
Abstract
Introduction
The concept of personhood as a ‘standing or status that is bestowed upon one human being by others, in the context of relationship and social being’ (Kitwood, 1997, p. 8) revolutionalised dementia care. Personhood places emphasis on those around the person living with dementia and the vital role they play in supporting personhood. As such, dementia can be regarded as both an individual and a shared experience. Over two-thirds of carers of people with dementia are spouses (Wimo et al., 2013), consequently, a growing body of research has begun to explore the concept of ‘couplehood’ defined as ‘the extent to which one person perceives being married to another person’ (Kaplan et al., 1995, p. 317) and ‘feelings of belonging to a ‘‘We’’ or feeling like an ‘‘I’’ (Kaplan, 2001, p. 87). In reviewing the literature exploring the impact of dementia on marriage, Evans and Lee (2014) found that couples experience a great sense of loss, including loss of companionship, social networks, reciprocity, sexual intimacy, and ultimately loss of partner and marriage. However, the review included studies that were predominantly spousal carer perspectives. In contrast, a review by Wadham et al. (2016) included the perspectives of both partners with and without dementia and found that couples demonstrated a strong sense of commitment, togetherness and resilience, as well as made great efforts to preserve each other’s identity when adapting to changes in roles and responsibilities (Wadham et al., 2016). In response to this increasing recognition that dementia is a journey often shared within couples, research has begun to explore relationship-centred interventions, such as couples counselling (Auclair et al., 2009) or the development of self-management guides (Bielsten et al., 2018) for couples where one partner has dementia.
However, alongside the challenges and changes brought by dementia, couples are also likely to be adapting to living with other chronic health conditions. People with dementia, aged 65 or above, on average, live with 4.6 additional health conditions (Guthrie et al., 2012). Common co-occurring health conditions in people with dementia include diabetes, stroke, vision impairment, urinary tract infections, depression, hypertension, anaemia and cardiac arrhythmia (Bunn et al., 2014; Poblador-Plou et al., 2014; Scrutton & Brancati, 2016). Spousal carers are also likely to experience multiple health conditions, given that increasing age is associated with an increase in health conditions (Barnett et al., 2012). In addition, many carers often experience physical and mental health issues due to the stresses and strains of caring, financial worries and social isolation (Carers UK, 2019) which in turn can have a negative effect on the person with dementia’s health and wellbeing (Stall et al., 2019).
Whilst it is the norm, rather than the exception, that couples living with dementia are also living with multiple health conditions, dementia research often excludes participants if they have other health conditions (see Bosco et al., 2019). Both of the qualitative reviews described above do not include the experiences of couples living with other co-existing health conditions (Evans & Lee, 2014; Wadham et al., 2016) and therefore a more holistic picture of couples’ subjective experiences has not been captured. The results from this current review may therefore help to inform the development of couple-based interventions that are tailored to the needs of couples living with dementia and multiple health conditions.
Review aim and questions
The aim of this review is to explore the interplay between couplehood, dementia and multiple health conditions in married or unmarried couples. Specifically, it aims to answer the following review questions, developed following the Population-Concept-Context (PCC) framework (Joanna Briggs Institute [JBI], 2015): 1. In what way (if any) does living with dementia and multiple health conditions impact on couplehood? 2. In what way (if any) does couplehood impact on couples’ experiences of living with dementia and multiple health conditions?
The protocol for this systematic review was registered on PROSPERO (CRD42022381728) and can be accessed at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022381728
NB: In this review, the term ‘couple’ is defined as “Two persons married, engaged, or otherwise romantically paired” (Merriam-Webster, 2022a) and the term ‘partner’ is defined as “a person with whom one shares an intimate relationship: one member of a couple” (Merriam-Webster, 2022b). Both of these terms are used in this review to refer to married or unmarried partners or couples in romantic relationships.
Method
Review approach
A meta-ethnographic approach (Noblit & Hare, 1988) was used, which involves translating and synthesising concepts shared across primary qualitative studies in order to create novel ‘third order’ interpretations of the combined study findings (Sattar et al., 2021). The ENTREQ (Enhancing Transparency in Reporting the synthesis of Qualitative research) statement was used as a framework to structure the review (Tong et al., 2012) and the eMERGe guidance (France et al., 2019) was followed to ensure all important aspects of meta-ethnography were reported.
Search strategy
The STARLITE approach was used to inform the search strategy (Booth, 2006). Two parallel database searches were conducted in order to answer the review questions. The first database search involved seeking qualitative research exclusively on couplehood and dementia. The second database search involved seeking qualitative research exclusively on couplehood and multiple health conditions. The rationale for completing two separate searches was to broaden the scope of the literature, as combining all three concepts (i.e., couplehood, dementia and multiple health conditions) did not yield any applicable papers. An information specialist from the University of Hull provided guidance on appropriate search terms and filters. Both literature searches were carried out within the following five databases using EBSCOhost: Academic Search Premier, CINAHL Complete, MEDLINE, APA PsycArticles and APA PsycINFO.
Search strategy 1 – Couplehood and dementia
A systematic search on ‘couplehood and dementia’ was conducted on 30.01.2022 and updated on 08.02.2023. The synonyms for the search terms ‘dementia’ and ‘couplehood’ were informed by the search terms used in Wadham et al. (2016) review on couplehood and dementia. Terms relating to ‘couplehood’ were restricted to ‘Title’ only in order to reduce irrelevant papers and make the review feasible (Sattar et al., 2021) (see Supplementary file 1).
Search strategy 2 - Couplehood and multiple health conditions
A systematic search on ‘couplehood and multiple health conditions’ was conducted on 17.02.2022 and updated on 09.02.2023. Terms relating to ‘multiple health conditions’ were selected based on the findings from a scoping review that explored the definitions and concepts of comorbidity and multimorbidity in dementia (Dunn et al., 2022). Terms relating to ‘couplehood’ were restricted to ‘Title’ only (see Supplementary file 2).
For both searches, the records retrieved were filtered according to papers written in English Language and peer-reviewed journal articles, excluding books, protocols and grey literature. This was in order to make the review manageable due to restrictions in time and resources (Sattar et al., 2021), but is also appropriate in a meta-ethnography, where the focus is on a homogenous group of papers that provide ‘rich’ and ‘thick’ data (Barnett-Page & Thomas, 2009). No limits were placed on date of publication. Duplicate papers were automatically removed in EBSCOhost. The records were then imported from EBSCOhost to EndNote (The EndNote Team, 2013), where further duplicate papers were removed using the automation tool.
Study screening and data extraction
Inclusion criteria.
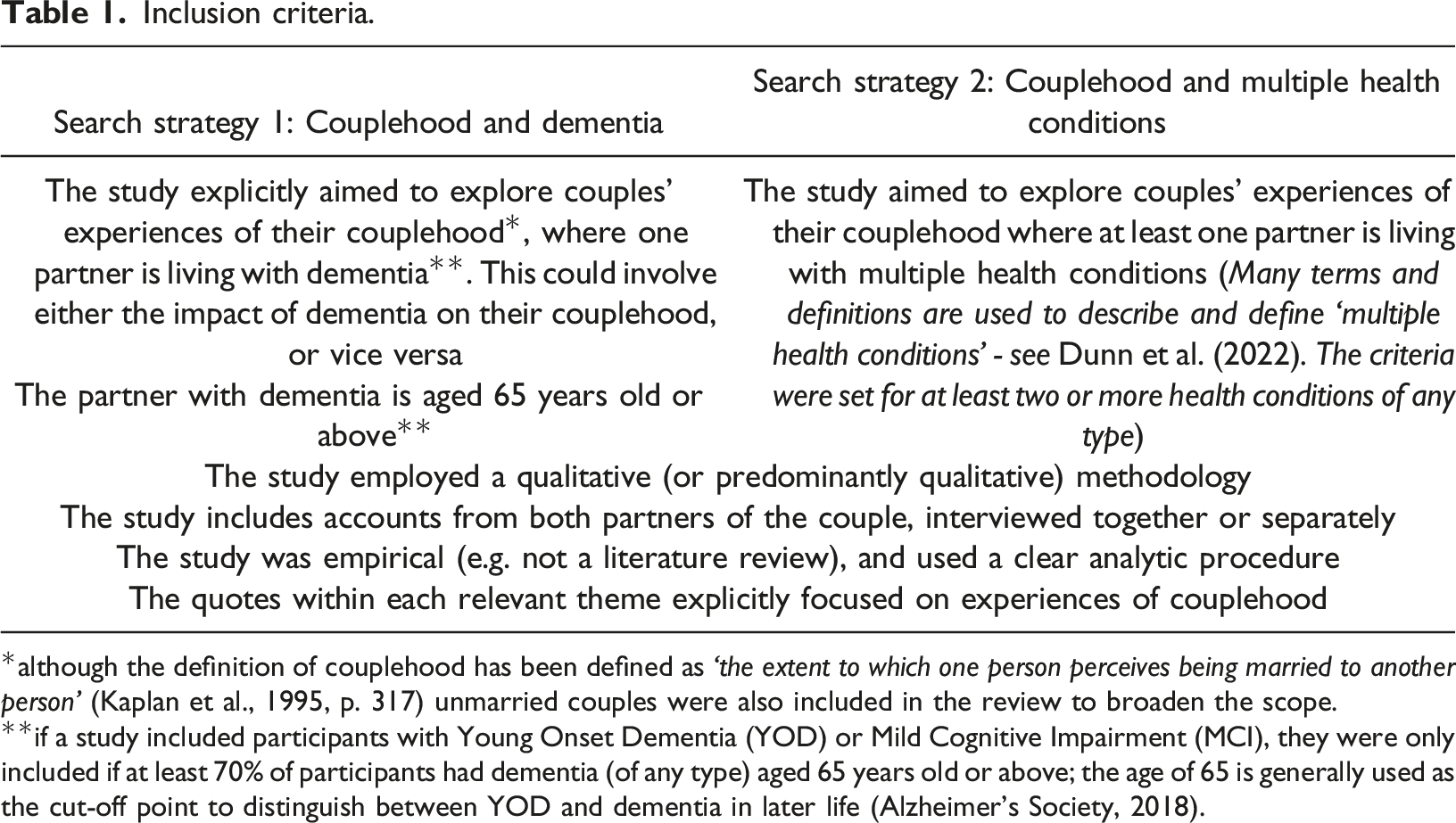
*although the definition of couplehood has been defined as ‘the extent to which one person perceives being married to another person’ (Kaplan et al., 1995, p. 317) unmarried couples were also included in the review to broaden the scope.
**if a study included participants with Young Onset Dementia (YOD) or Mild Cognitive Impairment (MCI), they were only included if at least 70% of participants had dementia (of any type) aged 65 years old or above; the age of 65 is generally used as the cut-off point to distinguish between YOD and dementia in later life (Alzheimer’s Society, 2018).
Exclusion criteria.
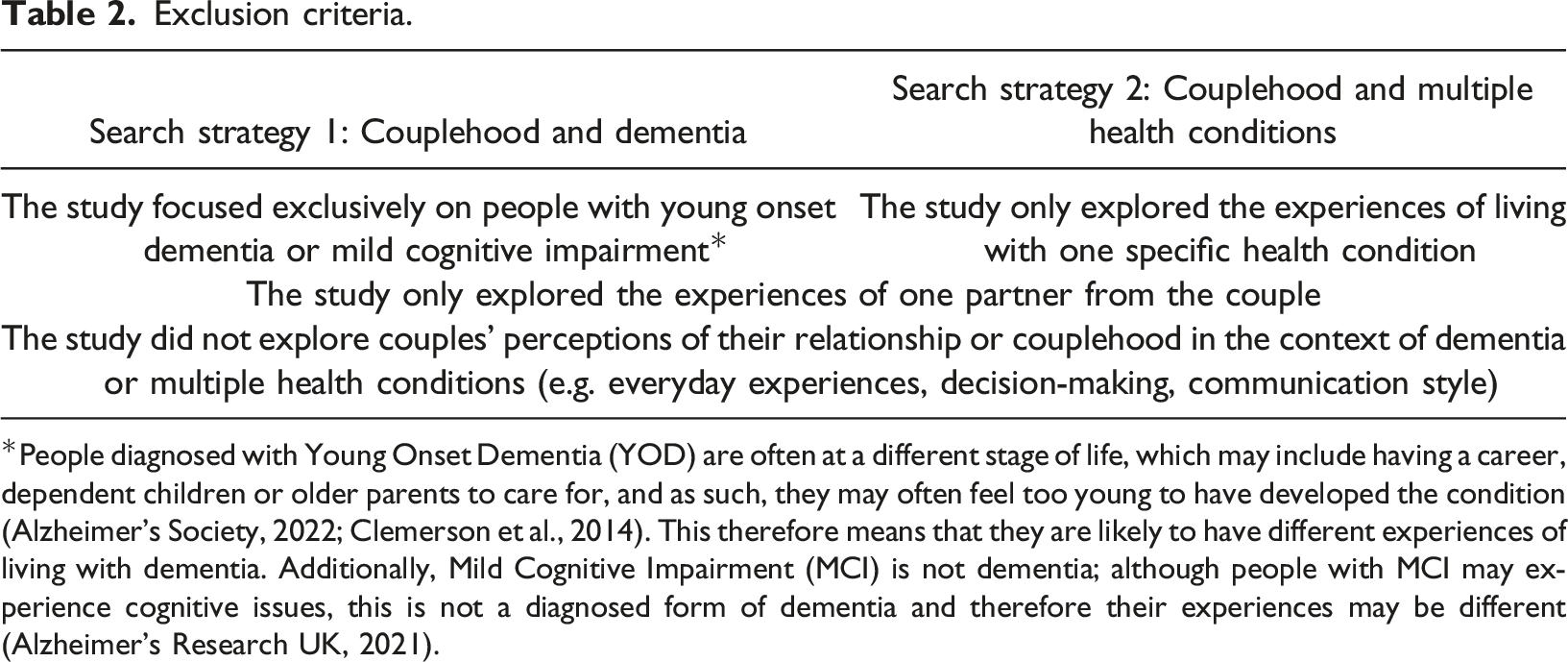
*People diagnosed with Young Onset Dementia (YOD) are often at a different stage of life, which may include having a career, dependent children or older parents to care for, and as such, they may often feel too young to have developed the condition (Alzheimer’s Society, 2022; Clemerson et al., 2014). This therefore means that they are likely to have different experiences of living with dementia. Additionally, Mild Cognitive Impairment (MCI) is not dementia; although people with MCI may experience cognitive issues, this is not a diagnosed form of dementia and therefore their experiences may be different (Alzheimer’s Research UK, 2021).
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021) was used to inform the procedure of selecting and retrieving papers (according to the above inclusion and exclusion criteria), which involved the following three steps: 1: screen titles and abstracts; 2: screen the chosen full texts for eligibility; and 3: retrieve and choose the final included papers for review. Additionally, the reference lists of the final included papers were checked to source any relevant papers missed from the initial search. RD conducted the search and screened the title and abstracts of papers, the full text of eligible papers and reference lists. The final included papers were discussed between RD, EW and AH, and any disagreements were discussed until a consensus was reached.
Quality appraisal
The Critical Appraisal Skills Programme (CASP, 2018) qualitative checklist was used to appraise the validity and rigour of the included papers. However, it was pre-determined that none of the papers would be excluded based on a low quality as the papers may still be relevant and offer rich or thick conceptual data pertinent to the research (Sattar et al., 2021). The order in which the studies are read and reviewed can affect the synthesis output (Sattar et al., 2021), therefore the studies were read in order of high to low methodological quality.
Meta-synthesis
Meta-ethnography was used to synthesise and interpret the qualitative findings across the studies, following the seven-step process developed by Noblit and Hare (1988) and further advanced by Sattar et al. (2021). The steps include: 1.Getting started (identifying an area of interest and determining if meta-ethnography is appropriate to answer the research question) 2.Deciding what is relevant to the initial interest (defining the focus of the synthesis, locating relevant studies, developing inclusion and exclusion criteria and quality appraisal) 3.Reading the studies (repeatedly reading and familiarizing yourself with the key concepts and metaphors, extracting the raw data) 4.Determining how the studies are related (looking across the studies for common and recurring concepts, developing initial themes and categories) 5.Translating the studies into one another (comparing and contrasting the concepts across the papers, considering study characteristics) 6.Synthesising the translations (the development of third order constructs through reciprocal translation/refutational synthesis. Developing a line of argument synthesis from the third order constructs). 7.Expressing the synthesis (the use of reporting guidelines such as eMERGE (France et al., 2019) and PRISMA (Page et al., 2021); summarising the findings, reporting the strengths, limitations and reflexivity and making recommendations and conclusions).
The study that scored highest on the CASP was read first and used as the ‘index study’ from which concepts were translated into other studies. First and second order data were extracted from each study using a data extraction form. The study findings were then read repeatedly (in order of high to low methodological quality), and any recurring concepts identified were highlighted and developed into themes. Each theme was underpinned by the study data, including participant quotes (first order data) and the author’s interpretation (second order data). The themes were discussed between the co-authors and refined in an iterative process to develop the final categories. The categories were then compared and contrasted across each paper, via a process of reciprocal translation, until third order constructs were generated. A line of argument synthesis was then created from the third order constructs, ‘making a whole into something more than the parts alone imply’ (Noblit & Hare, 1988, p. 28).
Findings
Search strategy 1 – Couplehood and dementia
Following the screening process, 14 papers were included for review (see Figure 1: PRISMA flowchart). The search was updated on 08.02.2023 (see Supplementary file 3). PRISMA flowchart for Search Strategy 1: Couplehood and dementia.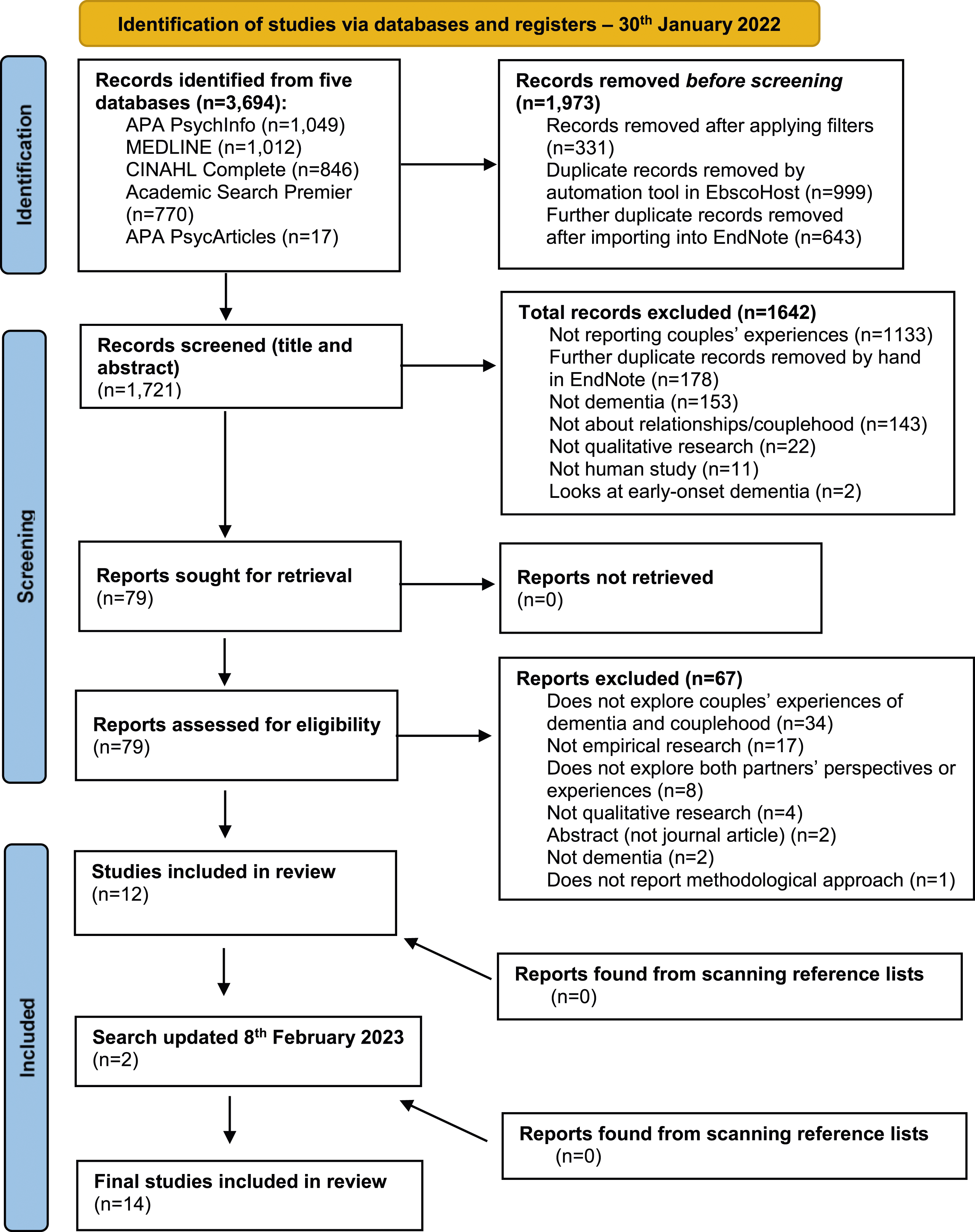
Characteristics of included studies
Participant characteristics
Summary of participant characteristics.
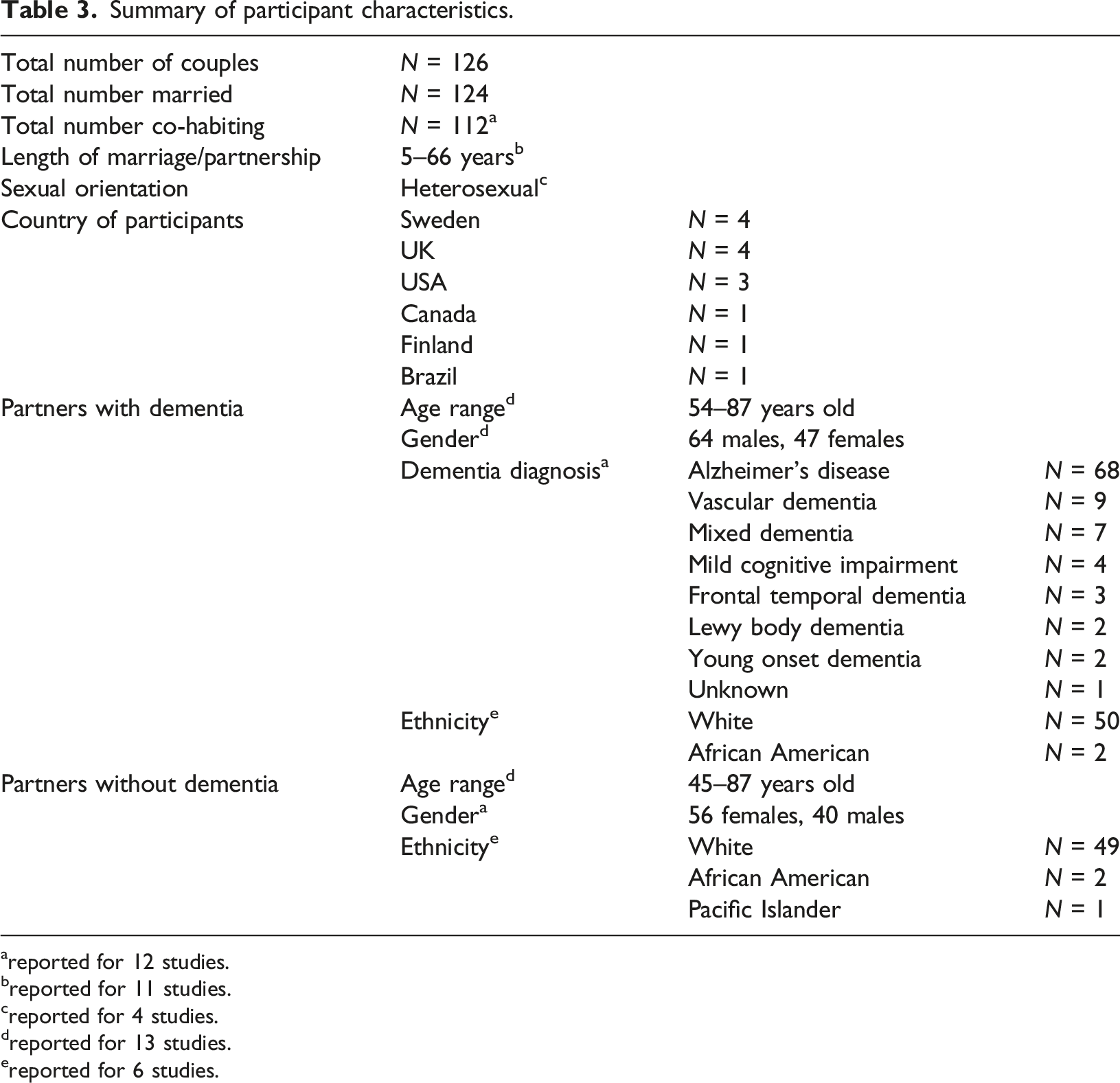
areported for 12 studies.
breported for 11 studies.
creported for 4 studies.
dreported for 13 studies.
ereported for 6 studies.
Only 7 of the 14 studies reported the severity or stage of dementia, which was; ‘mild’ or ‘early-stage dementia’ (Davies, 2011; Harris, 2009; Hydén & Nilsson, 2015); ‘mild to moderate stage’ (Albert et al., 2023; Sandberg, 2020); ‘mild to severe’ (Eskola et al., 2022) and ‘moderate stage’ (Swall et al., 2020). However, all 14 studies included participants that had capacity to consent to take part in the research.
Study characteristics
Summary of study characteristics.
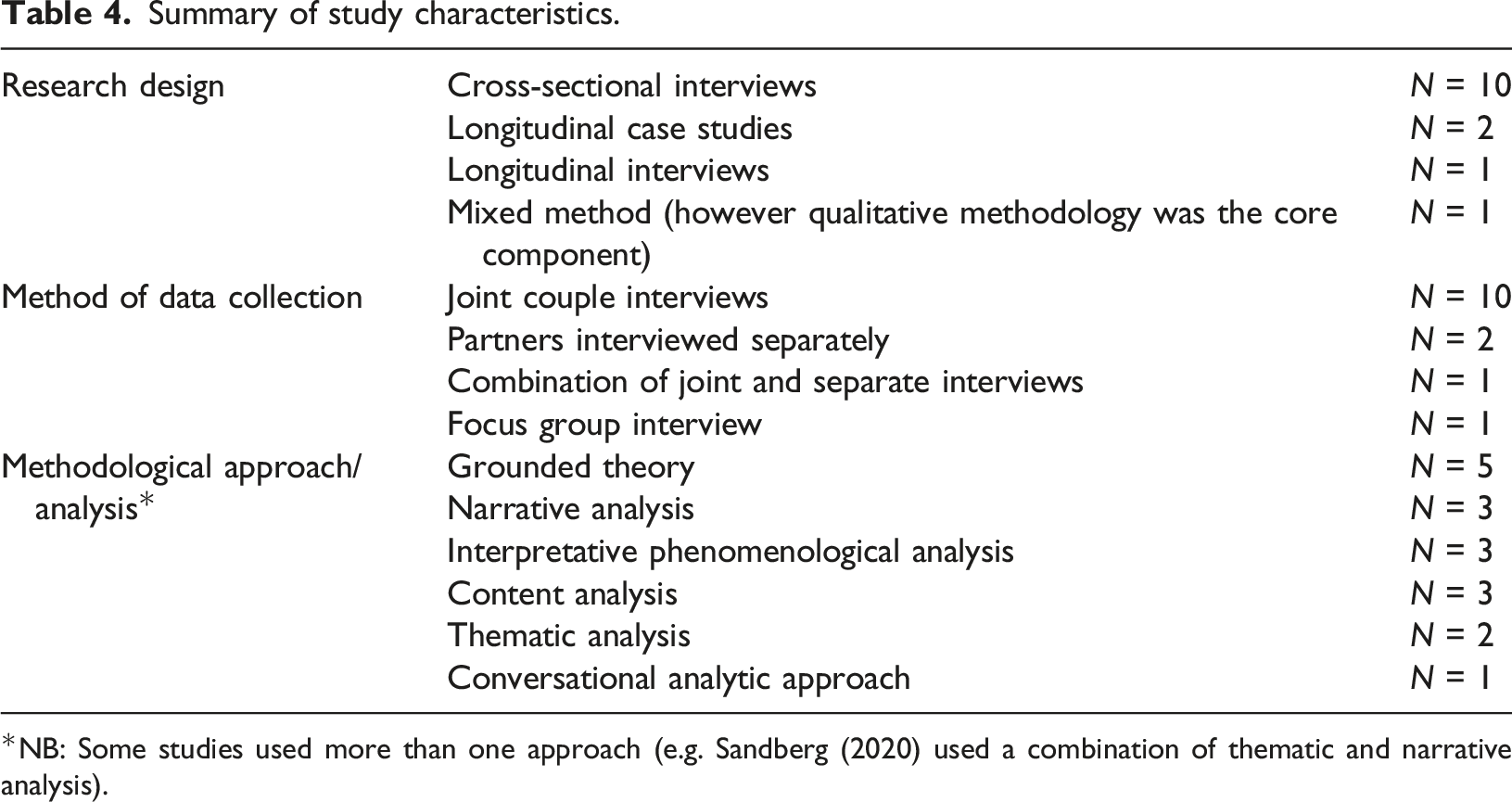
*NB: Some studies used more than one approach (e.g. Sandberg (2020) used a combination of thematic and narrative analysis).
Search strategy 2 – couplehood and multiple health conditions
This search did not find any papers that qualitatively explored the concept of couplehood in couples living with multiple health conditions (see Figure 2: PRISMA flowchart). This search was updated on 09.02.2023, however only one eligible paper was found (Sun et al., 2022: see Supplementary file 6), therefore a meta-ethnographic synthesis was not possible. PRISMA flowchart for Search Strategy 2: Couplehood and multiple health conditions.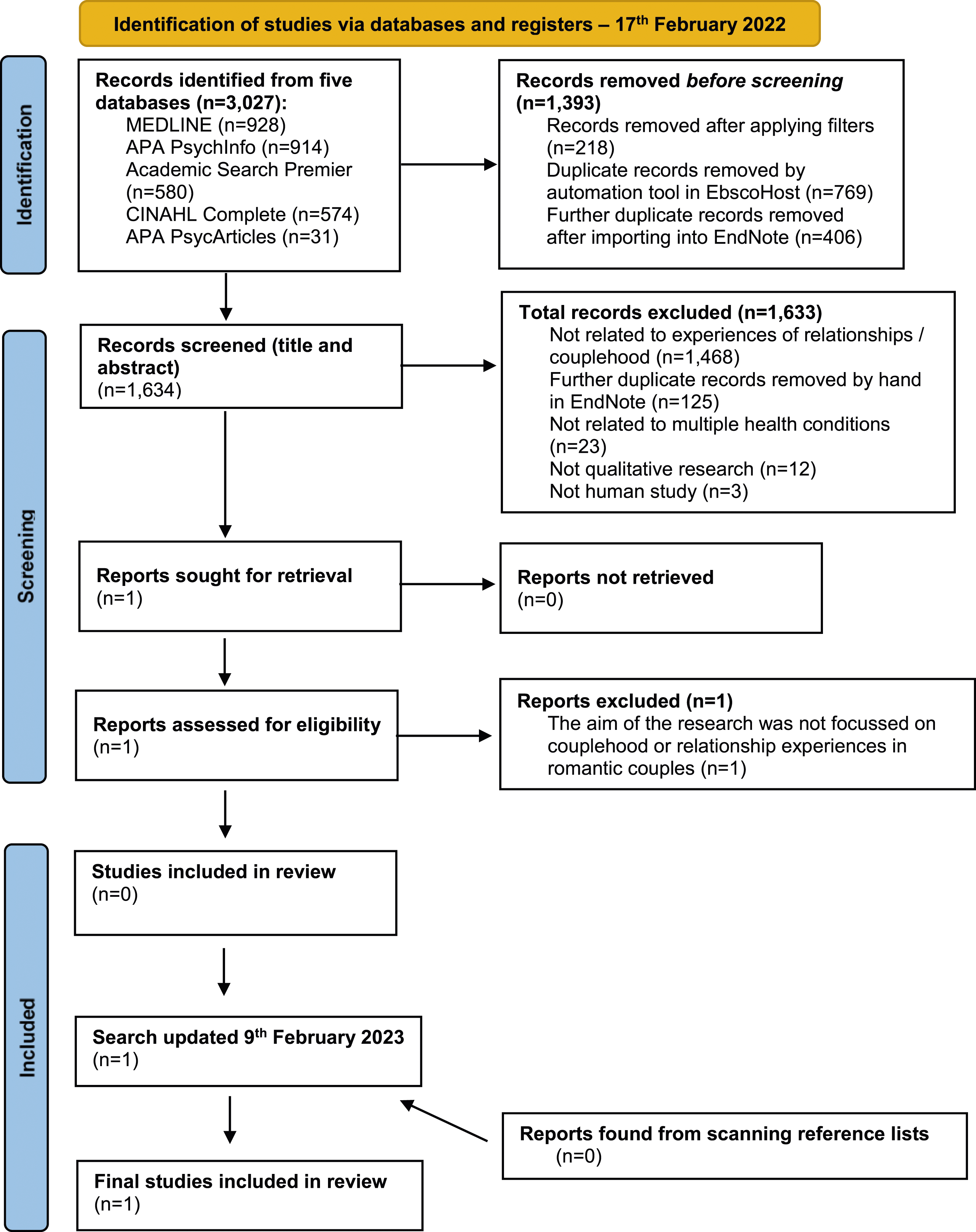
Consequently, the meta-ethnographic synthesis of this review is focussed on the findings from Search Strategy 1 (couplehood and dementia). Particular attention was paid to any quotes, concepts or themes that arose in relation to health when synthesising the findings from the 14 studies included in Search Strategy 1. The syndemic framework of health from Dunn et al. (2022) was used to help identify any factors that are important to consider in relation to health, such as acute and chronic conditions, symptom complexes such as pain, mental health, the health status of spousal carers, lifestyle, social and environmental factors.
Methodological quality
RD appraised the 14 included papers; co-authors EW and AH appraised 50% of the papers as part of a credibility check (Tong et al., 2012). Any disagreements in scores were discussed until consensus was reached. The CASP quality ratings are detailed in Supplementary file 7. Overall, the papers received a generally high appraisal score, with the lowest scoring paper achieving 14/24 (58%). Merrick et al. (2016) scored highest on the CASP and formed the index study from which subsequent studies were then compared.
Synthesis
Reciprocal themes and subthemes across the reviewed papers.
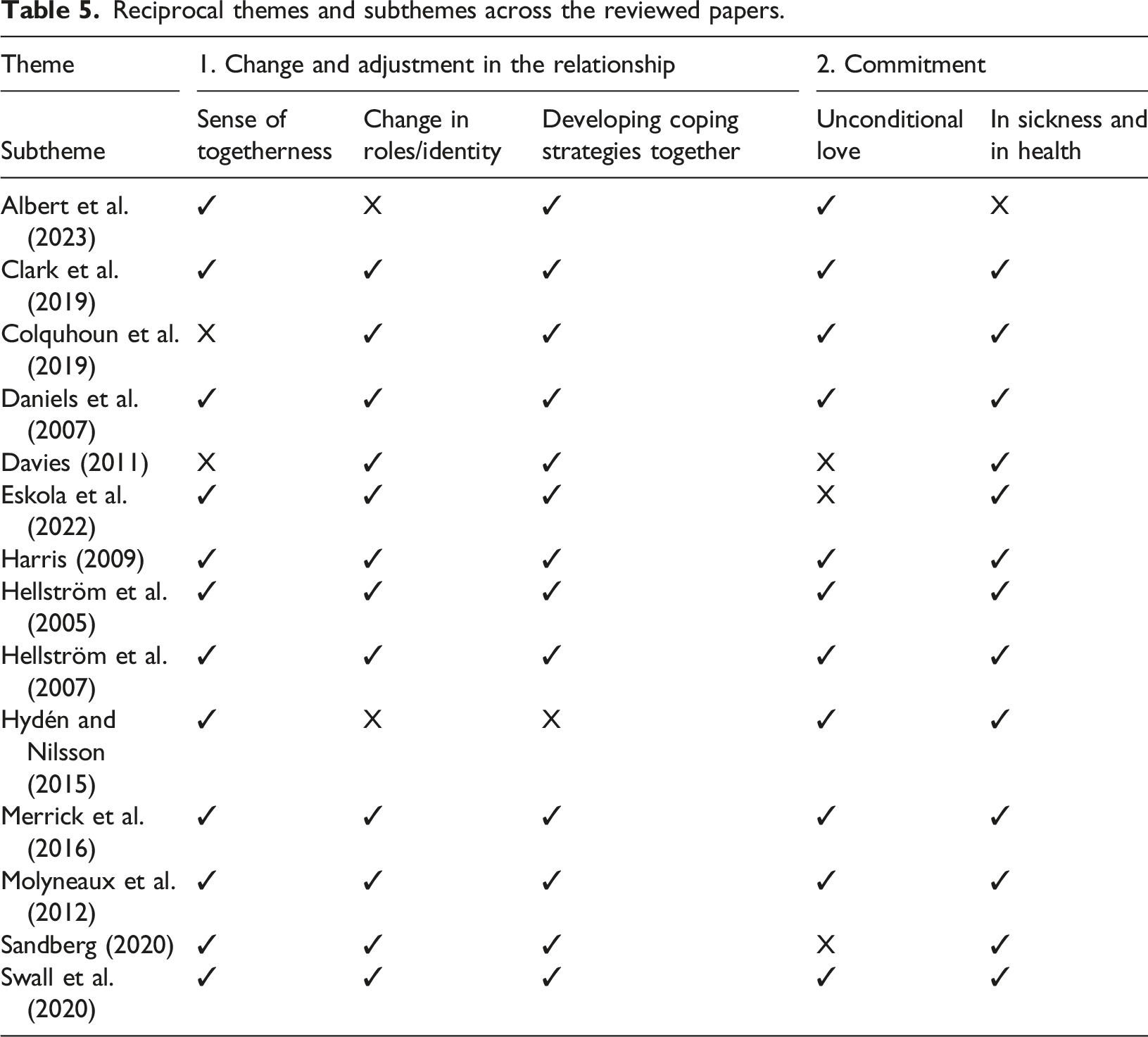
Theme 1: Change and adjustment in the relationship
Subtheme 1.1: Sense of togetherness
There was great divergence among couples as to how close they felt to their partners. For some couples, the partners had lost the feeling of togetherness (becoming an ‘I’) and expressed a sense of sorrow for this loss, for example one partner without dementia said: “About how I miss him, how I miss that closeness of the relationship that you had for all that time. Forty years, over 40 years at the time, you know.” (Clark et al., 2019, p. 1731).
This was particularly evident when a person’s dementia was more advanced. For example, in the extract below a partner expresses her sadness when her partner with dementia is unable to continue a joke or conversation due to his memory loss: “The bit that really gets me down is when we’ve had a bit of a laugh, . . . what gets to me is the fact of something will happen and then we have a laugh over it and then like ten minutes later I try and carry on the joke or conversation and he can’t remember the conversation.” (Merrick et al., 2016, p. 41)
Difficulties in communication as a result of advancing dementia also challenged this partner without dementia’s feelings of closeness: “I really feel like I’m a caregiver taking care of a child a lot of times. The closeness is not there. He doesn’t talk much. Yes, I’d say the intimacy is very low.” Partner without dementia (Harris, 2009, p. 70).
Changes in behaviour, such as verbal or physical aggression, was a strong factor in affecting the closeness within couples’ relationships. This was particularly true for partners without dementia who at times felt frightened by this change in behaviour that had not been experienced before: “This is not a nice situation, but there is nothing you can do about these diseases. But there will be difficulties. And now, when that fist gets swung in front of my face a little too often, it’s starting to get scary.” Partner without dementia (Eskola et al., 2022, p. 7)
For those with dementia, feelings of frustration or pressure could arise when they didn’t understand what their partner was asking of them, leading to a loss of closeness (Swall et al., 2020). Conflict could also occur when there was a mismatch within couples’ feelings of closeness or togetherness, for example, the following husband with dementia missed the closeness of his relationship with his wife, who had no interest in rekindling it: “I felt that I was in need of it really, well just closeness you know. . . she didn’t seem to be very interested at all.” (Clark et al., 2019, p. 1731).
Additionally, some couples felt an ‘enforced sense of togetherness’, where they longed for time to themselves or to pursue their own separate hobbies or interests (Eskola et al., 2022; Molyneaux et al., 2012). For example, some partners without dementia felt they could not leave their partner on their own, and some partners with dementia were aware of this and subsequently felt like a burden.
However, many couples still felt a strong sense of togetherness or closeness that was unchanged following a dementia diagnosis. As one partner without dementia said: “It is WE that is going through this. It isn’t him-me.” (Merrick et al., 2016, p. 39). Efforts to maintain this sense of closeness and to continue as normal was important to the following partner with dementia: “The main thing is to try to understand the relationship. Togetherness is the main thing…thinking, talking and having activities together. Togetherness [however it is expressed] means a whole lot.” (Harris, 2009, p. 74)
For some couples, their sense of closeness was strengthened through their experience of dementia: “Well we’ve always been very close, so it’s not a big change . . . I think we’ve become closer.” Partner without dementia (Merrick et al., 2016, p. 41) and a diagnosis of dementia was not going to change that: “I think the intimacy, the closeness of the relationship, probably even takes on more importance now because that IS here. And they can’t take that away from you.” Partner with dementia (Harris, 2009, p. 72).
The loss of a physical sexual relationship was reported by some couples. However other forms of intimacy and affection, such as cuddling, kissing and ‘just being together’ came to be more important: “Ah…yes, BUT [emphasizing]…we are sexually distant, but we are still loving. It’s very interesting, sexuality has decreased, but as it decreases, other things increase, affection, being together.” Partner with dementia (Albert et al., 2023, p. 396)
Subtheme 1.2: Change in roles and identity
Following the onset of dementia, partners (with and without dementia) experienced changes in their role and identity, which impacted on their perceived couple identity and couplehood. For some partners without dementia, they felt their identity changed from being that of a husband, wife or partner, to that of a parent (Harris, 2009) or carer:
“I’m not getting any younger myself you know, at 79 I’m suddenly 24 hours on the job, a carer and not being looked after myself, apart from my family who do. But it’s almost, just as if the roles have completely switched.” (Clark et al., 2019, p. 1732)
These changes could make some partners without dementia feel vulnerable, especially if they were older themselves: “I used to feel quite secure. But I don’t any more. And I’m 80 you see, I’m getting on and sometimes I feel when things crop up, difficulties, problems, I just can’t cope.” (Merrick et al., 2016, p. 40)
Equally partners with dementia felt a great sense of loss and grief in losing their abilities and independence: “She’s [his wife] busy; she’s got things to do. She’ll get [t]ouchy at times and I understand why. She’s carrying the major load. The responsibilities used to be mine. The biggest things that I miss are the fact that I was able to.” Partner with dementia (Harris, 2009, p. 67)
As seen from the extract above, some partners with dementia were aware of the increased responsibilities their partner had to take on and the increased pressure on them. This led to feelings of guilt: “I worry about (wife’s name). I hope she forgives me, she would be better off without me at times, I think.” Partner with dementia (Clark et al., 2019, p. 1734)
However, many partners without dementia would try to keep their partner feeling ‘involved’ by sharing tasks and responsibilities in order to try and preserve personhood (Hellström et al., 2007). Often, help and support was carried out by partners without dementia in an implicit, subtle way, to help preserve their partner’s dignity and sense of self (Hellström et al., 2005).
Rebalancing roles and responsibilities were part of the ongoing reciprocity in couples’ relationships or marriages. For example, the following partner without dementia wanted to repay his wife with dementia for all the help and support she had given him over the years:
“Whether we want to admit it or not, at least in my case, my wife did everything for me. I could say to her, “I’ve got a taste for ribs.” And I come home and there are ribs on the table. Or I say, “I got to cut the grass before we go out.” And I come home to grass that’s been cut. She did that for 40 years, and for the last 6 or 7, it was my turn. It wasn’t really all that difficult. It was difficult, but what I mean, it was a joy for me to take care of her.” (Harris, 2009, p. 71).
Subtheme 1.3: Developing coping strategies together
In response to these changes in role and identity within the relationship, couples used a range of strategies to help them cope with the challenges that dementia presented, both individually and together as a couple.
There were differences in couples’ ability or choice to integrate and accept dementia as part of their lives. Some partners struggled to accept this diagnosis, and denied that they had dementia (Clark et al., 2019) potentially as a protective coping strategy. Others accepted the diagnosis but distanced themselves from the idea by actively avoiding information about it (Hellström et al., 2007), choosing not to think about it (Colquhoun et al., 2019), or talk about it (Albert et al., 2023):
“My wife and I don’t talk about it either. As we feel that the milieu is shaped by this, but I am pleased and satisfied that it is like it is. The disease is on another plane, it doesn’t have to affect others.”
Partner with dementia (Hellström et al., 2007, p. 396)
Additionally, some chose to distance themselves from dementia by instead focussing on other roles that they identify with, such as being a parent or church volunteer (Colquhoun et al., 2019). Some couples used externalising language in order to blame dementia for any difficulties, rather than each other: “I know it’s not her; it’s that monster [the disease].” Partner without dementia (Harris, 2009, p. 72). In this way, the above strategies ‘push’ dementia into the background, in order to avoid the emotions that may come from a dementia diagnosis, and to preserve a more positive outlook in an effort to maintain their couplehood as it were before.
In contrast, some couples integrated and accepted dementia, although this was still difficult to accept: “I think it’s difficult for me to accept the fact that I don’t have the err . . . the facilities I had before. I mean I don’t find life as easy . . . And that annoys me in one way and I accept it in another . . . The fact is I have to make allowances for it.” Person with dementia (Merrick et al., 2016, p. 42)
The acceptance and integration of dementia was evidenced by a number of strategies that couples used together in order to adapt and cope with the diagnosis. Some couples sought help from family, friends and support groups, which provided couples with practical, social and emotional support: “The groups we go to, we’ve become good friends with everybody there. The honesty about having to talk about how angry you are, how sad you are. Maybe it’s about how you deal with it. And guess what? We don’t always deal with it. But, what are you going to do? There’s been times when I’ve been so upset and I talk about it at the Association [support groups].” Partner without dementia (Harris, 2009, p. 72)
Some couples chose to learn more about dementia, with the idea that ‘being forewarned is forearmed’ (Clark et al., 2019, p. 1735) and partners without dementia in particular learnt new skills to cope with adjusting to caring for their partner with dementia: “You reprogram and learn. You learn things that you never thought you’d have to, like makeup”. (Harris, 2009, p. 68).
The onset of dementia appeared to force couples to re-evaluate their lives and the time they had left with each other. For example, couples appeared to have a newfound appreciation for the smaller things in life: “I have learned to relish everything we can do together. It’s just a matter from taking all you can from life. But the good things don’t have to be the silver lining. They don’t have to be the big things. Not any more. Just give me a little bit of cream on the day.” Partner without dementia (Harris, 2009, p. 71)
Additionally, some couples elected to look for the positives in life, rather than focussing on the negative aspects of dementia: “Well, I try to think about the things that are a little brighter, on the bright side, than to think about all the bad stuff, you know. You just can’t dwell on it or it will run your life.” Partner without dementia (Daniels et al., 2007, p. 168).
Living in the moment, rather than dwelling on the past or worrying about the future, appeared to be another strategy couples use when living with dementia: “I don’t want to look forward, but to live today. It is much nicer.” Partner with dementia (Hellström et al., 2007, p. 397).
Other coping strategies include the use of humour: “I just think, well . . . laugh it off . . . I can laugh at anything and anybody. I think that’s my saviour actually . . .” Partner with dementia (Merrick et al., 2016, p. 42) and a sense of stoicism, as stated from the following partner with dementia: “Get on with it. Don’t let the bastards drag you down. You have to put up with it haven’t you and you have got to fight it.” (Clark et al., 2019, p. 1734).
Some couples reminisced on the good times shared together, possibly as a way to help give meaning and make sense of the situation. Upon reflection of their lives, couples reinforced their connection to each other and promoted their shared sense of couple identity:
Mrs Grant (Partner without dementia): “When we bought this place after we married, we worked on it together; we wallpapered the walls together, we did the garden together.
Mr Grant: I put a bathroom in.
Mrs Grant (smiling): He put a bathroom in. We did it all together.” (Colquhoun et al., 2019, p. 2167)
Some partners without dementia used strategies to try and ‘keep the peace’ and avoid conflict that may arise from difficulties experienced from the partner with dementia, for example by avoiding things that might trigger a negative reaction, the use of distraction and simply not reacting at all (Hellström et al., 2007). Additionally, some partners minimized their own struggles so that their partner did not worry: “Well, really I think that sometimes he gets a bit worried and if he gets worried about things I’ll say ‘‘yeah that’s fine, fine’’, just so that he doesn’t worry about me so much.” Partner with dementia (Merrick et al., 2016, p. 45).
The final coping strategy identified was how couples normalised some of the symptoms of dementia, such as memory loss, and conceptualised dementia as part of the normal ageing process. In the following extract, this couple attribute the partner with dementia’s forgetfulness as an aspect of his personality before he had dementia and as a normal thing to do:
“Denise (partner without dementia): But you had, must admit you were a, a bit, you’d forget something wouldn’t you before love. You always lost your keys. You always lose your keys, you can’t find them.
Peter: Oh round the house?
Denise: Yeah.
Peter: Oh well that, that’s natural that Denise.”
(Molyneaux et al., 2012, p. 493)
Some partners normalised memory loss by comparing their partner with dementia’s forgetfulness to their own, stating that their partner with dementia can often remind them about things (Molyneaux et al., 2012). Furthermore, some couples felt that their relationship had not changed as a result of dementia (Albert et al., 2023; Sandberg, 2020) but rather as a result of getting older:
“…what you're saying really is, that our relationship has changed as we've aged or grown old together or put in a happy way, or as we go on life changes, and we've changed with it. Now our relationship to each other has changed.”
Partner without dementia (Swall et al., 2020, p. 6)
Theme 2: Commitment
Subtheme 2.1: Unconditional love
Eleven studies evidenced that couples continued to express love and affection to each other regardless of a dementia diagnosis, which helped to sustain their sense of couplehood: “The most important thing ... is the love between us. I worship Betty and I know she worships me.” Partner with dementia (Merrick et al., 2016, p. 39)
Love and affection were often shown in the nonverbal communication, for example in the extract below, the wife with dementia takes her husband’s hand as she talks about their relationship, and the husband responds by clicking his tongue to acknowledge his wife’s compliment:
Wife with dementia: “and we’ve been together ever since (looks at her husband) and we have our own children who also have their own children and well, I like it with my Lennie. (takes her husband´s hand and shakes it)
Husband: (clicks his tongue) well there you hear (laughs and nods at the interviewers)
Wife with dementia: he is so sweet
Interviewer: yes
Husband: well we’re lucky, love still blossoms for us”
(Hydén & Nilsson, 2015, p. 724)
This shows how love is reciprocated. Couples believed that even when dementia reached the more advanced stages or if their partner had to go into residential care, the love between them would not change: “You can’t dump somebody off that loves you like that and forget about them, like a lot of people do, you know, put them in homes. That’s something I don’t ever intend to do as long as I am able to take care of her.” Partner without dementia (Daniels et al., 2007, pp. 169–170).
Subtheme 2.2: In sickness and in health
The majority of studies revealed that couples demonstrate a strong sense of commitment to one another. There was a sense of loyalty and duty to each other, particularly evidenced by partners without dementia, and this was often reinforced by their perceived sanctity of marriage and the vows they made to each other: “You become not just a role player; you go back to these vows you took. How you were standing up and how they tell, from death do us part, united for better or for worse. I always felt that she would give her heart and soul to do the same for me. It was never a question in my mind about what I had to do.” Partner without dementia (Harris, 2009, p. 71).
Additionally, a deep emotional attachment developed over the course of the marriage or relationship appeared to be a strong protective factor in maintaining a sense of shared identity, security and commitment to one and other:
“Mr Dunbar: I know it must be difficult for (my wife) to look after me, it must be, I’m not the most patient in the world, far from it, I know my faults and then I say things and after I think ‘oh you’re a sod, you shouldn’t have said that and so forth’
Mrs Dunbar (taking her husband’s hand): And we are always there for each other whatever happens
Mr Dunbar: Yes you’re always there for me
Mrs Dunbar: And you’re always there for me
Mr Dunbar: Yeah but not so good as I used to be is it?
Mrs Dunbar: But you’re always there for me
Mr Dunbar: I know love, yes
Mrs Dunbar: There for each other”
(Colquhoun et al., 2019, p. 2165)
The above extract shows how Mrs Dunbar (partner without dementia) changes the subject when Mr Dunbar voices his concerns about it being difficult for his wife to look after him, by reassuring him that they are always there for each other, rather than acknowledging the difficulties. In doing so, Mrs Dunbar preserves their sense of shared couplehood and identity, and reinforces their commitment to each other.
There was one exception to this, where a carer from Eskola et al. (2022) reports that she considered divorce due to her husband’s aggressive verbal behaviour. However, as her husband’s dementia had advanced, she felt it was too late to make that decision and felt responsible for his care and wellbeing.
Couplehood, dementia and multiple health conditions
No reciprocal themes were identified in relation to couples’ experiences of living with other health conditions alongside dementia and its impact (if any) on their couplehood. However, any first or second order data relating to health were purposely sought. Two areas of interest in relation to health were identified, however they usually appeared within the qualitative data serendipitously, rather than as a result of direct questioning. The first was the impact of dementia on couples’ emotional health and wellbeing, and how this may impact on their couplehood. Ten papers contained small snippets of data in relation to the psychological impact that dementia can have on couples (Colquhoun et al., 2019; Daniels et al., 2007; Davies, 2011; Eskola et al., 2022; Harris, 2009; Hellström et al., 2007; Merrick et al., 2016; Molyneaux et al., 2012; Sandberg, 2020; Swall et al., 2020) however they did not feature prominently as a theme or concept. An example of this can be seen from the following extract from a partner without dementia: “(my husband is) absolutely devastated and more and more depressed and every morning he says he doesn’t want to go on because of this (having dementia)… every morning he says that which is very upsetting for me and I still go to my (activities) but lots of mornings I don’t want to go and I’m crying all the way.” (Colquhoun et al., 2019, p. 2167)
One paper featured emotional distress from dementia more prominently (Clark et al., 2019) and has a subtheme entitled ‘The emotional impact (difficult to cope with)’. This subtheme describes how all of the couples in the study described a ‘rollercoaster of emotions’ such as sorrow, worry and frustration, and how life ‘had been cut short’ due to dementia. It is worth noting that partners were interviewed separately in this study, whereas the majority of the other studies interviewed couples together. It is possible therefore that partners may have felt more able to speak freely without fear of upsetting their partner.
The second area of interest was how the presence of other physical health conditions, in both partners with and without dementia, was reported to be the cause in changes or a loss of a physical sexual relationship, as opposed to dementia. This appeared in two papers (Harris, 2009; Sandberg, 2020), however both of these papers were focussed on sexuality and intimacy and only Harris (2009) contained quotes (first order data) from couples reporting this: “He is very interested in sex. But, because of his heart problems, he takes a lot of medicine for his heart every day; his heart is very weak. It’s not anywhere like it once was. He thinks about it, but he is just too tired. It’s difficult.” Partner without dementia (Harris, 2009, pp. 69–69)
Harris (2009) states that “it is important to note that for some couples because of other healthcare issues, such as diabetes, heart conditions, or prostrate problems, their level of sexual activity had already dropped, previous to the dementia diagnosis. Thus, dementia was not the cause, but it added to the change.” (Harris, 2009, p. 68). Similarly, Sandberg (2020) reports that: “Participants also discussed health and medical conditions, such as prostate or penile cancer and heart problems, as causing erectile problems for men, which brought about changes in their sexual relationships.” (Sandberg, 2020, p. 8, p. 8). It is unclear how, or if, the presence of other physical health conditions alongside dementia has an impact on a couple’s relationship or sense of couplehood in any other ways (other than changes in sexuality). Only one paper (Eskola et al., 2022) described the spousal carer’s accounts of caring for their partner with dementia in relation to other physical health problems, such as catheterisation or managing incontinence. These spousal carers began to identify as a ‘nursing professional’ which impacted on both physical and emotional intimacy.
Discussion
A significant finding from this review is how couples living with dementia continued to demonstrate mutual feelings of love, respect and intimacy toward each other, which enhanced their level of commitment and sense of couplehood. Even when a partner’s dementia had progressed, and other aspects of the relationship were affected, love endured for both partners. All human beings are motivated to experience a sense of love and belonging (Maslow, 1943). Indeed, Kitwood (1997) identified love as a central psychological need for people living with dementia. However, the concept of love has been largely ignored in the context of couples living with dementia and emerges serendipitously in the literature, rather than studied directly (see Baikie, 2002; Boylstein & Hayes, 2012; Evans & Lee, 2014; Kaplan, 2001; Wadham et al., 2016). This review found that couples living with dementia drew upon a capital of love, accumulated over many years of the relationship, and this was an important aspect to sustaining their couplehood. Love was reciprocated through expressions of both verbal and non-verbal communication and behaviour, and dementia severity did not appear to impact on the shared experience of love. This is an important finding, as it has been argued that love is a ‘character strength’ (Peterson & Seligman, 2004) that can be cultivated to improve psychological wellbeing. Further research is needed to understand how love can be capitalised through relationship-centred interventions to help support couples whose relationship feels threatened following the onset of dementia.
There was a significant emphasis on couples’ devotion to their marriage vows and to the sanctity of marriage. A sense of duty to provide care and support to their partner with dementia ‘in sickness and in health’ was felt particularly strongly among partners without dementia, and evidenced a show of commitment to the relationship. The importance of marriage and wedding vows may be linked to how couples reflect about their present experiences in the context of their past life history as a couple. The majority of couples in this review reported to have had positive, happy marriages or relationships, however it is not clear from the synthesis how (or if) this is linked to their present experiences of dementia and couplehood. Further research is needed to understand couples’ collective accounts of their relationship history and how this may impact on their couplehood following the onset of dementia.
This review found that although love remained (regardless of dementia severity) couples experienced a lost ‘sense of togetherness’ and reciprocity as dementia progressed. It appears that as the partner with dementia’s cognition declines in areas such as communication, memory and understanding, the more likely it is that couples experience a loss of emotional closeness which subsequently impacts on their couplehood. This loss of emotional closeness and reciprocity may trigger ‘anticipatory grief’ in partners without dementia (Dementia UK, 2023). In contrast, couples from this review who experienced milder symptoms or were in the earlier stages of dementia continued to maintain a strong sense of togetherness, and in some cases their perception of couplehood was strengthened following the onset of dementia. This is in line with other research that has also found closeness to increase following the onset of dementia (De Vugt et al., 2003). It is possible that the onset of a life-limiting condition such as dementia may cause couples to re-evaluate their life together, which may in turn lead to feelings of increased closeness in the relationship.
In contrast to a previous qualitative review on dementia and couplehood (Wadham et al., 2016), this review found that a ‘sense of togetherness’ was interpreted as a separate concept to commitment. Relationship ‘togetherness’ or ‘closeness’ has been defined as ‘the quality of the emotional bond between the caregiver and care recipient’ (Fauth et al., 2012, p. 2). Although there may be overlap between commitment and a sense of togetherness, it is important to recognise these differences. For example, a couple may continue to feel committed to each other through their love and devotion to marriage vows, but experience a loss of emotional connection or togetherness due to the progression of dementia. Distinguishing between these concepts is important in order to tailor relationship-centred interventions that are appropriate to couples’ experiences and needs and improve therapeutic outcomes.
Couples varied in their experiences of how they adjusted to changes in their role and identity following the onset of dementia. Much research has explored the impact of dementia on identity at an individual level for both the person with dementia (Sabat & Harré, 1992) and the carer (Hayes et al., 2009), however less is known about how it impacts a couple’s shared identity and further research is needed to explore this. Nevertheless, this review found that some couples rebalanced roles and responsibilities by developing coping strategies together to help sustain their couplehood and shared couple identity. It is important that future dyadic interventions consider both individual and shared couple-based strategies, in order to help sustain their sense of couplehood.
Dementia, multiple health conditions and couplehood
An additional search for qualitative data on couples’ experiences of other health issues in the reviewed papers revealed two tentative findings. Firstly, dementia impacted on couples’ emotional health and wellbeing which in turn impacted on their couplehood. Psychological distress is a very common experience for people following a diagnosis of dementia (Lai et al., 2018; Regan, 2016). Yet there are significant disparities of care for people living with both dementia and mental health conditions. There is a long-standing issue of Cartesian dualism (Mehta, 2011) in mental and physical healthcare services, where the mind and body are considered as separate entities, and the biomedical model continues to dominate. These views have led to a single-disease focus in health and social care and consequently, people who live with multiple health conditions receive fragmented care (Das et al., 2016; Naylor et al., 2016; Salisbury, 2012). This is particularly problematic for people with dementia because many symptoms of dementia overlap with other physical and mental health conditions, and therefore are often under- or mis-diagnosed due to diagnostic overshadowing (Clarke & Mantle, 2016). Earlier detection and treatment of underlying physical and mental health conditions may help to improve quality of life and physical functioning for people with dementia (Bunn et al., 2015). Additionally, stress and mental health problems are commonly experienced by those caring for someone with dementia (Karg et al., 2018; Stall et al., 2019). However, less is known about how mental health problems in addition to dementia impacts on couplehood from a couple’s shared perspective. Further research is needed to explore couples’ shared experiences of mental health and in how to support the couple holistically in order to maintain their quality of life and couplehood.
Secondly, couples who reported to have lost a physical sexual relationship attributed this to the onset of other physical health problems, such as erectile dysfunction or prostate cancer (Harris, 2009; Sandberg, 2020). This often occurred prior to the onset of dementia, therefore dementia was not considered as the cause but potentially ‘added to the change’ (Harris, 2009, p. 68) although it is unclear how. Additionally, couples often normalised this as part of the ageing process. Other forms of intimacy, such as touching, kissing and hugging became more important. Similar findings have also been reported from research studies that have explored sexuality and intimacy in couples living with dementia (Davies et al., 2010; Kuppuswamy et al., 2007), however this is often from spousal carers perspectives. These findings appeared in the reviewed papers serendipitously, and only two papers discussed other health issues in relation to sexuality and intimacy (Harris, 2009; Sandberg, 2020) therefore the findings need to be taken with caution. Nevertheless, the findings provide some indication that emotional and physical health problems in addition to dementia may impact couplehood for some couples living with dementia, and other reviews on couplehood and dementia have not explored this (Evans & Lee, 2014; Wadham et al., 2016).
Figure 3 below is an illustration of the reviewer’s interpretations and how these themes could be connected. Further research is needed to explore how the presence of multiple other health conditions and relationship history may impact on couplehood for couples living with dementia. Often support is targeted to individual conditions, and tailored individually either to the person with dementia or the carer. However, in reality dementia is a journey often shared as a couple, where dementia is usually not the only condition experienced. Qualitative research exploring couples’ shared experiences where both partners are living with multiple health conditions, and one partner is living with dementia, is needed in order to inform future research and relationship-centred interventions. A balancing act of couplehood. *It appears that all of the couples in this review were hetrosexual, therefore a man and woman are depictec in this illustration. However, only four of the fourteen reviewed papers explicitly state couples’ hetrosexual orientation (Albert et al., 2023; Eskola et al., 2022; Merrick et al., 2016; Sandberg, 2020). Therefore, this assumption is based from descriptions of gender, male/female assigned pseudonyms and husband-wife participant charcteristics. The author acknowledges there are many types of couples with different sexualities, and this should be explored (and explicitly reported) in future research.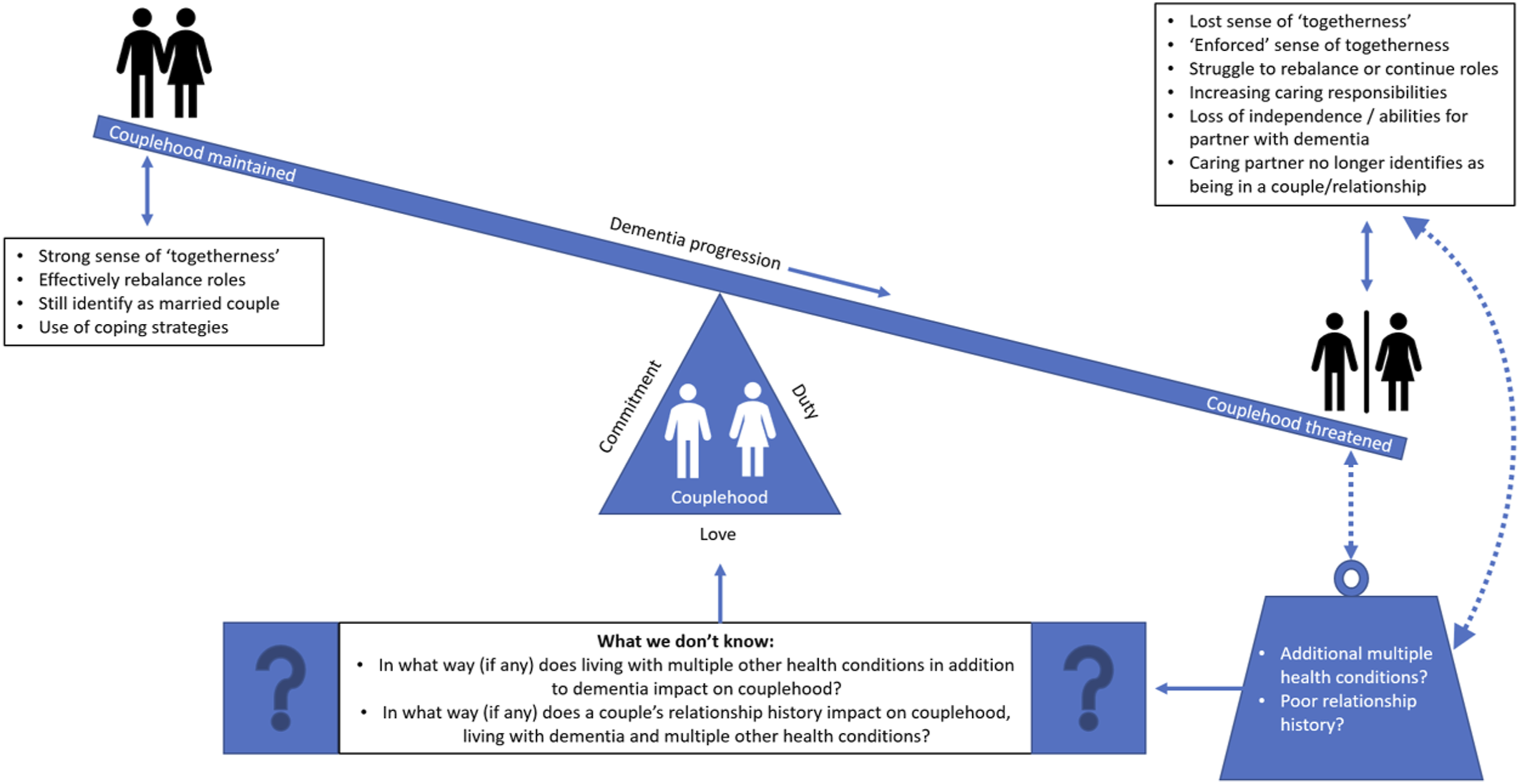
Reflexivity statement
RD engaged in a number of reflexive practices in order to set aside pre-conceived ideas, assumptions or experiences that could influence the interpretation of the data (Fischer, 2009). Firstly, RD read and re-read each paper repeatedly and grounded the interpretations made during data synthesis using participant’s verbatim quotes. Secondly, in line with the interpretative nature of meta-synthesis, RD engaged in a hermeneutic circle with the data, going backwards and forwards from the part to the whole (Smith et al., 2022). The interpretations were therefore developed in an iterative, and non-linear fashion. Thirdly, RD consulted with the co-authors at each stage of the review, from discussing the inclusion of papers during the literature search stage, appraising the quality of papers using the (CASP, 2018) tool, through to the development of themes and subthemes. Engaging with the co-authors provided the opportunity to openly discuss and debate concepts, uncertainties and disagreements in the data, thereby enhancing the credibility of the data synthesis and overall conduct of the review.
Limitations and future research
Most couples were of white ethnicity, reported positive relationship histories, and were heterosexual, therefore the findings may not represent couples’ views from these demographics. Further research is needed to understand the experiences of couples from other ethnic backgrounds and cultures, couples who report a difficult relationship history and same-sex couples. In addition, the majority of couples from this review were interviewed together, therefore a potential limitation may be whether partners felt they could be completely honest about their views and experiences in front of their partner in the interview.
Future research could also explore the experiences of couples who are not married, or have been divorced and remarried and have experienced shorter relationships. The accounts from this review are couples who were born mostly between the 1920s to 1960s. Couples born in this generation often married at a young age and the sanctity of marriage was held in a much higher regard. Societal norms around marriage today are changing; it is more common now to get married later in life, or not at all. Additionally, more people than ever are divorcing (Ortiz-Ospina & Roser, 2020). Therefore, the findings from the current review may not reflect the experiences of the future generations of couples. For example, a strong finding from this review were couples’ commitment to marriage vows, and how they reflected on their long relationship history together, which helped to reaffirm their shared couple identity and provide meaning to their current situation. Future research may opt to research the concept of coupledom, rather than couplehood, which is defined as ‘the state of living as a couple, especially when regarded as being interested in each other to the exclusion of the outside world’ (Collins English Dictionary, 2023). This concept does not include marriage and may be more relevant to some future couples.
Finally, only one paper was retrieved on couples’ experiences of living with multiple health conditions and couplehood (Sun et al., 2022), despite a thorough and extensive search, and none were found for those living with dementia. Therefore, it was not possible to answer the review question in full. However, this points towards a lack of research conducted in this area.
Conclusion
To the author’s knowledge, this is the first qualitative evidence review that has sought to understand couples’ experiences of dementia, multiple health conditions and couplehood. This review found that couplehood was threatened when dementia symptoms progressed and couples experienced feelings of loss of independence and identity. However, a strong foundation of commitment, love and loyalty to each other developed over the course of the relationship, was the ‘glue’ that helped couples face dementia together. However, further research is needed to explore couples’ experiences of living with both multiple health conditions and dementia in relation to their perception of couplehood in order to develop holistic, relationship-centred interventions.
Supplemental Material
Supplemental Material - Exploring the interplay between dementia, multiple health conditions and couplehood: A qualitative evidence review and meta-ethnography
Supplemental Material for Exploring the interplay between dementia, multiple health conditions and couplehood: A qualitative evidence review and meta-ethnography by Rosie Dunn, Emma Wolverson, and Andrea Hilton Ballard in Dementia
Footnotes
Acknowledgements
We would like to thank Fiona Ware, Information Specialist (University of Hull), for her advice on the literature searches.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Dr.
Dr.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.