
Abstract
Research documents the presence of stigma and discrimination as key components in the lived experience of dementia. However, to date, there is limited understanding regarding how social location, particularly as it relates to culture and race, may shape this experience of stigma and discrimination. In this qualitative exploratory study, personal interviews were held with ten Chinese Canadians living with dementia focused on better understanding how culture, race, and dementia stigma influence their experiences. From the onset, themes related to stigma and discrimination were woven into the participants’ stories about living with dementia. Consistent with other research, all participants described an increased sense of vulnerability and invisibility related to how both they and others responded to their diagnosis of dementia. Participants also provided examples of how this experience of stigma was compounded by culture, race, and immigration status. Importantly, these acts of stigma and discrimination were both externally and internally imposed, resulting in feelings of lack of safety and insecurity. This research draws attention to the increased vulnerability that accompanies a diagnosis of dementia and illustrates how this may be heightened by one’s culture and racism.
Introduction
A still pauce but growing body of research documents the stigma and discrimination faced by people living with dementia as a result of their diagnosis (Batsch & Mittelman, 2012; Gove et al., 2016; Milne, 2010; O’Connor et al., 2018; Swaffer, 2014). Research suggests that the lived experience of stigma can be both externally and internally imposed (Swaffer, 2014), often categorized as public-stigma and self-stigma (Corrigan & Watson, 2002; Nguyen & Li, 2018). Stigma fosters feelings of anxiety, shame and/or embarrassment (Maxfield & Greenberg, 2021; Riley et al., 2014; Swaffer, 2014) and has been linked to a reluctance to share one’s diagnosis (Oliveira et al., 2023; O’Connor et al., 2018) and seek support (Gove et al., 2016; Swaffer, 2014). Some research suggests that the experience of stigma can be far more distressing to deal with than the cognitive changes associated with the dementia diagnosis (Katsuno, 2005; O’Connor et al., 2018).
Most of the research focused on exploring the experience of stigma by those living with dementia is based on Western populations (Johnson, 2016; Nguyen & Li, 2018), but there is also growing evidence to suggest that the link between stigma and dementia may be experienced across the globe. For example, studies originating from South America (Blay & Toledo Pisa Peluso, 2010; Gajardo et al., 2022; Oliveira et al., 2023), South Africa (Jacobs et al., 2022), China (Zhang et al., 2020b) and New Zealand (Cheung et al., 2022) all draw attention to the importance of stigma in shaping the experiences of those living with dementia and their families. However, limited research also suggests that there may be geographic contextual differences in how it is experienced. For example, Lion et al. (2020) compared three European countries (the UK, Italy and Poland) and found that those in the UK reported more stigma, as measured by the Stigma Impact Scale, than either Poland or Italy.
The experience of stigma is thought to be particularly relevant in Chinese communities (Dao & Woo, 2014; Woo & Chung, 2013; Woo & Mehta, 2017). A small body of work has been helpful in documenting the impact of stigma from the perspective of the family carer. For example, a study by Baghirathan et al. (2020) in the United Kingdom, describes the paradoxical situation faced by Chinese family caregivers of people with dementia where they realized that they needed support to help deal with the physical and mental exhaustion of caring for someone with dementia but they feared reaching out for this support because of the stigma affiliated with letting other people know that they had a family member who had dementia. Similar findings were reported by Sun et al. (2015) in the United States, where Chinese spouse caregivers reported needing public support because they could not adequately look after their spouse with dementia on their own and did not want to bother their children and grandchildren, but they also feared the repercussions - including the shame - of letting other people know about having a family member with dementia.
There is, however, scant literature on the experience of stigma from the perspectives of Chinese people living with dementia. Notable exceptions include a study by Zhang and colleagues (2020b) that interviewed people with dementia and family members in Mainland China and found that people with dementia reported feeling frustrated by family members who did not accept their diagnosis of dementia and neighbours who were ignorant about dementia. Family members who did accept the diagnosis identified feeling stigmatized and receiving limited support from healthcare professionals who conveyed the impression that it was a waste of time speaking with them given the lack of a cure. In another study, Cheung and colleagues (2022) interviewed Chinese people with dementia and family members in New Zealand: they found that those living with dementia reported being afraid to tell anyone other than their closest family members about their dementia because of the stigma toward dementia in the Chinese community. These studies are important because they begin to hint at the importance of cultural context for interpreting the dementia experience. However, they are limited because while they do address cultural meaning, they do not consider how racism – and other aspects of social location including for example gender and immigration status - may help shape this experience.
Indeed, there is a paucity of more structurally, or critically oriented, research focused on intersections of culture, race, and dementia, especially from the perspective of those living with dementia. Describing this body of knowledge as “sparse and fragmented,” Chejor et al. (2022) conducted a systematic review and meta-synthesis of research focused on the experiences of older immigrants living with dementia and carers. Their review uncovered eighteen studies; only two of these were from the perspective of those with lived experiences of dementia, and neither of these examined the lived experience within the context of a critical lens that attends to culture and race. Similarly, Nguyen and Li (2018) conducted a systematic review of the literature focused on stigma and dementia – few integrated the voices of those with lived experiences, and neither culture nor race was addressed. There is a need for a more nuanced and culturally sensitive understanding of the lived experience of stigma and dementia (O’Connor et al., 2022).
An intersectional lens provides a useful framework for beginning to critically interrogate how social location may shape This lens recognizes that people hold multiple social locations with a mix of intersecting oppressions and privileges attached to these social locations(Collins, 1998a, 1998b; Crenshaw, 1989). Hence, those who embody an intersectional perspective consider how people are multiply situated and how coercive power and systematic oppression cannot be fully understood by asynchronous examinations of structural or relational power (Carastathis, 2014). In contrast to unitary or additive approaches to theorizing oppression, which privilege a foundational category and either ignore or merely ‘add’ others to it, four main analytic benefits are imputed to intersectionality as a research methodology or theoretical framework: simultaneity, complexity, irreducibility, and inclusivity (Carastathis, 2014). At its’ core, an intersectionality lens emphasizes that researchers have to pay attention to the voices of people in marginalized social locations about their lived experiences recognizing that marginalization happens because society tends only to hear the voices of more dominant groups (Esposito & Evans-Winters, 2022): For example, society may hear the voices of Chinese not living with dementia and White people living with dementia but not Chinese people living with dementia.
There has been some, albeit very limited, adoption of an intersectionality lens to understand the experiences of people living with dementia. For example, O’Connor et al. (2010) drew on one woman’s narrative to demonstrate how her social positioning as a younger, lesbian Indigenous woman constructed her experience of dementia in unique and unexpected ways. Similarly, Hulko (2009) draws attention to how privilege associated with gender, socio-economic status, culture and race impacted how a sample of people living with dementia interpreted their day-to-day experiences. More recently, Baril and Silverman (2022) examine the. the intersection of cisgenderism, ableism/cogniticism and ageism in framing the lived experiences of trans older adults with dementia and Westwood (2016) drew on an intersectionality lens to explore how the intersection of ageing, gender and sexuality magnifies dementia concerns among lesbian and bisexual women. This body of literature remains sparse however, and further research is needed to continue to how the experience of dementia intersects with other aspects of social location especially race.
This exploratory study aims to contribute to this important gap in knowledge by centering the voices of Chinese people living with dementia in order to consider how race (and racism) intersect with experiences of dementia-related stigma and discrimination. Two primary questions guided the research: What does dementia-related stigma look like in the experiences of Chinese-identified adults living with dementia, and how do culture and race/racism help shape the narration of their experiences? The purpose is to begin to develop a more complex understanding of how one’s social location helps to shape the lived experience of dementia.
Methodology
This study was part of a larger Participatory Action Research (PAR) study focused on understanding and taking action to combat the stigma experienced by people with dementia. [For further details, see https://www.flippingstigma.com/.] To ensure cultural diversity in this broader study, purposive sampling included seeking input from individuals from several diverse communities (South Asian, Spanish-speaking and Chinese) in the Vancouver area of BC. This paper focuses on the experience of people living with dementia in the Chinese community in Vancouver, Canada. The full study, including this smaller sub-study, received ethics approval from the Behavioural Research Ethics Board (BREB) of the University of British Columbia.
Semi-structured interviews were conducted with ten individuals who self-identified as culturally Chinese and living with dementia or cognitive impairment: We included people who self-identified as having cognitive impairment because some literature suggests that within the Chinese, the language of “cognitive impairment” is less stigmatizing than “dementia.” (see for example, Zou et al., 2017) . Aside from a willingness to talk about their experiences of living with dementia, no other criteria (e.g., age, duration since diagnosis, gender, immigration status etc.) were placed on eligibility, given that this was seen as an exploratory study with existing challenges related to recruiting a hard-to-reach population.
The interview began broadly by asking participants, “Tell me about your experience living with dementia?” This very open-ended question was followed by a series of probes, which included: “Have people treated you differently since your diagnosis? How have you responded to the treatment by others? Are there changes in what you do?” and a cultural probe (when not spontaneously volunteered) to explore how being Chinese influence their experience? If participants did not spontaneously speak to issues related to race/racism and/or dementia stigma, the topic was raised by the interviewer.
Recruitment and data collection mostly took place during COVID so were restricted to ZOOM or telephone contact. Four community organizations working with Chinese people and people with dementia agreed to help promote our study. Once we received a positive response, we sent out a poster with a brief summary of our study and our contact details which was then circulated to their service users through emails and word-of-mouth. We recruited five participants using this strategy. Based on recommendations from a service provider, who highlighted the use of local Chinese TV for conveying information, we emailed the local Chinese TV channel with our poster, and they advertised the study by announcing the information on the poster in their daily community news section. By far this was the more effective recruitment strategy as five people responded within weeks of the advertisements.
Based on personal preference, participants were interviewed either by ZOOM (n = 4) or by phone (n = 6). Participants also had the choice of being interviewed individually or with another family member – six chose to be interviewed alone, and four preferred to be co-interviewed with their spouse. The rationale for giving participants the choice to be interviewed with another person was to ensure that the participant felt as comfortable as possible. For those who were co-interviewed, the meeting began by reminding each participant and their accompanying spouse that this study was very much focused on hearing the voices of those with dementia diagnosis. This was respected by the spouses, who mostly saw their role as helping to convey complex ideas, providing supplementary information to the interviewer to facilitate the interview process, and, at times, clarifying details when the person with lived experience seemed to be having challenges. (For example, when one participant had difficulties trying to explain where he went in Chinatown, his spouse helped by noting that he was talking about a recreational centre for older adults.) When the family member added information/insights, the participant was invited to verify that they agreed with what the family member had contributed.
Demographics of participants.
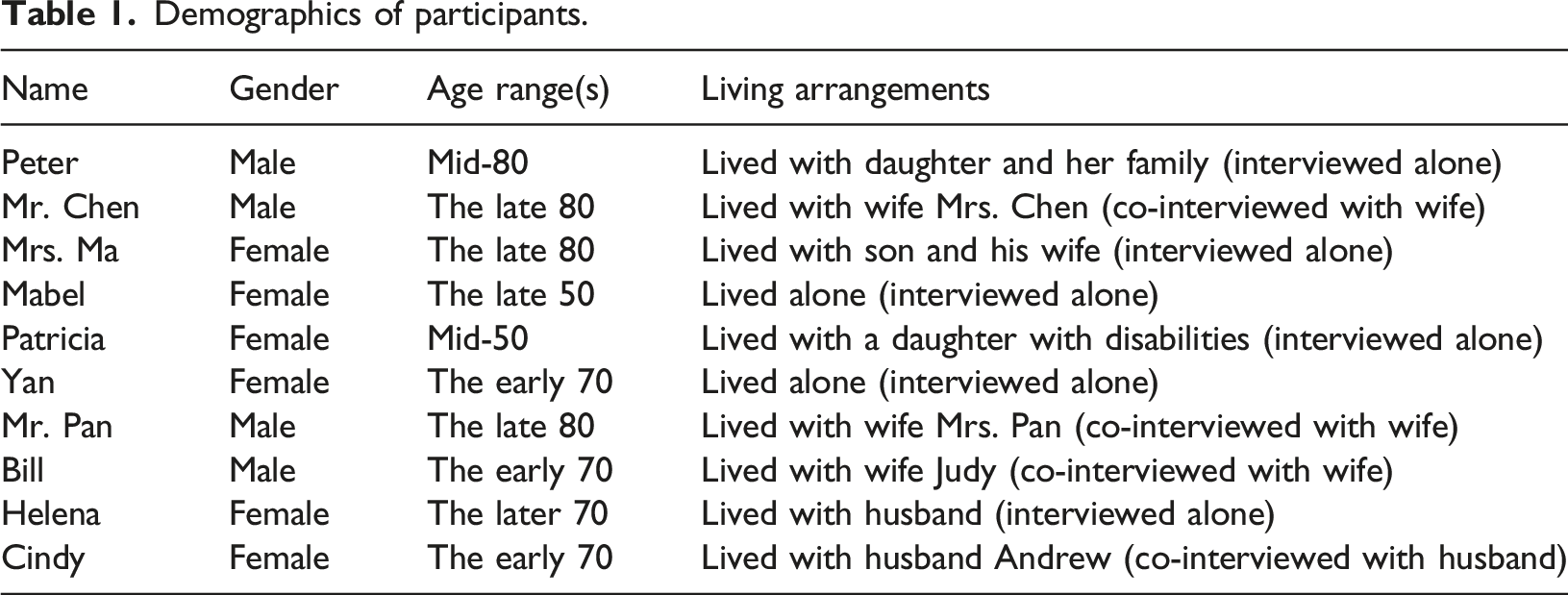
All interviews were conducted by the first author (KW) in the language of their choice (English or Chinese). All chose to be interviewed in the language of their birth – for nine participants, this was Chinese, and only one chose to be interviewed in English. It is noted that while the interviewer is fluent in both languages, her first language is Chinese, and upon reflection, she queried that this may have facilitated a relational closeness with the Chinese-speaking participants that was more difficult to achieve with the English-speaking participant.
Each interview lasted between one to 1.5 hours long. With the participant’s consent, the interviews were audio recorded and then transcribed verbatim (to the extent possible) by the first author/interviewer in the language of the interview; the Chinese transcripts were then translated into English in order to facilitate team analysis since the other two members spoke only English. To ensure the accuracy of the translation, snippets of the interview were randomly selected and back-translated into Chinese, compared to the first version and then, where necessary, the English version was adjusted. This process was time-consuming but useful as it insured that the transcripts reflected as closely as possible what participants had said.
Data analysis
Data analysis was ongoing throughout the interviewing process to identify emerging themes and help direct purposive recruitment. One strategy for analyzing the transcripts was based on Gilligan (2015) listening guide method. This method is an approach to “listening to” the different interview voices and was chosen because it has been used in other research to understand the experience of stigma (Gilligan, 2015). It has three steps. The first step is “Listening for the Plot,” in which researchers listen for the contexts where participants socially locate. The second step is “Listening for the I,” in which researchers pay attention to the parts where participants use first-person voices about their actions and being. The final step is “Listening for Contrapuntal Voices”. These voices may come from the participants. However, they may be from other people, but participants relay them in the interviews. They are often contrapuntal to the parts where participants use first-person voices. For example, in our study, participants saw the world differently from the people around them. However, people around them did not understand, stigmatized them, and said hurtful things to them.
A unique aspect of this study was the collaborative team discussions that contributed to understanding and moving the analysis forward. In conjunction with the initial analysis using Gilligan’s listening guide, the three authors met regularly via ZOOM to interrogate the emerging findings. Each meeting was about an hour to 1.5 hours. This research team consisted of a senior researcher (DO) who is an older white woman with a background in gerontological social work and extensive experience researching with people with lived experience, a doctoral candidate (KW) who is a younger Chinese immigrant woman with a background in Social Work, and a Black American man who has been living with dementia for over 13 years (GJ) and who drew on his insights around his own experiences related to culture and racism in order to raise questions of the data and push the analysis deeper.
There is no ‘one’ way to interrogate intersectionality as part of the analytic process. McCall (2005) suggested three approaches, each with different stances on considering categories of social locations in understanding the complexities of people’s lived experiences. The anti-categorical approach, informed by post-structuralist and post-modernist paradigms, suggests a deconstruction of categories. The challenge of this approach is that researchers may have limited clues about where to start to understand people’s lived experiences without even temporary categories. In opposition, informed by the positivist or post-positivist paradigm, the inter-categorical approach suggests the provisional adoption of existing categories. Researchers using this approach tend to be more interested in examining the relationships of inequalities among social groups based on existing defined categories. The downside of this approach is that it restricts researchers’ abilities to grasp the complexities of the lived experiences of people within the same social group. The third approach, an intra-categorical approach, attempts to bridge the limitations of the anti-categorical and inter-categorical approaches by encouraging researchers to temporarily use existing categories but with the flexibility to move between the two approaches. Given the exploratory nature of this study, this third approach guided our analysis. Specifically, we temporarily drew on the categories of race, culture, and dementia and throughout the entire analytic process, analytic sub-questions focused on reading race, culture, and lived experience of dementia and dementia-related stigma and considering their interactions. We continuously asked the texts, what was being conveyed about race, culture, and dementia stigma in how a participant talked about their experiences and the stories they told. These insights then guided further analysis and interviews as we attempted to refine and validate our reading/analysis. We also practised reflexivity through group discussions. Through these discussions individual understandings were extended and developed through the insights shared by other members of the analytic team.
Findings
Themes related to stigma emerged early and spontaneously as an essential part of the experience of living with dementia and were woven into all participants’ stories. Although the language of ‘stigma’ or ‘discrimination’ was not necessarily used, consistent with other research, all participants described an increased sense of vulnerability and invisibility related to how they. and others responded to their diagnosis of dementia. While some of this was linked to the changes in cognition they were experiencing, often it was clear that it was perception rather than the reality of these changes that were shaping both their responses and the reactions/responses of others. Participants' stories suggest that this experience of feeling marginalized and/or discounted was compounded by culture and race but in ways that were sometimes very difficult to tease apart.
The following section will begin to describe how the intersection manifested in the participants’ lives through their stories. Recognizing the importance of ensuring that the voices of those who are being ‘erased’ narrate the stories being told (Haynes et al., 2023) we have tried to draw in the actual words and stories used by the participants themselves.
Dementia stigma: Developing a cultural context
From the onset, participants’ stories recognized the dangers of stigma associated with dementia. Most discussed their concerns that others either explicitly or implicitly discounted them based on their diagnosis. Importantly, their stories suggest that this discrimination could come from both within and outside the Chinese community. For example, Peter is a person with dementia in his mid-80s. He is a widow and lives with his very busy daughter and her family. Prior to his diagnosis, he maintained active friendships within the Chinese community and was well-known in the Chinese community for his outstanding volunteer work which included helping the Chinese Christian church organize events as well as driving other older Chinese adults to medical appointments. Hence, he described himself as a “useful” person. However, following his diagnosis of dementia, he believes he lost his standing within his community, and people no longer came to him for help. Poignantly, Peter used a dustpan metaphor to describe his sense of loss of purpose: I feel that I am still useful. [emotional voice] I feel that people can use me! However, when I offer to help, people decline my offer. I feel I am useless. I am just like a dustpan. People used to use the dustpan, but they no longer needed it. (Peter)
Even his friends have begun to withdraw. He describes his increasing social isolation within his Chinese community, which he believes is caused by how his friends - whom he explicitly positions as ‘immigrants from China - see his diagnosis pejoratively: They are immigrants from China. In the beginning, two or three out of ten friends still contact me. It changed. I used to have a group of friends. We have been knowing each other for many years. Before, we would have gatherings. However, gradually, I don’t hear from them. (Peter)
Peter believes that he was no longer hearing from them because they are afraid of his diagnosis and the implications that they might be at risk from him and/or need to provide care to him. They [are afraid that they will] need to take care of me when they go out with me. They fear of my safety. So, they try to avoid having me. However, if I were them, if I had a friend who had care needs, I wouldn’t avoid having this friend. I would give a ride to this friend and came with him to the gathering. (Peter)
Other participants similarly talked about their experience of being discounted and loosing their voice with references to their Chinese culture. For example, Yan spoke haltingly about how her friends began to label her as ‘foolish and crazy’ due to her memory changes. This has resulted in her increasing isolation. She used to own a Chinese restaurant which she ran by herself and described herself as “smart and capable.” However, when she realized her memory problems, she became increasingly disconnected from her friends, fearing they would discount her and see her as even “more foolish and crazier” if she were to speak of her memory loss. Her response is to try to hide her dementia. I seldom tell other people [friends in the Chinese community] [about my diagnosis]. Well, those people think that I am foolish and crazy. [Sighs] Well, they already see me as foolish and crazy. If I told them that I think I have a memory issue, they would see me as more foolish and crazier. (Yan)
She felt silenced and unable to challenge the perception of her friends, ironically fostering their pejorative ideas that she was foolish and crazy (rather than suffering from a medical condition). Yan’s response to the fear that those in the Chinese community will use her diagnosis against her begins to demonstrate how participants perceived dementia as silencing and increasing one’s vulnerability.
Others talked about having their symptoms discounted and, again, contextualized this response within their Chinese background. For example, when Mabel wanted to talk to others about her dementia, she thought of her sister. She described her sister as a traditional Chinese woman who was caring and thoughtful. She thought she could share her concern about dementia with her sister, and her sister would understand. However, when she told her sister about her concerns, her sister discounted her concerns, attributing them to her poor sleep quality and worrying too much. My sister won’t believe that. We don’t have anyone in the family with dementia or Parkinson’s. She said that I just worry too much. She said I don’t sleep well, and lack of sleep can affect my memory too. (Mabel)
Another participant, Mrs. Ma went to her family doctor and expressed her concern about dementia. Her doctor told her that her memory is still good. This shut her down, and she did not ask further questions. Perceiving her concern about dementia as being discounted, she lost the opportunity to pursue the issue with further questions: I went to see the doctor. He talked to me for a while and said, “Your memories are still quite good.” After he said that, I did not continue to ask more. (Mrs. Ma)
Faced with a similar response from her physician, Patricia queried the extent that she was being silenced related somehow to culture. Patricia had the medical background to recognize the symptoms of dementia and began to pay attention to her own worsening cognitive functioning. When she experienced several accidents - including starting a small fire when she forgot to turn off the stove and flooding her home because she forgot to turn off the tap - she promptly sought medical advice. Here, she met with a dead-end. To access necessary diagnostic tests, she required a referral from her family physician, but he kept telling her she was fine and refused to make the referral. Well, I am sorry to say that, very often, doctors do not believe what patients say … I don’t want him [the family doctor] to make an excuse by saying, “You don’t have the problem.” Do I need to wait for the doctor to believe me until an accident has happened? I don’t want that. I want to be proactive. I don’t want to give him an opportunity to make excuses by saying, “You are just too worried.” … I can sense that my doctor does not want to make the referral. (Patricia)
Situating this experience within her cultural background, Patricia queried whether she was being discounted because her family doctor was Chinese. She compared her experience seeing her Chinese family doctor and a Caucasian doctor in the walk-in clinic. She commented that Caucasian doctors were more willing to spend time with their patients than Chinese doctors. He (family doctor) is Chinese … I am sorry to say that, but Caucasian doctors usually spend more time with a patient than Chinese doctors. (Patricia)
It is unclear whether or not the Caucasian doctors spent more time and if so, it is unclear why. However, what is important to note is that this was Patricia’s perception, and her heightened regard for Western healthcare professionals was an important part of her story. Did this reflect the internalization of racism? Did this reflect the residue of colonization propagating the dominance of a Westernized lens? Interestingly, research suggests that it is important to have a service provider whose racial and cultural backgrounds match the clients (Delman & Adams, 2022) but Patricia’s example demonstrates that cultural biases and stereotypes related to dementia may be internalized in ways that counter this suggestion.
Almost all the participants spoke to the increasing isolation they were feeling related to the diagnosis. Most also explicitly linked this to concerns regarding how others were responding to their diagnosis. Complicating this relationship, it is noted that interviewing for this study took place during the COVID pandemic which led to even more exclusion. For instance, Mr Pan often went out to the Chinese church. However, due to his cognitive and leg deterioration and having no one to bring him to church, he stayed at home most of the time. COVID-19 intensified the isolation. Interviewer: Do you miss going out? Mr. Pan: I am not going out. Interviewer: Why? Mr. Pan: Because of the pandemic.
Hence, while it was clear that all participants felt increasingly isolated, it was not entirely clear the degree that this isolation was compounded by the pandemic compared to the stigmatizing attitudes of family and friends. However, participants’ stories consistently identified their fear of disclosing their diagnosis related to concerns as to how others would react, fears that, based on their previous experiences, were often not unfounded. This is not inconsistent with general research examining the lived experience of dementia stigma (see, for example, (O’Connor et al., 2018)). However, what is unique about these participants’ stories is that all of them explicitly grounded their experiences of isolation and feeling discounted within their cultural context, suggesting that the perceived dementia stigma is, at least in part, culturally informed.
Cultural loss
Dementia is often presented as a time of loss. In this study, participants’ stories drew attention to loss related to cultural connections and voice. For example, Mr Chen described the importance of Chinese dim sum as essential to his weekly routine before his diagnosis. However, as his dementia progressed and his legs deteriorated, it became increasingly difficult for him to continue this tradition. He could not depend on his wife, as she also had health issues, so the couple became increasingly dependent upon their son and his family to go for Dim Sum. However, although his son lived locally with his wife and daughter, he was busy with work, and his Caucasian daughter-in-law spoke only English - which Mr Chen and Mrs. Chen could not understand – and disliked Chinese food. Excursions for dim sum became increasingly rare. During the interview, Mr Chen repeatedly talked about how much he missed Chinese dim sum, a loss that he linked to his dementia. Mrs. Chen: Well, they (daughter-in-law and granddaughter) don’t eat Chinese food. Interviewer: So, what do you like to eat? Mrs. Chen: We, of course, like Chinese food. Interviewer: How about you, Mr. Chen? Mr. Chen: I don’t have a preference. Well [stop for a few seconds), I like Chinese food, though.
While on the surface, this could seem insignificant, Mr Chen was clear that this was experienced as an important cultural loss with many meanings. First, he lost going to dim sum, his favourite cultural food and participation in cultural practices. Second, considering dim sum was a representative of Chinese cultural food, he lost his cultural connection, which was a vital part of his cultural self. He was disconnected from his cultural community. In this situation, Mr Chen felt his preferences were usurped by his daughters-in-law’s dislike of Chinese food. Mr Chen was clear that he saw this in some ways as a denial of the importance of his culture in this experience.
It is unclear the historical relationship between the Chen’s and their daughter-in-law: The relationship between the couple and daughter-in-law might be far more complicated and multi-faceted. However, it is significant that Mr Chen drew attention to this loss, which he blamed on his daughter-in-law. What was not said explicitly but implied was that Mr and Mrs. Chen expected that their daughter-in-law should be willing to meet their cultural dietary choice: Did the daughter-in-law even know their expectation, especially since she came from a different cultural background? Why did the couple only have expectations of their daughter-in-law but not their son? Mr Chen’s narrative raised questions about dementia as representing cultural loss but this theme was not well-developed by other participants.
Intersections of dementia with culture, race, or immigration status
Beyond an understanding that dementia stigma is culturally contextualized, this data begins to hint at the complexity of teasing out how racism intersects with dementia-related stigma. Participants’ stories repeatedly revealed the intersections between dementia and culture, race, and/or immigration status of people with dementia and how these worked together in ways that could not necessarily be named but increasingly leave one feeling vulnerable (See Figure 1). When asked about their experience of stigma related to dementia, seven out of ten participants spontaneously brought up culture, race, or immigration status elements in their experience. Intersection of race, culture, immigration status, and dementia stigma.
Mabel provides one example of how race and dementia are intertwined. One time it [discrimination] was obvious. I went to the supermarket. I was going to pay. I could not find my purse. The person lining up behind me said, (raising voice), “You Chinese, get away!” I said, “I am just finding my purse.” They said, (raising voice) “Get out! Get out of this way!” (Mabel)
While she attributed at least part of these experiences to changes related to her dementia, clearly her behaviour was interpreted within a racist framework. Once outgoing and sociable, Mabel began restricting her activities and interactions with others. For example, she discussed how this experience interfered with her willingness to disclose her diagnosis to a Caucasian friend of many years, given the anti-Asian sentiment she had encountered and how this might shape the interpretation of her dementia. I have known this colleague for 30 years. She is sincere. Since my experience being shouted at by a Westerner in the supermarket, I hesitate to tell her my condition. I was afraid that she would disconnect from me. I will lose my only friend. (Mabel)
Mabel provides more insight into how her symptoms of dementia could easily be interpreted through racist or anti-immigrant lenses. Mabel had immigrated to Canada many years ago and had mastered public transportation. However, with the onset of her dementia, she found taking buses increasingly challenging, could not keep track of the many stops and routes, so she began walking instead. Her Chinese colleagues, who were also immigrants to Canada, assumed that being an immigrant coming to Canada for a long time, she should be able to take buses. Mabel: I said that I don’t know which bus to take. Other people said, “You have already been to Canada for many years. You don’t know how to take a bus?” I said, “I seldom take the bus. I walk.” Then they said, “You need to learn now. Otherwise, you can’t take the bus in the future.” They say things like that often. Interviewer: Sorry to interrupt. Did you mean other people on the bus? Or people at the bus stop? Mabel: No, they are my colleagues … the Chinese colleagues.
Even those who knew about her dementia diagnosis failed to link her increasing discomfort with public transportation to her diagnosis, pejoratively viewing her as a ‘bad immigrant’ instead.
Mabel was not the only participant to speak explicitly about the complex link between dementia and one’s social location. For example, compared with most other participants, Patricia was relatively young, in her mid-50s, and was still employed as sales help in a medical supply shop. She recalled an incident where a Caucasian customer came into their shop with frustration, saying that he had been served by a Chinese staff and wanted to complain about this staff person. The customer could not recall the staff who served him but, seeing Patricia assumed it had been her since she was Chinese. This client probably didn’t recognize Chinese faces or just wanted to express his frustrations or find someone to blame. This client blamed me. (Patricia)
Patricia did not think she had served this customer. However, she could not tell for sure because of her poor memory. She was not confident to speak up to protect herself. As a result, she remained silent and increasingly vulnerable. I could not tell for sure whether or not I served him. Whatever gau si laap saap [note: This is a Cantonese idiom. Its literal meaning is dog shit and rubbish. People use this idiom to refer to bad things] happens, they [customers] will blame me. (Patricia)
Patricia makes clear her sense of vulnerability and inability to protect herself at least in part due to her diagnosis. Her story makes visible the complex intersection of racism and dementia. Similarly, her positioning as a Chinese woman is drawn in to help make sense of her experiences. Patricia was raised in a traditional Chinese family where men have historically had more say than women. She described a longstanding history of being taken advantage of by her brother financially: He owned a shop, and she used to work for him, but he refused to pay her salary. However, she could not challenge him because of her brother’s elevated status in the family as a male. Even though she no longer worked for her brother, she felt especially vulnerable given her dementia. She feared alerting him to her failing memory because she felt he would use this as an excuse to discount and invalidate her. I was afraid of telling him that my memory is poor. If I told him, he would say, [raising voice] “Your memory is poor! You haven’t returned many things to me yet!” I was afraid to tell. I don’t want to argue with him … You with good memory bully a person with poor memory…
Helena is in her late 70s who came to Canada about 30 years ago. Following a preliminary diagnosis of early-stage dementia by her family physician, Helena was referred for a more comprehensive assessment. Upon her arrival, she describes meeting a “White man” with whom she tried to speak. However, her proficiency in English has deteriorated as a result of her diagnosis, and rather than attempting to work with her to understand her limited English, he sent her away immediately to ask for a staff who could speak Chinese. The White man said, “When you are there, tell them (the staff) that you need someone who speaks Chinese, they will have someone to assist you. I asked him a couple of times, “May I talk to you?” He said, “No.” (Helena)
Helen remembered her frustration at being sent away immediately without any attempt to try and communicate. She felt discounted that she could not expect someone to even try to talk with her. Whether intentional or not, this was felt as linked to her status as an aging Chinese woman who was not important enough to even try talking to.
Subtle racism could be internalized by people living with dementia. Cindy believed that one way to slow down her cognitive decline was to keep herself active, so she joined a senior activity group at the local community centre. As she highlighted several times, the group was facilitated by “a White woman”. Cindy took pride in helping the facilitator with the group, for example, assisting with set-up and take-down before and after the group. Cindy described an occasion when she invited the facilitator to join a gathering with her and her Chinese friends at her home and the joy she felt when the facilitator showed up. I tried to invite her (the facilitator) to my home. She really came. I never thought a White person would come to my home. We Chinese usually only gathered among ourselves. I never thought she could come. What made me even more touched was that she invited me to her home. She said, “Next time, please come to my home.” I was so happy. I have never been invited to a White person’s home. Never! So, I was so happy. I was so happy! (Cindy)
While there are undoubtedly many reasons why Cindy was so touched, she emphasized the facilitator’s ‘whiteness’ several times in telling this story, suggesting that, at least on some level, the facilitator’s race mattered to her. Within a context of internalized racism, one interpretation is that Cindy might have felt especially flattered by being seen as ‘deserving’ when a White person treated her kindly by giving her the opportunity to volunteer within her cognitive abilities, coming to her place, and inviting her into her own home.
While Cindy’s link between her experience and race is explicit but not clear, other participants were more explicit about hinting at the systemic stigma they experienced both because of their race and because of their dementia. This was most clearly identified by younger participants. For example, Mabel, in her early 50s and still employed at the time of her diagnosis, believes she was fired because of her dementia. After a week’s hospitalization, explained by a physician’s letter, she returned to work to find that she had been replaced by a new colleague. When Mabel asked her supervisor why she was replaced, she indicated that Mabel had been away from her position for too long. Mabel challenged this, including drawing on the doctor’s letter to verify that she had been away for an appropriate medical reason. My supervisor asked me to go to the conference room. She said that my job was no longer available. I asked why. She said that when I was not in the office, someone else replaced me. I said that I had a sick leave letter. She said, but the position was demanding. I said that I was only away for a week, and it was not reasonable to have someone to replace me. (Mabel)
Mabel asked her union for help. Unfortunately, they did not support her and instead of returning to her position, Mabel was fired. When Mabel was asked whether she felt that there was discrimination Mabel said (raising her voice), “Definitely!” Mabel linked this discrimination to both her diagnosis but also to racism, noting that: “My supervisor is a White woman. I later found out that she wanted her niece in England to fill my position!” The loss of her job resulted in financial disarray, a loss of status as a working person, and left her feeling that she no longer had meaningful purpose in her life. Mabel felt impotent to fight this injustice.
Stigma in the system could also be found in older participants living with dementia. Unsurprisingly, this was manifested most clearly by the lack of attention to language. For example, Helena, diagnosed with early-stage dementia, heard on the local Chinese radio program about a community organization that provided services to support people living with dementia. When she contacted the organization, she was able to speak to a Chinese social worker who recommended a self-support group…but then noted that the group was held only in English. Because her English had deteriorated after her diagnosis, Helena declined to join the group despite her interest: The social worker said their activities are for White people. That meant they are primarily in English. If they are in English … I already have limited cognition, and my pace of understanding of what other people say is slow. How can I understand what people in the group say? I think if it is in my language, it would be better as I can understand what other people say.
Interestingly, the organization promoted the self-support group as welcoming people from diverse cultures and races in their promotion materials. For example, Helena noted that the front cover of the brochure had a picture of participants coming from diverse cultural and racial backgrounds. She said, “I saw in the picture that there are some White people, men and women, also Chinese, sitting together in a circle.” However, in maintaining English-only practices, the reality that many people who speak a second language may experience challenges maintaining proficiency following a diagnosis of dementia is clearly not addressed, and the support implicitly became exclusionary.
Of note, while several of the stories told by participants hinted at an awareness of themselves as Chinese immigrants in a context of increasing anti-Asian sentiment, only three of the participants explicitly named their experiences as ‘racism’. The degree that this was related to a lack of safety is unclear. However, of the three, one participant felt so uncomfortable that toward the end of the interview, they requested that any content related to racism be excluded from their transcript. He felt it was too risky to expose himself even within the confines of assured anonymity and even though he was being interviewed by another Chinese person. Per his request, the content related to racism was removed.
Discussions
There is a growing body of research linked to the experience of dementia-related stigma but much of this fails to draw in a critical or intersectional lens to consider how social location informs the experience. In other words, power is missing in the analysis. This exploratory study extends this literature by centering the voices of Chinese people living with dementia in dominant Western society, beginning to draw attention to the complex relationships between dementia, culture and race. We draw attention to two main insights. First, the stories told by participants suggest the importance of culture in shaping the meaning of dementia, sometimes in ways that may aggravate social isolation and loss. None of the participants suggested a cultural meaning of dementia that was not exclusionary and stigmatizing.
Second, the stories hint at the complex entanglement between racism and dementia stigma, suggesting that the two work together to construct situations that are especially disempowering and difficult to challenge. Specifically, while not a fully developed explanation, participants’ stories, at a minimum, begin to suggest how easily their dementia could create the space for a racist interpretation as well as demonstrate how the perceived vulnerability related to their dementia leaves them unprotected in situations of explicit racism and/or violation of human rights. Especially given the documented rise in anti-Asian racism (Zhao et al., 2022) this is an important issue to be aware of and address.
This study resonates with, and extends, existing research in several ways. The findings are consistent with previous literature that documents the existence of stigma within the Chinese community towards people with dementia (Baghirathan et al., 2020; Cheung et al., 2022; Mahoney et al., 2005; Sun et al., 2015). Within this study all the participants acknowledged feeling stigmatized as a result of their diagnosis and linked their experience of stigma to their cultural background and community while also highlighting that the loss of cultural connections may be an important issue to understand. However, stigma could also happen outside the Chinese community, as demonstrated by Mabel’s case in multicultural work setting. This raises questions regarding the need to look both within and beyond the Chinese community to fully understand the lived experience of dementia stigma.
Second, previous literature suggested that stigma is both externally imposed (public stigma) and internally imposed (self-stigma) (Swaffer, 2014). This study supports the interweaving of these, illustrating how these two types of stigmas can occur simultaneously and build and foster one another. Importantly, it suggests that racism may compound this. For example, Patricia’s experience with her customer provides an insightful example of how a Chinese person with dementia can concurrently experience externally and internally imposed stigma. She was subject to an unfair complaint by a customer because of her race, but she hesitated to challenge him due to her dementia. A similar point was raised by Gajardo et al. (2022)’s study in Chili that self-stigma could be an internalization process of external stigma. Recent literature thus raised how emotionally unsafe people with dementia could be because of constant concurrent public stigma and self-stigma (Grobosch et al., 2023) – this study highlights that this may be even worse within the context of racism.
Third, this study supports previous literature that loss of voice and discounting may be more structurally imposed. For example, some research has found that health professionals might be less willing to spend time with those living with dementia (Sun et al., 2014; Zhang et al., 2020a) – this was the perceived reality for four of the participants. As a result of their own uncertainty and recognition of how people responded to dementia, participants felt uncomfortable making demands and/or exerting their needs for support. Moreover, previous literature in China and the Chinese community in New Zealand also suggested that even if the person with dementia told their family members, including those closest to them, about their dementia, their family members tended not to believe them (Cheung et al., 2022; Zhang et al., 2020a) – this was mentioned by a few participants as an issue in this study. Importantly, challenges to second language retention, often affiliated with a dementia diagnosis, further foster silencing as those who cannot speak English are excluded from available support.
Perhaps most significantly, drawing on a critical intersectional lens, this study extends the research by beginning to address the gap in knowledge regarding how dementia stigma intersects with culture and race in significant and complex ways. While culture, race, and immigrant status are different concepts, they are closely related to each other, as there are high overlapping among racialized people, cultural minorities, and immigrants (Haralambous et al., 2018) – the study begins to shed some, albeit limited, light on this intersection. Further research is clearly needed to deepen insight into these relationships.
Limitations of the study
While this small exploratory study begins to open for scrutiny an important gap in the literature, it only reveals the ‘tip-of-the-iceberg’. In particular, the sample is very small, and composed solely of participants living in an urban city where there is a substantial Chinese population. Other aspects of social location – for example, gender, age and geographic living space (urban or rural) - are not considered, although some of the data here, as well as other literature, suggests that the experience will vary considerably. For example, while the sample was too small to meaningfully reflect age, we noticed that some of the issues related to systemic marginalization looked different for the two younger participants (Mabel and Patricia), whose experiences centered around their treatment within the workplace. For future researchers’ consideration, a broader intersectional approach, which considers the complex interplay of dementia stigma and racism with other aspects of social location, such as age, is needed.
Second, some literature suggests people living with dementia could build resilience and even grow because of dementia stigma (Seetharaman & Chaudhury, 2020; Whelan et al., 2020). In this study no-one drew on understandings that could suggest a link to support, resilience, and/or growth but this may be reflective of a methodology and analysis that focused on stigma and racism. Future researchers may ask invite participants to think about support, resilience, and/or growth.
Implications
This study highlights the importance of insuring that the voices of people with lived experience of dementia from diverse racial and cultural backgrounds are included in research, policy and service planning. There is increasing attention to involve people living with dementia as co-researchers and/or service users. However, too frequently, this translates as the inclusion of predominately White, socio-economically privileged (Fitzgerald et al., 2019; Wilkinson & Weaks, 2008). As narrated by participants in this study, race and culture matter in both how dementia is understood and experienced.
A lesson learned in this study was the importance of different venues for successfully gaining access to relevant participants. Initially, the use of conventional standards for recruitment (for example, targeting gatekeeping, culturally appropriate service) was only partially successful despite strong relationships between the researchers and the organizations. Shifting to a venue (the Chinese television station) that was well-embedded in the community was far more effective and revealing. The reason for success through advertising on Chinese television still needs further exploration. One possible reason might be that many Chinese people, especially those in middle and old age, accessed information through Chinese television. Another explanation may be that this venue is more ‘normalizing.’
Conclusion
This qualitative study explored the lived experience of dementia stigma from the perspective of Chinese adults living with dementia. It draws on critical intersectional theory as an analytic lens for exploring the complexity of social locations. Although only exploratory, it does support existing research on the importance of dementia stigma as a concept for silencing and draws attention to how this disempowerment and silencing is amplified within a context of Anti-Asian racism.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institute of Health Research.