
Abstract
Social work assessments underpin support plans for many people living with dementia in their own homes in England, but it is unclear how they acknowledge that dementia places people at greater risk of mouth and dental problems affecting their wellbeing. We explored if and how dental needs are addressed during care assessments and social workers’ perceptions of this aspect of personal care. This study analysed (a) semi-structured interviews with 14 social workers providing support to people living with dementia in their own homes, (b) data from 39 care assessments and support plans from two English local authorities. Interviews were recorded online, transcribed, and thematically analysed. Documents were analysed descriptively and presented visually. Participants acknowledged that oral care may be overlooked during assessments and reflected on various reasons, including assumptions of responsibility and role restrictions, limited training, and poor links with dental services. This was further evident in the analysis of assessment documentation. Participants identified potential strategies and practice changes to better integrate oral care in social work practice. These included increased awareness and more discussions around dental needs, skills training and streamlining of support. The findings have implications for social workers, educators, and commissioners or funders engaging with people affected by dementia in social work and beyond.
Introduction
Dementia is a global health and care priority giving rise to increasing social work interest and practice experience (Department of Health, 2015; Scourfield, 2022). Although all types of dementia have variable trajectories, a gradual and irreversible decline is expected that can severely affect the person’s cognition and decision making, leading to physical, social and occupational dysfunction (Geddis-Regan et al., 2020). Research suggests that interventions to promote the person’s wellbeing should be individualised and strengths-based, considering the person as a whole, their social and cultural factors, as well as input from their family carers (Geddis-Regan et al., 2020; Livingston et al., 2020; McGovern, 2015). Dementia care costs are high in England and estimated to increase even more over a 25-year period by 249%, including health and social care services costs and costs of unpaid informal care (Knapp et al., 2022). In England, the Care Act 2014 sets out the social work role in helping people with care and support needs to live as well as possible. For people living with dementia who are eligible for publicly funded support (on the grounds of need and means-testing) an individual care and support plan will be developed with the assistance of local authority social workers or care co-ordinators, to help promote their wellbeing (Larsen et al., 2019).
Having dementia is a risk for poor mouth and dental health (hereafter oral health) although due to limited evidence more research is needed on this topic (Daly et al., 2018; Kc et al., 2021). Research indicates that people with cognitive impairment have declining dentally-related function. For example, poor memory can disrupt the person’s daily oral and denture hygiene routines, or impaired executive function can compromise brushing and flossing (Chen et al., 2017). As a result, the person may not seek help for pain and other oral health needs, or consent to clinical treatment and homecare instructions. Thus, people living with dementia often have more dental plaque, increased risk of disease in their mouth or teeth, higher levels of tooth decay and more oral/mouthcare problems, periodontal disease, tooth loss, oral soft tissue pathology, and denture-related problems, than older people without dementia (Fiske et al., 2016; Chen et al., 2017; Kerr et al., 2020). These dental problems are often preventable through dental hygiene practices and thus advance care planning is recommended (Geddis-Regan et al., 2020). However, if oral health care is overlooked, it risks negative effects on general health, wellbeing, and quality of life.
Although there are some examples of social work integration in oral health education institutions in the United States (Stanhope et al., 2015; Zerden et al., 2023), oral health
Materials and methods
Study design
We conducted a randomly sampled documentary analysis of care assessments as well as individual semi-structured interviews with family carers, homecare or domiciliary providers and local authority employed social workers as part of an exploratory project across a sample of English local authorities. The anonymised care assessments enabled us to explore how the care assessments address oral and dental care. The individual interviews enabled the social workers to share examples, offer suggestions and reflect on their practices. This paper reports findings from interviews with social workers and the documentary analysis. Interview findings with homecare agencies and family carers are reported elsewhere (Soilemezi et al., 2023).
Ethics
The study was approved by the Health Research Authority Social Care Research Ethics Committee (SCREC – ref: 21/IEC08/0032). Participants provided informed consent before the interviews. Anonymity was assured subject to exceptions about the necessity to address safeguarding concerns. Internal approvals and agreements were in place in the two local authorities who agreed to share a sample of anonymised care records with the research team. All names in this paper are pseudonymised.
Study setting and participants
Interviews took place from November 2021 - August 2022, during the UK Covid-19 pandemic but at a time when social restrictions were limited. Recruitment was based on purposeful sampling with maximum variation to capture diverse experiences and views of social workers with different characteristics (e.g. different ethnic backgrounds, years of practice, age, location, gender, etc). To achieve this, we contacted several local authorities and other stakeholders and used a variety of techniques: direct emails and discussions with interested local authorities, promoting the study via social media and engagement with local and national networks. We selected these recruitment strategies based on our varied networks that covered South and North areas of England. Eligible social workers then contacted the main researcher (DS), who arranged mutually convenient times for interviews. They were asked to read the study information and return a signed consent form in advance of the interview. Participants could choose a face-to-face, telephone, or online (video/audio) interview. All eligible social workers that contacted the main researcher were interviewed covering various aspects of our sampling criteria as explained above and received a certificate of research participation in thanks.
Data collection
Interviews were guided by a semi-structured guide which was initially pilot tested (see Supplementary Materials). The questions were based on: previous research on dementia and oral health, our study objectives, and discussions with our public advisor, a former carer, and study advisory group. They included details of the process of care assessments and care plans, barriers and facilitators to addressing oral care, and ideas for better practice. We collected basic sociodemographic characteristics (age, gender, ethnicity, years of practice). All interviews were conducted by DS, a female researcher with a background in health psychology and dementia research. Interviews were recorded online (on the online video platform), and transcribed by an external company, under a confidentiality agreement.
Two local authorities representing diverse population composition agreed to assist with documentary analysis. This was a smaller number than planned but Covid-19 pandemic pressures were raised as a reason for being unable to assist by several authorities approached. A sample of care assessments and care plans for people recorded as living with dementia in their own homes and in receipt of local authority funded social care services was randomly selected by a volunteer designated social worker in the two local authorities, who anonymised, checked, and shared the redacted documents with the research team. Documents covered the period December 2020 – April 2022. These were read by the researchers and grouped under the relevant sections that were expected to have information regarding oral care needs and support. For care assessments, as recorded on the intranet computer generated forms, these categories covered communication, personal care/hygiene, nutrition, equipment. For the support plans, forms were populated with individually agreed arrangements, categories covering personal care needs, carer support, and the intended outcomes of support from a social care provider.
Data analysis
Interview data were analysed thematically following the framework approach (Gale et al., 2013; NatCen, 2012b). This thematic analysis approach was selected because: (a) it allows capturing a priori issues (as discussed based on our topic guide) and also capturing emergent data (new issues mentioned by participants that could not fit into existing codes), and (b) to help with the data management using an excel file which enabled the researchers to systematically look for similarities and differences between the interview data. One researcher (DS) independently read all transcripts and started coding the data on a preliminary coding/theme framework. The preliminary framework was developed based on the main interview questions and the first two interviews, then was further developed by the inclusion of new topics of interest discussed. If appropriate, data were grouped to form a bigger code or separated from a broader topic to form a new code. Remaining data were subsequently entered onto the final framework. When all transcripts were coded, the preliminary themes and subthemes were developed, based on recurring patterns and condensing similar codes. Preliminary themes were discussed with another researcher (JM) to reach consensus. The research team followed an interpretivist approach acknowledging that the participants’ views and lived experiences are subjective and unique.
Document data were grouped under the prespecified categories (communication/personal care/nutrition/equipment/informal support/risks) under which discussions and actions around oral and dental care could potentially be documented. The researcher (DS) searched for mentions of oral, dental or mouth care under these categories, then summarised the entries and coloured coded them to enable visual representation. The final table was discussed with another researcher (KW) to finalise the coding.
Findings
Document analysis
Visual presentation of the oral and dental needs addressed in care assessments and care plans from two local authorities (N = 39).
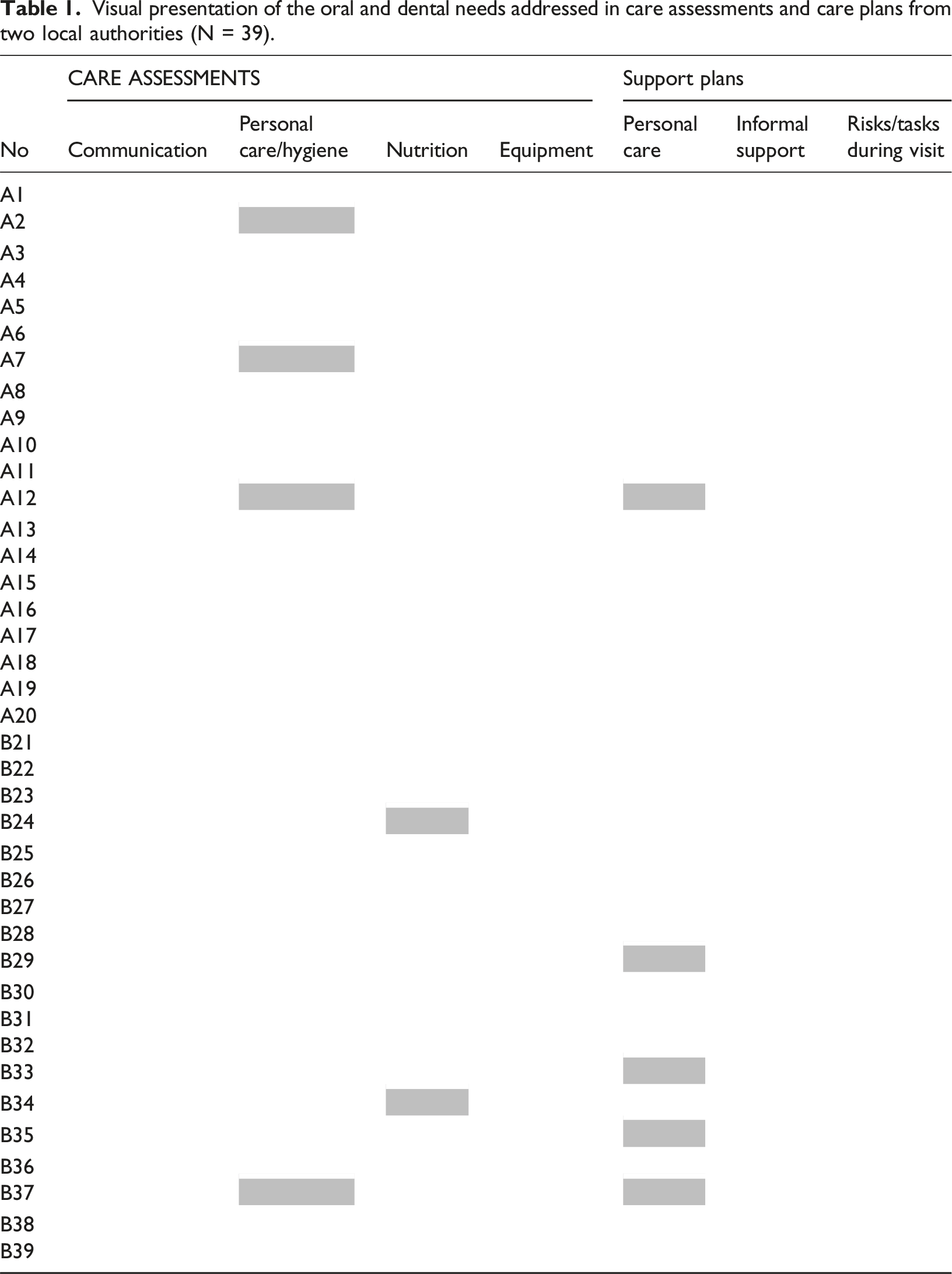
The care assessments contained comments around two areas: a) the person’s ability to undertake their own oral care and their general oral health status. For example (names pseudonymised), ‘John is able to brush his teeth’; ‘Kate has her own teeth at the bottom, she wears dentures on the top, but has lost her bottom set of dentures; she brushes her dentures with a toothbrush and uses mouthwash’, and b) directing homecare workers’ input to promote the person’s oral care. For example, ‘Sam will repeatedly brush his teeth throughout the day and every few days throws his toothbrush away, then requests support to purchase another’; ‘Clarice is often encouraged to wash her face and brush her teeth and requires supervision and prompting to wash her face and brush her teeth but needs full assistance, guidance, and supervision throughout personal care process’.
The two care assessments which mentioned oral care under nutrition referred to the use of dentures (‘Mo wears dentures, however, does not wear them reporting that they are causing some level of discomfort’; ‘Bill wears dentures, there are no reported issues with eating’).
Regarding support plans, mouth care was mentioned in relation to directing homecare workers’ input (e.g. ‘home carer to support with grooming and brushing teeth; offer support and encourage with washing, dressing and other personal care tasks such as hair care, mouth care etc’; ‘Joy requires support with all tasks relating to managing her personal care and hygiene such as washing/cleaning her body, oral care and applying cream; support with dental care… homecarers are requested to encourage to participate in completing simple tasks, such as washing her cup after having drinks, wash her face in the bath, brush her teeth, etc’). Only one entry mentioned the timing of oral care support during the morning care service and none in an evening call.
Interviews
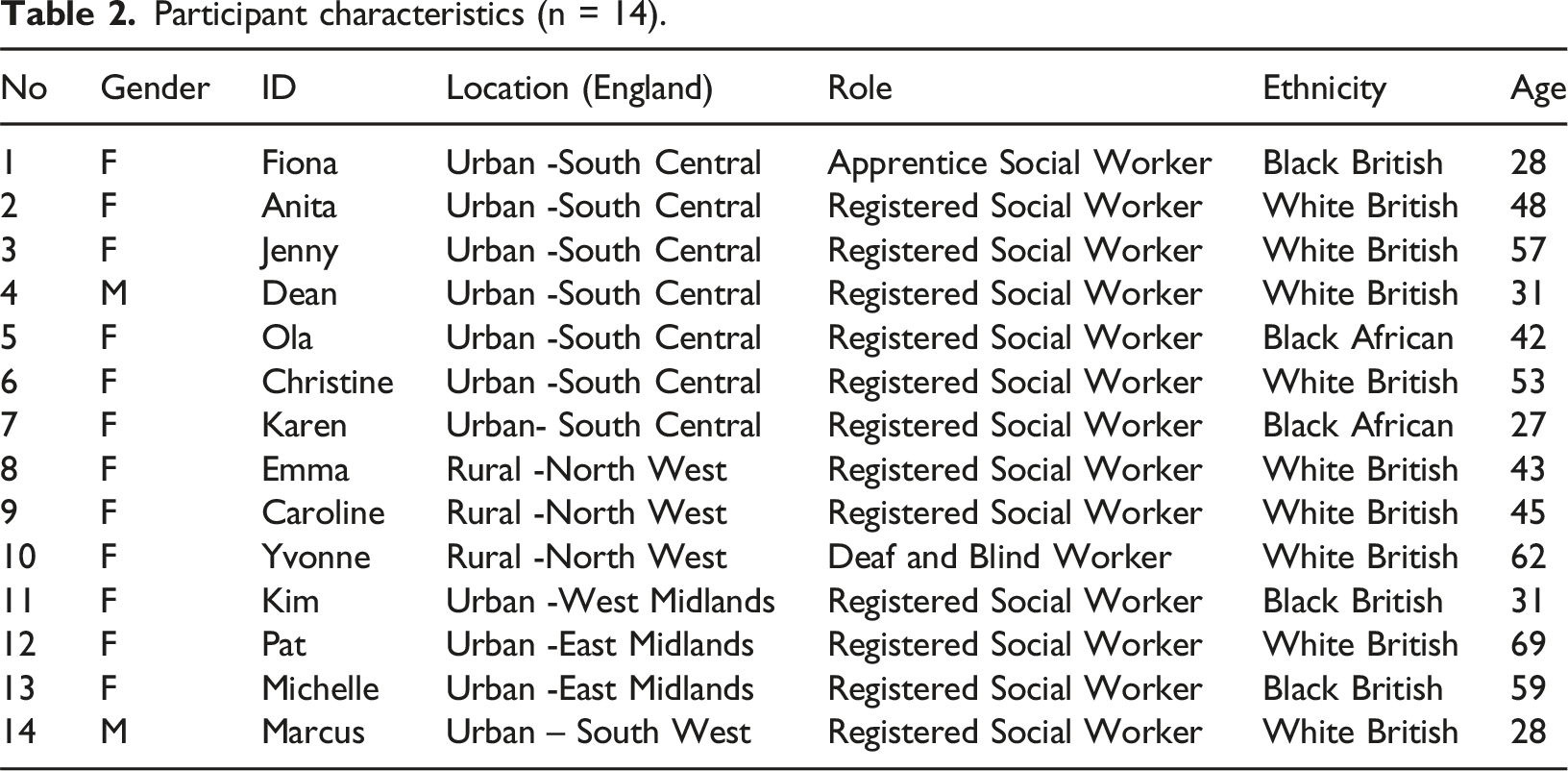
Participant characteristics (n = 14).
Overview of main themes and subthemes.
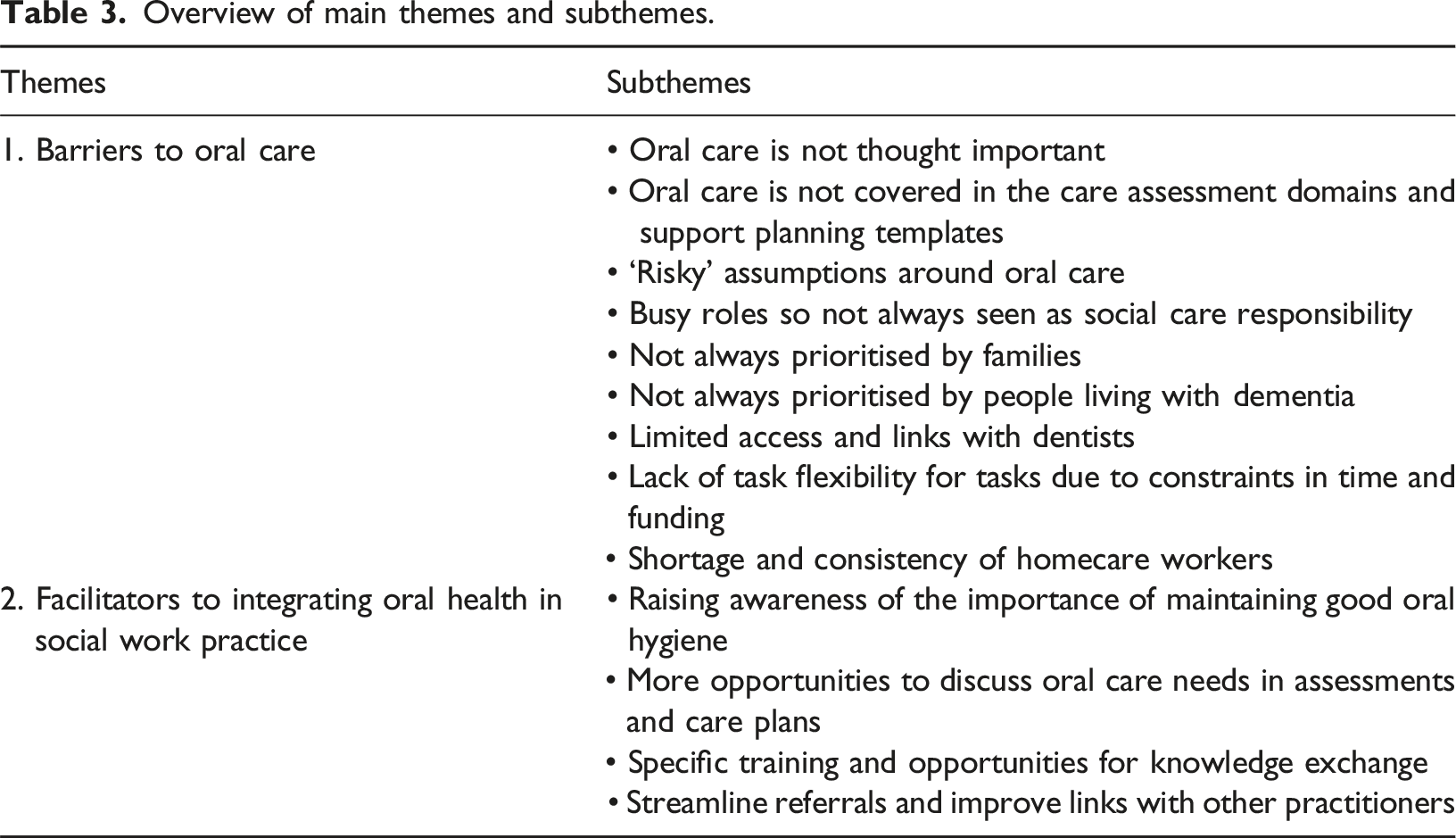
Theme 1: Barriers to oral care
Across interviews, social workers commonly declared that mouth and teeth care was very important for people living with dementia. Some highlighted the importance of a healthy mouth as it affects eating and drinking, and that there could be risks to psychological and health status if problems were over-looked. However, they acknowledged that oral and dental needs and risks associated with them were not generally discussed during an assessment unless there was a problem or a crisis. Some exceptions were mentioned (when a person wears dentures, is at the end stage of dementia, or living in a care home), presumably because these individuals experience further cognitive decline and have substantial difficulties with their own personal care so daily oral care is discussed in more detail. Practitioners reflected on various factors that impeded these discussions, as described below.
Oral care is not thought important
Several practitioners explained that oral health care (care for mouth and teeth) is often missed because it is “not deemed as a priority” (Pat - 69 year old social worker) and was “not a huge thing that seems to come up very often” (Anita - 48 year old social worker). Similarly, another thought it gets over-shadowed by more important needs, “it’s quite a small task as opposed to the bigger tasks of getting dressed or showered, or washed so I think it’s something that can be easily missed… I think people maybe don’t see it as important as when mentioning personal hygiene” (Fiona −28 year old apprentice/trainee social worker). Some practitioners reported tending to prioritise other competing needs so, unless there is a crisis or something of concern, daily mouth and teeth care could be missed.
Even during conversations about personal history and healthcare, dental health and appointments were typically not discussed. However, one participant mentioned that these would likely be discussed if there were a special requirement, for example a need for communication assistance or if the person had sensory difficulties. Despite asking briefly about their medical history in a Care Act assessment, information such as dental history and any dentist’s contact details were not commonly sought and so remained unrecorded: “It’s not something I’ve ever asked, Have you got a dentist?, no” (Dean - 31 year old social worker). However, practitioners always recorded details of the GP (family doctor), with some reflecting on this difference, saying “it wouldn’t be like asking, ‘have you seen the GP?’, which I would always ask, which is interesting” (Marcus - 28 year old social worker). One practitioner expected that the homecare staff would ask about this and another that “I’m prompted to ask about it more in residential homes” (Emma - 43 year old social worker).
Oral care is not covered in care assessment domains and support planning templates
By explanation, one practitioner, checking the domains in their employer’s Care Act online assessment documentation, pointed out that “on there, there is nothing about ‘tell me about your oral care'… so, in actual fact, all the way through there isn’t anything about oral care on there” (Christine - 53 year old social worker). Most social workers thought that daily oral care was generally subsumed under personal care or hygiene “so the heading would be personal care or domestic routines and then it’s up to the flow of the conversation to see where that takes you” (Yvonne - 62 year old specialist in work with Deaf and blind people). Some reflected that “actually, we lump everything in with personal care” (Christine −53 year old social worker) although this was not always thought very helpful, because, as one practitioner explained, “their care notes, it says personal care completed and it’s just to me, it doesn’t tell me anything” (Michelle - 59 year old social worker). Four practitioners reported that they would “put it in eating and drinking…[and] in the nutrition bit” (Pat - 69 year old social worker). Even when it was addressed, most acknowledged that mouth and tooth care “tends to be quite minimal” (Dean - 31 year old social worker), “nothing too in-depth” (Kim - 31 year old social worker) and “we’re not drilling down into detail” (Yvonne - 62 year old specialist in work with deaf and blind people). However, exceptionally, one very experienced participant (Michelle - 59 year old social worker), who was personally interested in disability, said she always discussed oral care in depth during her assessments not only as part of personal care, but in relation to safety, nutrition, and emotional wellbeing.
A few practitioners mentioned that mouth or tooth care was covered more often “if the person’s got any dentures” (Kim – 31 year old social worker). However, one participant was adamant that she had “never seen it [oral care]” (Yvonne −62 year old specialist in work with deaf and blind people) mentioned in any care plan. Fiona (28 year old apprentice/trainee social worker) was typical of the participant group: “I would say most care plans and assessments that I have seen, and I’m probably guilty of doing it too, don’t include dental hygiene, and brushing of the teeth. It’s not something that you often see in a care plan, and I think it may be sometimes missed”
A small minority of practitioners stated they generally asked about the last time the person living with dementia had visited the dentist but acknowledged it could be difficult to gather this information if there was no family to provide it. A few practitioners considered that people living with dementia at home may lack opportunities to prevent dental problems unlike care home residents who generally had regular dental checks.
‘Risky’ assumptions around oral care
Most practitioners thought daily oral care would be covered under personal hygiene tasks undertaken by homecare workers or family. Several thought that this was sufficient: “We would expect them [care providers] to do their own assessment and we would expect them to include oral care if it’s required as part of that assessment… Because when we put that somebody needs personal care and support, we don’t put the granular detail, like they need to wash their face or they need to wash their legs or their arms, we would expect the agency who are delivering personal care to work with the individual about exactly what is required” (Anita - 48 year old social worker)
A few raised the risk of oral and dental health being missed but only one expressed this in strong terms: “I won’t work on the premise of assumptions, because it’s dangerous practice” (Michelle - 59 year old social worker).
Some practitioners reflected that conversations around oral care would only happen in crisis, “if something sort of suddenly cropping up, you know, either you know, refusing to brush or, you know, some, you know, concerns with, you know, their teeth” (Ola - 42 year old social worker). A minority acknowledged that such assumptions may lead to neglect and potential health risks.
Busy roles so not always seen as a social care responsibility
Two practitioners described their work as demanding and busy, dealing with individuals’ complexities and different needs. Some said they tried to practice holistically and to cover all aspects of life, which meant “there is so much to think about in the assessment” (Christine - 53 year old social worker). But most highlighted contextual pressures such as “obviously everyone is busy, and they’ve got time constraints” (Caroline - 45 year old social worker) which meant some matters could be overlooked.
However, two practitioners made the point that that dental care was more of a health service responsibility and not necessarily part of their role: “…there’s a clear divide between social care and health, oral is seen as healthcare. And it could be seen as a medical appointment, so therefore we, in terms of the budget, we won’t -it would be seen as health responsibility” (Michelle - 59 year old social worker)
Nonetheless, in emergencies or when other alternatives were exhausted, practitioners might seek funding to ensure wellbeing such as authorising payment for a homecare worker to accompany a person to a dental appointment, generally if the person lived alone and had a homecare worker who could do so. In line with the strengths-based approach, an influential practice framework in English social work (Department of Health and Social Care 2019), where people are encouraged to draw on their own resources, several practitioners explained that the responsibility to address dental needs lies with the family and/or homecare staff who should be able to use this approach to identify any emerging problems and assist with dental appointments. However, four practitioners had experience of clients’ family members raising concerns about the adequacy of oral care delivered by homecare workers as part of their feedback to the local authority funder.
Not always prioritised by families
There were mixed reports of family involvement in maintaining oral care. Many practitioners viewed relatives as vital in gathering mouth and teeth related information, as well as planning and delivering daily care and acting on problems such as “bad breath” (Anita - 48 year old social worker), “eating… swallowing” (Pat - 69 years old social worker) and “communication” (Fiona −28 year old apprentice/trainee social worker). However, some practitioners considered that families generally do not address daily oral care and “If you don’t mention it, they won’t” (Michelle – 59 year old social worker).
Not always prioritised by people living with dementia
Practitioners reported that mouth or teeth care was not always considered a priority by the person living with dementia and some may resist support because, “it’s too personal, isn't it? You are really in their personal space which can be quite difficult” (Karen −27 year old social worker). Some people’s daily oral routines and dental appointments had altered or sometimes never established: “A lot of people that we have come across just simply do not have a dentist anymore, either because they have failed to attend for more than 12 months or two years, so they’ve been removed [from their patient list] … We meet a lot of people, regardless of their physical disabilities, who don’t do regular oral hygiene.” (Anita - 48 year old social worker)
Limited access and links with dentists
Accessing dentists was described by many practitioners as a problem. Shortage of NHS (state-funded) dentists, especially specialist or community dentists, but also arranging referrals, registrations and transport, were mentioned as additional barriers in promoting dental care for people living with dementia at home. Few practitioners were aware of dementia-related dental services: “The biggest access problem to it is finding the right support for somebody who has got dementia… I’m certainly not aware of any specialist dental service for people with dementia, so there’s not a separate one” (Jenny −57 year old social worker)
Lack of flexibility for tasks due to constraints in time and funding
Having sufficient time and flexibility in a homecare visit was acknowledged as important but hard to include in agreed support plans that were constrained by local authority resources. Two practitioners commented that people receiving a direct payment (local authority cash instead of an agency service) have greater flexibility if they need support with any dental appointments than those with a standard care package. Some acknowledged that dementia-related symptoms meant difficulty in addressing all aspects of an agreed care plan: “Because if you think somebody has got dementia, it could take 10 or 15 minutes just to do the very smallest of tasks really, which you know, to everyone else is done within two or three, five minutes” (Caroline - 45 year old social worker)
Shortage and consistency of homecare workers
Having the same homecare worker or a familiar team was perceived helpful to people living with dementia to enable the building of relationships with them and the family. Consistency enabled homecare workers to quickly spot that something was not right but high staff turnover in homecare agencies meant this was difficult: “there’s a shortage of staff everywhere and to get the right staff, I mean, we’ve had difficulties in the past with getting the right staff that are able to implement the support that’s needed. But, you know, it is even more difficult now because you can’t get any staff, you know, and the staff you have are rushed off their feet” (Pat - 69 year old social worker)
Theme 2 Facilitators to integrating oral health in social work practice
The need for more focus on oral care and helpful strategies was discussed by many participants. Oral care could be included in elements of social work practice in various ways, such as raising the profession’s awareness, increasing opportunities for multi-disciplinary discussions, skills training, and other ideas, as described below.
Raising awareness of the importance of maintaining good oral hygiene
There was agreement that daily oral care needs to be more specifically addressed in assessments of people living with dementia at home and their support plans – with recommendations that it needed to be mentioned in assessment and planning documentation (the domains of their documentation, for example under personal care, nutrition, potential risks, and so on): “Oral care should be treated just as important as other domains… I think dental care should be seen in its own right as part of personal care. Like we do like nutritional care, that’s a separate entity. It’s a recognised separate entity, incontinence care, bowel care, it’s a separate entity, but they all link” (Michelle - 59 year old social worker)
More generally, a lack of confidence among many social workers about signposting people to advice and information and in some cases specialist support, was evident. This was despite the recognition that problems could arise that were directly part of social work practice, for example, safeguarding from abuse and neglect: “I did do a safeguarding enquiry for a lady and that was part of the concerns is that they [care workers] weren’t able to support her with brushing her teeth. The dementia had advanced quite significantly, and she would kind of lock her mouth shut so they would struggle to actually get the toothbrush into her mouth… they hadn’t looked at kind of alternative ways. We were saying “she can swallow liquid, she could – we could give her mouthwash to kind of swirl around her mouth” (Marcus −28 year old social worker)
More opportunities to discuss oral care needs in assessments and care plans
A few social workers reflected on how best to promote good oral care and suggested that initial care assessments should be focused more on such subjects. Adding to this, many thought “definitely there is more that could be done” (Christine) to increase opportunities to address it in assessments and/or care plans: “Do you know the first barrier is we don’t have the conversation. That’s got to be removed; let’s start having the conversation… first and foremost, we don’t ask the question about oral health, necessarily… it’s not a specific question that I know that anyone ask… we always advocate that we want family to tell the person if they’ve got dirty clothes on or if they’ve got marks on their faces. That’s the same with teeth, isn’t it? If their teeth look as if there’s a problem, we’d want them to tell them, but we don’t actually say that. But yes, there’s definitely room to have that conversation” (Yvonne - 62 years old specialist in work with deaf and blind people)
On the other hand, another participant thought this discussion need not be in the initial assessment, but could occur later in reviews: “We need to kind of update assessments all the time, which we should be doing anyway, I think most people would. But again, to go in your first assessment and say, you know, have you got all these issues with anything is probably a bit too much, too invasive to start with” (Pat - 69 year old social worker)
Amendments to the assessment domains by adding reminders or questions or sub-headings and templates were among other suggestions to help practitioners make “sure really that we talk about everything” (Caroline - 45 year old social worker). Such changes to the intranet holding assessment documentation would have to be made at senior levels: “Maybe something if it was on the assessment, it would be something like ‘how would this person like to care for their teeth?’ or – just a prompt really so that it’s acknowledged that you then have to kind of make a note on that” (Marcus – 28 year old social worker)
However, caution was expressed by one participant who asked “how do we stop social work getting so bureaucratic?” (Emma - 43 year old social worker) if conversational topics were mandatory.
Apart from addressing daily oral health needs during the care assessments, adding “a bit more emphasis” (Ola - 42 year old social worker) in the care plan by noting this as separate task (linked with a prompt on the app used by homecare workers as in some provider agencies), was also thought potentially helpful. Recording details from families and homecare workers on daily oral health routines and potential challenges was also proposed and one participant stressed the importance of also documenting “If they've refused, they need to document that” (Karen – 27 year old social worker). In the absence of these systems some social workers explained how they currently tried to provide some oversight of this area in the support plan agreed with the homecare agency: “I put it in bold that this must be completed and if there any concerns, basically I don’t give them a get-out clause” (Michelle - 59 year old social worker). Others called for more content in care plan records: “the interesting thing is homecare services they do often just do what is written on your support plan so unless as the social worker you clearly documented this person needs daily support, not just with personal care but specifying brushing teeth once, twice a day, … I doubt lots of home care agencies would have the initiative to just kind of do that themselves because they might have the assumption that this person is managing that by themselves unless it’s a documented need” (Marcus - 28 year old social worker)
Specific training and opportunities for knowledge exchange
Reflecting on how social work practice could improve, many practitioners suggested that oral care “could be brought up as well in the training areas” (Pat - 69 year old social worker). Several thought they would benefit from further training “to remind me again to the importance of oral care, to constantly remind me” (Michelle −59 year old social worker), spotting and reporting concerns, specifically on the risks of poor oral care, but also strategies to promote daily oral care routines. One participant explained that “it highlights the need for training around it because it wasn’t until I saw your study that I thought, Oh actually that’s a big, a big gap in my thinking and my knowledge” (Emma −43 year old social worker). Most practitioners considered that training would bring “that awareness of, you know, like this is an area that is neglected perhaps” (Ola - 42 year old social worker) and “it’s long overdue” (Michelle −59 year old social worker) and would welcome free online training: “I think we need to be educated as social workers what are the risks if one does not encourage good oral health, hygiene… I think a video, actually, would be really good, perfect. Some e-learning that the Council could use and perhaps spread throughout the teams. We do eLearning modules, for instance, on various things; mandatory ones, safeguarding, health and safety and so on. I’ll go back to the risks: what’s the severity of the risks of not looking after oral care?… you start to be aware of things and then you start to incorporate that within your assessment… So there still probably wouldn’t be headings but I think if we did some e-learning and had some prompts, we would include those in the assessment anyway. For me, I’d dearly like to see some more information on the risks of not addressing it” (Yvonne −62 year old specialist in work with deaf and blind people)
Some practitioners raised the importance of better links with other health professionals, for example dentists, dieticians, and speech and language therapists (SALTs). They welcomed the idea of joint training with dentists and other therapists to learn how to improve assessments: “That would be quite useful if we could have links with the dentist because we have easy links with the GP; GP is very common for us to contact but the dentist isn’t actually and it is part of the body, it’s an organ so it’s just as important as the GP. So, I’d say more connections with dentists and being able to see how they support people with dementia because it would be interesting to know from their perspective the differences or practice of what they have to do for people with dementia and that would then form, probably improve my practice of questions that I ask. It will be easier to get information for my assessment as well and to expand on oral care for that person” (Kim - 31 years old social worker)
Only one social worker reported very positively on their engagement with healthcare professionals on this subject: “I must admit I work very closely with SALTs (Speech and Language Therapists) so therefore for me, and I can only speak for me, and I understand the importance of oral care, because I work closely with them… What diet is the person having? Because if they are on a soft diet and they’re wearing dentures, I would say, ‘have they seen the dietician? Are they aware? Has the dietician discussed oral care as part of their own assessment?’” (Michelle - 59 year old social worker)
Overall, practitioners agreed that the homecare providers also need to be adequately trained “to discuss creative solutions with the family” (Karen −27 year old social worker) and be able to try “different tactics” (Christine −53 year old social worker) to promote oral care.
Streamline referrals and improve links with other practitioners
When asked about making referrals to dentists and attending dental appointments, most social workers considered this the family’s responsibility. Occasionally they offered some practical support, varying from printing out a list of local dentists to referral to a community dentist. One practitioner had referred someone directly to community dental services, but several others had not heard of domiciliary (able to make home visits) dental services and were unaware of local resources: “I think in the same way that we – when you come into these jobs you learn about processes of the kind of local hospitals or the GP surgeries, the psychiatric hospitals, or maybe just knowing what the processes are for the local dentists, where they actually are. I don’t even know where they are in [my town] … that’s just kind of – the basics we need to learn… I don’t know if they [dentists] do home visits.” (Marcus −28 year old social worker)
Another topic discussed at system level was information sharing. One participant reflected that although their local authority and NHS share the same information system, as social workers they did not have access to all its information. Another thought better links with dentists and access to medical records would inform her assessments: “Records, I’d like to view the person’s records. That would be quite useful if we could have links with the dentist, because we have easy links with the GP, GP is very common for us to contact but the dentist isn’t actually” (Kim −31 year old social worker)
Discussion
This is the first study that has explored how oral and dental care is addressed in care assessments and support planning, and the views of social workers on this topic. Our interview data showed that oral care, although thought important, was not consistently covered in the care assessments and support plans for people living with dementia at home. There were several barriers for this that the participants identified: the social workers may assume that there are no oral issues to discuss, or they may not see this area as their care responsibility or something that client and/or families prioritise, or due to difficulties in accessing dental (friendly) professionals. Lack of time and flexibility in payment together with the shortage and/or inconsistency of homecare workers were also mentioned as barriers to identifying and addressing oral care. This lack of discussions was also evidenced by our documentary analysis where we found that less than a third of the documents had any mention of dental/oral care. To rectify this gap, the study participants offered valuable suggestions such as: raising awareness of the importance of maintaining a good oral hygiene in the workforce, create more opportunities to discuss oral care needs during the assessments, care plans and reviews, attending specific training and other opportunities for knowledge exchange, and improve links with other practitioners, such as dentists.
On prompting about the subject of mouth and teeth care, this was considered important by all participants, but was often overlooked or overshadowed during assessment and care planning. Similar views were expressed by family carers and homecare providers who acknowledged that there may be missed opportunities to address oral care (Curtis et al., 2020; Soilemezi et al., 2023) as was also evident in the document analysis. Problems related to their busy roles, perceptions around responsibility, lack of training and absence of links with dental professionals and other general obstacles that they laid at the door of homecare providers (shortage, turnover of care workers, and so on) making preventative dental care hard to implement. Expanding the role of social workers to promote holistic care has been discussed in the US literature and it has been suggested that social workers could also be trained to assess for dental needs (Stanhope et al., 2015; Zerden et al., 2023). Previous studies involving homecare providers and family carers have identified similar challenges, including factors related to the care infrastructure and policies such as training, allocated time, and continuity of care (Larsen et al., 2019; Soilemezi et al., 2023). Dementia-friendly dental environments and continuity of care are considered fundamental as they can enable the person with dementia (and their carers) to build a trusting relationship with their oral healthcare professional and monitor any dental changes over the course of dementia (Kerr et al., 2020). Although many acknowledged that maintaining good oral hygiene is challenging for people living with dementia and their families (see Curtis et al., 2020; Doshi et al., 2021), recommendations largely related to homecare practices, such as trying alternative approaches, improving awareness of devices and tools for homecare staff to develop personalised care plans (Dalgrano et al., 2021; Doshi et al., 2021). Not explicitly mentioning oral care in a domain of assessment or care planning documentation meant it was documented only by exception.
Participants offered various suggestions of how mouth and tooth care could be integrated more systematically in social work practice under the Care Act 2014. They provided examples of ways to raise awareness, but these were rather unsystematic and reliant on personal interest and memory. Training of the workforce (social workers, dentists, homecare providers) was also suggested as helping to raise awareness of risks that could be more regularly documented, plans made to mitigate them and thus minimised. This finding echoes suggestions by previous research on oral training and education that advocated the expansion of social work to integrate oral care assessment to advance integrated care delivery and interprofessional synergies (Zerden et al., 2023). Care providers and family carers (Soilemezi et al., 2023), also called for more attention during care assessments and more detailed care plans to address oral care in greater depth, linking it with other domains (such as swallowing, speech, nutrition, hydration, pain) and/or distress that made it difficult to support this aspect of personal care. As evidenced by both our document analysis and the interview dat
In addition, while some participants had encountered people living with dementia with dental problems and made direct referrals to dental services, many acknowledged that they lacked the skills to notice such problems and did not know local referral procedures. As a result, some oral problems may be unmet, or the onus placed on families, homecare agencies or/and primary health teams to do something. This is consistent with studies reporting lack of training (Doshi et al., 2021; Fiske et al., 2016; Soilemezi et al., 2023) and problems accessing dental care (Kc et al., 2021; Soilemezi et al., 2023).
Our findings raised interesting questions around participants’ perceptions of what constitutes personal care and where mouth and dental care ‘sit’ as a matter of professional oversight and responsibility. Researchers could explore professional understandings of this subject and how to improve practice in this area. This might include a more holistic approach by dental and medical practitioners including adjusting treatment plans if a patient lives with dementia. Advance care planning is also recommended to record the person’s preferences and wishes regarding their dental care (Geddis-Regan et al., 2020). Community dental services, which provide specialised care including appointments at home, need encouragement to do this (Kerr et al., 2020; Lim & Borromeo, 2019). Dementia-friendly dental practices are also important and could have links with local authority social workers. Dental care professionals might provide health messages, advice on assistive aids or remote reminders to their patients and nominated carers (Wanyonyi et al., 2022) in synergy with care and support plans.
Highlighting the importance of maintain good oral care to social workers during their training and in social care texts could also be another way to raise awareness and promote integration oral care early in social care education, something that has slowly been implemented in the US (Zerden et al., 2023). Use of existing or new resources (e.g. checklists, training videos, local/national guidelines, etc) could also be the subject of further research to examine their use, acceptability, costs and successful implementation of such resources in homecare practice. Resources such as the Oral Health Assessment Tool (developed by the Australian Institute of Health and Welfare -AIHW) and the Dental Activities Test (Chen et al., 2017) are brief and available, but further research could investigate whether they are fit for social care assessments as were designed for health professionals. How oral care is promoted for people living with dementia from different cultural or minority groups could also be an area of future research.
Limitations and strengths
Despite our best efforts and liaising with various local authorities, we recruited a small sample of social workers and gathered a small number of anonymised care assessments and support plans, likely influenced by the sector pressures and greater priorities of care during the prevailing pandemic. Although we included a small sample size (N = 14), we managed to recruit a diverse sample covering our pre-defined sampling criteria from different regions around England (South Central and South West, North West, East and West Midlands). As this was an exploratory study with a small sample, we aimed for diverse but rich data and information power. Most participants were of White British ethnicity and female (mainly practicing in two largely urban counties) therefore our findings may be relevant to other English regions but may not be transferable to other countries or populations.
However, our sample included social workers of different ages and with broad professional experience. Our topic guide (see the Supplementary) was designed to raise very focused questions and prompts, acknowledging that our participants were unlikely to have much time for a longer interview. While the interviews ranged from 18 - 45 minutes (average 25 minutes), they were highly informative and enabled a meaningful analysis. Data collection, analysis and reporting were undertaken by a psychology researcher, with two other researchers involved in the final stages of data analysis from different professional backgrounds (social care, dentistry). Emerging findings and selected quotations were discussed with our study’s lay advisor (a family carer) before finalising the findings. To our knowledge this is the first study focussing on social work practice in this area and so may offer researchers, practice leaders and educationalists much needed evidence about a neglected area in England and internationally.
Conclusions
Our findings highlighted that oral and dental care can be overlooked and that there are many systemic barriers to encouraging social workers’ attention to oral care. Practitioners would welcome more training and links with dental professionals and the use of other resources to remind them that mouth and dental care should be consistently discussed and included in assessment and care planning practice. While developing oral health care guidelines for good practice in homecare may be timely and would mirror those available to care homes, the domains of Care Act 2014 assessment might also be extended to ensure oral care is explicitly covered during this important conversation and in care planning.
Supplemental Material
Supplemental Material - Social workers’ consideration of dental support for people living with dementia: Findings from interviews and care assessment documentation
Supplemental Material for Social workers’ consideration of dental support for people living with dementia: Findings from interviews and care assessment documentation by Dia Soilemezi, Kristina Wanyonyi, Valerie Hill, Jill Manthorpe in Dementia
Footnotes
Acknowledgements
We are most grateful to all study participants and members of our study advisory group.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute for Health and Care Research (NIHR) School for Social Care Research and supported by the NIHR Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust.
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.