black and other non-white knowledges of dementia (Fletcher, 2021) and the corresponding overwhelming whiteness of dementia studies (Zubair, 2023). In other words, there is a gap between rhetoric and reality with researchers and policymakers acknowledging health and health care disparities and advocating for better training of care providers to address culture and cultural safety in dementia care, yet a paucity of DEPs actually doing this or calling into question the whiteness and Eurocentricity of our knowledge base in dementia education and practice.
The sheer number (n = 20) of different measurement tools used in DEPs aligns with other findings on the variety and large number of evaluation tools in use (Mast et al., 2021). There is clearly a need for a synthesis of measures used in DEPs that maps out which tools should be used for measuring the different domains and speaks to the psychometric properties of various tools. There is also a need for more standardization in the evaluation of programs, including researchers assessing the effects of the same program (e.g., GPA, PIECES, Dementia Friends, Virtual Dementia Tour) or those examining a similar domain (e.g., knowledge or attitudes about dementia), as emphasized by Resciniti et al. (2021). Earlier reviews of DEPs used the Kirkpatrick model for evaluation (Moehead et al., 2020; Surr et al., 2017), however; this model was not used in any of the studies in this scoping review. This model could be used for assessing the effectiveness of training as considering the higher levels of behavior and results would improve upon the near exclusive emphasis in DEPs on the lower levels of reaction and learning.
The findings on the content of DEPs resonate with those of Riesch et al. (2018) on the common topics in DEPs for nursing home staff, that is, person-centered care, communication strategies, and information about dementia; and extend their list of content to be developed by adding culture. This study differs from previous reviews on DEPs (Eggenberger et al., 2013; Moehead et al., 2020; Riesch et al., 2018; Surr et al., 2017; Zhao et al., 2021) in that students were included as well as providers working in a range of healthcare settings, and the content and format of DEPs, in addition to characteristics of the study and impact on learners, including evaluation measures and tools, were analyzed. Williams and Daley (2021) also focused on students and Riesch et al. (2018) paid attention to the content, as well delivery and evaluation methods, however the former did not include healthcare providers and was restricted to nursing home settings. Applying Kirkpatrick Partners’ (2022) four-level model and focusing on the practice change elements (behavior and results) in particular could assist researchers to produce high quality results which allow for the determination of effect size in meta-syntheses. This also would more accurately inform the design and delivery of DEPs and the provision of dementia care, assuring researchers and practitioners they can be confident in the results of studies (i.e., validity and reliability) to make health care decisions.
The dominance of quantitative methods was not found in this scoping review, unlike other systematic reviews (Mast et al., 2021; Resciniti et al., 2021) that only considered quantitative instruments, overlooking qualitative and mixed methods designs. Moehead’s et al. (2020) integrative review of web-based DEPs was more inclusive in that they considered a wide variety of research and non-research articles, yet found a lack of attention to translation to practice. Knowledge/attitudes is the primary focus of studies to date, with competency and practice change being overlooked, along with the role and influence of culture. Harto (2018) argued that while knowledge is important in dementia care, it is not enough; learners need to have the opportunity to put dementia knowledge into practice (see also Christianson et al., 2021; Riesch et al., 2018) and the longer-term effect of DEPs needs to be assessed.
There is a need to reconsider the format of education for health care students to allow for sustained exposure to persons living with dementia across the care continuum throughout their education. This could involve regular visits with persons living with dementia, as implemented by Banerjee et al. (2021), or supplementing first year placements in long-term care with a return to this practice area in an upper year. These are both ways of reinforcing the interaction between aging, culture, and dementia, which should be considered in the development and evaluation of future DEPs.
Limitations
Some studies met the inclusion criteria but did not discuss DEPs to the depth we sought. For example, Moore et al. (2017) was a feasibility study of the role of an Interdisciplinary Care Leader (ICL) and the cost of implementing the Compassion Intervention and omitted details on the education sessions the ICL delivered to staff and family care partners during the six-month intervention. Further, with the shift to remote delivery of education during the COVID-19 pandemic, some in-person programs discussed in this review may have developed on-line or hybrid modes of delivery which is not yet reflected in the literature. We did not include “student” as a search term, thus we may have missed articles about DEPs for non-health care professional students; this is unlikely though as our search strategy found a DEP for students studying design, which is not a healthcare profession.
One criterion in our initial search - ‘at least one abstract mention of population of interest (healthcare professionals, workers, or providers)’ - may have omitted relevant articles. Those articles referring only to staff, clinicians, professionals (with no mention of healthcare) or interprofessional teams in their abstracts would not have surfaced in our search results. Similarly, articles using ‘implementation science’ rather than ‘education’, ‘training’, ‘teaching’ or ‘learning’ would not have matched with our subject headings. Another limitation is that we included only articles published in English which may be why there was limited geographic spread and cultural representation across the studies. Finally, as scoping reviews only focus on the extant peer-reviewed literature and omit grey literature, this review does not address the full range of DEPs, only those that have been studied and published.
Conclusions
This scoping review shows that a wide variety of DEPs for health care students and practitioners are delivered and evaluated in different practice contexts, using numerous measurement tools. Future research should consider the impact of DEPs on performance (behavior) and the practice context (results), not only learners’ knowledge, attitudes and reactions, and whether or not a change in knowledge and attitudes leads to practice change – at individual and system levels – and how best to sustain knowledge use and practice shifts over time. There needs to be consistent education about dementia to ensure fidelity and quality dementia care. At the same time, it is also important to tailor education to local socio-cultural and geo-political contexts and settings.
While many DEPs use person-centred approaches, there continues to be a lack of focus on culture in relation to persons living with dementia and care models. Given the increasing diversity of aging societies across the globe, it is crucial that educators design programs that address ethno-racial diversity and prepare practitioners to deliver culturally safe care. A focus on culture - in terms of how ethno-racial background can affect views and experiences of dementia and disparities and implicit bias in dementia care - will ensure a more nuanced and deeper understanding, not only of care recipients, but also of care staff. While physicians, nurses, social workers and other professional care providers are mostly white (CDC, 2021), the majority of health care workers in assisting positions are immigrant and visible minority women (Statistics Canada, 2022); and the ethno-racial backgrounds of the latter, which may be the same as or similar to those of residents, are also not affirmed in DEPs. Making sure DEPs address culture and culturally safe care could ensure that health care practitioners are more prepared and/or encouraged to meet the cultural needs of persons living with dementia, irrespective of the involvement of families and communities.
Footnotes
Acknowledgements
We thank Erin Broughton for her assistance with the Prisma diagram (Figure) and tabulations and Katlyn Mellett for article searches when BSW practicum students.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Thompson Rivers University (Internal Research Fund and Research Accelerate Grant).