
Abstract
Objective
The main aim of this study was to evaluate the feasibility and acceptability of using a GPS tracker to mitigate the risks associated with wandering for people with dementia and those caring for them and further evaluate the impact of trackers in delaying 24-hour care and the potential for reducing the involvement of support services, such as the police, in locating patients.
Methods
We recruited forty-five wearers-carers dyads, and a GPS tracker was issued to each participant. Dyads completed pre-and post-outcome questionnaires after six months, and a use-log of experiences was maintained through monthly monitoring calls. At six months, focus groups were conducted with 14 dyads where they shared ideas and learning. Data analyses were performed on outcome questionnaires, use-log analysis, and focus groups discussion.
Results
A 24% (N = 14) attrition rate was recorded, with 76% (N = 34) of the participants completing pre- and post-outcome questionnaires, of which 41% (N = 14) attended four focus group meetings. Participants reported enhanced independence for wearers as fewer restrictions were placed on their movements, peace of mind and reduced burden for the carers with less need to involve police or social services, and delays in 24-hour care.
Conclusion
The results supported the feasibility of routine implementation of GPS trackers in dementia care with clear guidance, monitoring and support to family carers on safe use. This could delay admission into 24-hour care as wearers and carers have a greater sense of safety and are better connected should help be required. Studies with larger sample sizes, diverse participants and health economic analysis are needed to develop the evidence base further ahead of the routine implementation of GPS trackers in health and social care services.
Introduction
Maximising the time people with dementia can live independently has become a public health imperative (Department of Health, 2016). Dementia is the leading cause of death in women in the UK and one of the most significant causes of disability and dependency among older people globally (WHO, 2022). Over 55 million people estimated to live with dementia worldwide and forecast to rise to 139 million by 2050 (Alzheimer’s Disease International, 2022). It is estimated that 60% of people diagnosed with dementia will get lost at some point, with many doing so repeatedly (Alzheimer’s Association, 2023). Bantry-White and Montgomery (2015) found the risk of getting lost partly account for the placing restrictions on people with dementia. Incidences of wandering in the community often lead to admission into 24-hour care (Bartlett et al., 2019), Carers might be embarrassed and guilty reporting family to the police, with a negative reaction by people with dementia (Shalev Greene, et al., 2019). When people with dementia are missing, the consequences can result in severe injury and death with the attendant emotional trauma for carers (Lindeza et al., 2020), and a considerable financial burden for the services that may be called to find or rescue them. Carers cohabiting with people with dementia will experience a significantly greater burden and poorer psychological well-being than those who dn not (Brini et al., 2022), due to a restricted social life for the carer (Biggs et al., 2019), a feeling of captivity in their role and/or the tension arising from concerns for the health and safety of their loved ones (Dreyfus et al., 2018). In the geographical area covered in this study, it is estimated about a third of missing persons reported to the police relate to persons living with dementia. 1 Aside from the cost to police, health and social services, family members suffer anxiety and distress while police search for the person, is being searched for, increasing the likelihood of residential care. This can have a huge cost implication (for example, in Barnsley, this costs nearly £37,000 per year at an average of £708.65 per week 2 ) and the associated emotional stress of the move to a nursing home (Hähnel et al., 2022; Johansson et al., 2014).
There is a need for an intervention that suits a domestic setting and enables access to a good support network, improves capabilities and enhances social wellbeing for people with dementia and people caring for them, supported by Assistive Technology (AT) (Alzheimers Society, 2023). Many AT interventions have been proposed for use with dementia to reduce falls risk, teleprompting, telepresence, coping and self-management (Brims & Oliver, 2019; Evans et al., 2021; Moyle et al., 2019; Pappadà et al., 2021; Øksnebjerg et al., 2020). GPS trackers may reduce emotional distress and risk of physical harm by assisting family members to find relatives much quicker, reducing the burden on themselves, the police, rescue services and health and social care services (Bartlett & Brannelly, 2019). Recent systematic reviews of the use of GPS systems in dementia care concluded that the application of GPS methodologies in dementia care show promise for increased safety to users, reduced burden for carers and increased activity and improved health for both, although the consensus remains that evidence of the beneficial effects of GPS remains insufficient (Ehn et al., 2021; Firouraghi et al., 2022; Megges et al., 2018; Rohne et al., 2017). Further research is required to evaluate the efficacy of GPS tracking on enhancing the independence and well-being of people with dementia and reducing the burden on carers. However, the feasibility of conducting a research trial of GPS tracking in dementia care is unclear and feasibility studies are required to explore feasibility to conduct a research trial and acceptability of GPS to support a more definitive study (Milne et al., 2014).
Therefore, this was a feasibility study in preparation for a larger, that evaluated the feasibility of a GPS intervention and methodology in terms of recruitment, adherence, attrition, assessments, safety and follow-up, We also evaluated the overall acceptability of a GPS tracking device for people with dementia at risk of wandering and their carers. 3 The main objective was to evaluate whether wearers and carers found the tracker usable and practical, while acceptable in terms of independence for the wearer and reduced burden for the carer. The study also considered whether the GPS trackers reduce the risk of harm, prolong independence at home, reduce the use of service response and delay the need for 24hr care. This study was conducted in Barnsley and Wakefield in Yorkshire, England.
Method
The study used a mixed-method approach combining qualitative interviews and focus groups with pre and post questionnaire data. Wearer-carer dyads, consisting of people with a diagnosis of dementia or significant cognitive impairment who had a history or were adjudged to be at risk from wandering, and their nominated carers. A range of questionnaires were conducted at baseline and then at six months follow-up. The research team contacted wearer-carer dyads monthly on the phone or at home during the six-month follow-up. This allowed monitoring of the device’s usability and ensures participants’ circumstances are documented consistently throughout the follow-up period. We conducted follow-up assessments at six months (or as soon as dyads exited the study for any reason) to understand the device’s actual use, acceptability and impact using exit questionnaires previously used successfully in a similar study by Liu et al. (2017). Four focus group meetings were conducted with a sample of wearer-carer dyads (n = 14) and stakeholders (n = 3).
Ethical issues
The study was approved by the Health Research Authority (IRAS 297216) and the host University Research Ethics and Integrity Committee. It was also registered with a clinical trial Web site (Doyle et al., 2022). The carers and wearers provided informed consent. Where the person with dementia lacked capacity and could not consent, their wishes were considered through liaison with their nearest legal relatives, weighing the benefits and proportionality of the intervention balanced against the risks. GPS tracking is, by nature, intrusive and in this study only the wearer and their relative had access to the tracking software.
Inclusion/exclusion criteria
The individual given the GPS tracker (wearer) was included in this study if he/she: (a) lived within Barnsley and Wakefield district, (b) deemed to be at risk of wandering by the carer or referrer and/or if a record of going missing on the police’s missing persons database (c) had cognitive impairment (e.g., dementia) confirmed through memory services, (d) lived alone, or with family members, (e) had a designated family member/close friend (as a carer) to supervise the use of the GPS tracking device. Participants who lived in a 24-hour care setting were excluded.
Interventions
Wearers were issued a GPS tracker, and their carers monitored them for six months. Carers received instructions on how to use the device and had the GPS app downloaded on their phones. The GPS tracker used had a proven track record as a lone worker device for healthcare staff. All costs for the tracker and mobile data were covered by the project and there was no external/third party monitoring using the tracker. The tracker was worn with a lanyard, on a keyring, or inserted in a handbag or pocket. The wearer can speak to their caregiver by pushing a button. A loudspeaker function allows the carer to contact the wearer directly. The trackers have a geofencing function, which allows carers to receive real-time location updates through an app and be alerted when the wearer leaves a predefined perimeter. Carers can monitor the real-time movement of the wearer on the map and access location history, allowing for alternative locations search in the event the wearer gets lost without the tracker. The trackers also send fall alerts to registered numbers and can inform carers when the battery needs charging. The trackers can register up to five mobile numbers and send alerts in turns until call is taken.
The research assistant contacted the dyads monthly and logged participants’ experiences. Once a dyad stopped using the tracker, a research assistant met them face-to-face to complete exit interviews. A multi-agency steering group sat monthly to review and address issues arising from the study.
Outcome measures
The primary outcome was the feasibility and acceptability of the intervention. This included uptake and use of the GPS for six months period, and considered adherence, attrition, viability of assessments and follow-up. Feasibility was also assessed on whether the person with dementia came to any harm through wandering whilst wearing the trackers and how quick it was to retrieve them when they get lost without needing to contact the police. Acceptability of the intervention was also assessed through focus group discussions using a topic guide (see later) Responses recorded in a use-log database were combined with focus group data at the end of the study for overall analysis.
Further outcome measures included quality of life for both the person with dementia and the carer. Quality of life for the person with dementia was evaluated through focus group feedback and extent to which they were able to continue living and socialising independently. Carer burden assessed by asking whether they felt anxious about their loved ones getting lost despite the tracker, though monthly contacts and focus group feedback. The following measures were completed at baseline, then at follow-up: (a) Zarit Burden Interview - a 22-item scale measuring how carers perceive their burden due to caring for a person with dementia (Stagg & Larner, 2015; Zarit et al., 1980). (b) Cornel-Brown’s Quality of Life Scale - a self-reported tool to measure a person’s perceived quality of life (Ready et al., 2002). (c) Revised Algase Wandering Scale - a 28-point questionnaire based on five dimensions of wandering designed to measure wandering behaviours in persons living with dementia (Algase et al., 2001). (d) The University of Alberta useability questionnaire - evaluated the degree to which participants believed the GPS was helpful, the degree of ease associated with using the trackers, their actual behaviour, and their future willingness to pay for it (Liu et al., 2017). Completed at six months or when a participant exited the study.
Data analysis
Demographic and diagnostic information was recorded at baseline and summarised. We reported participant flow in accordance with the CONSORT statement (Eldridge et al., 2016; Figure 1). We compared the mean of pre-post assessment using a paired-sample t-test (Table 4) and used descriptive statistics to summarise after-action review ranks based on the exit interview questionnaire. We used the median scores as a benchmark for accessing high and low scores in performance and ease-of-use experiences. For example, a median score of four for the carer and two for the wearer would indicate a positive impact and acceptance. CONSORT diagram to demonstrate participant flow.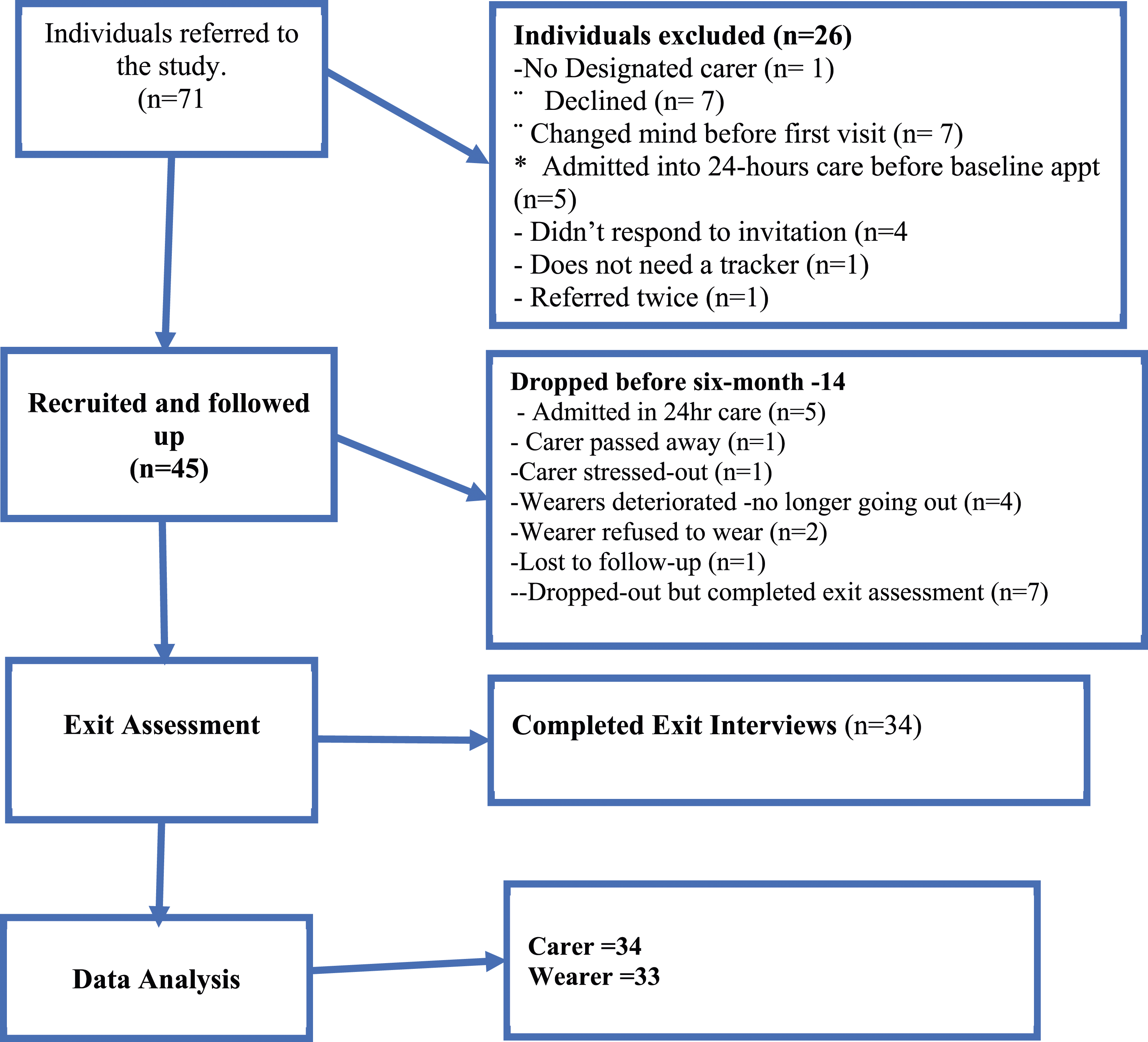
The use-log database and focus group data were analysed using a general inductive approach (Thomas, 2003) based on study objective and themes emerging from the study data. Use-log analysis was analysed separately and highlighted themes included in the focus group guide based on three main topics: (1) experience and outcome of using the GPS tracker, (2) experience and impact of the GPS tracker on the person with dementia and the carer, and (3) challenges and key improvements for the device. The focus group discussion was recorded and moderated by the Chief Investigator, The recordings were transcribed verbatim and coded by researcher. Themes from the dataset were reviewed by the research team for consistency and validity.
Results
Participants
Seventy-one (71) potentially eligible participants were referred from NHS and voluntary services. Forty-five dyads gave consent to participate in the study and were issued a GPS tracker. Of the 26 referred who did not participate 14 (19.8%) refused to participate and four (5.6%) did not respond to invitation. to participate. In total consent rate was 75%. Five were ineligible as taken into 24-hour care (Figure 1).
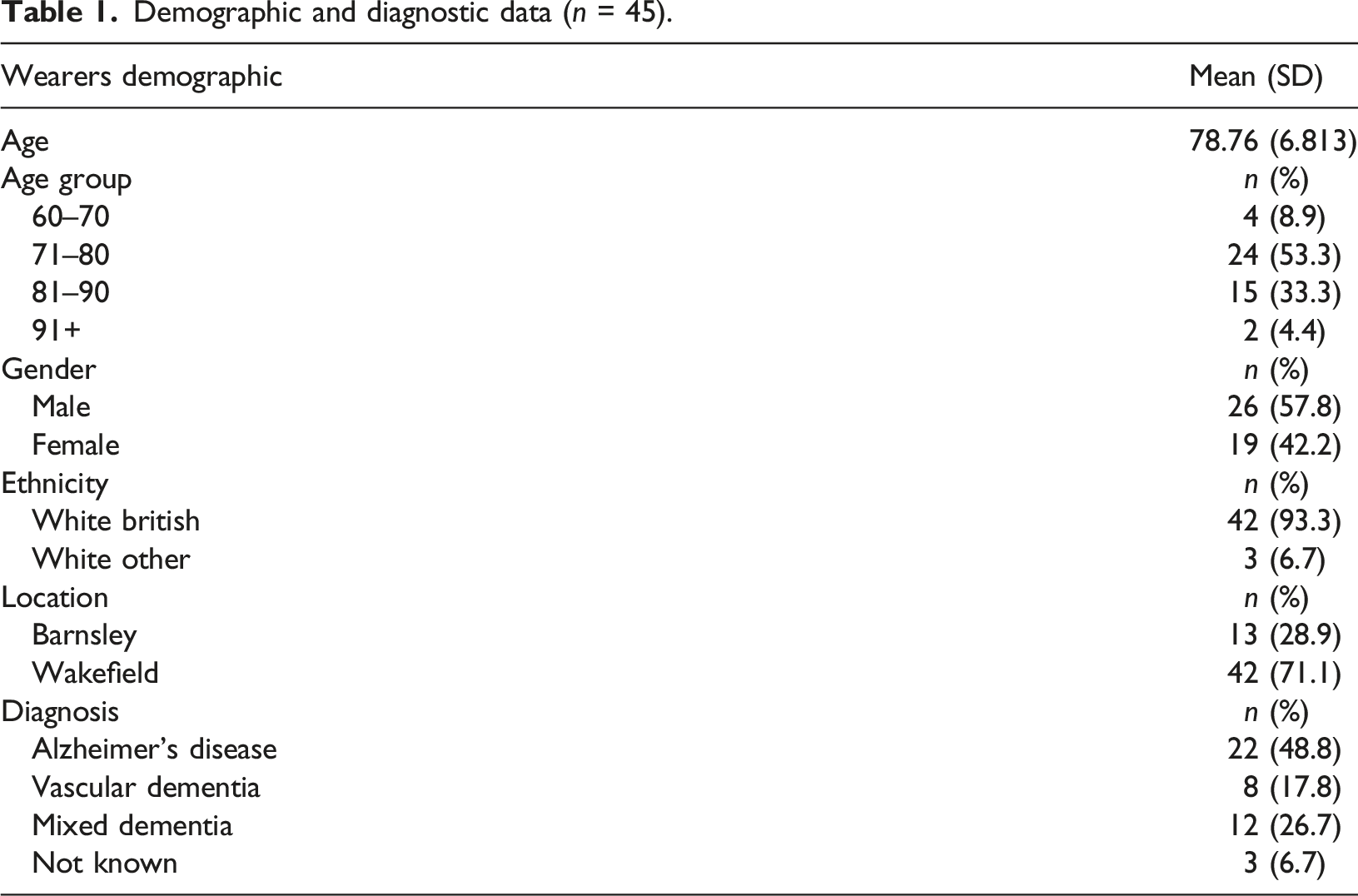
Demographic and diagnostic data
Demographic and diagnostic data (n = 45).
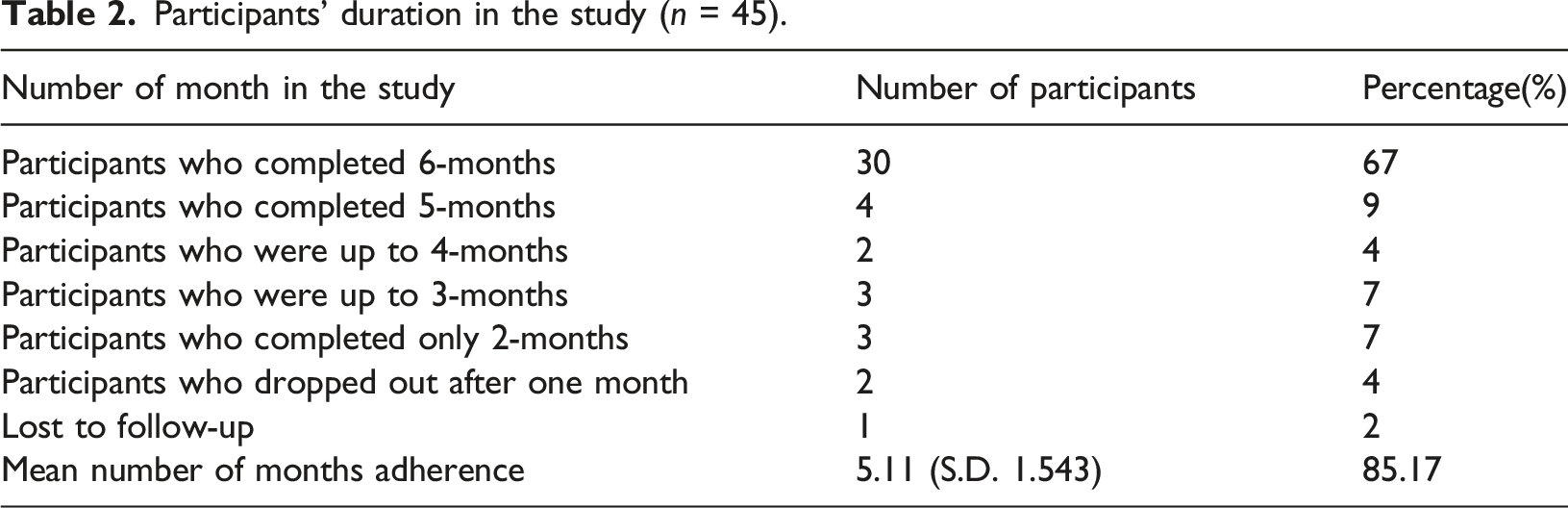
Participants’ duration in the study (n = 45).
The feasibility measures (use-log database)
Practical and usable
In all the 45 dyads that were followed up, only four (9%) carers reported the tracker was not practicable for their relatives because the person with dementia refused to wear them. Nearly all, 91% of the wearers either wore the tracker in a lanyard or on a key ring; others reported inserting it in the wearer’s handbag or pockets.
Four main circumstances for use were identified: 1) The person with dementia lives independently and is routinely being monitored by a carer through the GPS app (22%, n = 10)). Two incidents were logged where the tracker sent an alert to the carer when the person with dementia fell from bed and couldn’t get up. The carer travelled to the wearer’s residence to help. (2) The person with dementia lives with the carer and is allowed some independence within the neighbourhood while being monitored by the carer (44%, n = 20) (some individuals have the cognitive ability to operate the device while some don’t). (3) The person with dementia lives with the carer and only wears a tracker when being left alone in the house (13%, n = 6). The carer monitors the wearer’s activities in the house and uses the loudspeaker phone function to communicate. (4) the person with dementia lives with family and wears the GPS when travelling with the carer or family, so if missing in a busy environment, they could be easily located (18%, n = (8) (Table 2).
Evaluation of most used features of the GPS trackers by carer-wearer dyad and use circumstances (n = 44).
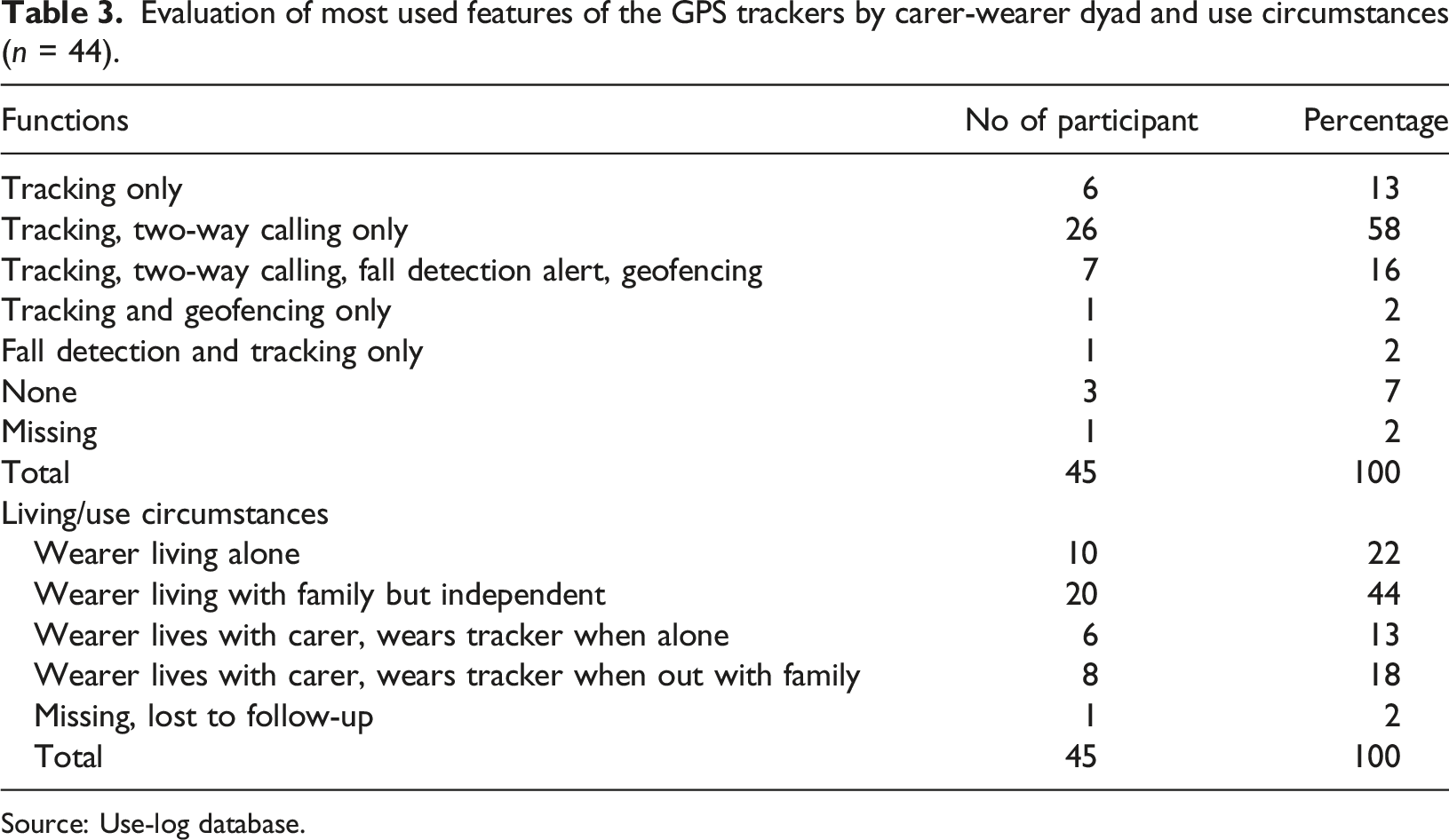
Source: Use-log database.
Quality of life, useability (exit interviews)
Pre and post measures of carer burden, RAWs and CB_QoL.
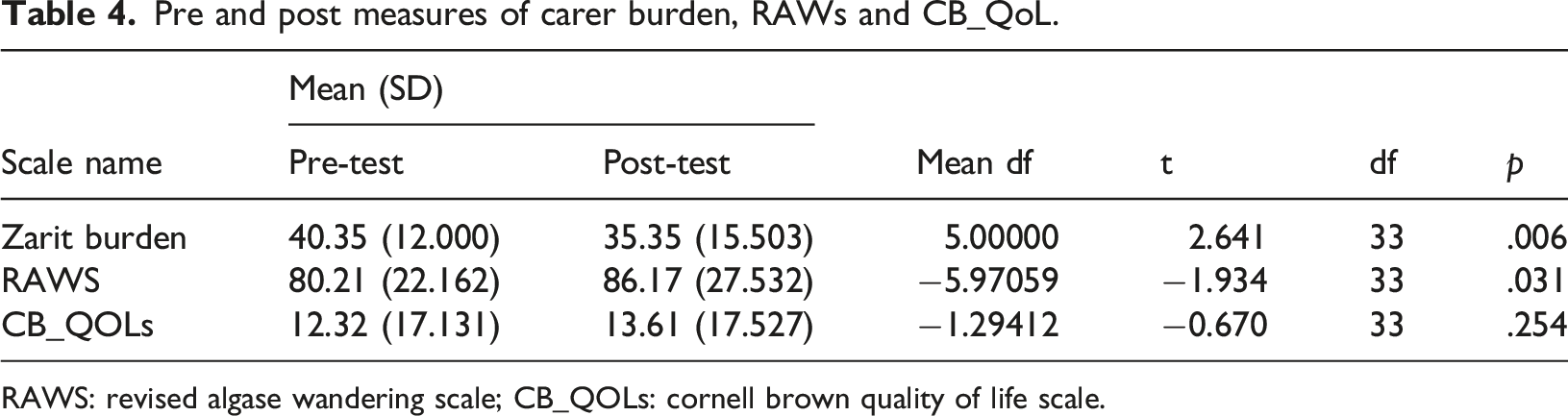
RAWS: revised algase wandering scale; CB_QOLs: cornell brown quality of life scale.
Evaluation of the performance and ease-of-use experiences of the GPS trackers by wearers (N = 33) and carers (N = 34).
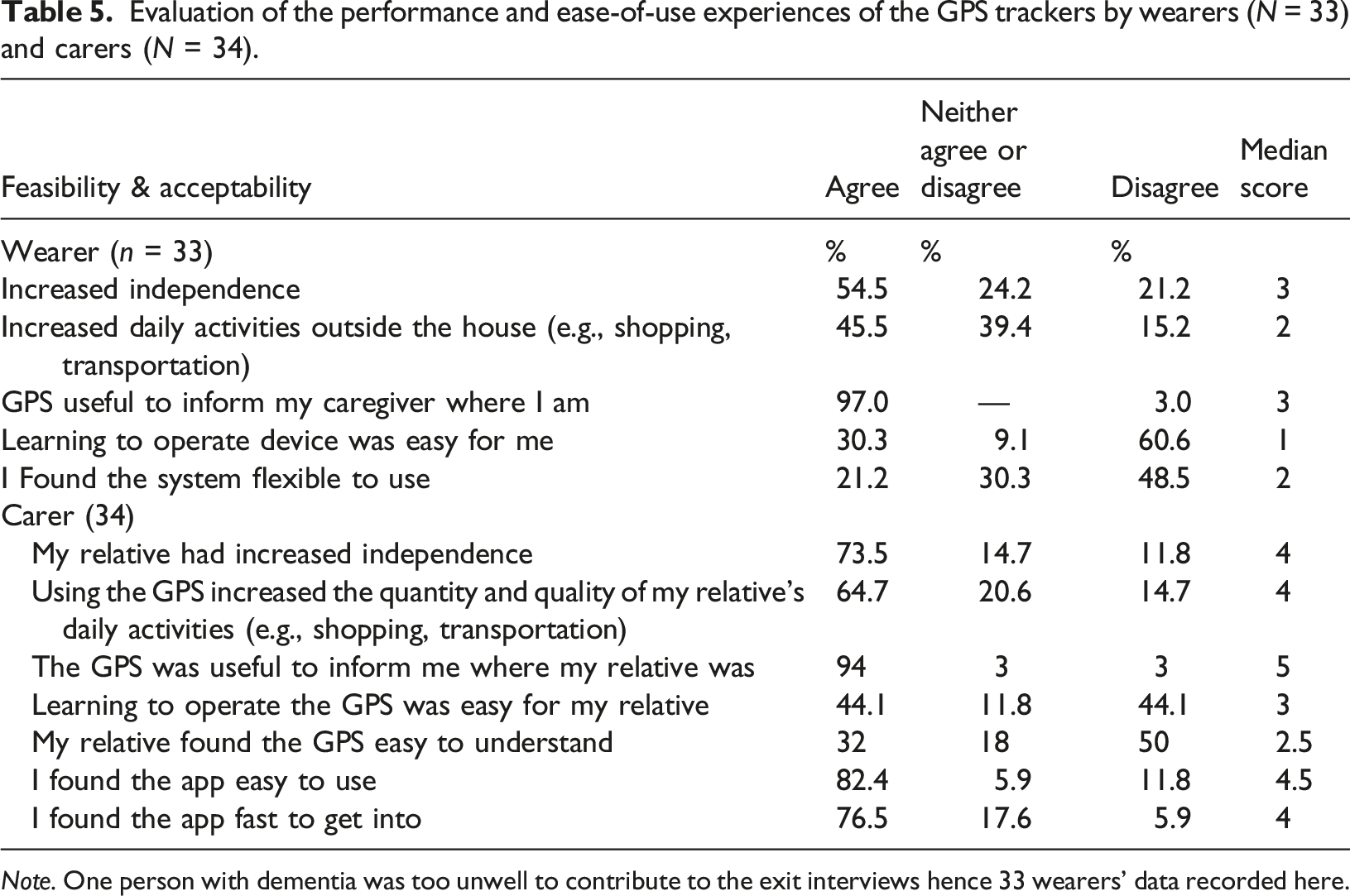
Note. One person with dementia was too unwell to contribute to the exit interviews hence 33 wearers’ data recorded here.
Table 5 shows, carers appear to find the tracker app easy to use (82.4%) or fast to get into (76.5%). However, learning to operate the device was not easy for the majority of people with dementia (60.6%). Carers reported they would continue to support the person with dementia to use the tracker if they are able to do so, and a majority (94.1%) were happy to use it at their own expense.
Focus Group Analysis
Four focus groups of 60 minutes were held virtually via Microsoft Teams in accordance with best practice guidance (Kreuger & Casey, 2014), with a range of three to four dyads in each group. A total of 14 wearer-carer dyads and three stakeholders attended the focus groups. Most carers were spouses and children of the wearer. Other stakeholders participating were representative of the police and NHS memory services. Figure 2 illustrates how theme number three (Device features) had an impact on theme one (Experience of carers) and theme two (Experience of the person with dementia). Thematic structure of focus group analysis.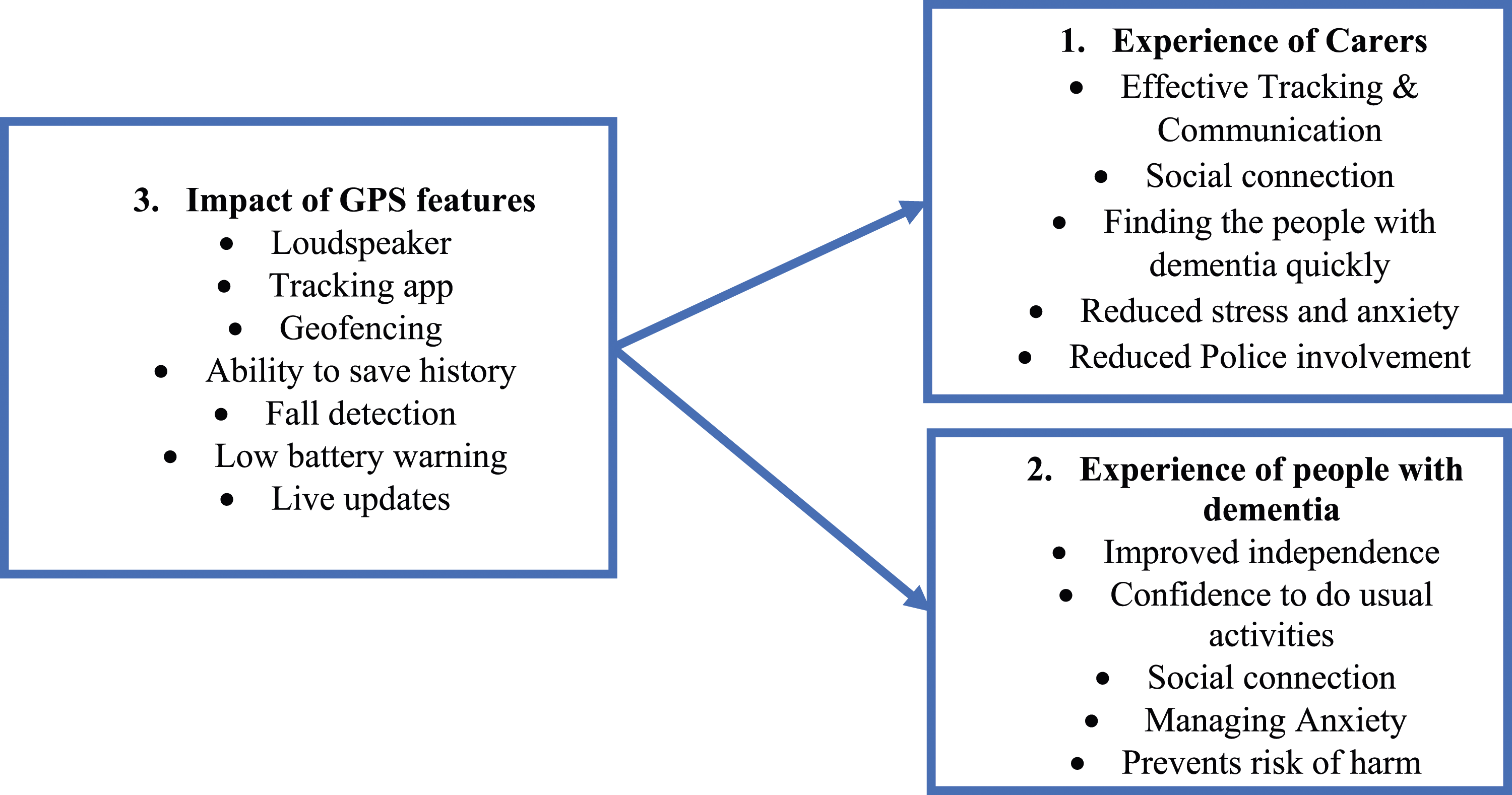
Case examples to support benefits identified from focus group discussions.
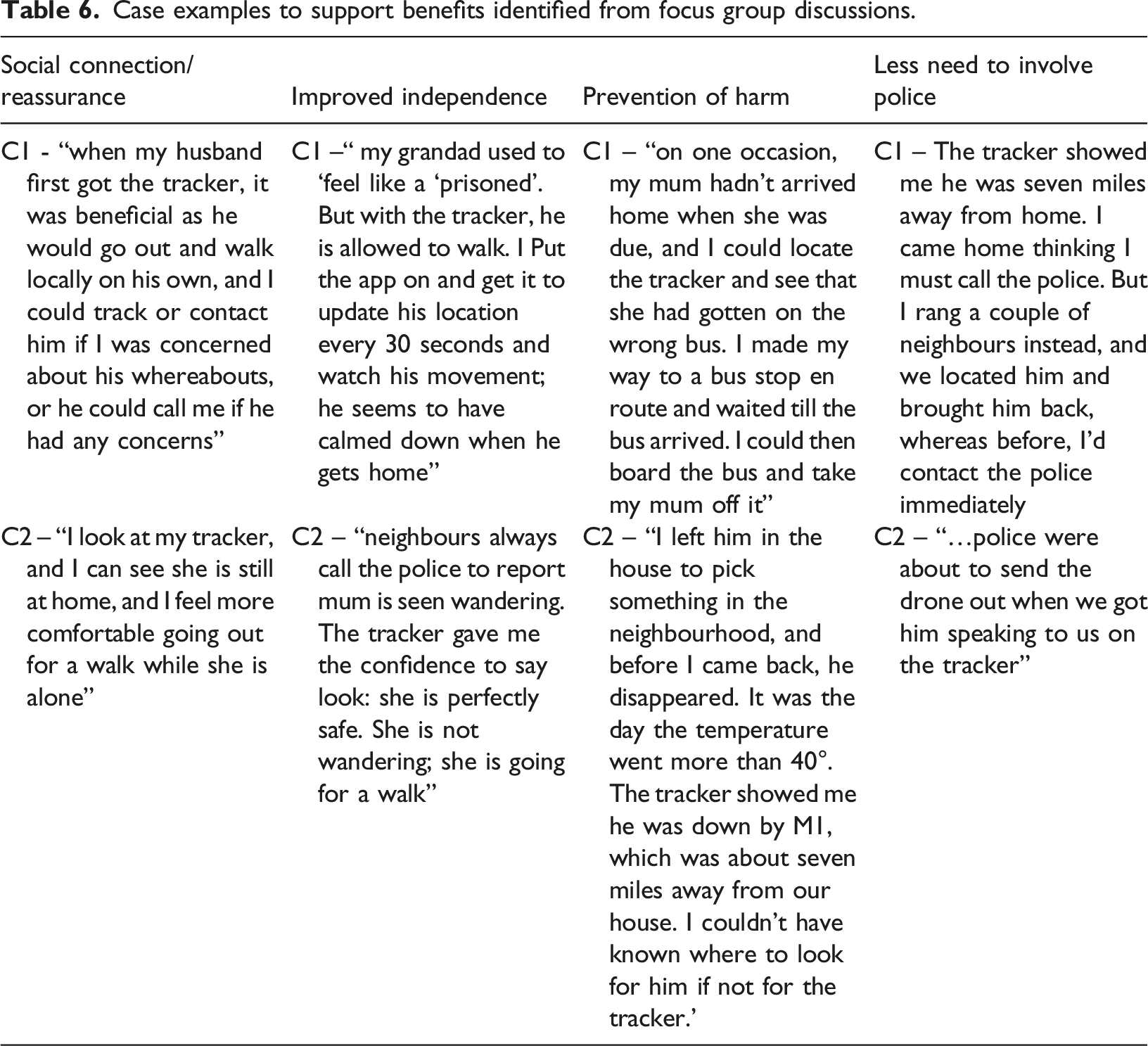
Participants described different experiences for the person with dementia. Some persons tend to put on the device by themselves with regular reminders. For others, ‘My wife keeps her handbag all the time, and I pop in the tracker in her handbag’ or ‘he seems very proud of it, so; fortunately, he just keeps it in his chest pocket all the time but would forever take it off if put round the neck’. Many carers indicated their loved ones initially rejected the device but eventually accepted using it routinely. Some people with dementia felt it was bulky to wear around the neck and used a key fob as a ‘safety blanket’ for reassurance instead. As Figure 2 depicts, the impact of the GPS features show they benefitted the person with dementia and their carers. Participants liked the ‘tracking function’, especially the ability to save a history of wearers’ movement, as they could use this history when searching if wearers went missing without the tracker. Others included ‘the loudspeaker function’, geofencing, fall detection and live update functions and low battery warning. Examples of benefits of the tracker summarised in Table 6.
However, there were some challenges and room for improvement. For example, the accuracy of location and absence of sound when it rings may prove finding the tracker difficult if misplaced. Other issues included supervisory commitment required. Some participants described what they did to locate the device when misplaced, including attaching ‘a tile – a tiny square tracker used for keys’– or ‘Chipolo’ to the GPS. One participant suggested fitting in ‘What3word app (a separate location mapping-search app) for better tracking accuracy.
The results show that the intervention was feasible and acceptable for wearers and carers. The refusal rate of 25%, attrition over six months of 33% and adherence to full duration of the study follow-up of 85% are satisfactory in terms of feasibility for future implementation studies and trials. The independence of the person with dementia was greatly enhanced, with the burden on carers much reduced as they felt more comfortable leaving wearers alone. Additionally, police involvement was significantly reduced, suggesting possible economic savings, and no untoward incidents. The intervention could delay admission of the person with dementia into more restrictive care. GPS trackers may be provided to people with dementia earlier in the course of their illness to build their confidence and improve their mobility behaviour in the long term.
Discussion
This findings suggest that GPS trackers can be implemented safely and practically for people living with dementia and their carers. The intervention could be delivered with minimal risk of harm, with satisfactory recruitment, consent, adherence and attrition rates, suggesting the methods employed in this study are feasible, safe, and acceptable for future roll-out in a larger implementation study or trial. Safety and psychological well-being were significant elements of carers’ acceptability of the device. Knowing you could be found when lost was one of the reassuring experiences of the person living with dementia in this study. This is consistent with previous studies that prioritised physical safety over privacy concerns, with the perception of safety as the biggest driver of uptake (Dreyfus et al., 2018; Gibson et al., 2015) and for wider benefits related to independence, safety, reduced burden and activity (Ehn et al., 2021; Firouraghi et al., 2022; Rohne et al., 2017). As with previous studies, some improvements in optimising the methodology and interventions would be useful (Megges et al., 2018), and further thought required on how to make it easier for wearers and carers to provide reliable feedback sooner and more frequently ahead of future research (Milne et al., 2014), and issuing earlier before person starts to get lost. Unlike previous studies, which suggested that GPS technology is only feasible for people in the early stages of dementia (Pot et al., 2012), our study shows that people at more advanced stages of dementia can benefit from the trackers, either living independently or with family members. Carers had different perspectives on independence for the people with dementia. This included physical and emotional independence, which accounts for those who are mobile and those who can no longer wander, while others could still engage in activities of daily living and socialise in the neighbourhood. The emotional independence is described as the feeling of reassurance, a sense of safety and social connectedness for dyads, increasing their social wellbeing. Carers reported concerns about neighbours who were unaware of the benefits of the GPS tracker and in one case a neighbour called the police when they saw the wearer out alone. This suggests the need for greater public awareness of the potential benefits and resonates with Spilker et al. (2019) who suggest a ‘techno-organisational network’ where the implementation of GPS technology involves human and non-human actors. The safety and well-being of the person with dementia is a function of the supervisory commitment of different actors. This means that GPS itself cannot produce the desired result alone without a carefully designed delegation of supervisory roles and responsibilities and ‘a fine-tuned interplay between the technical and organisational elements’ (p.294) involving different sets of carers, healthcare staff, community members, network providers, and especially the police tasked with searching for missing persons. This is consistent with previous studies emphasising the potential impact and benefits for the wider community and stakeholders (Firouraghi et al., 2022; Rohne et al., 2017) and GPS tracker implementation must consider the role of significant others (Ehn et al., 2021; Liu et al., 2017; Milne et al., 2014), particularly as carers’ social norms and the ability to overcome psychological barriers could influence GPS uptake and evaluation.
Optimising the care of the people with dementia within their homes is not only a public health imperative (Samus et al., 2018) but also preferred by people with dementia (Scocco et al., 2006); it costs less and guarantees greater quality of life (Olsen et al., 2016). Our study suggests family members also relied on neighbours and wider social network in addition to the GPS trackers to find the person with dementia when lost, while there was a reduction in the police interventions. The impact of the trackers varied according to carers’ perceived ability of the wearer to interact with it. As the cognition of the wearer begins to wane such that he/she cannot operate the tracker, some carers stopped the wearer from going out alone. People in their early diagnosis may benefit more than those who have progressed with the disease, initially as a proactive safeguard should the person start getting lost. Any intervention that alleviates carers’ burden when managing wandering behaviour is desired. Consistent with this, the study demonstrated that tracking and communicating with the person with dementia offered carers peace of mind. Carers showed confidence in dealing with loved ones getting lost without needing to contact the police despite the severity of the incidents. Such confidence and social connection indicate that people with dementia could remain in the community for longer. Although we did not measure the health economics of using the device specifically, the outcome of this study suggests the technology may mitigate the cost of finding a person with dementia when lost and reducing the need for 24-hour care.
Overall, both the exit questionnaire, the use-log analysis, and the focus group results confirm the GPS technology’s impact and show that participants have used the device for its intended purpose effectively, efficiently, and with a feeling of satisfaction (Lewis, 2014).
Limitations and study implications
The study had some limitations. Aside from the relatively small sample size, most people with dementia in this study have progressed in their dementia illness, making the reliability of responses variable (Milne, et al., 2014). Our results suggest that cognitive ability had an impact on the degree of independence of the wearer and the confidence of the carer to continue use of the device. We did not measure the severity of the dementia on the wearer at baseline or follow-up, but future studies will need to do so to determine the relative impact at different stages of dementia. Wearers were generally unable to complete quality of life questionnaires, and a similar study has recommended carers as a proxy for the responses of dementia clients in GPS studies (Liu et al., 2018). There was no control group in this study making it difficult to draw any firm conclusions about the effectiveness of trackers, but the feedback was overwhelmingly positive. A larger randomised trial or implementation study with a matched control group would be useful. Most dyads in this study are of white ethnic backgrounds, which may limit generalisability. Future studies should recruit a culturally diverse population. Future studies should aim to recruit people with early-stage dementia and evaluate the health economics of GPS technology in dementia care in relation to reducing costs of rescue, admission into health and social care settings and quality of life.
Conclusion
The GPS trackers used in this study were acceptable, safe, and feasible for the dyads and in terms of feasibility for future research when implemented with clear guidance and support from the research team. Wearers and carers had a greater sense of safety, were better connected should help be required, and participants were willing to continue using the trackers at their own expense. The confidence, ‘peace of mind', and the ability to locate the person with dementia quickly and safely with less need to involve the police support the conclusion that the technology can potentially delay admission into a 24-hours care setting. Based on the findings in terms of recruitment, retention, adherence, safety and acceptability, future larger trials of GPS trackers should be feasible, although need to consider mixed methods for data collection. The study also highlighted possible challenges and limitations of the technology, including carer supervisory commitments, rapid deterioration of the wearer, location accuracy and ability to keep up with technical procedures. Future studies should prioritise regular technical support and, provide an easy reference guide for carers. There is also a need to simplify data collection instruments for a better participant experience and improved reliability of data in future research studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the West Yorkshire ICB Research Capability Funding (RCF-2021-004), West Yorkshire Integrated Care Board and the University of Huddersfield.