
Abstract
Background
Dementia disproportionately affects women including persons living with dementia and caregivers. Person-centered care, rather than disease-focused, is recommended to improve care for affected persons including caregivers. General practitioners play a central role in dementia care but find it challenging due to inadequate training. The study aimed to assess if and how dementia guidelines provide clinicians with guidance on person-centred care for women affected by dementia.
Methods
We searched for publicly available English-language guidelines on the overall management of dementia in MEDLINE, EMBASE and the Guidelines International Network repository. We employed deductive and summative content analysis, and categorized person-centered care guideline content based on established frameworks, and conveyed our results using summary statistics, text, and tables.
Results
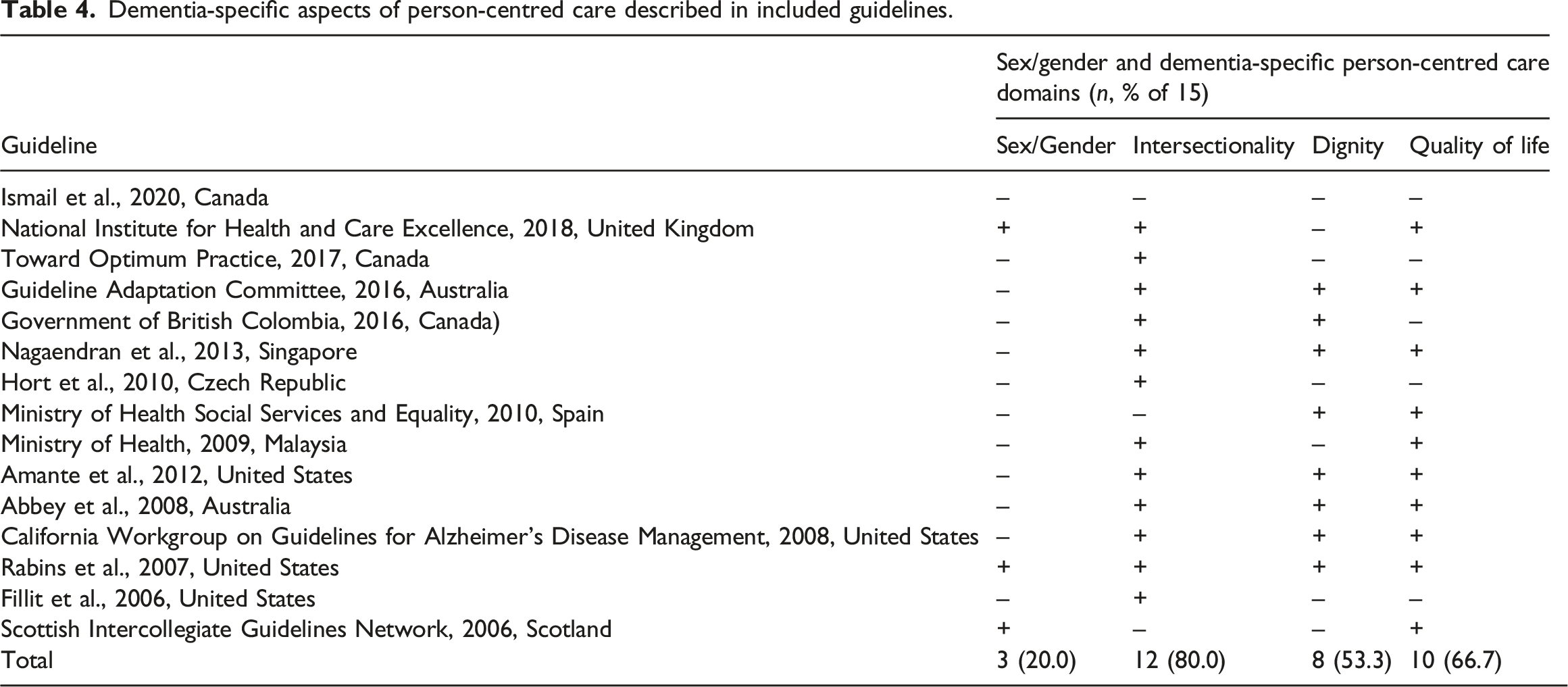
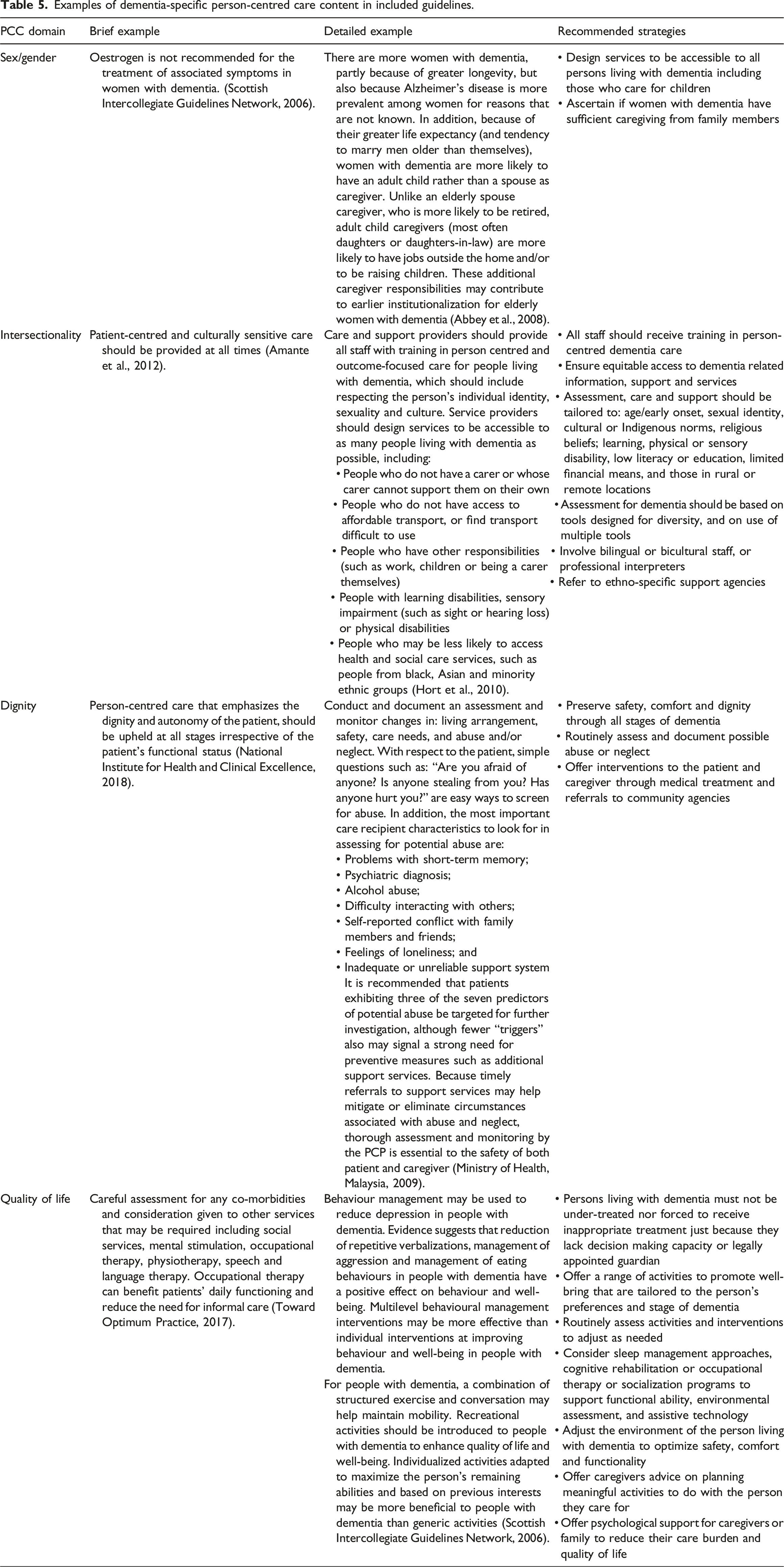
We reviewed 15 guidelines published from 2006 to 2020 in eight countries. Few (4, 23%) involved persons living with dementia or caregivers in guideline development. Regarding general person-centred care, guidelines mostly addressed the domains of exchange information (93%), share decisions (93%), enable self-management (93%) and address emotions (87%), while few offered content on manage uncertainty (33%) or foster a healing relationship (13%). Regarding dementia-specific person-centred care, most guidelines addressed intersectionality (tailoring care for diverse characteristics) (80%), but few included content on the domains of quality of life (67%), dignity (53%) or sex/gender issues (20%). Even when mentioned, the guidance was typically brief. We identified 32 general and 18 dementia-specific strategies to achieve person-centered care by compiling information from these guidelines.
Conclusions
This study identified inconsistent and insufficient guideline content on person-centred care for women with dementia. Compiled strategies for achieving person-centred care could be used by developers to enhance existing and future dementia guidelines; and inform the development of policies or programs, education, tools for clinicians, and quality improvement measures for evaluating dementia care. Future research is crucial for promoting person-centred dementia care for women living with dementia.
Background
Dementia is an increasingly prevalent condition characterized by gradual cognitive decline that impedes daily functioning (Canadian Academy of Health Sciences [CAHS], 2019; Gerlach & Kales, 2018; Tisher & Salardini, 2019). Its impact on physical, cognitive and mental health is often devastating for both persons living with dementia and their caregivers. Dementia is the second largest cause of disability for older persons and the seventh leading cause of death, and by 2030, it is estimated that 78 million people will have dementia (Prince et al., 2015).
Dementia disproportionately affects women. In 2021, 65% of total deaths due to dementia were in women (Prince et al., 2015), and based on 2019 data, the greater female:male ratio pattern was expected to continue to 2050 (Global Burden of Disease 2019 Dementia Forecasting Collaboration, 2022). Women face inequitable access to dementia care and support, often due to factors such as younger age of onset, delayed diagnosis of dementia, and socioeconomic status (Sourial et al., 2020). In a sample of 318,350 community-dwelling adults aged 65 and older, women had a higher occurrence of emergency department visits, lower continuity of care and longer discharge delays (Sourial et al., 2020). Furthermore, as most persons living with dementia reside at home, caregiving largely falls upon women, with wives more likely to support husbands than vice-versa, and daughters more likely to care for parents compared to sons (Bott et al., 2016), impacting caregiving women’s employment, health and well-being.
Despite the disproportionate and inequitable impact on women (i.e., persons who identify as women), limited public health or health system guidance is available on how to support women affected by dementia, who include persons living with dementia and women who are their caregivers (Bartlett et al., 2018). For example, analysis of national dementia strategies in 29 countries found they did not address sex or gender issues, thus offering no insight to leaders for health system planning (Chow et al., 2018). A scoping review on what constitutes high-quality dementia care in home, community or outpatient settings identified only 22 studies published from 2001 to 2019 (Marulappa et al., 2022). Most studies involved clinicians, either exploring barriers of dementia care (e.g., knowledge or attitudes about dementia, perceived lack of control or time) or evaluating the impact of educational strategies to improve clinician knowledge about dementia care (Marulappa et al., 2022). Three studies evaluated interventions targeted at persons living with dementia or caregivers, but did not report findings by sex or gender, thus offering no evidence to inform public health or health system policies on how to tailor and support dementia care for affected women (Marulappa et al., 2022).
Research shows that the needs of the growing number of persons living with dementia and their caregivers are not being met (Clarkson et al., 2018; Hinton et al., 2007; Morrisby et al., 2018; Yaffe et al., 2008). General practitioners, who play a central role in diagnosing and caring for those affected by dementia, report they lack training in dementia care, find it to be complex and challenging, and note a lack of dementia care guidance and support for primary care providers (Bourque & Foley, 2020; Koch et al., 2010; Mansfield et al., 2019). Furthermore, physicians lack training and knowledge in women’s health, which extends beyond reproductive health to conditions across the lifespan; and in person-centred care (Anderson & Gagliardi, 2021a, 2021b), which involves patients, family and clinicians working together in tailoring care to individual health needs, life circumstances and personal preferences (Epstein & Street, 2011; Institute of Medicine (US) Committee on Quality of Health Care in America., 2001). Person-centred care optimizes patient care experiences and clinical outcomes (Doyle et al., 2013; Rathert et al., 2013). It long been advocated in the context of dementia rather than disease-centred care (Fazio et al., 2018; Kim & Park, 2017), and stands to reduce gendered inequities in access to and quality of dementia care because it focuses on personalizing care (Erol et al., 2015).
Clinicians often refer to clinical practice guidelines, which are decision-making tools that inform the approaches and treatments to offer when caring for individuals with specific conditions. Guidelines consolidate and synthesize scientific evidence, and offer recommendations for care delivery that can enhance patient-important and clinical outcomes (Shekelle et al., 2012). While dementia guidelines have been appraised for methodological quality of their development and for consistency in clinical recommendations across guidelines (Azermai et al., 2012; Ngo & Holroyd-Leduc, 2015), no prior research has assessed whether or how dementia guidelines support person-centred care, particularly for women affected by dementia.
Given little guidance in policy or research on how to optimize care and support for women affected by dementia (Bartlett et al., 2018; Chow et al., 2018; Marulappa et al., 2022), and the potential role of guidelines in doing so (Shekelle et al., 2012), the purpose of this study was to assess if and how dementia guidelines address person-centred care for women affected by dementia. The specific objective was to assess dementia guidelines for content on the care and support of women with diverse characteristics who have dementia or are caring for persons living with dementia. Exemplar content could be widely emulated by developers of dementia guidelines, and those guidelines could inform public and health system dementia policies and programs. Identifying gaps in content could help guidelines developers strengthen the relevance of dementia guidelines so that they better support clinicians in achieving equitable, person-centred dementia care.
Methods
Approach
We used content analysis to assess the content of international dementia guidelines (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005). This approach employs both deductive and summative content analysis procedures to first organize and describe content in categories (deductive), and then count and compare categories across documents (summative). In the absence of reporting criteria specific to content analyses, to enhance rigor, we complied with the Standards for Reporting Qualitative Research (O’Brien et al., 2014). We did not obtain ethical approval because the study did not involve human participants from whom we needed to obtain informed consent.
Eligibility criteria
We included English-language guidelines on the overall management of dementia, referring to two or more of screening, diagnosis, any form of therapy or supportive care for Alzheimer’s disease or other major forms of dementia (e.g., Parkinson’s, Lewy Body disease, frontotemporal disease). We chose to include guidelines that addressed overall management so that the sample would include guidelines with uniform characteristics, given the many guidelines related to dementia on a wide array of specialized topics. We included guidelines published from 2000 onwards to capture guidelines the reflected up-to-date underlying clinical evidence, and because it coincided with publication of a landmark report that recognized person-centred care, after which time guideline developers may have been aware of this concept (Institute of Medicine (US) Committee on Quality of Health Care in America, 2001). Guidelines referred to publicly-available new, updated or adapted/adopted documents developed using standardized methods including a systematic review of evidence, assessment of the benefits and harms of alternative care options, and synthesis of evidence into one or more recommendations. Eligible guidelines were developed in any country by non-profit organizations such as professional societies, academic institutions, government agencies, disease-specific foundations, or quality improvement/monitoring agencies. Guidelines were not eligible if they did not employ systematic methods to formulate evidence-based recommendations (e.g., consensus statements), or if they focused only on prevention or end-of-life care for dementia, or on topics relevant to ageing but without a focus on dementia.
Searching and screening
We searched for guidelines in MEDLINE and EMBASE, the largest indexed databases of published medical research most likely to include dementia guidelines, using [(dementia or Alzheimer disease) AND (practice guidelines as topic or guidelines as topic) OR (publication type: guideline or practice guideline)] in December 2021 and updated the search in December 2022. We also searched a comprehensive repository of international guidelines maintained by the Guidelines International Network with the keyword dementia. Searches were conducted and compiled by NG, AB (both trainees) and NNA (Master-trained Research Associate). To pilot test screening, NG, AB, NNA and ARG (PhD-trained investigator) independently screened the first 50 titles/abstracts against eligibility criteria, then met to discuss and resolve discrepancies. This was repeated twice until selection of potentially eligible items was congruent. NG and AB retrieved full-text guidelines and assessed their eligibility concurrent with data extraction, and NNA and ARG independently resolved uncertainties.
Data extraction
We extracted data on guideline characteristics and content related to person-centred care. Guideline characteristics included year of publication, developer organization, type of developer (professional society, government, academic group, charity), country, development methods (if persons living with dementia/caregivers involved in development), dementia cause (Alzheimer’s only or other causes) and dementia stage (mild, moderate, advanced). For general aspects of person-centred care, data included content relevant to a framework generated by McCormack et al. (2011). We chose this framework to guide data extraction because it was rigorously-developed based on a literature review, observation of clinical encounters, and input from patients and healthcare professionals (Scholl et al., 2014). With 31 elements across six domains, it is more comprehensive than other person-centred care frameworks (Scholl et al., 2014). While originally developed in the cancer context, its relevance to women with a range of clinical conditions was validated in other research (Filler et al., 2020; Gagliardi et al., 2020; Nyhof et al., 2020). The six domains include foster a healing relationship, exchange information, address emotions and concerns, manage uncertainties, share decisions and enable self-management. For dementia-specific aspects of person-centred care, there is no established framework or universal agreement. However, we derived key themes from a synthesis of published research that described person-centred dementia care: focus on dignity, referring to value and respect for self-hood or person-hood; and quality of life, referring to self-determination, purposeful living and a positive social environment (Fazio et al., 2018). In addition to general and dementia-specific aspects of person-centred care, we also extracted data on mention of sex, gender or intersectional factors (e.g., age, ethnicity, culture, education, employment, marital/partnership status, ability, sexual orientation, urbanity/rurality), which clinicians must consider when tailoring dementia care to individuals. To pilot test data extraction, NG, AB, NNA and ARG independently extracted data from two guidelines, where text as it appeared in the guideline was copied and pasted into a table organized according to general and dementia-specific aspects of person-centred care. They met to discuss and resolve discrepancies. This process was repeated once more, at which time data extraction was congruent. Thereafter, NG and AB extracted data from remaining guidelines. All data were reviewed independently by NNA and ARG.
Data analysis
We used summary statistics to report guideline characteristics, and the number of guidelines that addressed general and dementia-specific person-centred care domains. We used tables and text to highlight the degree to which guidelines addressed these domains. We synthesized strategies recommended across guidelines for achieving both general and dementia-specific person-centred care.
Results
Search results
The search yielded 623 results, of which 605 were unique. After title and abstract screening, we excluded 568 items and 37 remained. After full text screening, we excluded 22 items due to clinical topic (n = 16), methodology (n = 4) and publication type (n = 2). Overall, we included 15 guidelines in this study (Figure 1). PRISMA diagram. Flow chart of search results and guidelines included.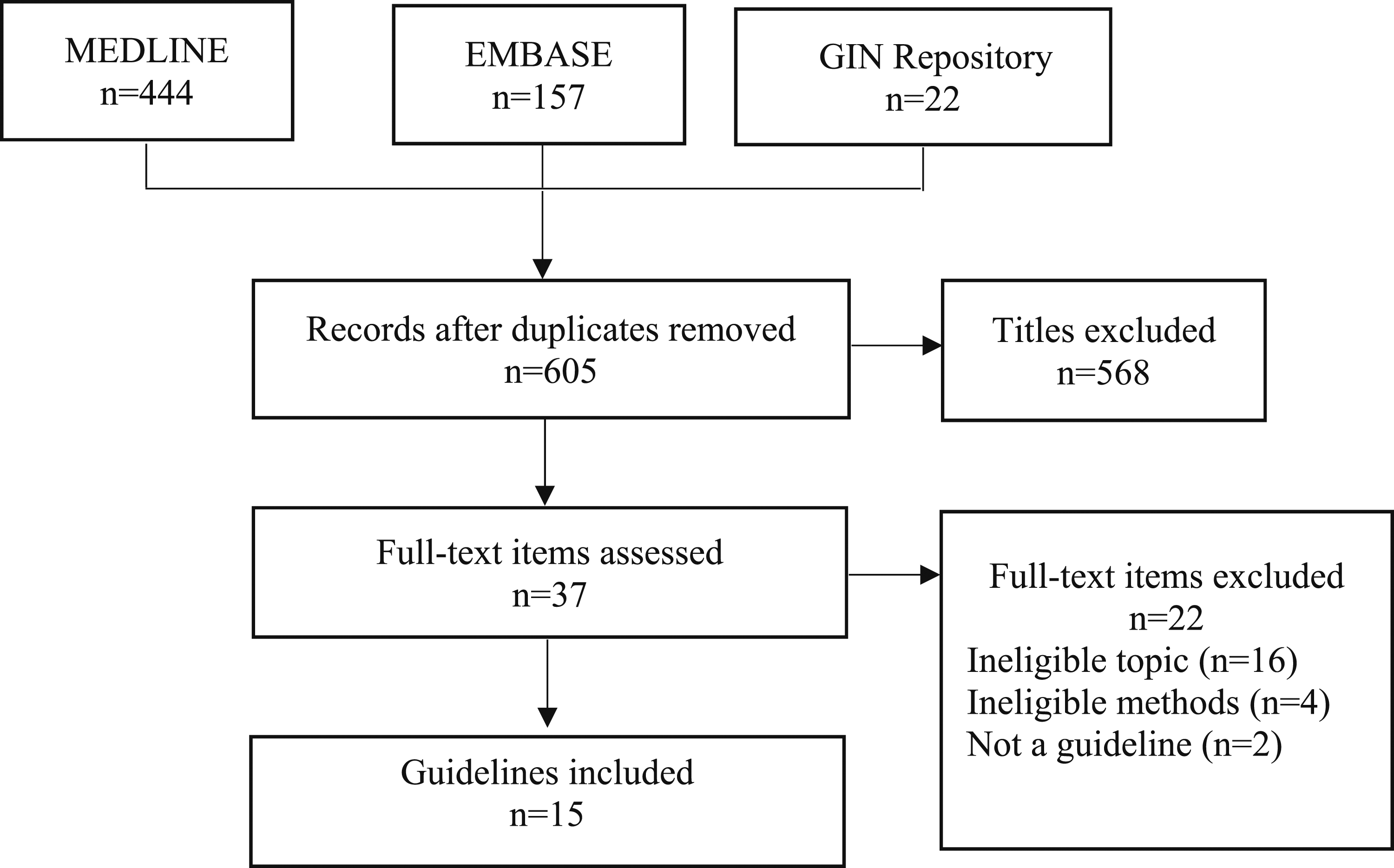
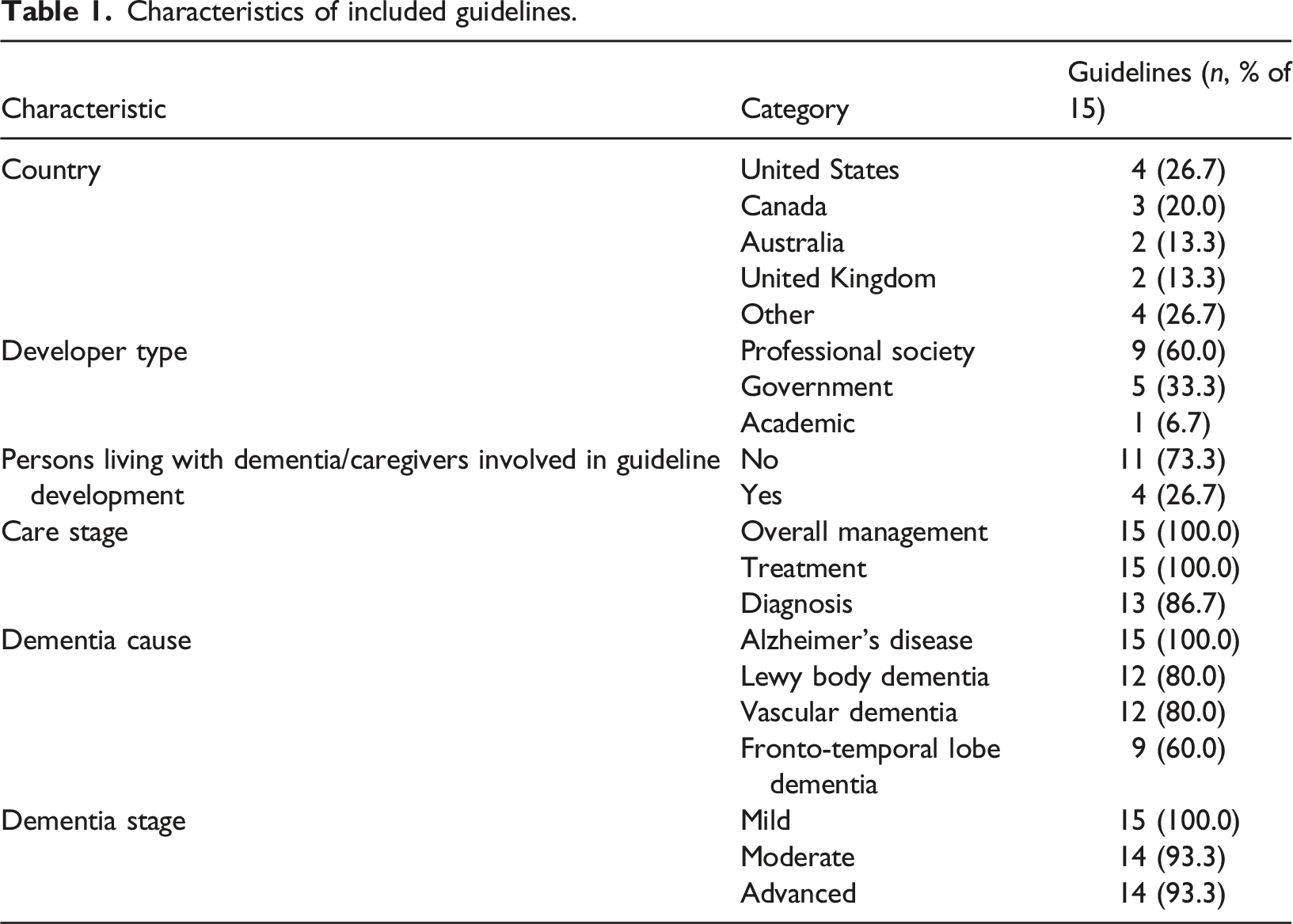
Guideline characteristics
Characteristics of included guidelines.
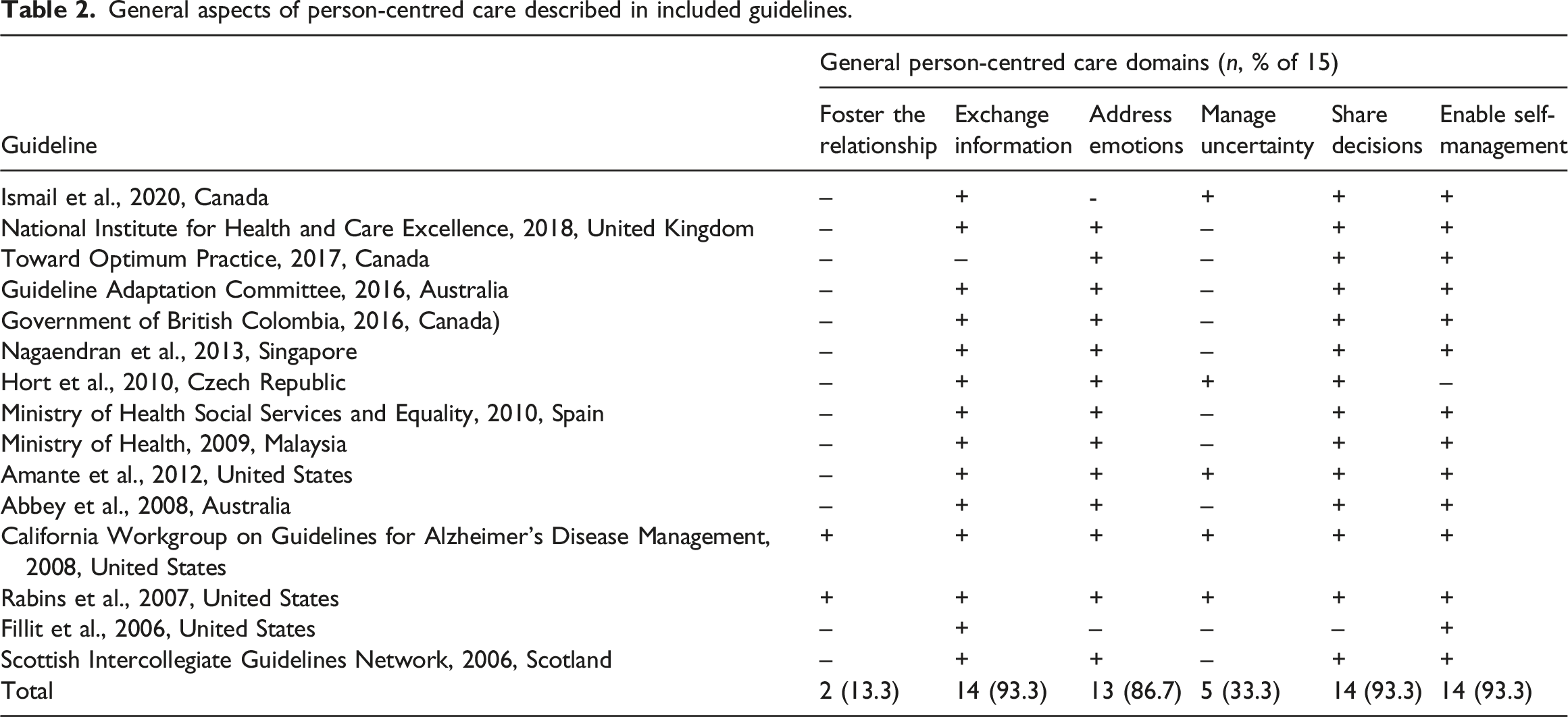
General aspects of person-centred care
General aspects of person-centred care described in included guidelines.
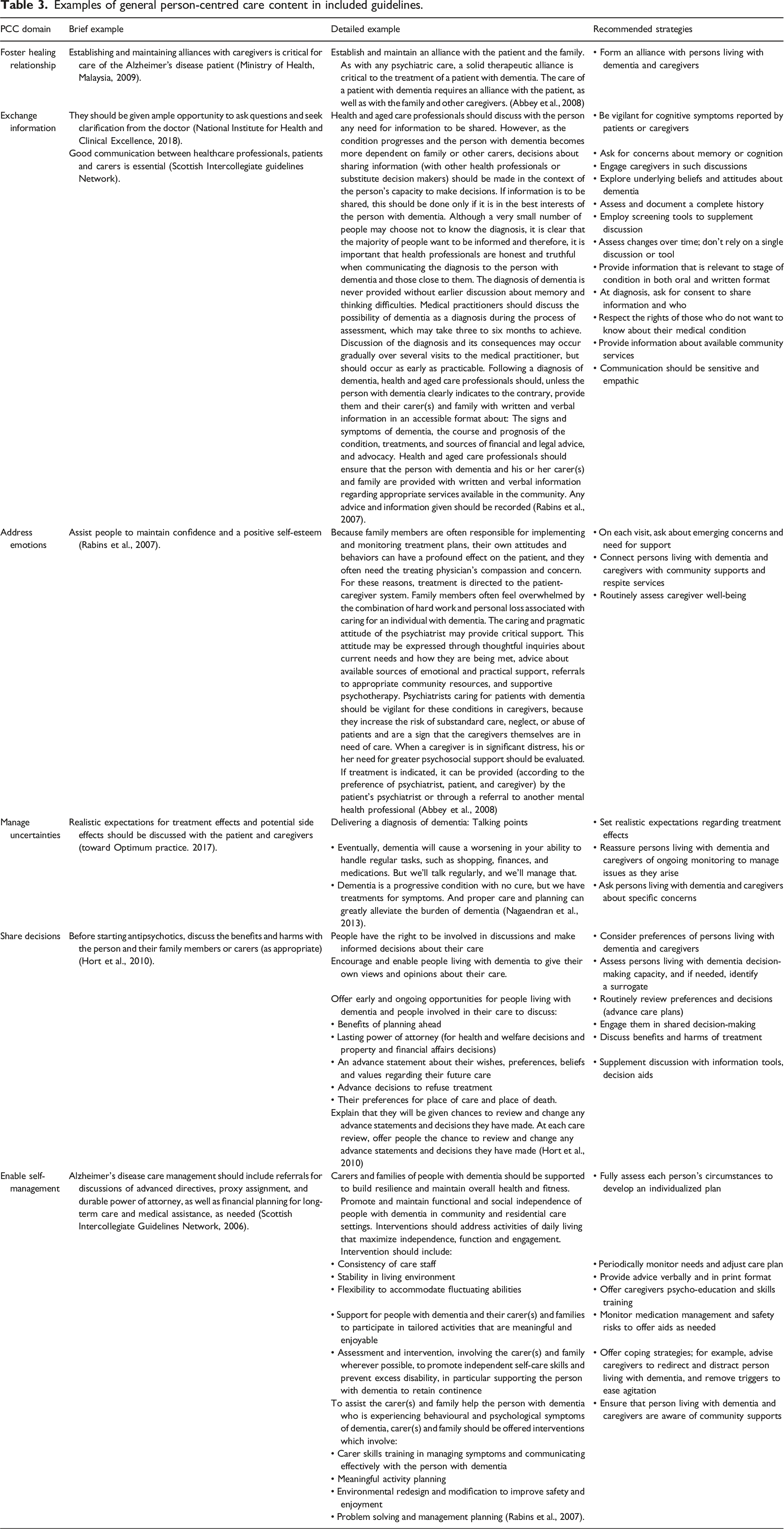
Examples of general person-centred care content in included guidelines.
Dementia-specific aspects of person-centred care
Dementia-specific aspects of person-centred care described in included guidelines.
Examples of dementia-specific person-centred care content in included guidelines.
Discussion
Analysis of the content of 15 guidelines on the overall management of dementia published in 8 countries from 2006 to 2020 revealed inconsistent and limited content across guidelines on person-centred care and support for persons living with dementia or caregivers who are women. With respect to general person-centred care, guidelines most commonly addressed the domains of exchange information, share decisions, enable self-management and address emotions, while few offered content on the domains of manage uncertainty or foster a healing relationship. Regarding dementia-specific person-centred care, most guidelines addressed intersectionality by recognizing the need to accommodate the needs of person living with dementia and caregivers with diverse characteristics and circumstances, but few included content on the domains of quality of life, dignity or sex/gender issues. Even when these general and dementia-specific domains were mentioned, guidance was often brief. Hence, most guidelines included in this analysis offer limited guidance and support to clinicians involved in caring for women affected by dementia.
The findings of this analysis reinforce prior research that revealed little guidance in dementia policies or published research on how to optimize person-centred dementia care for persons living with dementia and caregivers who are women (Bartlett et al., 2018; Chow et al., 2018; Marulappa et al., 2022). This research highlighted a similar paucity of such guidance in dementia guidelines, which are fundamental knowledge resources referred to by clinicians (Shekelle et al., 2012). This study also builds on considerable research that explored barriers of high-quality dementia care. For example, a scoping review of 88 studies published from 1998 to 2015 on implementing evidence-informed dementia care identified numerous barriers that were largely at the organizational (e.g., time constraints, workload, leadership) and clinician (e.g., lack of knowledge and training, resistance to change) levels, and found that education of professionals was the most common strategy employed to improve dementia care (Lourida et al., 2017). Interviews with 129 healthcare managers, clinicians and service staff, and 17 person living with dementia and 31 caregivers also identified barriers of post-diagnostic support for persons living with dementia including lack of clinician time and knowledge, inconsistent follow-up, lack of a holistic approach to care and limited planning for future needs; and recommended support to enable non-specialists to deliver dementia care (Wheatley et al., 2021). The same study generated 20 desired clinician behaviours to improve timely identification and management of needs, understanding of how to manage dementia, provision of support for emotional and psychological wellbeing of persons living with dementia and caregivers, and the integration of other support services (Bamford et al., 2021). Our work is novel because it explored how guidelines do and could overcome the many barriers of high-quality dementia care by providing clinicians with knowledge and strategies for addressing the needs of person living with dementia and caregivers. Unlike prior research that focused on critically appraising the methodological quality of dementia guidelines (Elo & Kyngäs, 2008; Ngo & Holroyd-Leduc, 2015), our analysis specifically examined dementia guidelines for content that would help clinicians deliver person-centred dementia care tailored for persons living with dementia and caregivers who are women. In so doing, it supplements the aforementioned qualitative research (Bamford et al., 2021; Wheatley et al., 2021) by revealing strategies that clinicians can apply to achieve holistic, person-centred dementia care. Our work also expands upon a prior analysis of dementia guidelines that specifically focused on intersectional factors, and like our study, found that most guidelines recognized the need to tailor dementia care to the needs of diverse persons (James et al., 2022).
Several key implications emerge from this study for future policy, practice and research. While no single guideline offered comprehensive guidance to clinicians on how to optimize dementia care, compiling content across guidelines generated considerable guidance (32 general and 18 dementia-specific strategies) to optimize person-centred care. The identified gaps help to improve guidance on dementia care for women in two ways: by revealing how to enhance content on person-centred care, which can help clinicians tailor care for women who vary by a range of intersectional factors; and by revealing the need to specifically acknowledge disparities among women, which can encourage clinicians to apply the aforementioned strategies. These strategies can serve as the basis for developing new or strengthening existing dementia care policies or programs, education and point-of-care tools for clinicians, and measures for evaluating dementia care in the context of quality improvement or future research. Given the long-standing emphasis on person-centred dementia care, yet lack of wide agreement on explicit processes to achieve its broad conceptual components (Fazio et al., 2018), the strategies identified here for achieving person-centred care, both general and dementia-specific, extend prior conceptual frameworks.
This study found that many guidelines lacked person-centred care content, and even when mentioned, details were brief, providing little assistance to clinicians who have advocated for greater guidance (Bourque & Foley, 2020; Koch et al., 2010; Mansfield et al., 2019) given lack of training in person-centred care (Anderson & Gagliardi, 2021a; 2021b). This raises the question of why included dementia guidelines, and guidelines on other topics did not address person-centred care for women (Abuwa et al., 2023; Gagliardi et al., 2019). Notably, few guidelines included in this study involved women living with dementia or caregivers in their development. It is now well-recognized that guidelines better address patient and family perspectives and preferences when those stakeholders are involved in establishing guideline topics or questions, assembling and reviewing guideline content, and formulating the recommendations (Armstrong et al., 2016). Resources are available to assist developers in engaging patients and families in guideline development (Kim et al, 2020; Kim et al, 2021; The Guidelines International Network (GIN) PUBLIC Working Group, 2015). Those resourcesand the strategies identified in this research could be used by developers of dementia guidelines to expand the person-centred content of their guidelines, particularly for domains that were not well addressed: fostering a healing relationship, managing uncertainty, promoting dignity and enhancing quality of life.
Despite the disproportionate impact of dementia on women, the near absence of content related to sex and gender represents a considerable gap in guidance for clinicians on how to enhance person-centred care for women living with dementia and caregivers, which is needed to overcome a lack of training among clinicians in women’s health (Anderson & Gagliardi, 2021a), documented disparities in the quality of dementia care experienced by women (Sourial et al., 2020), little research on how to alleviate the burden on women caregivers, and a lack of research on support for women living with dementia (Bartlett et al., 2018; Erol et al., 2015). Future research is urgently needed to more fully understand the experiences and needs of women living with dementia and caregivers, and how to promote and support person-centred care for women affected by dementia, knowledge needed to enable clinicians and health systems to optimize care and associated outcomes. In the meantime, guidelines could be strengthened by noting the disproportionate impact of dementia on women (Bott et al., 2016; Prince et al., 2015; Sourial et al., 2020); including guidance generated in prior research based on consultations with women on how to improve person-centred care (Filler et al., 2020; Gagliardi et al., 2020), and specific guidance compiled in this research on how to do so; for example, fully assess women’s circumstances to develop an individualized plan and ascertain if women with dementia have sufficient caregiving from family members or other supports.
This study featured multiple strengths. We used rigorous methods to search for and extract data from guidelines, and complied with relevant research reporting criteria (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005; O’Brien et al., 2014). To guide data extraction and analysis, we employed established frameworks of general and dementia-specific person-centred care (Fazio et al., 2018; McCormack et al., 2011). To guide future guideline development, we charted gaps in guideline content, which identified guidelines that better addressed person-centred care and guidelines that should be strengthened in future iterations. To guide future policy and practice, we compiled examples of person-centred content and strategies to achieve person-centred care. We must note a few limitations. Despite employing a comprehensive search strategy, we may not have identified all relevant guidelines. This was further limited by including only guidelines on the overall management of dementia, and those published in English language. However, using this research and its findings as a guide, others can examine the content of guidelines on specific dementia topics and guidelines published in other languages.
Conclusions
Despite the disproportionate impact of dementia on persons living with dementia and caregivers who are women, and the long-standing emphasis on person-centred dementia care, this analysis of 15 guidelines on the overall management of dementia revealed inconsistent and limited content across guidelines on person-centred care and support for women affected by dementia. Hence, guidelines, which are tools used by clinicians to inform practice, must be strengthened with guidance to help clinicians achieve person-centred dementia care for women living with dementia and caregivers. Our study revealed 32 general and 18 dementia-specific person-centred care strategies. This compiled knowledge could be used by developers to enhance the content of current or future dementia guidelines, and to develop dementia care policies or programs, education and point-of-care tools for clinicians, and measures for evaluating dementia care in the context of quality improvement or future research. Given the lack of content on sex and gender, and a similar lack of existing research on these issues, future research is essential to understand how to promote and support person-centred dementia care for women affected by dementia.
Supplemental Material
Supplemental Material - Do clinical guidelines support person-centred care for women affected by dementia: A content analysis
Supplemental Material for Do clinical guidelines support person-centred care for women affected by dementia: A content analysis by Nevetda Gengeswaran, Alec Brandwood, Natalie N Anderson, Jessica U Ramlakhan and Anna R Gagliardi in Dementia
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
All data generated or analysed during this study are included in this published article and its supplementary information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.