
Abstract
More than half of older people in long-term care facilities have dementia. Little is currently known about the methods and instruments which can be used to capture the perspectives of older people, including those with dementia, regarding the quality of care provided in such facilities. The main aims of this scoping review were two-fold. Firstly, to identify quality of care instruments that have been applied in long-term care settings. Secondly, to evaluate how these instruments have been developed and validated, particularly in terms of their applicability among older people with dementia. Seven databases (Medline, Web of Science, Scopus, ProQuest, Ageline, CINHAL and google scholar) were searched for relevant literature without any date limit. We used quality criteria adapted from COSMIN (Consensus-based Standards for the selection of health status Measurement Instruments) guidelines to assess the psychometric properties of the instruments. The search identified 16 quality of care instruments which had been used in long-term care settings. Of which, two (12.5%) were specifically designed for older people with dementia, and three instruments (18.7%) were modified for use with older people with mild to moderate dementia. A variety of methods were used to develop the identified instruments including literature reviews, qualitative interviews, expert panel reviews, pre-testing and piloting with older people. None of the identified instruments had been subjected to comprehensive psychometric assessment. Most instruments for assessing quality of care in long term care settings lack alternative communication techniques tailored to people with dementia. This review highlights the need for more rigorous psychometric testing of existing instruments for assessing quality of care in long-term care settings. Several existing measures show promise and may be taken forward for further testing and development for widespread application with older people, including those living with dementia, in long term care settings.
Introduction
The global population is rapidly aging both in developed and developing nations. People are living longer with associated declines in cognition and functional capacity and consequently have higher care needs (WHO, 2015). To cater for their care needs, more older people (aged
In 2019, 10.7% of older people in the Organization for Economic Cooperation and Development (OECD) countries were living in long-term care facilities, whereas a significantly higher proportion of older people (68%) received aged care services at home (Organisation for Economic Co-Operation and, 2021). While the larger proportion of care is provided in home-based settings, care provided in long-term care is a significant proportion of spending. The average expenditure on long-term care in OECD countries (1.5% of GDP), and more than half is spent on long-term care settings (Organisation for Economic Co-Operation and, 2021).
Recent evidence from several countries has shown a systemic failure of long-term care to meet basic standards for person centred care (Carey et al., 2018; WHO, 2021). In Australia, the Royal Commission into Aged Care Quality and Safety highlighted long waiting times, poor quality care, reporting and accountability in the sector. They concluded from this the need for significant reform, including the use of person centred quality of care assessment (alongside traditional clinical indicators of care quality e.g., falls, malnutrition, pressure injuries) as an important quality indicator (Khadka et al., 2020; Ratcliffe J et al., 2020; Royal Commission into Aged Care Quality and Safety, 2021). Similar quality of care concerns, coupled with increasing calls for significant changes in policy and practice have been raised internationally in other countries including in the UK and Canada (CRESC, 2016; Lewis, 2022; Lloyd et al., 2014).
Despite global improvements in life expectancy over the past century, new challenges have emerged, including chronic illnesses and dementia, for which age is a leading risk factor (Dattani et al., 2023). Dementia is a chronic and progressive condition, characterized by a gradual decline of brain function causing memory loss, impaired cognitive function, difficulty in communication and mood changes (Australian Institute of Health and Welfare, 2017; Nyman, 2019; Prince et al., 2013). As dementia progresses, an individual will experience increasing symptoms and impacts to their daily life, which often require high level, resource intensive and therefore relatively expensive physical and labour-intensive care and a greater reliance on caregivers (AIHW, 2017). Dementia has now become one of the biggest challenges in health and aged care at the global level, representing a major public health concern (Alzheimer’s Disease International, 2015; Australian Institute of Health and Welfare, 2017). The worldwide prevalence of dementia is expected to reach 75 million by 2030, and is expected to double every 20 years thereafter (Alzheimer’s Disease International, 2015). Long-term care facilities in countries such as the United States, the United Kingdom, Australia, Canada, Taiwan, the Czech Republic, Austria and Norway are estimated to have a prevalence of dementia ranging from 52% to nearly 90% (Auer et al., 2018; Australian Institute of Helath and Welfare, 2022, Canadian Healtcare Network, 2021; Callisaya et al., 2021; Gaugler et al., 2014; Harrison et al., 2020; Martin et al., 2019). Older people living in long term care settings with dementia have been found to experience worse health and social outcomes, including lower quality of life, reduced social interactions, and greater levels of depression than those without dementia (Afram et al., 2014; Callisaya et al., 2021; Castle & Ferguson, 2010; Martin et al., 2019). However, despite the ubiquity of dementia among recipients of long-term care, voices of older people living with dementia have been remarkably absent from the discourse on quality of care (Afram et al., 2014; Orrell et al., 2008; Phillipson et al., 2019; Taylor et al., 2012). Instead, quality of care assessment has been dominated by an overreliance on organisational structure, governance and clinical indicators of care quality (Castle & Ferguson, 2010; Taylor et al., 2012). In order to improve care quality and to deliver person-centred aged care, regular quality assessments should involve self-reports of experiences and outcomes including from older people living with dementia (Kahanpää et al., 2006; Triemstra et al., 2010; WHO, 2017).
Self-reporting is the preferred way to measure quality of care since the individual is the best judge of their own situation. Older people including those with dementia themselves are the primary informants of their own lived experiences with the care and services that they receive (Kahanpää et al., 2006; Kane, 2004; Lood et al., 2020). While proxies (such as family members or health or aged care workers) are sometimes used instead of self-report by people with dementia, it is well documented that proxies themselves are not without issues of bias or poor reporting, such as known weak agreement with self-report on non-observable domains, being overly critical, not having a complete picture of the other person’s values, and not necessarily having enough contact with the resident to be able to accurately assess their care quality (Hutchinson et al., 2022)
However, involving older people living with dementia in assessing the quality of care they receive is not without its challenges. Firstly, many generic instruments of quality of care have not included the voices and language of older people living with dementia during their development, and therefore the existing instruments are less likely to be sensitive to capturing the aspects of care which are most important to them (Brazier et al., 2012; Stevens & Palfreyman, 2012). Secondly, the existing instruments are traditionally text-based and it is well documented that older people with cognitive impairment and dementia may experience difficulties using text-based instruments (Phillipson et al., 2019; Rand et al., 2019). Emerging evidence indicates that a number of approaches can be adopted to assist individuals with diverse communication needs to self-report their own quality of life (Buitenweg et al., 2018; Kaufmann & Engel, 2016; Milte et al. 2016, 2026; Shiells et al., 2020). These include accessible and alternative communication methods such as easy read materials (simple layout and format, plain English), the use of images, pictographs, audio-visual materials and symbols. These alternatives approaches have been found to make self-reporting of quality of life more feasible in respondents with diverse communication needs e.g. for people with intellectual disability, aphasia and culturally and linguistically diverse background, and may also be relevant to support self-reporting quality of care in the long term care setting (Phillipson et al., 2019; Rand et al., 2019; Samuelsson & Ekström, 2019).
Other evidence, aside from quality of life measures, such as measures that assess personal care preferences has shown that individuals with dementia specifically those with mild to moderate dementia are capable of responding to questions about their care (Lichtenberg, 2010; Mast, 2011). While they may struggle to recall factual information, they can accurately express their choices for daily living; articulate queries about simple preferences; make informed decisions and communicate their care preferences. Additionally, individuals with dementia can actively participate in sharing their experiences in care planning and assessment. This is achievable through thoughtful and specific approaches aimed at understanding the person with dementia and their unique experiences. By employing supportive methods to supplement self-reported data from individuals with dementia, their perspectives can be effectively integrated into the care assessment process. (Lichtenberg, 2010; Mast, 2011; Sunderland et al., 1988). In principle such approaches may also be helpful in improving the feasibility of self-reported quality of care experience of older people living with dementia. However, the extent to which such approaches have been formally used and tested in populations of older people with dementia is currently unknown.
The main aims of this scoping review were two-fold. Firstly, to identify quality of care instruments that have been applied in long-term care settings. Secondly, to evaluate how these instruments have been developed and validated, particularly in terms of their applicability for populations of older people with cognitive impairment and dementia.
Methods
Search strategy
A comprehensive search strategy was developed using key words and subject headings consisting of four main concepts, namely quality of care, evaluation tool/survey/questionnaire, long term/nursing/residential care, and people with dementia and/cognitive impairment (Appendix I). In addition, all relevant MeSH terms and synonyms were identified and included in search strategies as appropriate. In March 2022, the search was performed in seven databases (Medline, Web of Science, Scopus, ProQuest, Ageline, CINHAL and google scholar) without any upper date limit. References of identified articles were also searched for additional relevant references.
Study selection
Articles reporting the development, testing, and validation of quality of care instruments for application in long term care settings with older people including those living with dementia were included. Papers reporting in English and theses were included Additionally, grey literature materials were examined in various online repositories and databases. We conducted hand searches of reference lists of included articles to identify any articles that were not captured by the search, and the full texts generated were screened and assessed for eligibility.
Any case reports or conference abstracts were excluded as the findings may not be generalizable.
The selection of articles was conducted in a stepwise process. Initially, the titles and abstracts of the extracted articles were screened for duplicates and ineligible records. Secondly, the full texts of the remaining articles were reviewed by two reviewers in accordance with the inclusion criteria previously specified. Two reviewers initially reviewed half of the articles and reached 92% agreement for the full text articles included and excluded (Cohen’s kappa = 0.70). For the second half of the full texts, review was carried out by one reviewer only.
Data extraction
A standardised data extraction form was developed and utilised for data extraction. The following data was extracted: authors, year of study, location of study, sample characteristics, the quality of care instrument/s applied, number of items, dimensions of quality of care covered by the instrument, response categories, the methods used to develop or adapt the instrument, and the extent and components of validity and reliability testing undertaken. Quality assessment of the identified quality of care instruments was also conducted using the criteria developed by Pesudovs et al., and the Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN (Mokkink et al., 2010; Pesudovs et al., 2007) to rate the content development, validity and reliability of the instruments (see attached appendix I, II and III). Each of the identified instruments was assigned a positive rating (score A) where it fulfilled the specific criteria completely. A minimally acceptable rating (score B) was assigned where the instrument partially met the criteria and a failure/negative rating (score C) was awarded when the instrument failed entirely to meet the criteria. Half of the identified instruments were assessed by two reviewers, who agreed 86% of the time, while the other half was rated by a single reviewer.
Results
Flow of studies through the review
The flow chart (Figure 1) illustrates the process of selecting articles for the scoping review. A total of 4713 articles were retrieved from the database searches using the key terms. Of these, 995 were duplicates, which were removed using Covidence software. 3718 articles were screened, of which 195 articles were identified as eligible for full text review, 16 articles met the inclusion criteria and were included in the scoping review. PRISMA flow chart.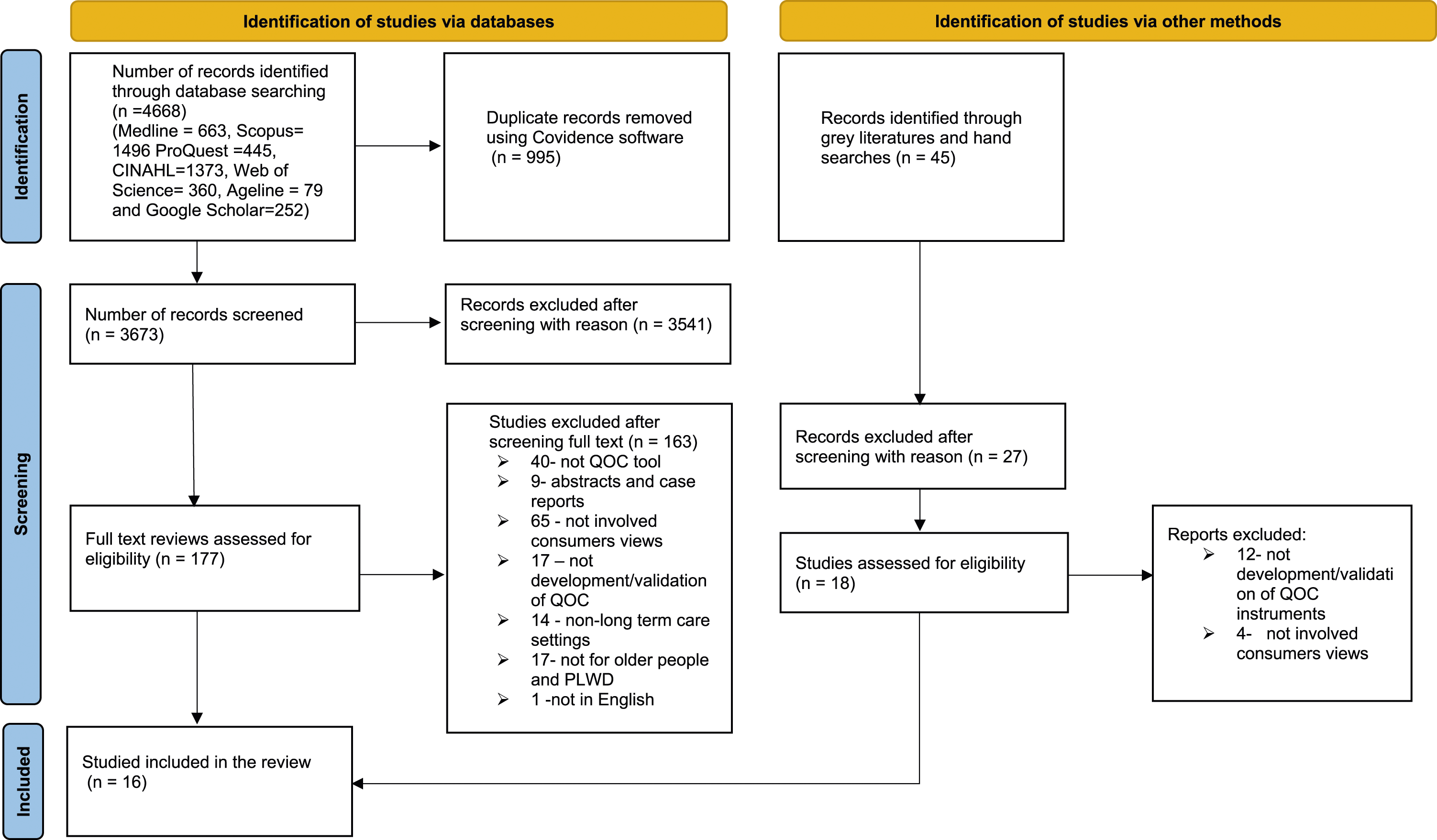
Characteristics of the included studies
All of the studies included in this review were published between 1993 to 2021 (Table 1). Fourteen of the studies were focused either on development or a combination of development and validation of person-centred quality of care instruments. Only two studies (Gill et al., 2007; Yeung et al., 2016) were solely focused on validation of the instruments.
Of the total 16 quality of care instruments included, two were developed explicitly for people living with dementia in long term care settings, namely the Consumer Choice Index six dimensions (CCI-6D) (Milte et al., 2019) (which was co-designed with older people with mild and moderate dementia) and the Scale on Domains of Resident Satisfaction
Seven instruments (46.7%) were developed in the USA followed by three (18.7%) in Australia and two (12.5%), in the Netherlands and one each in New Zealand, Norway, Finland and Hong Kong. There was a large variation in the number of participants in the process of development and validation of each of the quality of care instruments (ranging from 34 to 18,869 residents). No psychometric validation were identified for three of the instruments, the NHCAHPS (Sangl et al., 2007), PELI-NH (Curyto et al., 2016) and Schedule Designed to Measure Satisfaction with Care (Pearson et al., 1993).
Overarching dimensions of included instruments
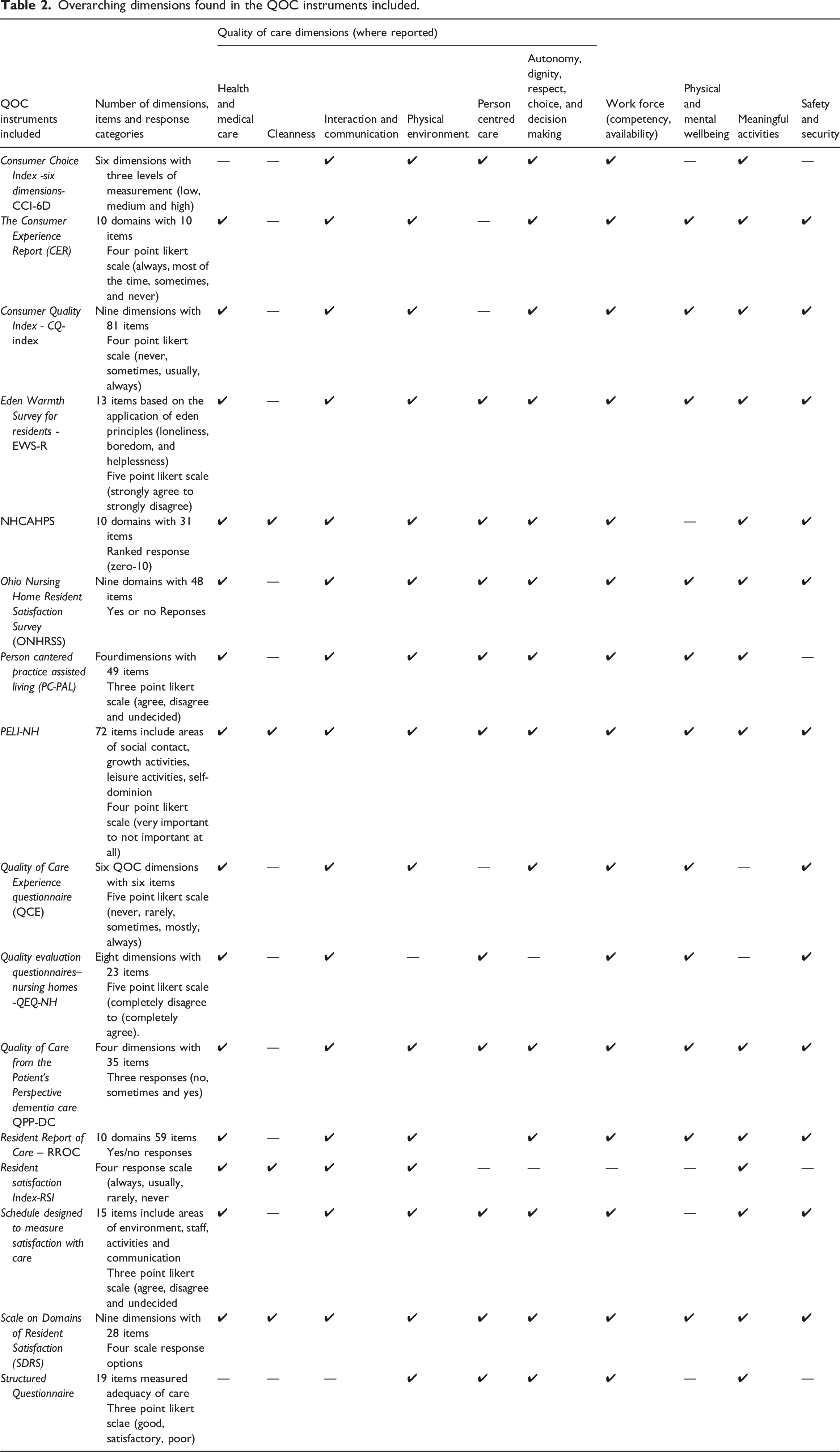
In terms of encompassing the ten overarching dimensions of QOC identified (Australian Government, 2019; Triemstra et al., 2021), over 90% of the quality of care instruments covered the dimensions of interaction and communication; the workforce; autonomy, dignity, respect, choice and decision making. Two instruments (12.5%), the Preferences for Everyday Living Inventory Nursing Homes Residents (PELI-NH) and the Scale on Domains of Resident Satisfaction (SDRS), covered all ten of the over-arching dimensions (Table 2). Two thirds of the quality of care instruments (66%) addressing safety and security; person-centred care; and physical and mental well-being. However, the dimension of cleanliness was the least commonly covered dimension.
Additionally the identified instrument varied considerably in instrument length (ranging from six to 72 items). In terms of response categories used, the majority of the instruments (68.75%) used Likert type responses, with the remaining using ranked/ordinal scales such as the use of zero to ten rating ranges, and dichotomous (yes/no) responses.
Techniques used in the processes of developing the instruments
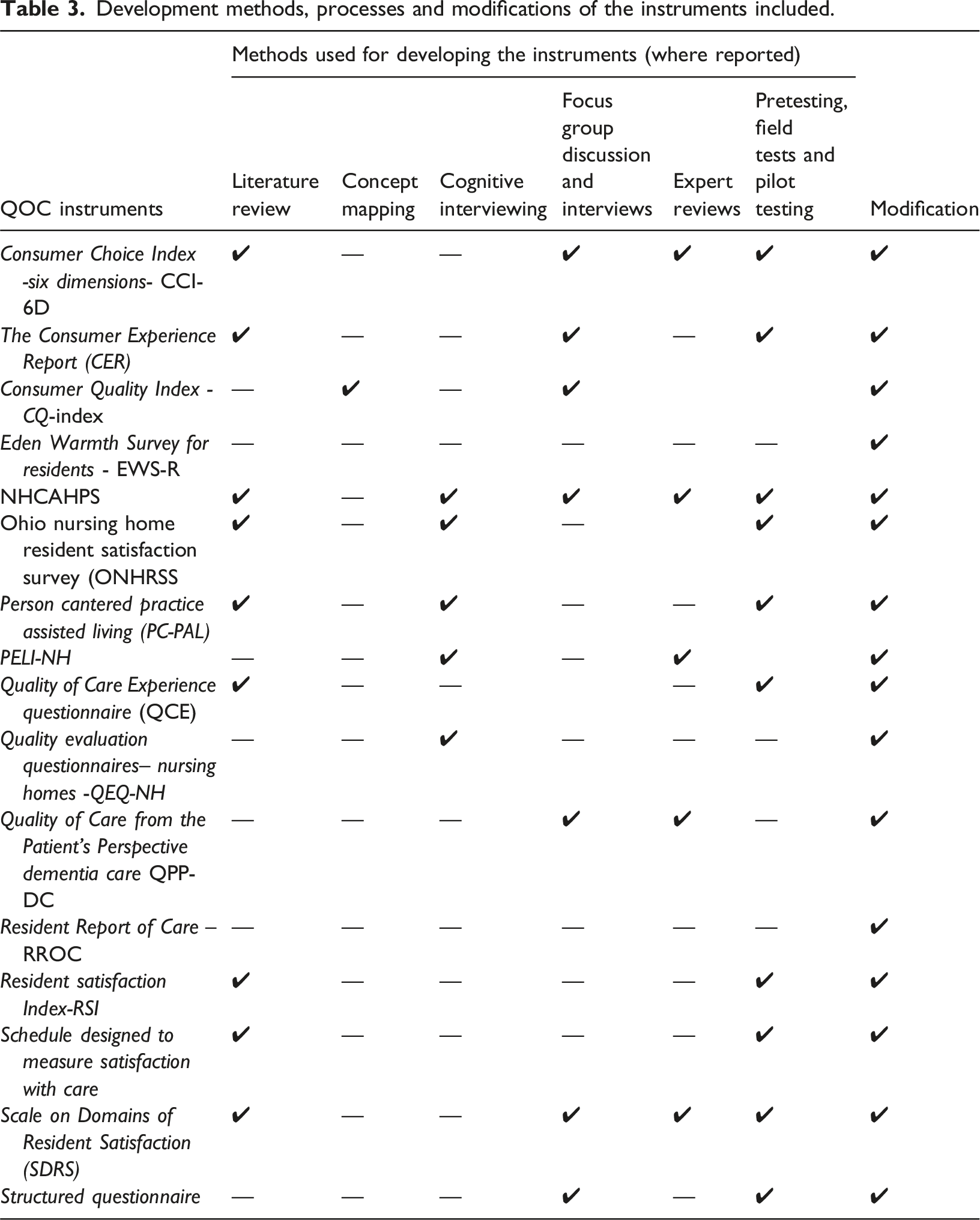
As outlined in Table 3, a literature review was conducted to develop content of more than half, specifically 9 (56%) of the QOC instruments (Chong and Chi, 2001; Khadka et al., 2020; Milte et al., 2019; Pearson et al., 1993; Sangl et al., 2007; Simmons-Mackie et al., 2014; Straker et al., 2007; Wells et al., 2019; Zimmerman et al., 2015). Additionally, five instruments (31%) were utilized cognitive interviewing (Curyto et al., 2016; Sangl et al., 2007; Straker et al., 2007; Triemstra et al., 2021; Zimmerman et al., 2015) and experts review were utilized by another five instruments (Chong and Chi, 2001; Curyto et al., 2016; Helgesen, 2019; Milte et al., 2019; Sangl et al., 2007). Interviewing and focus groups were also incorporated into seven (43.7%) of the instruments (Chong and Chi, 2001; Helgesen et al., 2020; Kahanpää et al., 2006; Milte et al., 2019; Sangl et al., 2007; Triemstra et al., 2010; Wells et al., 2019). There has been a dominant use of pretesting, field testing, and pilot testing i.e., 10 (62.5%) (Chong and Chi, 2001; Kahanpää et al., 2006; Khadka et al., 2020; Milte et al., 2019; Pearson et al., 1993; Sangl et al., 2007; Simmons-Mackie et al., 2014; Straker et al., 2007; Wells et al., 2019; Zimmerman et al., 2015).
Modifications were applied to prepare the final version for future use with older people and people with dementia in long term care facilities. Among these modifications were the addition of items; the removal of poorly performed, redundant, irrelevant, ambiguous and incomprehensible items; rephrasing, re-wording and simplification of item wordings; and the relocation of items from one domain to another, the change of response categories, the change of administration mode, the changes to question types, formats, and response options, and the addition of content clarification.
Performance of instruments against the COSMIN quality guidelines
Based on the COSMIN instrument quality assessment (Table 4), the majority, 13 (81%) of the QOC instruments included in this study were rated A for their focus on the intended population during their development or adaptation of the instrument. This implies that these instruments have been thoroughly studied with the intended target population identified in the study, reflecting an excellent level of inclusion. The remaining three instruments were either generic or did not thoroughly incorporate the target population into the instrument development process. Eight (50%) were rated A for their ability to identify items (selection of items to be included in the pilot) through comprehensive focus group discussions, interviews, expert opinions, and literature reviews. However, only four (25%) of the instruments received score A for item selection (a pilot instrument was developed and tested with statistical justification for items that were removed) and eight (50%) received score B while three (18.7%) were given score C. Regarding dimensionality, the extent to which all items fit with a single underline construct, three (18.7%) have received score A, followed by eight (50%) with score B, and five (31.2%) have no reported tests of dimensionality. The Person-centred Practice Assisted Living (PC-PAL) was the highest quality in terms of content development with A ratings across four content measurement properties. Overall, among the 16 quality of care instruments included, seven (43.7%) had only content development reports and no information was presented regarding their validity and reliability testing.
Three (18.7%) instruments including the Consumer Choice Index- Six Dimension (CCI-6D), the Scale on Domains of Resident Satisfaction (SDRS) and the Resident Report of Care (RROC) have at least one validity assessed with score A of the four validity measurement properties. Another five (25%) instruments including QEQ-NH, QCE, EWS-R, ONHRSS and RSI have at least one validity assessed with score B.
Regarding the reliability tests reported, the majority (87.5%) of the instruments included had no reliability tests although one instrument (CER) had a score B whereas two instruments, ONHRSS and RROC had a score C for the reliability score.
Discussion
This review identified 16 instruments for measuring quality of care in long term care facilities. Instruments developed for older people and specifically for older people with dementia, including the use of accessible-communication methods were a particular focus of this review. While we searched for quality of care instruments that incorporated accessible communication methods, none were identified. Only two instruments were identified that were explicitly developed for older people living with dementia, namely the Consumer Choice Index Six Dimensions (CCI-6D) (Milte et al., 2019) and the Scale on Domains of Resident Satisfaction
The remaining eleven instruments were designed for use with older people in long term care settings but were not specifically developed or validated for use with people living with dementia. Five instruments including CER, CQ-Index, PC-PAL, QCE and QEQ-NH purposively excluded people with dementia from the developmental process. For the remaining instruments, the extent to which older people with dementia were included in the development and/or instrument validation process was not clear.
None of the instruments in this review, including those explicitly developed for people living with dementia have applied communication enhancing techniques such as easy read, pictures, images, pictographs, or audio-visual materials despite emerging evidence that these approaches can support participants to self-report the quality of care they received. These techniques have been successfully applied to a variety of groups, including individuals with disabilities, post-stroke aphasia, or CALD backgrounds, in order to support or replace written communication methods in the evaluation of quality of life (Chinn & Homeyard, 2017; Hahn et al., 2004; Long et al., 2008; Phillipson et al., 2019; Trigg et al., 2007). The techniques have also been demonstrated to be effective with individuals with dementia, supporting them to respond to personal and preference questions and facilitating their engagement in the care assessment process (Lichtenberg, 2010; Mast, 2011). Consequently, future research should examine the application of these techniques in self-reporting experiences of quality of care for people with dementia.
The overarching dimensions of quality of care covered in the instruments were also identified and synthesised. There were ten overarching dimensions adapted from the Australian and Dutch aged care framework, including health and medical care; cleanness; interaction and communication; physical environment; person centred care; autonomy, dignity, respect, choice, and decision making; long term care work force; physical and mental wellbeing; meaningful activities and safety and security (Australian Government, 2019; Triemstra et al., 2021). Two instruments comprised of the ten dimensions including the Preferences for Everyday Living Inventory nursing homes residents (PELI-NH and SDRS. More than 93% of the quality of care instruments covered the dimensions of interaction and communication; the workforce; and physical environment; however less of them (87.5%) covered meaningful activities; autonomy, dignity, respect, choice and decision making and health and medical care. There were three quarters of instruments that addressed safety and security and 68.75% addressed person-centred care and physical and mental wellbeing.
More than 90% of the quality of care instruments covered six of the ten over-arching quality of care dimensions including interaction and communication; the workforce; autonomy, dignity, respect, choice and decision making. Approximately two thirds (66%) of the instruments were addressing safety and security; person-centred care; and physical and mental well-being. The dimension of cleanliness was the least commonly covered dimension included in only 25% of the identified instruments. This is despite the fact that the potentially catastrophic impact that poor hygiene standards can have a crucial impact on residents health, due to the potential frailty and compromised immunity that residents may be experiencing, and the potential for fast and extensive transmission of infectious diseases in the communal living setting (Clemens et al., 2021; Schweon & Kirk, 2011; The Nursing Home Abuse Center (NHAC)). It is possible that cleanliness may not be considered as a key quality of care enhancing dimension by residents, or it may be considered to be more appropriately assessed through other methods, such as through auditing procedures or checking governance arrangements to ensure that proper maintenance is being carried out (Hall et al., 2015; Mitchell et al., 2019; Shaban et al., 2020; Stone et al., 2015).
There have been eight studies on the development of quality of care instruments, six on the development in conjunction with the validation of the instruments, and two studies exclusively focused on the validation of the instruments. Within those studies, a variety of approaches and methods were used. A literature review was included in the development of more than half (56%) of the QOC instruments to identify the aspects of quality of care relevant to residential aged care. Additionally, cognitive interviewing and expert review were utilized with 31% of the instruments. Interviewing and focus groups were also incorporated into 43.7% of the instrument’s development. There has also been a dominant use of pretesting, field testing, and pilot testing (62.5%).
Additionally, 13 studies undertook some form of psychometric analysis, although the depth of analysis varies. No validation identified for three measures despite having already been in use for over a decade, namely the NHCAHPS (Sangl et al., 2007), PELI-NH (Curyto et al., 2016) and schedule designed to measure satisfaction with care (Pearson et al., 1993). Generally, all instruments should have their reliability and validity tested in the population they are to be applied with prior to widespread use as a quality indicator (Pesudovs et al., 2007; Terwee et al., 2007). This helps to ensure, among other things, that the contents are accurate, and that the scale is measuring what it is intended to measure. In order for instruments to be appropriate, they must be supported by validity test evidence in a particular context as it will not be effective across all populations and purposes (Kane, 2016). As part of the psychometric evidence for an instrument, a variety of validation tests should also be employed, including convergent, discriminant, predictive, and other hypothesis-based construct validity tests (Kalkbrenner, 2021). Accurate instruments must be validated with the specific target population, not with the general population, and with the specific setting, language, and culture (Lai, 2013).
We used the criteria developed by Pesudovs et al. (Pesudovs et al., 2007) and the COSMIN criteria (Mokkink et al., 2010) to assess the quality of the instruments identified in the review. The criteria assess the content development, validity and reliability of the instruments on the basis of established criterion. The content development criteria encompass the focus on the intended population, selection of relevant items and dimesionality of items chosen. The criteria for the validity tests included convergence, discriminant, predictive, as well as other hypothesis-based construct validity tests. Reliability test consists of test-retest agreement as well as interobserver agreement. Based on these criteria, 43.7% of the quality of care instruments reported only their initial development stage and had no published information regarding their validity and reliability.
Characteristics of studies included.
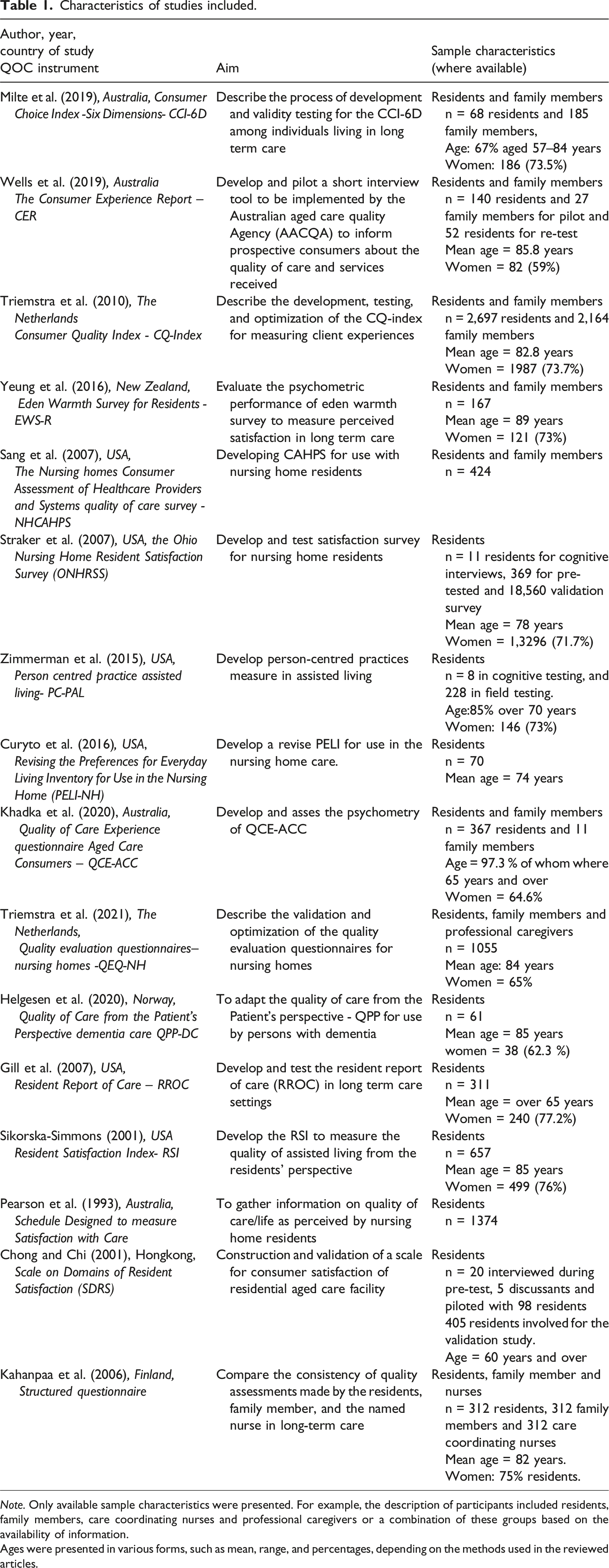
Note. Only available sample characteristics were presented. For example, the description of participants included residents, family members, care coordinating nurses and professional caregivers or a combination of these groups based on the availability of information.
Ages were presented in various forms, such as mean, range, and percentages, depending on the methods used in the reviewed articles.
Overarching dimensions found in the QOC instruments included.
Development methods, processes and modifications of the instruments included.
Quality assessment of the included instruments against the COSMIN quality guidelines.
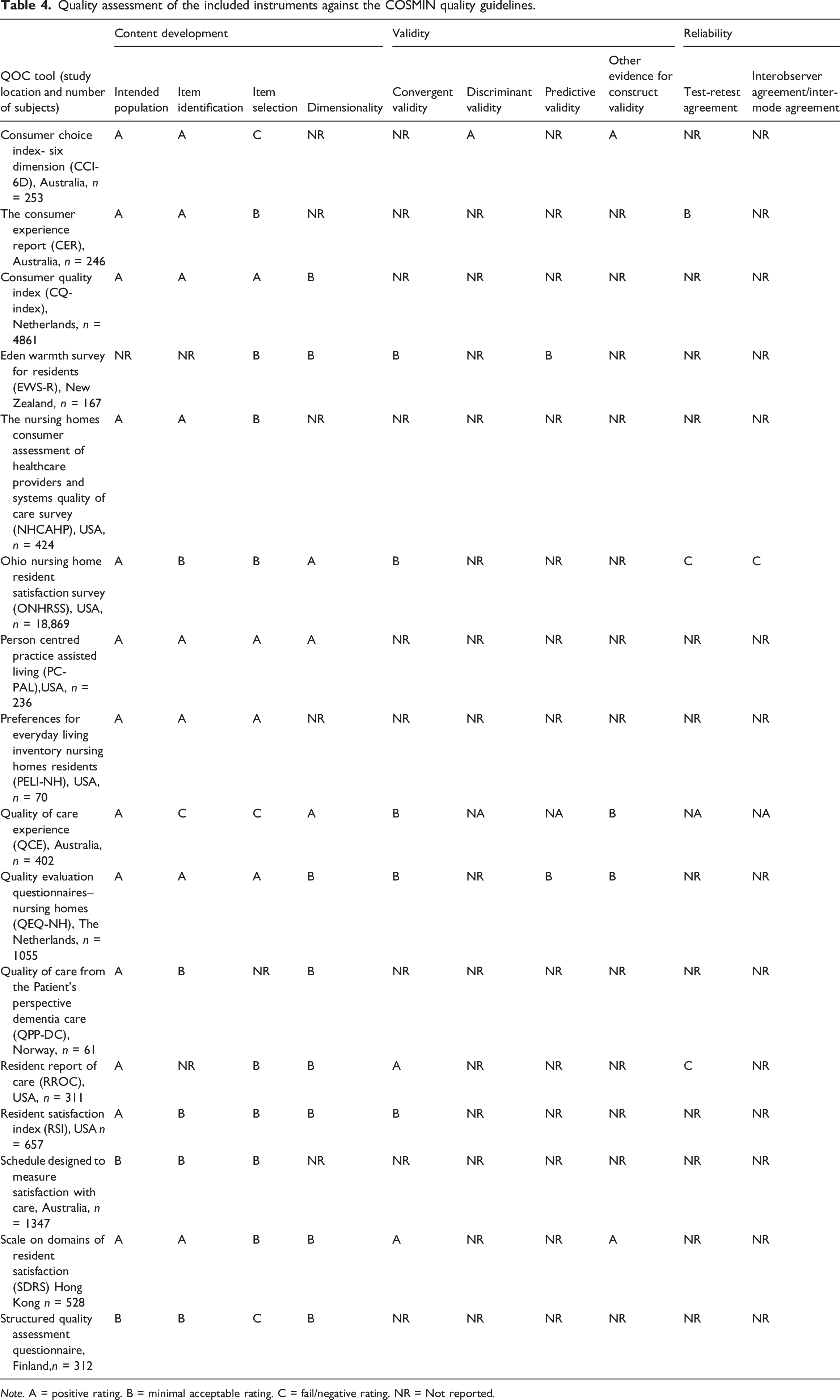
Note. A = positive rating. B = minimal acceptable rating. C = fail/negative rating. NR = Not reported.
In general, none of the quality of care instruments have met all the listed quality criteria, particularly the section of validity and reliability tests. There were either no detailed reports found, or minimal information provided which leaves the instrument with doubts about the strength of the latent constructs to measure the intended construct and, its reproducibility for the target population. Despite the fact that the instruments do not meet all of the criteria utilized, this does not necessarily suggest that they are defective, rather, that they have not been adequately tested and therefore any findings from the instruments need to be interpreted cautiously. In addition, some of the validity and reliability tests were not presented clearly or comprehensively in some of the instruments, so the quality was determined based on the limited information available in the studies. This indicates that more attention needs to be paid to validating the instruments used to evaluate the quality of care being provided to older people and people with dementia in long-term care facilities.
Limitations of the review
The authors acknowledge some limitations to this review. We attempted to make this review comprehensive in identifying existing QOC instruments developed for older people in long term care facilities. However, it is possible that some unpublished research that is not accessible through academic citation databases or the academic grey literature was not have been included. Furthermore, the heterogeneity of the studies precluded the ability to undertake meta-analysis and made drawing cohesive conclusions difficult. Despite these limitations, the review offers valuable perspectives. It provides a detailed overview of the development and validation of the QOC instruments used in long-term care facilities for older people and people with dementia and cognitive impairment, based on the known quality assessment criteria, COSMIN. Also, it highlights areas for further research in developing and validating QOC instruments for older people and people with cognitive impairment in long-term care.
Conclusion
To date there have been very few instruments available for measuring the quality of long-term care facilities which have been developed with the perspectives of older people particularly for those living with dementia. Future research directions should focus on driving the inclusivity and participation of people living with dementia in the development and validation of quality of care instruments including investigating the potential for applied communication enhancing techniques to facilitate self-reporting of quality of care experience wherever possible in this population.
Supplemental Material
Supplemental Material - Are quality of care instruments inclusive of older people living with dementia? A scoping review in long-term care settings
Supplemental Material for Are quality of care instruments inclusive of older people living with dementia? A scoping review in long-term care settings by Digisie M Jemere, Julie Ratcliffe, Jyoti Khadka, Kiri Lay and Rachel Milte in Dementia.
Footnotes
Author contributions
DM Jemere developed the study protocol, performed database searches, coordinated the screening of the articles and drafted the manuscript. K Lay provided support in screening articles. R Milte, J Khadka, and J Ratcliffe supervised the entire process, including protocol preparation, data extraction, and the drafting of the manuscript. They also provided valuable feedback on the revised manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Flinders University Research Support under the Research Training Program (RTP) Tuition Fee Offset for Higher Degree by research students.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.