
Abstract
Metaphors to describe and understand dementia have been used in Western culture for many years. However, the ways in which people living with dementia and care partners use metaphors and symbols to illustrate and give meaning to their own experiences has been less understood. In this paper we explore the use of metaphor as methodology-- a way to support people living with dementia and their care partners in reflecting on and sharing their experiences of dementia. More specifically, drawing on our experiences using metaphor and symbols to map out the dementia journey from the perspectives of people living with dementia, care partners, and health and social care providers in Ontario, Canada, we describe our process of employing metaphor as methodology. We reflect on the use of metaphor as methodology through framing the dementia experience, exploring complexity, and representing multidimensionality. The use of metaphors has the potential to open space for new understandings of dementia.
Keywords
Receiving and living with a diagnosis of dementia is an experience of change and adaptation. Research studies have explored various aspects of the experience of dementia, including the onset of dementia and diagnosis, adapting to and living with a diagnosis of dementia, and maintaining continuity and a sense of self (ADI, 2022; Bunn et al., 2012; de Boer et al., 2007; Górska et al., 2018; Steeman et al., 2006; Vernooij-Dassen et al., 2006; Wolverson et al., 2016). Typically, these have been explored as discrete events, rather than as part of the overall experience of dementia over time. The research that does exist demonstrates the complexity and fluidity of dementia experiences and responses over time (Górska et al., 2018; Harman & Clare, 2006). In the last decade, some people have started to refer to the experience of dementia as the dementia journey (McDonald, 2019; Minghella & Schneider, 2012; Smith & Phillipson, 2022).
Seeking out a diagnosis is often precipitated by a significant event or “tipping point”, followed by a long period of tests, specialist visits, and waiting for a diagnosis (Bunn et al., 2012; Castaño, 2020). Throughout the diagnosis period, common responses from people with dementia include denial, emotional responses such as feelings of loss and sorrow, insecurity, uncertainty, disbelief, shock, anger and frustration, and positive or accepting responses (Aminzadeh et al., 2007; Bunn et al., 2012; de Boer et al., 2007; Pearce et al., 2002). Often related to the stigma associated with dementia and responses of others, people living with dementia also report feeling embarrassed, humiliated, and inadequate, and are often excluded and dismissed, leaving them feeling lonely and isolated (ADI, 2019; de Boer et al., 2007). While receiving a diagnosis of dementia can be emotional and challenging (Aminzadeh et al., 2007; Pratt & Wilkinson, 2003), many people with dementia and their care partners are forced to come to some level of acceptance and get on with living their lives--what some people with dementia call their “new normal” (Bunn et al., 2012; de Boer et al., 2007; Wolverson et al., 2016). Many, in fact, find some relief from knowing what is happening to them, acknowledging their challenges, working through conflicts to accommodate a diagnosis, and developing strategies and resources together with their families and support systems in order to adapt (Bunn et al., 2012; Górska et al., 2018; Robinson et al., 2005). While many people are aware of the forthcoming cognitive decline with their diagnosis, they find creative ways to negotiate the changes they are experiencing (Bellass et al., 2019; Górska et al., 2018; Harman & Clare, 2006; Robinson et al., 2005).
Research on the experiences of dementia has tended to focus on individual groups and perspectives, with the majority of the literature focused on the experiences of family care partners (e.g., Cabote et al., 2015; Ivey et al., 2013; McDonald et al., 2017; Svanberg et al., 2011; Teel & Carson, 2003). This occurs despite the fact that dementia experiences and care are inherently relational, involving the person living with dementia and their informal and formal carers (Mitchell et al., 2020; Nolan et al., 2002, 2004). Further, much of the existing research fails to consider the social, cultural, and physical contextual factors that can shape dementia experiences, “[largely reflecting] the view of a person with dementia as a closed system, isolated from [their] environment” (Górska et al., 2018, p. e192). In a meta-synthesis of qualitative research on the lived experience of dementia, Górska et al. (2018) found that characteristics of interpersonal relationships, the physical environment, and the socio-cultural environment all intersect to shape the experiences of dementia in profound ways. In particular, caring, accepting, non-stigmatising social contexts, and supportive social networks can assist people to accept their diagnosis, face it in a more positive way, and live well with dementia (Clare et al., 2008; Litherland & Williamson, 2013; Mason et al., 2005; Menne et al., 2002). On the contrary, over-protective, patronizing, disrespectful, and insufficient support can impact experiences in negative and harmful ways (Kitwood, 1997).
This conceptualisation of dementia is consistent with Kitwood’s (1997) articulation of the malignant social psychology of experiences of dementia, that includes the range of actions that can threaten the personhood of people living with dementia. However, Kitwood’s malignant social psychology has been critiqued for its failure to consider the broader cultural, structural, and political contexts within which people living with dementia and their families are embedded (Adams, 2005; Gilliard et al., 2005). A more social relational perspective focuses on the importance of all relationships, including interpersonal, socio-cultural and socio-political, in shaping experiences of dementia (Jonas-Simpson et al., 2021; Kontos et al., 2017), often leading to marginalisation and oppression. It is this relational ontology (Gergen, 2009, 2015) and social relational perspective that guided our decision-making throughout our research.
Metaphors and dementia: From representation to methodology
Moser (2000) describes metaphors as “analogies which allow us to map one experience in the terminology of another experience and thus to acquire an understanding of complex topics or new situations” (p. 3). Metaphors help us make sense of the world and our experiences in it, particularly when those experiences are new or unfamiliar, and also provide us with a means to communicate our experiences to others (Castaño, 2020; Lakoff & Johnson, 1980, 1999; Stoddard Holmes, 2011; Zeilig, 2014). Lakoff and Johnson (1980) explain that a metaphor cannot be “comprehended or even adequately represented independently of its experiential basis” (1980, p. 19) describing how metaphors are always interpreted individually thus providing extensive pedagogical possibilities (see Sameshima, 2006). As an instrument to promote self-reflection, and to reflect and communicate about complex topics and experiences, metaphors have long been used to describe experiences of illness, including dementia (Bleakley, 2017; Castaño, 2020; Sontag, 1990; Wohlmann, 2022). In fact, metaphors and symbols to describe and understand dementia and dementia experiences have been used in Western culture for many years (Zeilig, 2014).
Metaphors are complex and don’t necessarily have positive or negative consequences; their value, rather, lies in how they are used. Metaphors can have negative and harmful consequences (see Sontag’s 1990 analysis of the dangers of metaphor, as an example), as well as more positive and transformative implications (Stoddard Holmes, 2011). For instance, Wohlmann (2022) suggested that the use of metaphors in illness can be complex, and while some metaphors may seem limiting or negative, they can also be given new meanings by those experiencing the illness or disease. Most often, metaphors associated with dementia and dementia experiences have been created and used by people and organisations who do not have lived experience of dementia, such as the media, government, and healthcare and Alzheimer organisations, rather than being created and used by persons with lived experience. These outside-made metaphors become common lexicon in Western culture (Zeilig, 2014, 2015), and thus “[people living with illness] have always had limited influence on (also limited) stock of public metaphors that shape their own care [and experiences]” (Stoddard Holmes, 2011, p. 266).
Most research on the use of metaphor in the dementia context has focused on and illuminated the stigmatizing nature of these metaphors. For example, dementia is often referred to with negative or frightening metaphors, such as a ‘wave’, ‘tsunami’, and ‘rising tide’ (Zeilig, 2014) or with war imagery, such as a ‘crusade’ or the ‘war on Alzheimer’s’ (Swinnen & Schweda, 2015). Dementia is also often associated with older people (Zeilig, 2015), and is portrayed as “. . . a complex, unknowable world of doom, aging and a fate worse than death” (Zeilig, 2015, p. 17). People living with dementia are often described by their losses (Zeilig, 2015) as well as by their behaviours (e.g., wanderer, feeder) (Dupuis et al., 2012; Paterniti, 2003) and by metaphors that conjure up images of “the zombie”, “the living dead” and “the monster in the mind” (Behuniak, 2011; Mitchell et al., 2013, 2020). These metaphors create a picture of dementia as one of tragedy and loss, causing much fear for people with and without a diagnosis of dementia (Mitchell et al., 2013, 2020). Additionally, these stigma-laden metaphors are perpetuated and typically used by people without a diagnosis of dementia to describe someone with dementia (Zimmerman, 2017a). Given the potential for harm and suffering, Sontag (1990) called for the elimination of metaphor in the illness context, stating: “the most truthful way of regarding illness – and the healthiest way of being ill – is one most purified of, most resistant to, metaphoric thinking (p. 3). Others, however, suggest that metaphors can be helpful in communicating and can enhance deeper understanding of the illness experience (Bleakley, 2017; Stoddard Holmes, 2011; Wohlmann, 2022). In the education field, metaphors have been indispensable to transformational learning, particularly when strong connections in the metaphor can be made “between the sensory and the conceptual, and which offer comparisons that hold under extension” (Tsun Haggarty & Sameshima, 2023, p. 3).
Despite the complexity and cognitive nature of using metaphors (Sopory, 2017), people living with dementia frequently use metaphors to describe and make meaning of their experiences. A more recent and much smaller body of research has begun exploring the use of metaphors by people living with dementia and their carers from texts (Zimmerman, 2017a, 2017b) and blogs (Castaño, 2020). This research suggests that similar to people experiencing other illnesses, people living with dementia use a range of conventional metaphors to describe their experiences, including descriptors such as death sentence, game, war, roller coaster, secret, and loss, robbery and transformation metaphors (Castaño, 2020). Although similar metaphors are used by carers, the metaphors are often deployed differently compared to persons living with dementia (Zimmerman, 2017a, 2017b). One of the most common metaphors used by people living with dementia and their care partners is the journey metaphor (Castaño, 2020; Zimmerman, 2017a, 2017b). The metaphor of a journey has been used often in health writing, and can give narrative shape to one’s experiences of illness (Wohlmann, 2022). The metaphor of a journey has been used throughout a variety of illness experiences, including chronic pain (Declercq et al., 2023), cancer (Hommerberg et al., 2020; Sopory, 2017), and dementia (Castaño, 2020; Smith & Phillipson, 2022; Zimmerman, 2017a). Research focused on the lived experience of illness, including dementia, demonstrates the complexities of metaphor, and the many ways metaphors can be used with both negative and positive implications (Hansen, 2018). In addition to the potential for harm and suffering caused by their use, metaphors have also been found to enhance communication between health-care providers and their patients (Appleton & Flynn, 2014; Casarett et al., 2010; Gallagher et al., 2013), can have a visual component that can be helpful in both comprehending and sharing experiences, help people to “recreate a sense of continuity … [by providing] a transforming bridge between the image of the old life and the new one” (Becker, 1997, p. 60), help structure complex experiences (Moser, 2000), and when paired with narrative, “allow us to piece fragments of information together into a cohesive whole” (Baugher, 2015, p. 215). Related to the use of the journey as metaphor more specifically, Minghella and Schneider (2012) emphasise: The critical premise of a journey is that there are some common predictable elements (or phases), which enable planning and prevention for the people living with dementia, commissioners and providers of services. Helping people living with dementia understand that journey, working with them to manage it and providing critical interventions proactively are all likely to improve experiences, prevent crises and target resources more efficiently and effectively. (p. 129)
Further, using metaphor as a heuristic device with people living with dementia can help them “restructure the framing of the issue in focus and open up new ways of conceiving it, thereby providing a basis for those involved to tell alternative stories and create a new identity” (Hansen, 2018, p. 7). When coherent narratives break down, the use of metaphors can provide important insights into people’s experiences. As Kruger (2015) stated, “It could be argued, then, that fear of dementia is linked to the way the disease challenges the coherent narrative—the unimaginable terror of an existence without ‘story’—and the implied chaos this brings, the inevitable break between soul and body” (p. 123). For these reasons, other researchers have sought an expanded understanding of metaphor in illness situations, always being aware of their potential harm while recognizing the power metaphor holds in supporting the sharing of experiences and for transformation (Hansen, 2018; Stoddard Holmes, 2011). Wohlmann (2022), for example, suggests that metaphors be evaluated based on their adequacy, their ability to explain or describe an experience, and their effects particularly as it relates to empowerment and liberation.
To sum up, much of the existing research on metaphor and dementia focuses on metaphor as representations of dementia and people living with it. What is most interesting to us, is that we could find little research that has used metaphor as a methodology and a research device to support the telling of one’s story in the dementia context. Recognizing the relational nature of the dementia experience, the purpose of our larger project was to use one of the most commonly used metaphors by people living with dementia and their carers, the journey metaphor, as methodology to “map the dementia journey” from the perspectives and experiences of people living with dementia, care partners, and health service providers in Ontario, Canada. Our ultimate goal was to provide a frame of the dementia experience trajectory for service providers to better support people living with dementia and their care partners in more proactive ways. The purpose of this paper is to share our process of using metaphor as a research strategy for exploring experiences of dementia. We were drawn to the metaphor of the journey because it recognises that experiences of illness are never stable, but shift over time depending on changing contexts, requiring more flexible and adaptable policies and practices. Also, we were interested in how the intentional use of metaphor might support people living with dementia in reflecting on and sharing their experiences of dementia over time, and ultimately provide a common language and enhance communication between people living with dementia, families, and health care providers (Hommerberg et al., 2020).
Methodology and methods
Participant characteristics.
Participants and participant recruitment
Three local organizations that work with people living with dementia and their families agreed to support the research and assist with identifying and recruiting people living with dementia, family carers, and health and social care providers. At each of these three organizations, our primary contacts gave people the information about the study and asked if they would like to attend a focus group. Those indicating an interest were provided with an information letter about the study and were asked to sign a declaration of informed consent. Dates and times were then set up for the focus groups. The study was approved by two university Research Ethics boards prior to data collection (Lakehead University and the University of Waterloo). Because our partnering organizations were familiar with the participants, people living with dementia who were invited to the study were able to provide their own consent to participate during the recruitment phase as well as at the beginning and during the focus groups, consistent with process consent recommended when working with people living with dementia (Dewing, 2007, 2008). These organisations were also prepared to provide support to people living with dementia should it be needed following the study; however, there were no instances where this was needed.
The people living with dementia who consented to participate in the project were generally in early phases of the dementia journey and able to give informed consent to participate in the research. They had been diagnosed between one and over 10 years prior with most living with dementia for over 2 years. One person living with dementia was living independently and all others were living with their family care partners. In order to capture both earlier and later phases of the dementia journey, we tried to recruit care partners who were caring for people across the dementia journey, including those supporting someone still living in the community and those who were caring for someone with more advanced dementia living in long-term care homes. Two care partners were caring for someone living in a long-term care home, and the remainder of care partners were caring for someone living in the community. Six care partners were men, five of whom were caring for their wives and one caring for his mother-in-law. Eighteen care partners were women, with 17 women caring for their husbands and one daughter caring for her mother. Finally, the health and social care providers worked across the spectrum of dementia care. These health and social care providers worked in community and long-term care settings to support people with dementia, including home care, psychogeriatric services, long-term care homes, and non-profit charitable organizations (Table 1).
Data collection
Focus groups were conducted separately with the different participant groups (i.e., persons living with dementia, care partners, health and social care providers) in three locations in Ontario, two in southern Ontario and one in northern Ontario. These locations were chosen to capture experiences of people living with dementia in different parts of the province and because of their proximity to the researchers who had existing relationships with organizations who assisted with participant recruitment. Given the number of family members interested in participating and the need to keep the focus groups small, our goal was to conduct four focus groups in each location — one with people living with dementia, two with care partners, and one with health and social care providers. However, in one site only one participant was available for one of the focus groups, and we conducted an interview with this person. In total, 11 focus groups, each between four and eight participants, and one interview were conducted. All focus groups and the interview were audio-recorded with permission from the participants. The focus groups and interview lasted on average about 2 hours with a break mid-way. Although we did not anticipate that the focus groups would last this long, participants had much to share about their experiences and were eager to hear about others’ experiences and perspectives; they remained actively engaged throughout the focus groups, including our participants living with dementia.
Below we describe our metaphor as methodology process in more detail, including each of the steps of our process, and some of the challenges of data analysis and how we approached our analysis. In particular, we focus on how metaphors were used in our methodology and detail the benefits of using metaphors as methodology.
Methodological reflections: Metaphor as methodology process
We used metaphors in three different ways throughout this project. First, we used metaphors to
Framing the experience through data collection
We used the metaphor of the dementia journey to help frame the experience for participants and to give them visual and metaphorical cues to assist in telling their stories. The intent of using metaphorical and visual data was for the following: using visual prompts to develop rapport; initiating storytelling; and capturing stories. We describe each of these below, using quotes from our focus groups to provide examples from our process on how we achieved this.
Using visual prompts to develop rapport
To provide engagement in the focus groups, build rapport, and create a safe space for sharing, participants in all focus groups (i.e., people living with dementia, care partners, health and social care providers) were first invited to choose a vehicle from the range of die-cast collectible and toy vehicles provided that best reflected their personality or their dementia journey. Once they had chosen a vehicle, they were asked to introduce themselves to the rest of the group by sharing the vehicle they chose, why they chose that vehicle, and what they most wanted people to know about them. The car selections were used as an ice-breaker to facilitate introductions and to help participants to begin to think about the metaphor of the journey. The use of objects such as the toy vehicles opened space for people to share their stories in a fun way. The use of visual and tactile prompts is a common method in facilitating discussion, supporting the telling of stories and reminiscing with people living with dementia (McLeod et al., 2021). The use of concrete artifacts allows for empirical examinations and reference points for symbolic interpretation (Sameshima, 2019). We tried this strategy with two initial focus groups of people living with dementia and care partners and found that the use of the cars initiated conversations about memories of cars and travelling, and seemed to provide delight and laughter among participants, creating the safe space needed for collaborative sharing and dialogue. As evidenced by the below quotes, the use of visual and tactile items prompted significant discussion.
Many of the participants chose a vehicle that represented something about their dementia journey. For example, a person living with dementia chose a bright shiny car and talked about her lack of ability to drive anymore: ‘Well, I picked this one because it’s bright and shiny and I can’t drive anymore, so this one – which is a very nice car – I dream of having if I ever get back to driving. That’s why I picked that one.” (Community #1, focus group with people with dementia, P3). A care partner chose a car that reminded her of her youth, and opened the space for her to talk about the changes in her life since her spouse was diagnosed with dementia: …this car reminds me of my youth in the 50’s. I never had a car like that, but I wouldn’t have minded [one]. Elegant and expensive, and that’s why I picked it, really. I don’t know much about cars myself and unfortunately I’m learning about them because my husband doesn’t drive any longer. And I think that was probably the hardest thing for him to accept and also for me, because it took me at least two years to feel comfortable behind the wheel… (Community #3, focus group with early care partners, P4)
Another care partner chose a camper, stating: “I chose a camper because we’re on a journey. We don’t know where we’re going, lots of baggage. But also there’s another element of, there’s a certain amount of freedom. We don’t have a schedule, I guess.” (Community #1, focus group with later care partners, P2). And finally, a health service provider chose a taxi because of the relational nature of her job and how it reflected the ways she was able to help people get to the places they wanted to go: “… when I saw taxi, I said – okay, I can help some people to get to the places they want.” (Community #1, focus group with health service providers, P6).
By anchoring participants’ experiences to a visual object particularly at the start of the focus group, they were able to begin to share salient aspects of their journey and themselves with the other participants. During this process, participants affirmed each other and often responded to others’ sharing.
Initiating storytelling by visualising the whole
Once everyone had introduced themselves, we shifted to more directly exploring the dementia journey as a whole. We wanted to use this part of the process to identify key timepoints along the journey. We asked participants to reflect back over their entire journey thus far, or on their journey supporting people living with dementia and their care partners, and describe some of the key things that had happened along their journey, what the significant moments were in their journey, and why these moments were significant for them? We started by asking people about the beginning of their journey. We did not provide starting or ending points, but rather asked participants to tell us what their starting or ending points were. As we invited people to share their story, we captured key points on sticky notes to add to the canvas that laid across the table. We continually asked participants to clarify, to review what we had summarized, and where the points should be placed on the blank canvas. We began to capture these key moments on the road mapped out on the canvas, to begin to build the skeleton of the journey as described by people living with dementia, family members, and professionals.
By using this strategy, we were able to determine how participants viewed different parts of the journey. For example, participants talked at length about the beginning of their dementia journeys, which often started long before the diagnosis. In fact, many participants described incidents prior to diagnosis which they described as the start of their journey: And about three years ago – first of all, I was a licensed practical nurse, and about three years ago I started to take bus trips around the city and getting lost. I’d forget where I was going. So I went home and I started to think about it for awhile. I discussed it with my daughter – oh Mom, you’re just growing old. So I had a lady doctor that was very kind, very considerate. And I said to her – you know, I think I’m slipping. So she contacted [a service organization], and they came and they talked to me. And I met a very nice gentleman by the name of Dr. X. at the [health clinic] and he tested me again – nothing with machinery, just verbal – and came to the conclusion that I was in the early stages of Alzheimer’s. (Community #1, focus group with people with dementia, P1)
By asking participants about how they might use the space of the blank canvas to reflect those key moments along their journeys, we were able to better understand how they viewed different timepoints along the journey: Researcher: I’m interested in how you would sort of imagine the stages or if there are stages. We’re trying to map the journey and I think that if I can sort of imagine – here is sort of the beginning and what do you imagine this at the future or the end? What’s in the middle? I think you talked about that you wanted to call that area sort of adjustment. And would you call that diagnosis a space - a stage of some sort? How do you imagine breaking up the space? Care Partner1: It’s a critical point. Care Partner2: The diagnosis is certainly a critical point. Care Partner3: Yeah, I think so. Care Partner2: You have to face facts. (Community #1, focus group with later care partners)
In another example, the metaphor of the journey helped care partners to differentiate the diagnosis from the start of the dementia journey, what one carer partner called the “spotting trouble” phase: Researcher: So is that what you would call the first part? Care Partner 1: No, absolutely not. No. You’re spotting trouble. Care Partner 2: And being really upset about it too. I think that’s – there’s denial; there’s all kinds of things that go on. (Community #1, focus group with later care partners)
Capturing the details of stories
Once we had started to capture a sense of the key moments or points along the journey, we then used guiding questions to delve more deeply into each phase of the dementia journey, starting with the beginning of the dementia journey, moving to the diagnosis process and immediately following the diagnosis, and continuing along the journey to where they were currently at in their journey. We used common road signs to help participants to detail their stories, including how they felt at different points along the journey. For each of the key points along the journey identified, we asked participants to choose, from a broad range of common road signs, the sign(s) they felt best represented that aspect of the journey. We then asked them to describe how the road sign reflected that aspect of the journey and what the road looked like for them at that point. As participants talked, the researchers worked with the participants to sketch out the road and capture key details about that moment in time (see Figure 1). An example of one of the canvases.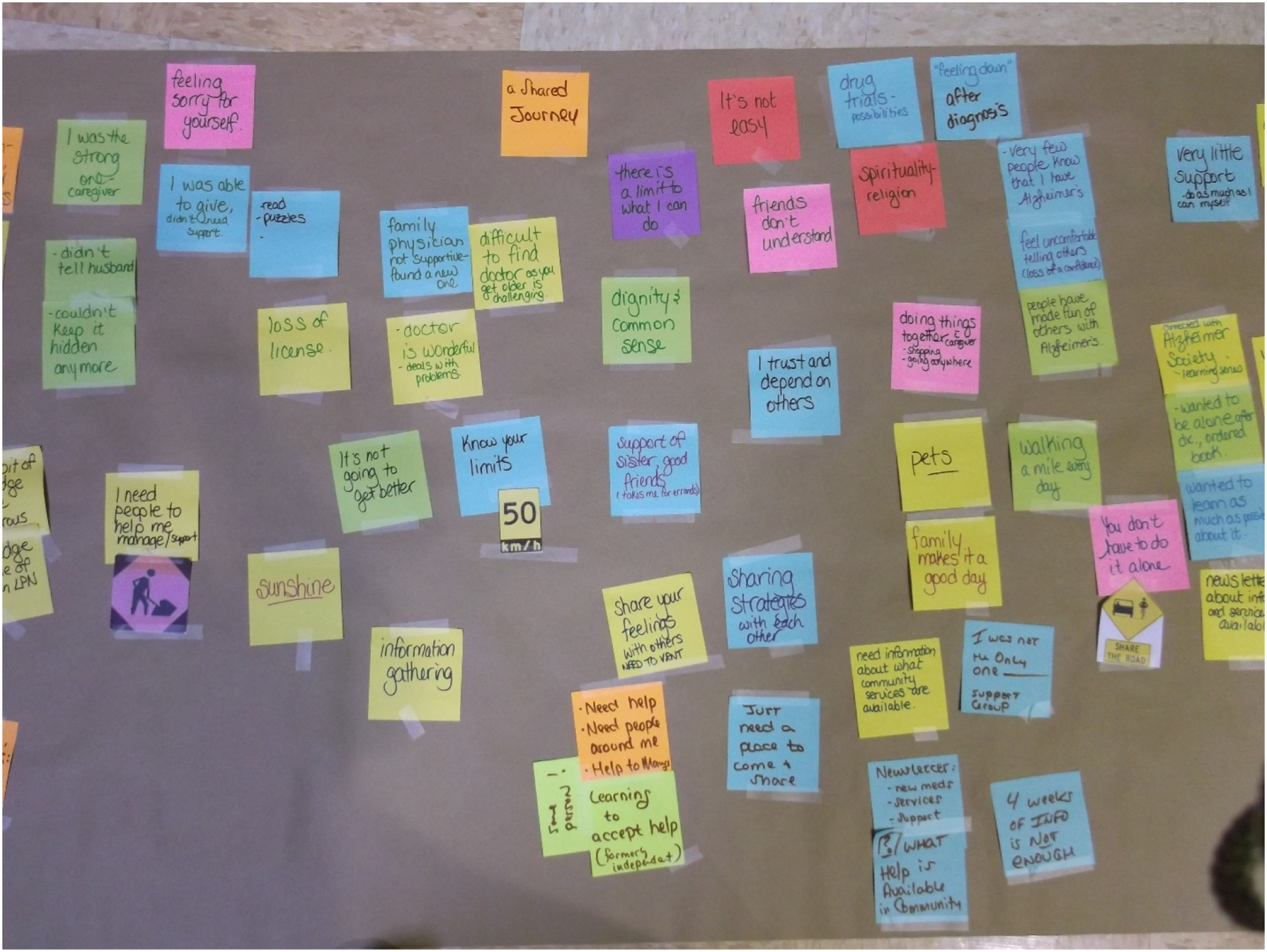
The use of road signs enabled participants to use metaphor in a different way to describe parts of their experiences with dementia, bringing about different discussions about their experiences. For example, in one focus group with people living with dementia, when asked what road sign(s) they associated with their experiences prior to diagnosis, one person living with dementia stated, “I think that slippery one there” (Community #2, focus group with people with dementia, P5), to which a second person with dementia responded, “Yeah, because you’re sliding around and not sure what’s going on.” (Community #2, focus group with people with dementia, P2).
When discussing the diagnosis of dementia, one care partner shared, “I think for me, it’s like going down the road and it forks off in two directions and you don’t know which one to take. I think that’s what it is for me.” (Community #1, Focus group with early care partners, P1). This participant continued, “For me, it would be after that – after you find at the fork in the road that you’ve got to change… I think it would be after the diagnosis for me, because that certainly makes a detour in your life. You’re going down a road now you never expected to go down.” Another care partner stated in response, “I think construction, because we’re redefining our life.” (P2).
When people living with dementia moved to discuss their present lives, one person living with dementia stated that a “share the road” sign was most appropriate “this one here – Share the Road” to which another person with dementia replied: “So as we can see, we’re all three on the same journey, so we’re sharing the road.” (Community #1, focus group with people with dementia, P1 & P3). Another participant living with dementia stated, “You asked for a road sign. I probably would go for a construction, okay? I need help. I need lots of people around me to get me out of this or have to manage the best I can.” (Community #1, focus group with people with dementia, P3). Another person with dementia discussed how important it was for her to have a safe place to share her feelings about her diagnosis, and labelled it as a rocky road: “And then probably get ready for a rocky road… Even then, you are not alone. Even then on the rocky road, you are not alone. (Community #1, focus group with people with dementia, P2).
The use of the road signs thus demonstrated both the similarities and the uniqueness of individual experiences, with some participants identifying road signs (e.g., the construction zone) reflecting their experiences at one point along the journey and another identifying the same road sign at a different point along the journey. The roads signs helped participants to reflect, delve more deeply, and explain further what different experiences along the journey were like, and connect them to other points along the journey. The road signs also helped to illuminate the similarities and differences within their own journey and between their journey and others’ journeys.
Interpreting metaphors as data in data analysis
We engaged with metaphors throughout the data analysis process in combination with the transcripts of the audio recorded interviews. In this section, we describe our analysis process and how we embedded metaphors in different parts of our analysis process. Finally, we explored, revised, and refined the maps with a broader group of participants in a face-to-face analysis process to help create a consolidated map of the dementia experience.
Analyzing individual maps and transcripts for common themes and symbols
At this stage, we were engaging primarily with the metaphors and symbols of the dementia journey shared during our data collection phase. We analyzed both the visual (road maps) and the textual (transcripts of audio-recorded focus groups/interview) data both separately and together. Data were analyzed drawing on an adapted constant comparative method (Charmaz, 2006). More specifically, in initial coding, we began by analyzing each separate road map. For each critical point along the way, we summarised the signs and key patterns emerging for each participant group separately. At this stage, we did a preliminary search for common patterns, road signs, and symbols within each road map and across the different road maps. We then conducted a comparison within each of the road maps as well as across the different road maps for each group to begin to identify differences in the road maps that reflected differences in experiences.
Once this was done, we turned to the textual data. All audio files of the focus groups and the interview were transcribed verbatim, and entered into the qualitative software program NVivo10. Initial, line-by-line coding of each individual transcript was conducted. From there, a more focused coding process involved identifying the most salient codes, comparing the codes, grouping related codes together into broader themes, comparing the broader themes across the different groups, and beginning to build what we came to call the experiential paths. We then compared our analysis of the textual data from the transcripts with the analysis of the visual data from the road maps with a focus on identifying, further developing, and clarifying the sub-paths within each of the larger experiential paths of the journey and the themes associated with those sub-paths. At this stage, we also explored what else might have been missed on the visual maps from the mapping exercise.
Representing the road maps of different participant groups
After analyzing the individual focus group/interview maps and transcripts, we then began to consolidate the maps based on participant groups—people living with dementia, care partners caring for someone in the community, care partners caring for someone in a long-term care home, and health and social care providers. Through this process, we aimed to understand and consolidate the key features of the journeys and similarities and differences between the groups’ journeys and experiences. This step also involved analyzing the relationships between the experiential paths developed during focused coding for each group to explore how some or all of the experiential paths worked together in an overall representation of the dementia journey for the separate groups. The maps were summarized, detailed notes were made as the maps were compared across groups and communities, and consolidated maps representing the different journeys were then created for each group. In particular, where common road signs might have been used by different focus groups, we ensured that these were used on the consolidated maps. These experiential paths were then compared against some of the key findings from the analysis of the individual maps to ensure that the data analyses were consistent with and captured all the key aspects of the journey shared. Keeping to the metaphor of the journey used in the focus groups and interview, these consolidated maps (four of them representing people living with dementia, early care partners, later care partners, and health and social service providers) were presented as roads with road signs identifying key points along the dementia journey. Finally, we returned to the data to identify quotes and stories in the transcripts that illustrated the key points along the dementia journey for each group.
Exploring, refining, and revising the consolidated maps
Once all the focus groups and the individual interview were conducted, initial and focused coding were completed on the focus group/interview data, and the drafts of the consolidated maps for each of the groups had been finalised, some of the original participants along with other individuals were invited to a one-day workshop in Toronto, Ontario. Two of the key objectives of the workshop were to: provide an opportunity to reflect on the journeys created in the focus groups/interview data and some of the emerging key findings; and build on the dementia journey maps by identifying key supports and resources needed along the journey.
Participants were divided into the groups that they represented and were asked to explore that particular map. For example, people living with dementia explored the consolidated map of people with dementia’s experiences. People were asked to participate in a series of activities in their small groups focused on their particular map. First, people were asked to reflect on the map and reflect on the following questions: What did they think about it? How did it represent, or not, their experiences? What was missing? Second, participants were asked to read exemplar quotes from the transcripts, place them where they felt they fit on the consolidated map, and to discuss what they thought was really going on and what the quote told them about that particular part of the dementia journey. People were then asked to identify resources and supports needed to help navigate each point along the dementia journey. Finally, participants were asked to consider and discuss how the maps might be used to better support people living with dementia and their family members.
Details from the small group discussions were captured by note takers. At the end of the workshop, we had both the documented notes from each of the small group discussions as well as the visual representations of the maps of the dementia journey, with the changes, missing pieces, quotes from the transcripts, and the supports and resources added to the maps. This process was invaluable in opening up reflection and dialogue on the dementia experience more broadly, demonstrating the complexity of the experience for the different groups involved, and identifying supports and resources needed at different points along the dementia journey. The process also illuminated the limitations of the maps. The insights from participants led us to re-analyze and rethink our ways of presenting the data. For example, we recognized that the maps may not capture all of the minute elements of people’s journeys with dementia and may not represent different groups such as people living with young onset dementia. The discussion also highlighted the inadequacies of a two-dimensional map, leaving us to think more deeply about how we might capture the complexities of the dementia experience. Following the workshop, any changes and additions made to the maps and all notes taken during the workshop were then compared with the original maps and findings, and revisions made accordingly (Figure 2). Example of the revised consolidated map from workshop participants.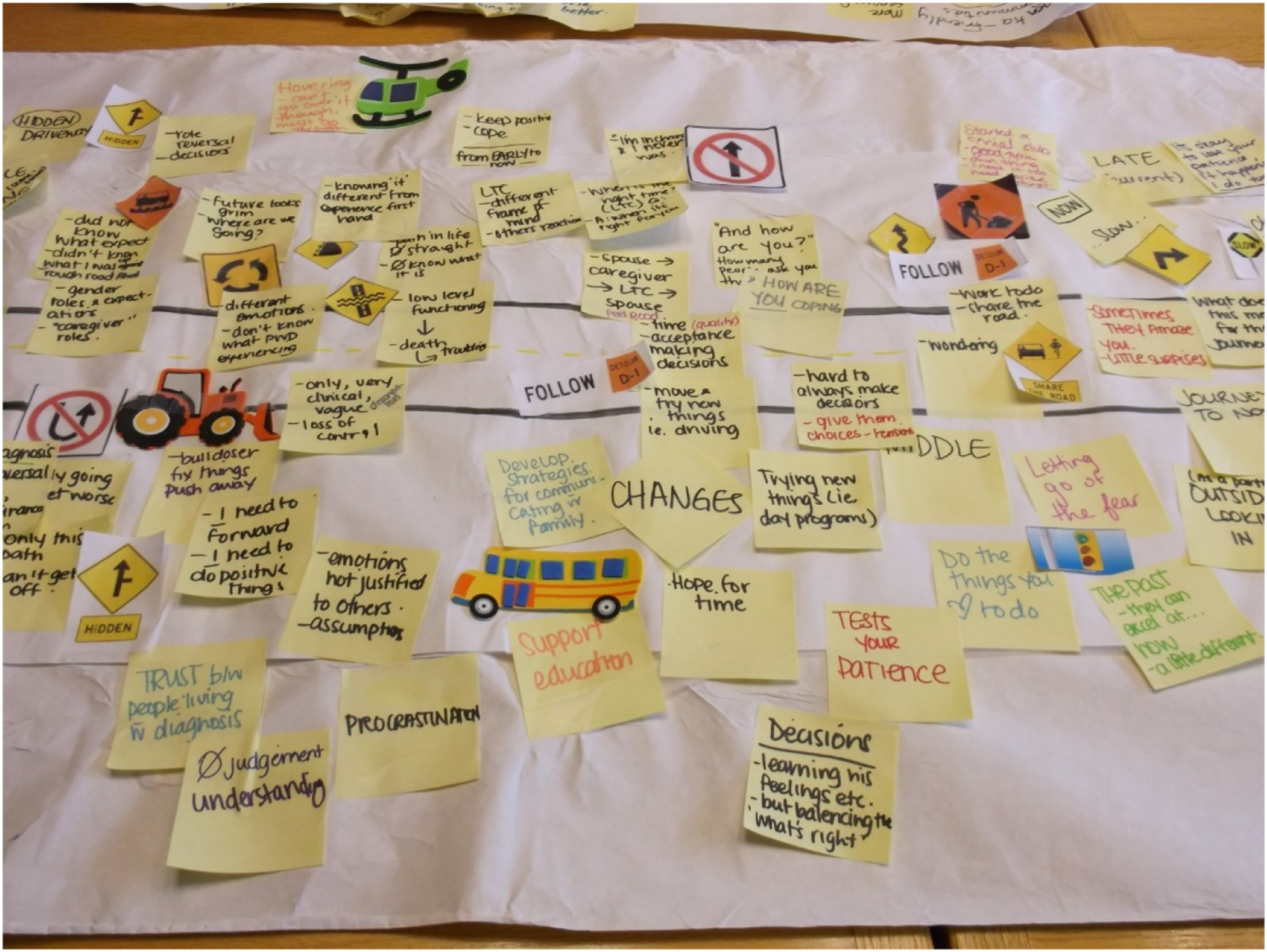
Representing the dementia journey—complexity, multidimensionality, and non-linearity
Creating a single map from the individual focus groups maps and from the consolidated group maps was a particularly challenging task. We discussed as a research team how to capture the complexity of the dementia experience from multiple perspectives of those involved in the dementia journey. While the use of the journey metaphor and road image was particularly helpful to elicit perspectives from diverse participants, particularly with the props we used, a linear model representing the dementia journey oversimplified the complexity and nuanced aspects of individual journeys with dementia. This became even more evident when we tried to consolidate all the maps into a final representation of the dementia journey. Key questions we grappled with at this point in our process, included: Was a road leading to somewhere? Where was the road leading to? How do we best capture when participants described feeling stuck in a loop? How do we capture when participants wanted to get off the road or when one aspect of the journey went on for a long period of time for some? What was the end of the journey? How did we capture the descriptions of participants with dementia and care partners who discussed the need to change and adapt through all aspects of the dementia journey?
After careful consideration and ongoing discussion, the research team came up with the concept of the subway map as a way to reflect the separate yet interconnected aspects of the overall journeys shared by participants (see Figure 3). This subway map captured the diversity of each individual’s journey, the interconnectedness of aspects of the journey, the complexity of the journey, and the multidimensionality of the journey. Within each of these four main paths, the sub-paths were represented with road signs identified by participants as symbols for these various aspects of the journey. The overall dementia journey map.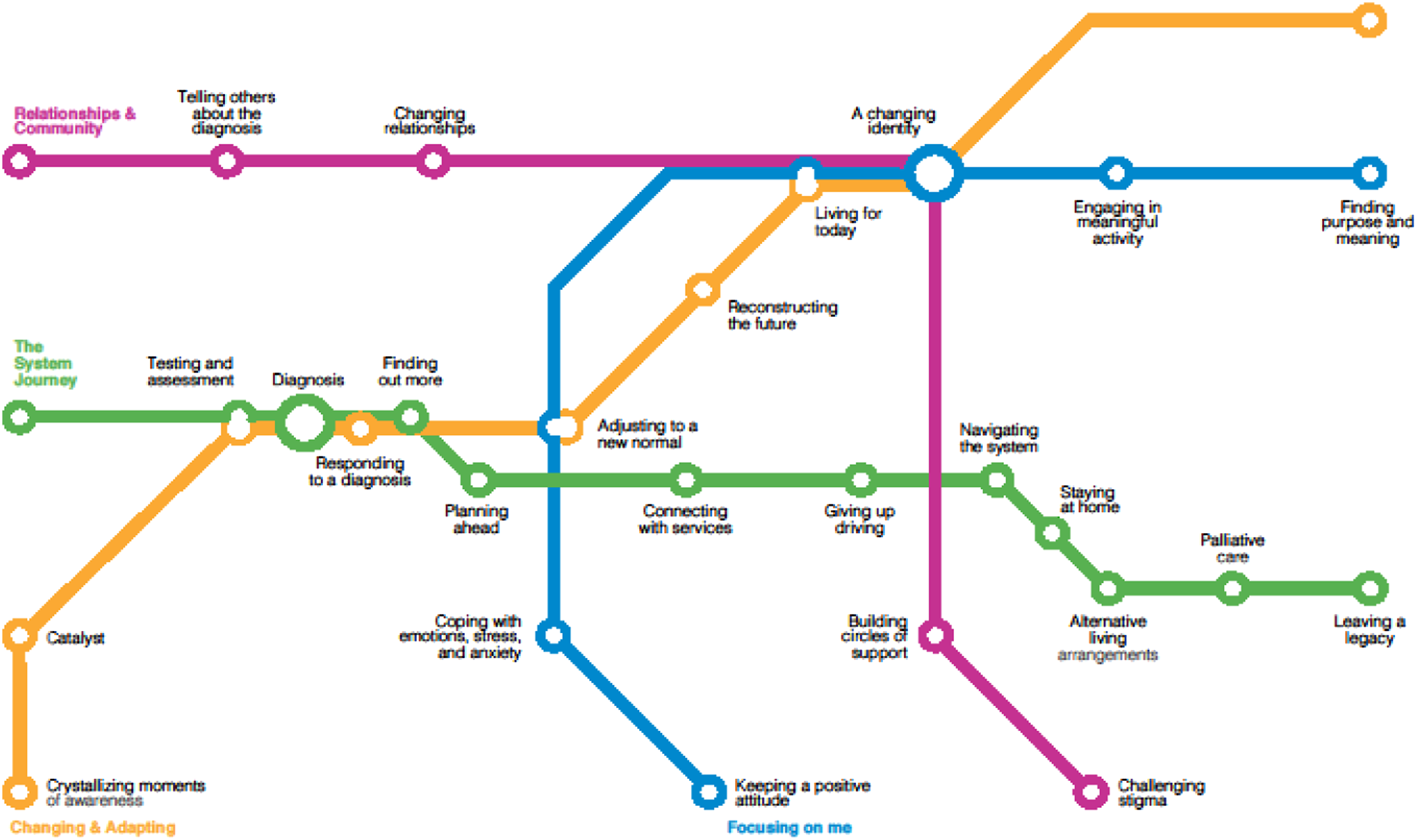
The metaphor of travel, particularly along a subway, has a number of different features. First, a subway typically doesn’t have an end since subway trains traverse their routes over and over again. Second, subways operate on a different physical level, often unencumbered by roads. Once one emerges from a subway station, there is a another world awaiting at street level, with both new possibilities and obstacles to traverse. Third, subway routes are interconnected, where one can travel to a different subway line and make multiple and different transfers along the journey. Fourth, subways are typically contained within one geographic area (e.g., a city). And finally, a subway does not preclude the use of other transportation such as a car or bus. We also felt that while not every city has a subway, the visual of a subway map with different subway lines was relatively familiar to many people.
Four key experiential paths emerged from the data which were represented as subway lines: the system journey, changing and adapting, staying well and focusing on me, and relationships and community. The System Journey represents interactions within the health and social care system, particularly the medical and long-term care systems. Changing and Adapting referred to the kinds of changes that might occur along the dementia journey, and how people responded and adapted to those changes. Staying Well and Focusing on Me captured things that people living with dementia and care partners did to stay well and to care for themselves. Relationships and Community encompassed other people and the interactions with others throughout the dementia journey. While there are numerous themes within each of these broader ‘subway lines’, the broad themes capture the essence of what all the participant groups discussed.
We chose to represent these experiential paths visually as a subway map with the four paths symbolized as separate but interconnecting subway lines. At each subway station, the findings were presented as the street above the subway, with the corresponding road signs that were identified by participants. In this way, a layered and textual analysis was able to be visually represented. Even with the use of one type of metaphor like a journey, there are numerous additional choices of metaphors to be used within this overall concept.
Discussion
This study is one of the first that we know of that uses metaphorical thinking as a methodological device to support the sharing of stories and experiences of dementia. We specifically focused on one of the most common metaphors used to describe experiences of dementia, the journey metaphor, to explore the experiences of the journey from the perspectives of people living with dementia, care partners, and service providers, reflecting the relational nature of the dementia experience and care (Jonas-Simpson 2021; Nolan et al., 2002, 2004).
This research supports more recent research on the use of metaphor for people living with dementia and their care partners, primarily that people living with dementia are able to think in metaphorical ways and can use metaphors as a means to make sense of their experiences (Castaño, 2020). With our focus on the dementia journey, people living with dementia, family members and professionals drew on a number of different and associated metaphors to describe the journey, such as detours they experienced along the way, being stuck on a round-about, taking the scenic path, and other road related images. The use of metaphors can be a complex cognitive process, and yet people with dementia were able to draw on the metaphor of a journey and use this frame to describe their experiences. In fact, we found that the use of the different metaphors and symbols used in the focus groups and interview and the maps created prompted deeper reflections and descriptions of experiences by helping people to visualise specific moments in the journey – return to those moments – and reflect on what the metaphor/symbol represented about their experiences and why the metaphor/symbols were meaningful to them. It also helped them to compare their own experiences with others’, opening up explorations of what it was that made those experiences unique.
Consistent with this research, our findings also demonstrate how metaphorical expressions can have similar and different meanings for people living with dementia compared with their care partners (Zimmerman, 2017a, 2017b). For example, both care partners and people with dementia described “construction ahead” when thinking about the future. However, people living with dementia tended to talk abstractly about the future, whereas care partners described concrete concerns and described this experience as ‘roads diverging’. As another example, people with dementia used the road sign of a bicycle to describe having to give up their driving licenses, whereas care partners used this road sign as a way to describe slowing down and enjoying the moment.
Further, our research showcases the potential of metaphor as both a visual and cognitive device to support the telling of stories that we believe holds great promise for future research focused on people living with dementia as well as other marginalised and stigmatised groups. Using the metaphor of the journey and using symbols and visual aids to talk about the dementia journey, including different types of cars and road signs and symbols, created a safe and often fun space that enabled rich and varied discussions about the experiences of dementia. Choosing and describing the cars participants wanted for their journey helped build a sense of rapport and safety for those who did not know each other and provided key insights on the personalities of participants and how these different personalities might have influenced experiences. It also helped us to set up the journey metaphor and have participants begin to think about the dementia journey. The complexities of metaphors (Hansen, 2018), particularly of the dementia journey, opened up space for people to tell their stories, including how they were thinking and feeling during different events, and document those stories in visual and emotional ways.
The collaborative creation of the road and the use of the road signs elicited deep descriptions about participants’ experiences and also brought back memories of specific incidents and situations that had occurred. It gave participants points of comparison as they agreed or disagreed with others in the focus groups and stimulated new ways of understanding their experiences of dementia. Researchers have argued for an expansion of how metaphors are thought about and used in illness experiences (Hansen, 2018; Stoddard Holmes, 2011), and our research expands understandings in this area by pointing to the importance of both familiar metaphors and the use of visual and tactile aids associated with the metaphor to structure and elicit conversation and support the telling of one’s story in new ways.
This study aimed to take an overall look at the experiences of dementia, or as we titled –the Dementia Journey. Providing an overall picture of the dementia journey is important to enable people to put their experiences into context, to think about and to plan for the future, and to provide a broad overview of what this diagnosis looks like from different perspectives (ADI, 2022). This broad overview also provides a base upon which professionals can critically reflect on and dialogue about the services and resources currently offered and what is needed to better support people living with dementia and their care partners at different points along the dementia journey. Our intent with the maps is not to suggest there is one way to experience dementia or one-size fits all solutions and responses. In fact, our research would suggest that experiences of dementia are far more complex and require flexible, adaptable, and multi-modal approaches at all phases of the dementia journey. What we hope to provide here is a starting point for discussion about the complexity of the dementia journey for people living with dementia, their families, and the professionals who serve them. As numerous authors have suggested, metaphors can be critical communication tools for health service providers to open up dialogue with those experiencing conditions such as dementia (Bleakley, 2017; Wohlmann, 2022). By learning more about how people living with dementia, care partners, and health and social care providers use a metaphor like a journey and what meanings they attach to it, we were able to provide a framework for our partner organisations to use.
While we recognize that the use of the journey metaphor is one that seems to be used by people with dementia (Zimmerman, 2017a), we also recognize that by using this metaphor to structure our methodology, we may have limited the opportunities for participants to be more creative with their own metaphors and to tell their stories in ways that they wanted to. While we view the idea of a journey as a relatively neutral metaphor, participants may have not seen the journey metaphor in this way. Future research should explore the use of other metaphors as research devices to support the exploration of the lived experiences of dementia and the people who support them.
While this broad overview of dementia experiences has the potential to provide some structure to understanding the dementia journey, we recognize that this is a small sample of participants. While we do not pretend that this work is generalizable across all populations, we do think that it can provide some helpful frameworks for discussion. In addition, most of the participants were Caucasian, and the diversity of people from various cultural and racialized backgrounds, socioeconomic status, age at diagnosis, at later stages in the dementia journey, and other factors were limited in our research. The use of metaphors may not be a common reference point and may not apply across different groups and cultures (Macagno & Rossi, 2019). As such, future research should explore whether the dementia journey metaphor as methodology is one that resonates and works with diverse people living with dementia, including people living with dementia from different cultures, at later stages in the dementia journey, and who experience social categories that intersect to cause marginalisation and oppression. From a critical lens, important questions to be answered going forward are: What are the limitations of the dementia as journey metaphor? Who benefits from using the metaphor of the dementia journey? Whose interests are not served, and perhaps harmed, by the dementia as journey metaphor? In addition, by combining the findings in the final composite subway map as representative of all groups (i.e., people living with dementia, care partners, and health service providers), we run the risk of not capturing the nuances of individual people’s experiences. As such, we recognize that each of these areas of the dementia journey can be further explored.
In conclusion, we view the use of metaphors as a tool with great possibility in research with groups such as people living with dementia and care partners. The metaphor of a journey elicited in-depth responses about how people were thinking and feeling about dementia, and provided a framework for people to think about their diagnosis or a family member’s diagnosis. Qualitative research approaches are being utilized more and more to explore the experiences of people living with dementia, and despite the complexity of the use of metaphors, they appear to be a helpful tool to facilitate discussion. Given the above noted limitations, not every situation requires the use of a metaphor, but we encourage researchers and practitioners to consider how metaphors might enrich discussion and understanding of the experiences of dementia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eli Lilly and Company.