
Abstract
Introduction
This article reports on the co-production of a dementia research funding application, involving a diverse group of people with lived experience of dementia collaborating with a researcher. This article is also co-produced by the group. The application was successful. Here we reflect on the process and what we learned from it, to inform future work in this area. First, we outline the context of Patient and Public Involvement (PPI) in the UK, before outlining the nature of the co-production work, presenting our reflections on the experience and sharing key learning points.
Patient and public involvement and engagement
Patient and Public Involvement (PPI) means people who have lived experience of an area of health or social care informing and shaping research in that area. It is different from taking part in research as a ‘research participant.’ PPI allows research to be conducted ‘with’ or ‘by’ patients and the public, compared to traditional models of research, where studies are conducted ‘to,’ ‘about’ and ‘for’ them (National Institute for Health Research: 2003). PPI aims to improve health and social care research, ensuring that it focuses on priority outcomes for real people in the real world (Innovations in Dementia, 2023). The term ‘Engagement’ has recently been incorporated into what was previously PPI, creating the title Patient and Public Involvement and Engagement (PPIE), to denote that people with lived experience should also play a significant role in how research information and knowledge is shared with target audiences.
Patient and Public Involvement and Engagement (PPIE) origins can be traced back to the 1970s (Beresford & Russo, 2020; Ocloo et al., 2021) emerging within the context of two main developments. Firstly, emancipatory disability research aimed to ‘equalize the relationships of research production between researcher and researched’ (Beresford & Russo, 2020) to bring about health and social care change in line with the rights of underrepresented groups. Secondly, a later movement came from within the health and social care and research institutions themselves, with the emergence of INVOLVE (2003), which in 2020 became the NIHR Centre for Engagement and Dissemination. The NIHR goal, based on the democratic principle that people who are affected by research have a right to have a say in it, is to embed PPIE in health and social care research processes. PPIE has become a key requirement of many UK research funding bodies.
It is important to highlight that the term Patient and Public Involvement and Engagement (PPIE) has been contested as disempowering, including by people living with dementia. The Dementia Enquirers (Innovations in Dementia, 2023), a group dedicated to research led by people living with dementia themselves, argue that the use of an acronym can be confusing, that people tend not to identify as ‘patients’ in relation to their dementia, and that PPIE feels too much like a term created by academics. It is increasingly advocated that PPIE groups create their own group name with which they identify, for example, the NHS Research Scotland Neuroprogressive and Dementia Network PPIE group labelled themselves ‘Partners in Research’ (NHS Research Scotland, 2023).
Co-production
In practice, approaches to Patient and Public Involvement and Engagement (PPIE) vary from patients and the public involved in a purely advisory role, aligned to the idea of having a right to a say in things, to a more empowering ‘co-production’ approach, with power shared equally with researchers or with researchers acting as advisors. Key principles of co-production are power sharing and joint ownership of key decisions, including and valuing the unique skills and perspectives that each person contributes, reciprocity (everyone should get something from it), and building and maintaining relationships between contributors (NIHR, 2021).
Equality, diversity and inclusion
UK Patient and Public Involvement and Engagement (PPIE) contributors have traditionally been drawn from white middle-class populations (Russell et al., 2020) despite evidence that in most healthcare systems, ethnic minority populations and those from areas of deprivation experience disproportionate difficulties accessing health services, and experience poorer health outcomes (British Medical Association, 2021; The Kings fund, 2022).
There is a need to ensure wider representation within PPIE particularly including those who are underrepresented in research about their own care and support (Ocloo et al., 2021): people from minority ethnic backgrounds, those with varied cultural and religious beliefs, those from areas of deprivation and/or rural communities, LGBTQ + people and those with cognitive difficulties. Widening PPIE is essential if health and social care research is to be co-produced in a way that understands and meaningfully addresses inequalities faced by diverse groups in society.
Co-production in dementia research
Existing published work on co-production in dementia research covers a wide range of perspectives. General guidance on co-production includes accessible guides with tips for researchers, written by or co-written with people living with dementia (Donaldson et al., 2023; Innovations in Dementia, 2023; Dementia Voices, 2021) Other work focuses on the reflections of people living with dementia who have taken part in co-production (Dementia Voices, 2021; Lord et al., 2022). Gordon and McKeown (2020) for example explore the personal impact of the first author’s involvement in several co-production groups and activities, experienced as part of his rehabilitation, and an important legacy he will leave his grandchildren.
There is a body of research on co-producing or ‘co-designing’ dementia-related health and social care interventions (Davies et al., 2019; Dodd et al., 2021; Lord et al., 2022). This includes engaging people with dementia, family carers and health and social care professionals in co-designing interventions to support people with dementia to remain living in their own homes. This work highlights the importance of creating a positive and enabling atmosphere for the co-production work, of contributors feeling that they had impacted on the outcome, ensuring contributors have the information they need, supporting those with cognitive difficulties, providing accessible regular updates, and prioritising the needs and voices of people with dementia (Lord et al., 2022).
Co-production of health and social services is another area addressed in the literature, for instance for reporting on how people with dementia co-produced ‘Meeting Centre’ services, providing peer support for people newly diagnosed with dementia (Söderlund et al., 2022). There is also work on co-producing data analysis in dementia research, for instance, involving people with experience of dementia in analysis of video data of interactions between doctors and patients in care homes (Dooley, 2020). McConnell et al. (2019) combined co-production and evidence approaches to develop a definition of empowerment in dementia.
Addressing a gap in the literature
Despite this growing body of literature on co-production in several areas of dementia research, there is a lack of published work on co-producing a dementia funding application: developing a proposal and a credible funding bid from the very start of an idea. Innovations in Dementia (2023) comment that ‘PPIE can (and should) happen even before the research starts, with academic researchers encouraged to talk with people to find out the issues that are most important to research. However, in our experience this does not happen very often!’ (Innovations in Dementia, 2023, p. 3).
This paper aims to address this gap in the literature, by providing an example of how we co-produced a dementia research funding application and to share lessons learned in the process, to inform other researchers and non-researchers who are thinking of getting involved in co-production.
Background to study
Setting up the lived experience group
At the beginning of 2022, first author SG, a researcher, had a broad idea for a research project on developing primary care workforce communication skills training, to support delivery of personalised dementia care planning within primary care. This was based on NHS England’s vision for every person with dementia to have a personalised support plan, outlining their priorities for action, achieved through ‘proactive personalised conversations’ focusing on ‘what matters to them, paying attention to their needs and wider well-being’ (NHS England, 2017). However, there is limited guidance on how to facilitate these personalised conversations to find out what really matters to people with dementia and carers. The idea was about developing workforce communication training to address this issue and was inspired by SG’s previous work on primary care-based dementia projects D-PACT (https://www.plymouth.ac.uk/research/primarycare/dementia/dementia-personalised-care-team) and PriDem (https://research.ncl.ac.uk/pridem/) and her speech and language therapy background.
In April 2022, SG was awarded a ‘National Institute for Health Research Three Schools Dementia Career Development Fellowship’ to fund Patient and Public Involvement and Engagement (PPIE) work, specifically to help develop the research idea into a funding application. Early on, given the potential difficulties with terminology around PPIE, it was decided to refer to members as a lived experience group, and to later co-produce a name for both the group and the project. The aim was to recruit six people with lived experience of dementia, including underrepresented groups in dementia research.
The group would work with SG to co-produce a research funding application over eight group meetings. Most meetings would take place remotely, with funding allowing for one face to face meeting. Calls for membership targeted social media and national dementia organisations including DEEP, Touchstone, Opening Doors, and the Young Dementia Network, as well as an existing University College London group of ‘Experts by Experience’ who had been involved in other research projects. The statement in Box 1 was included in the call out to emphasise the aims of inclusivity and diversity:
Box 1: Inclusivity and diversity statement
Who am I looking for? People with a diagnosis of dementia, carers, or former carers, who would I would like to include a
SG spoke individually via phone or video call with the first eight people who responded to the call out, to explain more about the group purpose and find out more about the individuals’ backgrounds and motivations. She prioritised inclusion of the one person with dementia and achieving a diverse mix of people. With the aim of power sharing within the group, SG identified two co-leads, with a wealth of PPIE experience, with whom she would collaborate to plan and facilitate meetings. They would provide advice and support to SG and collate ongoing feedback from the group. Two respondents who did not join the group started PPIE roles on other dementia studies within the University. SG was concurrently collaborating with a practitioner advisory group for GPs, social prescribers and dementia advisors, the discussions from which fed into the lived experience group and vice versa, however this is not the focus of the current paper.
Representation within the group
The group consisted of one person with dementia, four carers and one former carer, and was a culturally diverse group, with members identifying as Asian British (Indian), White Irish, White English, White Scottish and Mixed (South Asian and Black). Group members lived in London, the Midlands, the North of England and Scotland, and included four females and two males. Two of the group experienced significant visual difficulties. For the purposes of this paper, members chose to provide a mini portrait to give a flavour of themselves and why they joined the group, shown in Figure 1. Mini portraits by group members.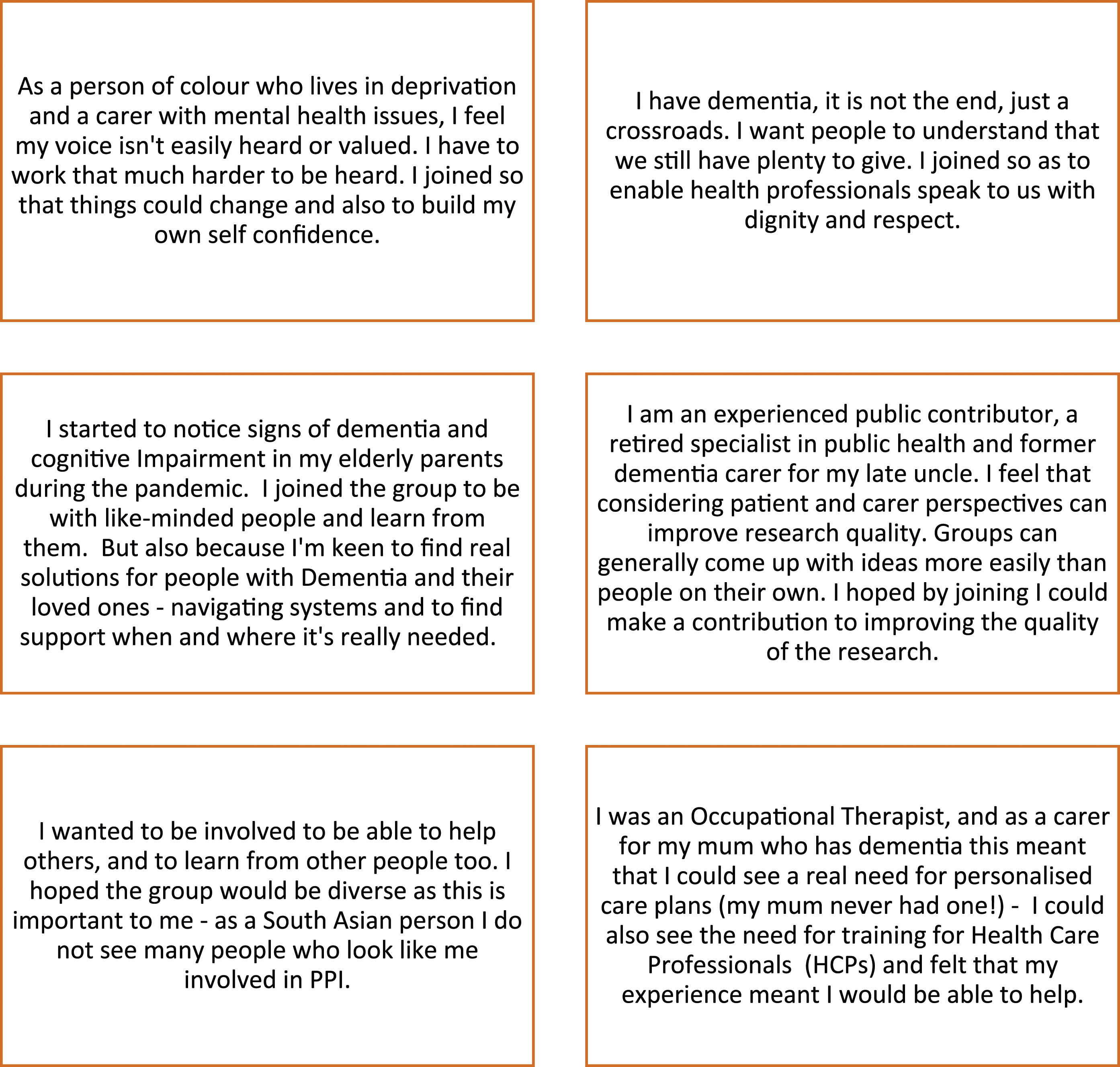
Aspirations for the group
Most of us hoped the group would be supportive and respectful, that the group would be diverse and that everyone would feel involved and learn from each other. As dementia can be an emotive and highly personal topic, we hoped everyone would feel free to express themselves without having to censor their real experiences; that they would feel protected psychologically, listened to and understood. It was hoped the group would instil a sense of belonging and camaraderie and that it would be enjoyable. One member expected that the group would just involve being ‘given stuff to look at and critique’ but hoped for a greater level of involvement.
Group meetings
Meetings of 90 minutes were held roughly monthly, from July 2022 to June 2023, according to the research funding application timeline, which involved two stages and an interview with the funding panel, depending on success as each stage. The approach to facilitating group meetings was informed by guidance on co-production in research, for instance ensuring members understood the purpose of the group and the meaning of co-production, agreeing ground rules, building relationships and continuous reflection on the successful running of the group and progress towards planned outcomes (NIHR, 2021). Meetings were also informed by guidance on co-production in dementia (Donaldson et al., 2023; Innovations in Dementia, 2023). Practical tips on running online meetings involving people living with dementia were considered such as scheduling regular breaks, making sure there are no surprises (e.g., by sending a regular agenda), pacing sessions by allowing members time to digest information and ask questions, trying to limit screen sharing and allowing space for building relationships: ‘a sense of camaraderie is so important’ (Donaldson et al., 2023).
At the suggestion of and facilitated by the co-leads, ice breaker activities were incorporated in some sessions, for example, sharing a favourite holiday or song. In addition to verbal methods of communication, a variety of methods for contributing were available including the Zoom chat function, Padlet (Fisher, 2017), Google docs and email. Although the aim was for at least one meeting to take place in person or as a hybrid meeting, despite attempts to make this happen, it was not possible due to illness and the practicalities of bringing together a group of people who were spread out over the UK. SG planned a visit to our Scottish group member one to one, but even this was hampered by a last-minute flight cancellation.
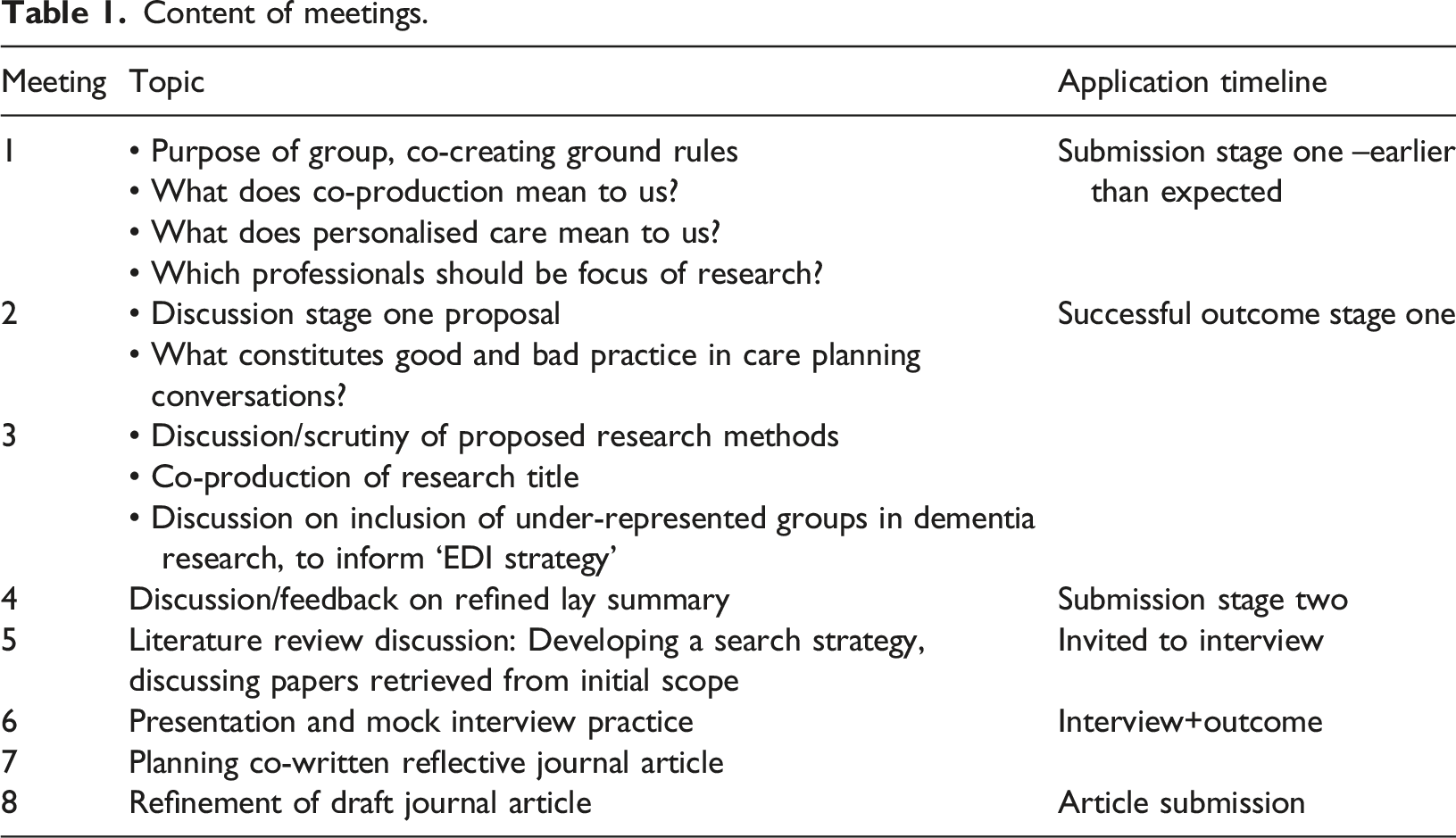
Content was iteratively produced rather than planned in advance. Table 1 shows the topics discussed throughout the eight meetings. The Supplementary File sets out in detail the activities undertaken in each meeting, the resulting outcomes/decisions and ongoing progress with the funding application.
An opportunity to submit a stage one outline application arose much earlier than expected to a funding stream that was different from the one we had built the timeline around. However, even after one meeting we found that the research question had been narrowed down and we had formulated a clearer plan, enabling SG to write and submit the stage one application. Table One shows that the group engaged in some important discussion that informed the application development and provided a mock interview for SG ahead of her interview with the funding panel.
We decided that we wanted to share our experiences of working together to inform other researchers and public contributors who may wish to get involved in co-production at this early stage of shaping a research project.
Methods
We co-produced a set of questions to guide our reflections; broadly: ‘What were the strengths of the group?’ ‘What were the benefits to group members?’ ‘What were the challenges?’ and ‘What improvements could be made in the future?’
All agreed that SG would meet individually with each person to gather reflections. After meeting with each group member, SG wrote a first draft of the reflections. Some of the group chose to send suggested amendments in writing and others fed back verbally in the next group meeting. We agreed changes, including those that would make the article accessible to a non-academic audience such as reducing the use of acronyms, simplifying language in places, and keeping paragraphs short.
Initially, we presented our reflections as responses to the co-produced questions we asked ourselves, but following peer review of this article, we restructured the reflections to make sense of them in terms of the overall categories of diversity and inclusion, benefits to group members, and challenges. We embedded our insights on future improvements into the discussion.
Results
We now set out our reflections on our experiences relation to Diversity and inclusion (diversity within the group, enhancing inclusion through group facilitation and equality of reimbursement), benefits to group members and challenges. We agreed to illustrate our reflections with illustrative quotes. All quotes are from the authors of this article.
Diversity and inclusion
Diversity within the group
We valued the diversity within the group. The inclusion of a person of colour ‘in a position of power’ as co-lead was particularly welcome, as a signal that representation was going to be taken seriously. This was felt to contribute to a safe environment to share culturally related experiences of dementia. The inclusion of a person living with dementia as a co-lead was felt to be inspiring and helped to raise awareness within the group that a person living with dementia can be a role model and advocate: ‘the ultimate expert.’ The fact that the group was diverse in terms of gender mix, age and geographical location was also appreciated. We saw that the group was not ‘London centric’ and that important knowledge could be shared of variations in healthcare provision throughout UK, both rural and urban. Neither was the group ‘English-centric.' Our Scottish member was able to share knowledge about the inclusive nature of Scottish dementia strategy (Scottish Government, 2023), co-produced with those with lived experience and the third sector, from which we could learn.
Content of meetings.
Enhancing inclusion through group facilitation
We reflected on the elements of group facilitation that enhanced meaningful inclusion. Our aspirations for feeling supported and heard were fulfilled. Group members appreciated the contact with SG one to one, prior to the group. Hearing about her background and initial ideas for the project allowed them to feel reassured that the group would not only be interesting but run by someone who had background knowledge and empathy. The involvement of co-leads in facilitation, helping to steer the group, was felt to be inclusive and democratic. The co-leads themselves felt valued by SG, who met with them separately to the meetings and sought their advice throughout. One co-lead commented: ‘Sometimes health researchers think we are rent a mouth – they may not see us as intelligent enough to work alongside them.’
Agreeing ground rules with each other from the beginning led to an atmosphere of respect, acceptance of diverse backgrounds and cultures, enjoyment, and a mutual desire to share knowledge: ‘There was a plethora of knowledge to tap into and offer.’ The tone set by the SG was that she was there to learn, and for some members that was refreshing: ‘There was a willingness to learn about people’s experiences. For real!’ ‘This hasn’t come over as all academic as some groups do. It’s been human.’
Having agendas and regular meeting notes sent out in a timely fashion was appreciated: There was a balance between sticking to an agenda and allowing for free-flowing conversations, and this was felt to help build relationships: ‘It was good that we felt free to roam. Everything is relevant – even the weather and whether we are having a good day or not.’ ‘There hasn’t been much time to bond but we seem to have done it without any effort. For co-production to work, there needs to be empathy between people – which has come without making the effort.’
Having feedback in each meeting about what had been achieved was felt to be important: ‘It always felt like we’d achieved something, and it was clear what we’d achieved.’ Being able to use a range of options for contributing, such as the Zoom chat function or Padlet (Fisher, 2017), allowed members to express their thoughts before the conversation had moved on, and went some way towards compensating for interactional difficulties associated with virtual meetings. Some of us were naturally quieter than others, and co-leads felt it was particularly important to find a balance between opening space to contribute if wanted, whilst not putting anyone on the spot: ‘Everyone has different processing speeds. It felt OK to step back and then say something when feeling comfortable.’ ‘Sometimes what you’re thinking has already been said, so it’s not that you don’t want to contribute.’ It was felt that, in the spirit of co-production, everyone was enabled to share insights that influenced the ongoing aim of shaping the funding application.
Contrary to one member's expectation that involvement would mean solely critiquing a researcher’s plans, members felt they had truly been included in creative co-production: ‘This group exceeded all my expectations. This is the most involved in anything that I’ve ever been.’ ‘It’s been exciting to be able to help create something. Normally we are just quotes in a paper.’
Having distinct themes for each meeting was felt to be helpful, for instance in one meeting the discussion was on research methods and in another it was developing an EDI strategy. In addition, having the opportunity to ‘delve deep into things’ with the potential for new lines of enquiry to be opened and explored, was seen as exciting in comparison to some previous experiences of Patient and Public Involvement work: ‘Sometimes health researchers have a hidden agenda. They have their own theories and ask closed questions “do you think it’s because…” to get you to answer in a constraining way.’
We felt that the way in which the research project name was created represented true co-production, with members putting forward ideas, gradually shaping the name, until one group member (FD) came up with an acronym and name acceptable to and agreed by all: CAPPD.’
A crucial element of the content was that throughout, members felt they could understand the potential outcomes of the proposed research project. One member reflected on how a key motivator for continuing to contribute was being able to envision the potential real-world impact.
Equality of remuneration
All members felt that navigating university systems for claiming expenses can be inaccessible for people with dementia and carers. SG supported every member to complete their university expense claims and chased overdue payments on their behalf. This was appreciated and seen as crucial to feeling recognised and equal: ‘This is something I can’t do myself. It should be a simple process. All universities have different processes - it’s a headache.’ ‘Some studies take a long time to pay you – it has been up to 8 months. When you are properly paid in a timely fashion, you feel valued. Payment shouldn’t be an afterthought. This shows the power balance. The researchers get paid on time. They are up there, and we are down here.’ ‘You shouldn’t feel like you have to chase or beg.’
Not all lived experience contributors wish to be paid. ‘Some might feel they can’t take the money because they feel guilty. Some might feel they don’t want to. Some might feel they want skills and development rather than money. Some might want real recognition in a space rather than money. Some might feel it is a token gesture. Remuneration is complex.’ However, the group felt strongly that proper remuneration should always be offered in a way that is inclusive to all.
Benefits to group members
We all reflected that we had learned something from being involved; about ourselves, about other people and about research in general. This included learning from the expertise of others, becoming more skilled in actively listening, learning that ‘Everybody is going through their own thing. All experiences are unique and valid’ and learning how funding bids are put together. This opportunity for learning was described as ‘Catnip to the brain.’
The co-leads felt they had learned new skills in leadership and mentoring and formed a relationship with each other that would outlast this project. One co-lead commented: ‘I’ve become more connected with the other co-lead, and we feel more empowered now to share experiences but also expertise in our respective areas. If done well, co-leading provides development for individuals who can enrich a specific project but also go on to enrich other academic research projects.’ Involvement also led to changes in how we felt about ourselves: ‘It made me feel even more useful to society than I did before. People living with dementia need to realise they can be useful. I feel proud and happy…gives me a warm fuzzy feeling.’ Some of us felt the experience had helped build our confidence and self-esteem, and that this was in part due to feeling heard and valued as equals: ‘Whatever I say is being appreciated and is actively making a difference. The more we meet the more I look forward to it. I can relax and take the time to think. You can’t bring great thoughts without space to have a voice. It makes a difference.’ Being able to reawaken parts of the self was also a key benefit: ‘As a carer you can lose your sense of self. The status of carers is zero. This reminded me of my former qualification as an OT and makes me feel good about myself. My experience is valuable and is recognised by the group. I’ve been cynical about attending these things in the past.’
For some of us, long-lasting friendships developed. For the two co-leads, this led to a collaboration on their own project and becoming mentors on the co-produced funded project. Our member living with dementia stated: ‘Pre-diagnosis I had no real academic experiences. This gave me the confidence to come out of my shell and admit to myself first, and then the others, I could do even more than I thought I could, having dementia, so much so I’m going to be a mentor and help with carrying out interviews on the funded project.’
Some of us became connected with the university Patient and Public Involvement and Engagement (PPIE) network, which opened opportunities for contributing to a range of dementia related projects.
Challenges
Whilst virtual meetings have advantages in terms of increasing diversity, several of us felt important aspects of co-production were missing. Relationship-building was more challenging due to the formality of Zoom and the flow of discussion could be hampered at times. For instance, it was more difficult than in face-to-face meetings to interject in a timely manner to challenge a point, and harder to show empathy remotely, making virtual meetings feel unnatural at times. As a result, some of us felt we were only really getting to know each other and bond as a group once it was nearly all over.
When members chose not to have their cameras on, this was accepted by the group with compassion - ‘everyone has their reasons,’ however this meant having to work harder to ‘tune in’ to what people were saying due to a lack of non-verbal cues: ‘It would have been good to see everyone. People with dementia find that helpful.’ We felt that more ice-breaker activities and time to share more about their own lives would also have supported relationship-building: ‘I wish people had talked more about their caring experiences.’
Accessibility of group materials was another area that could have been improved. Hard copy documents were posted to those with visual difficulties, but this offer could have been more tailored in terms of preferred font size, as this can change over time.
There were also challenges associated with discussions around developing an EDI strategy (see Table 1, Session 3). This was in part because experiences of marginalisation are so individualised and highly emotive, often rooted in historical experiences of racism. For some, it felt like a competition about which communities most needed to be represented in the research. The discussions were ranging and unfocused. It was strongly felt that the links between racism and lack of access to services should have been foremost in the discussion, and experiences of people of colour within the group prioritised.
Discussion
Although group diversity was a strength, greater representation of people with dementia would have been enriched the group. Under-represented groups within dementia were also not given a voice, for example, people from the LGBTQ + community. Whilst it would not be realistic to include all marginalised groups in society, in future we would look to include a wider range of perspectives and also ensure that individuals’ needs for accessible resources is reviewed regularly.
Our suggestions for managing EDI discussions include presenting background literature on EDI in dementia research and definitions of terms such as racism, xenophobia, discrimination and ‘health inequalities’ from the outset, to ensure everyone starts with the same understanding and a focus for discussion. Facilitating the discussion in a more structured, directive way than usual, so that everyone has equal time to talk, may also help to avoid feelings of competition or exclusion.
Despite the challenges associated with EDI discussions, some illuminating experiences were shared. Powerful personal stories of good and bad practice in care planning conversations threaded through the eventual application and will always stay with group members, informing their future work. For instance, one member told us about how he has supported a relative in care planning conversations with a health care professional (HCP). The relative was a devout Muslim woman. When she requested support with meeting her spiritual needs, the HCP responded that there was nothing that could be done about that and rolled her eyes. The group talked about what an alternative personalised response might look like, for example, ‘Let me try and understand more…Let’s work out how we can make that happen.’
At times we asked ourselves ‘Is this really co-production?’ especially as SG took a lead by presenting ideas, proposing methods, searching for literature to bring to the group, and writing an initial draft of this article. However, co-production is about each member bringing their unique skills and knowledge to the process, and together creating something out of their combined talents. One member described this a ‘a critical mass.’ As a group we negotiated our roles and involvement; a key element of co-production (Innovations in Dementia, 2023). A counter argument is that researchers should work harder to rebalance the existing power dynamic between researcher and non-researcher. Time and funding constraints limit what can be achieved, but it would have been more truly ‘co’ to build in more time and resources for people to develop skills. Warren et al. (2023, p. 5) argue that it is important in co-production to ensure ‘… everyone can take part in the elements they choose to be included in, and support and training is provided for any elements that may require this for meaningful participation.’
Conclusions
Working alongside a diverse lived experience group to develop a research funding application, from the very start of an idea, has led to funding success in this instance. The involvement of co-leads sent a powerful message to the group that equality and inclusion were priorities. When taking a co-production approach, it does not matter if initial ideas are unformed or vague. We would argue that if a researcher is not rigidly wedded to an idea, but comes with an open mind, and wants to learn and be challenged, this helps open the door to creative thinking and allows co-production to happen. In turn, this can lead to a research proposal addressing the interests of those the research seeks to support.
Co-production is built on trust and respect (The Dementia Enquirers Gold Standards for Co-Research, 2023) and research culture needs to be kinder and more focused on building relationships for co-production to flourish (Staniszewska et al., 2022). Our reflections emphasise the importance of bonding as a group and we learned how this can be challenging, but possible, when meeting virtually. Building in time for ice breaker activities, everyday conversation and sharing life stories is essential for trust to develop. ‘Achieving equality of power in co-production is extremely challenging, but ‘building trust and maintaining strong and respectful relationships….can work towards attenuating some power disparities’ (Gaffy et al., 2022, p. 4). Offering hybrid meeting options could also be explored, in addition to facilitators travelling to visit group members in person one to one.
There was a strong element of reciprocity. Mutual learning was a key benefit felt by all, including learning that people living with dementia can be advocates and role models. This helps recast the narrative of dementia ‘beyond binaries of tragedy or living well, proposing different possibilities for liveable lives that encompass vulnerability and struggles as well as happiness.’ (Ward & Sandberg, 2023). This learning will be taken forward by group members into future PPIE work, thus benefitting wider research.
When applying for funding to undertake development work, researchers need to cost in time for relationship building, prioritising this as an essential element of successful co-production. This should include realistic funding for travel, to enable individual or group in-person relationship building.
Finally, remuneration is a key issue. If payment processes do not operate smoothly, co-production partners do not feel recognised as equal co-workers whose contributions are valued. Navigating university systems for claiming expenses can not only be inaccessible for people with dementia and carers, but also for many other groups with lived experience of physical and mental health conditions that universities seek to engage in research. Simpler, more streamlined processes, and options for alternative payments (e.g., gift vouchers) whose earning ability is capped due to the state benefits system, would enable Universities to engage a more diverse network of co-production partners. That can only be a good thing for the future of co-produced dementia research.
Supplemental Material
Supplemental Material - Reflections on co-production: Developing a dementia research funding application with a diverse lived experience group
Supplemental Material for Reflections on co-production: Developing a dementia research funding application with a diverse lived experience group by Sarah Griffiths, Martin Robertson, Chandrika Kaviraj, Firoza Davies, Marie McDevitt, Al Richards and Marcelline Russell in Dementia: the international journal of social research and practice
Footnotes
Acknowledgments
SG would like to thank her NIHR Dementia Career Development Award supervisors for their ongoing support: Nathan Davies (Associate Professor Ageing and Applied Health Research, Research Department of Primary Care and Population Health, University College London), Greta Rait (Professor of Primary Care and Population Health, Research Department of Primary Care and Population Health, University College London), and Mike Clark (Associate Professorial Research Fellow and Research Programme Manager, Care Policy and Evaluation Centre, at London School of Economics and NIHR School.
Author contributions
SG wrote the first and final draft. MR, CK, FD, MM, AR, and MR were members of the lived experience group, the subject of which forms this article. They contributed to planning the outline of the paper, they contributed their reflections on the co-production process, commented on all drafts, agreed changes to wording and content and advised on ensuring that the article would be accessible for non-researchers as well as researchers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute for Health and Care Research Three Schools’ Dementia Programme (6653765 Career Development Award). SG also receives support from the NIHR Applied Research Collaboration North Thames and Alzheimer’s Society and is funded through a Post-Doctoral Fellowship.
Ethics statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
She has been campaigning for better stroke, elder and palliative care and has been involved in research for several universities. She believes passionately in real world outcomes which directly support patients and their loved ones in challenging situations.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.