
Abstract
Data from the Vietnamese Aging and Care Survey (VACS) showed the high prevalence of disability, depressive symptoms, and cognitive impairment in older Vietnamese immigrants and refugees. We proposed a Community-Engaged Dementia Education Program to examine the Houston Vietnamese American community’s literacy on dementia and develop a one-pager educational material. This is a cross-sectional, qualitative study (interviews and focus groups) using the Cultural Exchange Model as a conceptual framework. We interviewed fourteen Vietnamese key informants and assessed the community’s knowledge of dementia based on Edwards’ 9-stage Community Readiness Model. The community’s low literacy on dementia (Stages 2–3: Denial/resistance to vague awareness) was revealed. Approaches to introducing dementia conversations to the community and what to include in the one-pager were discussed. Based on the key informants’ insight, we developed a dementia one-pager tailored to the community by using lay language with a representative image of the target population, indicating warning signs of dementia, and encouraging them to see their doctors for cognitive check-ups. The plan for the next steps includes utilizing the local ethnic media, collaborating with the existing pillars of the Cultural Exchange model, leveraging the university students’ learning opportunities, and disseminating the culturally and linguistically tailored one-pager.
Introduction
Until the South Vietnamese government collapsed its position in 1975, there were hardly any Vietnamese people living in the United States (U.S.). However, following the fall of Saigon, three distinct waves of Vietnamese refugees arrived in many U.S. cities. The first wave of 125,000 refugees consisted of the U.S. military or the South Vietnamese government families who were educated professionals (Rkasnuam & Batalova, 2014). The second wave of 280,500 refugees arrived between 1977 and the mid-1980s. The majority were farmers or fishermen with limited skills and low education, known as “boat people” because they fled by boat (Klineberg & Wu, 2013; Rkasnuam & Batalova, 2014). The third wave of 532,000 refugees arrived throughout the 1980s and 1990s primarily to unite with their relatives who were in the U.S. already (Pyke, 2000). Many were children of U.S. servicemen and their mothers, or political prisoners (Alperin & Batalova, 2018; Klineberg & Wu, 2013). The Vietnamese population grew from 988,000 to 1,241,000 between 2000 and 2010. Currently, it is estimated to be 2.2 million and still growing (Alperin & Batalova, 2018). They are the fourth largest foreign-born Asians (68% foreign-born) after India, the Philippines, and China. However, compared to well-established Asian immigrants such as Chinese and Japanese, they are more recent immigrants consisting of first and second generations (Ta Park et al., 2018).
Vietnamese Americans possess unique migration characteristics from other Asian Americans. While they are a recent immigrant group, they came to the U.S. with adverse conditions such as having experienced extensive and long war-time traumas, tough migration journeys with possible physical injuries, as well as loss and separation from family members (Alperin & Batalova, 2018; Rkasnuam & Batalova, 2014). Upon arrival in the U.S., they experienced low socioeconomic status, low English language proficiency, cultural and lifestyle changes, and loss of their professional status, all of which predispose them to a higher risk of poor physical, mental, and cognitive health (Gold, 1992). Despite the growing population and the high risk of adverse health, the health data on this vulnerable population, especially Vietnamese older adults is scarce (Kim et al., 2010; Meyer et al., 2015; Torr & Walsh, 2018) and covers limited domains of health such as mobility and depressive symptoms only (Fu & VanLandingham, 2012; Leung et al., 2010).
To fill this knowledge gap, we developed the Vietnamese Aging and Care Survey (VACS) and collected health data on community-dwelling older Vietnamese (≥65 years) and their family caregivers (≥18 years) in 2018 (VACS 1: N = 199) and 2021 (VACS 2: N = 204) in Houston, Texas. Houston is the second largest Vietnamese-populated metropolitan area in the nation with 143,000 Vietnamese living in ethnic enclaves (Pew Research Center, 2021). The VACS is a cross-sectional, comprehensive health survey, modeled after the Hispanic Established Population for Epidemiological Studies of the Elderly (Markides et al., 2016). The surveys assess the biopsychosocial aspects of an individual’s health including Asian cultural context (e.g., filial expectation, religiosity) written in Vietnamese and English.
Limited literature and the VACS studies have found that older Vietnamese suffer from a high prevalence of physical disability and mental health challenges (depressive symptoms and loneliness) (Fuller-Thomson et al., 2011; Miyawaki et al., 2020a, 2020b, 2022a, 2022b). Moreover, the VACS 2 data revealed that 82% and 40% of Vietnamese older adults had mild cognitive impairment and dementia respectively measured by the Vietnamese versions of the Mini-Mental State Examination (Folstein et al., 1975) and Montreal Cognitive Assessment (Do et al., 2022; Nasreddine et al., 2005), but hardly any caregivers took their loved ones to a doctor’s office for a cognitive assessment. Vietnamese adult children practice filial caregiving as it is their tradition (Yeo et al., 2002). They tend to believe that memory problems are part of the aging process and that memory loss in old age is normal revealing their low literacy on Alzheimer’s disease and related dementias (Lee & Casado, 2019; Meyer et al., 2015; Ta Park et al., 2018) as having Alzheimer’s disease and related dementias is not a normal part of aging and it interrupts people’s daily lives (Centers for Disease Control and Prevention, 2023). In addition, memory loss is highly stigmatized and caregivers may deny or refuse to accept their loved one’s symptoms (Meyer et al., 2015). Several research studies have found that Vietnamese adults in Vietnam are at significant risk of cognitive impairment due to their low socioeconomic and education levels (Kaup et al., 2014; Tschanz et al., 2013). It may be plausible that their adverse living conditions and extensive trauma, Vietnamese may be prone to a higher risk of cognitive impairment in their older years. Given the prevalence of cognitive issues among the Houston older Vietnamese from the result of VACS 2 and their seemingly low literacy on dementia, it is critical to improve the level of dementia health literacy not only at an individual caregiver level but also at a community level. It is also imperative to educate the Vietnamese community and demystify the belief that memory loss is a normal aging process.
Based on these backgrounds, we proposed a Community-Engaged Dementia Education Program (CEDEP) for the Houston Vietnamese American community. The specific aims of the CEDEP were to examine the Houston Vietnamese American community’s current literacy/knowledge level of dementia (Aim 1) and develop educational materials on dementia appropriate for the Houston Vietnamese American community (Aim 2). This paper reports on the results of the key informants’ perception of the Houston Vietnamese American community’s health literacy on dementia/Alzheimer’s disease, the production of the educational material, and plans for the intervention: the implementation and dissemination of the CEDEP educational material.
Methods
Study design and procedures
We used the Cultural Exchange Model (Haralambous et al., 2014, 2018) as a conceptual framework for this study. The Cultural Exchange Model was developed for older Chinese and Vietnamese Australians to improve the understanding of the barriers and enablers that older Chinese and Vietnamese living with dementia face when seeking help. This model works based on a collaboration between two pillars of researchers and stakeholders such as service providers and community members to build evidence about a particular topic. Similar to the Australian original model, leveraging our existing partnerships with the Houston Vietnamese American community, we developed our model of two pillars as researchers (i.e., our research team) and stakeholders (i.e., Houston Vietnamese American healthcare professionals, social service agencies, and the Houston Vietnamese American community) (Figure 1). We started the study by inviting 14 Vietnamese key informants, consisting of active and influential figures who have been known in the community including 5 Vietnamese healthcare professionals, 3 executive directors of social service agencies, 2 social media-related professionals, as well as 4 dementia family caregivers. Modified Cultural Exchange Model.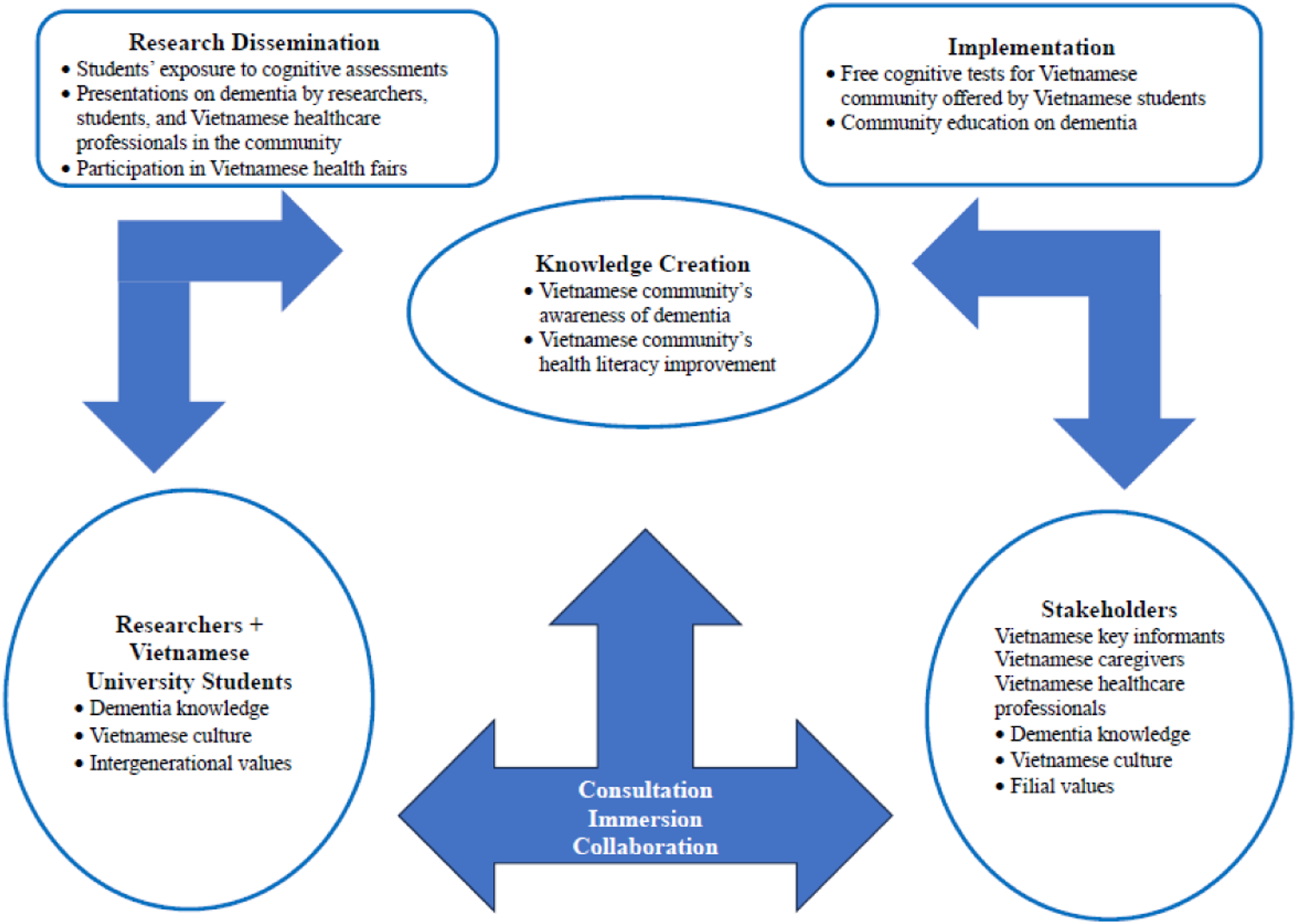
To examine the current knowledge of dementia in the Houston Vietnamese American community (Aim 1), we used Edwards and colleagues' Community Readiness Model (2000) (Figure 2), which consists of nine stages of community readiness levels that range from [Stage 1] “no awareness of the problem” to [Stage 9] “professionalization in the response to the problem within the community” (2000, p.1). We interviewed key informants to assess the community’s readiness stage for an issue that needs to be addressed and changed. Community Readiness Model.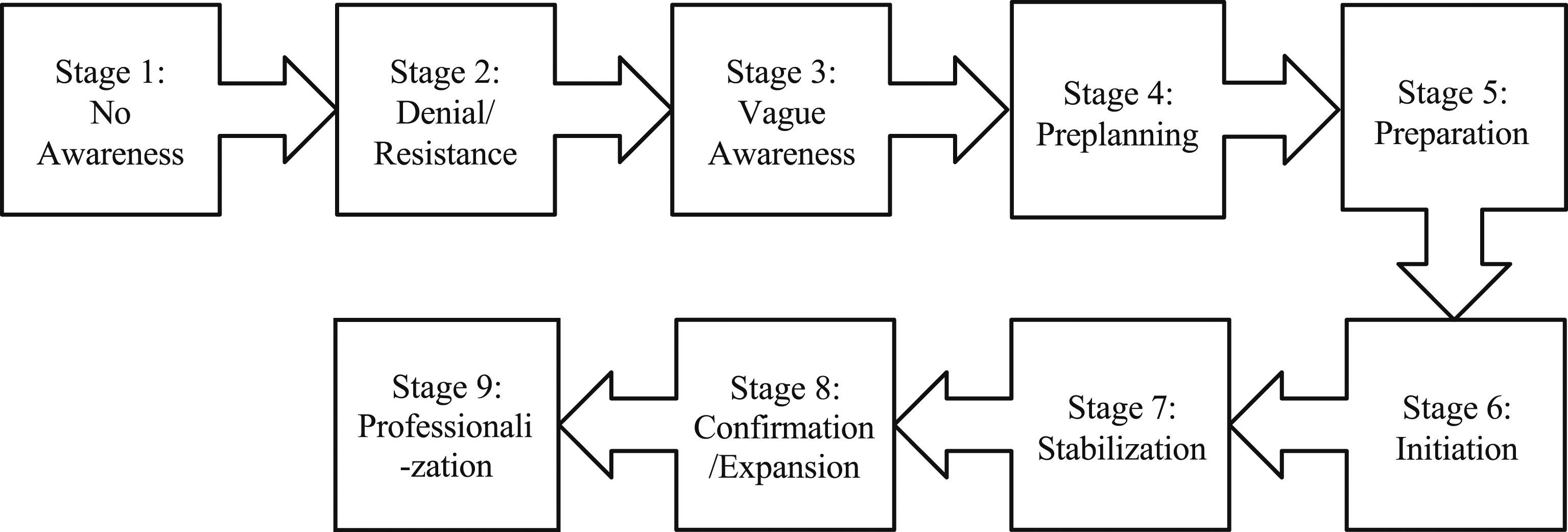
The interview guide (see Supplementary Material) was developed guided by two Vietnamese public health experts and pilot-tested before the interviews took place. The interviews explored the key informants’ personal experience/knowledge about dementia; the community’s perceived knowledge about dementia; stigma and cultural factors that involve dementia; perspectives on the educational materials for the community; and tangible ideas for the educational materials.
In order to develop educational materials on dementia appropriate for the Houston Vietnamese American community (Aim 2), all 14 key informants were invited to two focus group meetings. The focus group guide (see Supplementary Material) was developed and also guided by the same two experts. The first focus group meeting provided the key informants the opportunity to learn the results of the individual interviews, the research team showed the existing educational materials for dementia, shared potential photos and contents of the educational material (i.e., one-pager) in English and Vietnamese, discussed appropriate translation for terms such as “dementia” and other dementia-related English words in Vietnamese, and finalized the draft one-pager. The second focus group meeting was to review the final versions of the one-pager, modify/edit the contents tailored to the Vietnamese language, culture, the target population (i.e., middle-aged caregivers and older care recipients), complete the final versions of the one-pager, and discuss each key informant’s contribution to the implementation and dissemination stage of the CEDEP. This study was approved by the University of Houston Institutional Review Board (STUDY00003493). Written consent was obtained from all the study participants before the interviews took place.
Data analysis
With permission from all the key informants, interviews were audio-recorded. All recordings were transcribed verbatim by a professional transcriber, and Research Assistant 1 (KN) developed a summary of each interview with some key points as our notes. For Aim 1, we used thematic analysis (Braun & Clarke, 2006) and analyzed the key informants and the community’s knowledge and understanding of dementia. The Principal Investigator and Research Assistant 2 (AM) read the transcripts separately, the Principal Investigator developed a code book, and Research Assistant 2 reviewed and edited as necessary (Strauss & Corbin, 1990). For Aim 2, the Principal Investigator and Research Assistant 2 took notes of the key informants’ suggestions and recommendations and conducted member checking (Birt et al., 2016) with six key informants for validation purposes. All the interviews were analyzed using the qualitative software, Atlas.ti Web (Version 3.15.0-2022-03-09).
Results
Sample characteristics
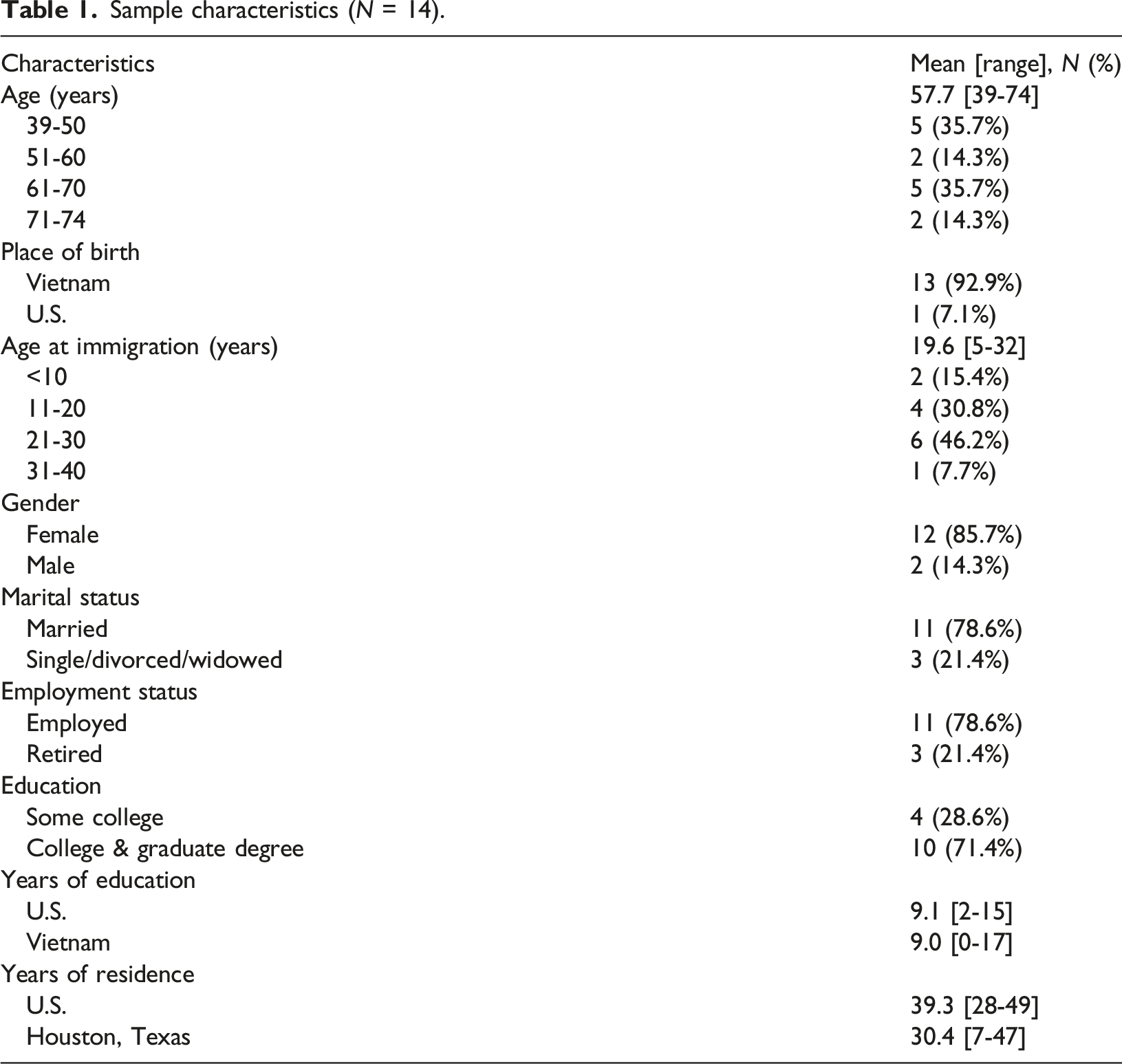
Sample characteristics (N = 14).
Key informants’ interviews
The semi-structured interviews covered the topics of family background, community involvement, caregiving of older Vietnamese with dementia, perspectives on the educational materials for the community, and tangible ideas for the design and dissemination of educational materials (see Supplementary Materials). All the interviews were conducted between March and May 2022 by the Principal Investigator and took place at the key informants’ workplaces (57.1%) or homes (42.9%). The average length of the interviews was 53 minutes (range: 27–77 minutes), and a store card of $30 was provided as compensation.
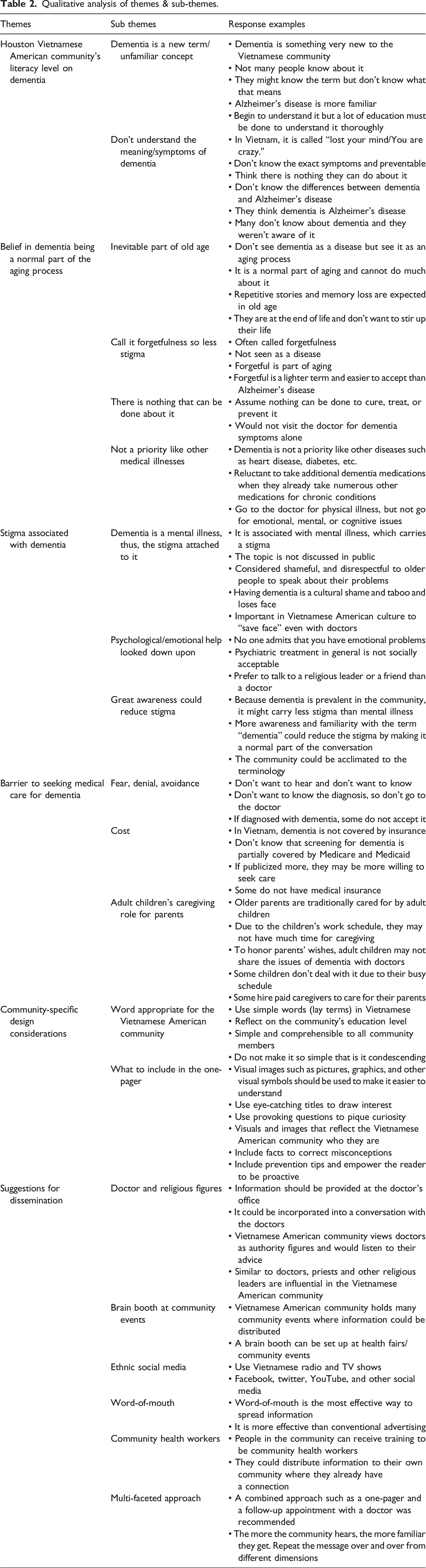
Qualitative analysis of themes & sub-themes.
Houston Vietnamese American community’s literacy level on dementia
All informants expressed the fact that dementia is still an unfamiliar word within the Vietnamese American community as no direct Vietnamese translation exists or is known of. Some may have heard of it, but the vast majority of the community does not know its symptoms, and few truly understand what it means. Confusion over the terms Alzheimer’s disease and dementia was common with few able to distinguish between the two. After a series of discussions among all the key informants, a term, bệnh mất trí nhớ was proposed as the closest translation of dementia in Vietnamese. Overall, their dementia literacy level was considered to be Stages 2–3 out of 9 stages of the Community Readiness Model: Stage 2: Denial/Resistance to Stage 3: Vague awareness (Figure 2). “In Vietnam, they didn’t call it dementia. They call it, lost - lost your mind…You lost your mind. It’s like you’re crazy.” (Informant 1) “Dementia is something very new to the Vietnamese community…They know of Alzheimer’s, but they do not know dementia…They thought that dementia is Alzheimer’s…Yeah. they knew of Alzheimer’s. But they [don’t] know what kind of symptoms at all.” (Informant 1) “Vietnamese people can’t distinguish between dementia and Alzheimer’s.” (Informant 3) “The term, dementia is new to the community. Even Alzheimer’s disease, not all of them know.” (Informant 9)
Belief in dementia being a normal part of the aging process
Some Vietnamese know that Alzheimer’s disease and/or dementia if they know the term, are associated with memory loss but the Vietnamese American community considers forgetfulness to be a natural part of the aging process. Memory loss is seen as inevitable and something that everybody will go through eventually in their lives, and thus, having memory loss is something that cannot be prevented or helped. They also have the common misconception that “with dementia or Alzheimer…there’s no treatment” (Informant 11). Because “there’s nothing they can do about it” (Informant 2) and eventually everyone gets Alzheimer’s disease or dementia, having Alzheimer’s disease and related dementias is not understood or prioritized in the same way as other physical ailments such as diabetes or heart disease, and thus, they rarely seek medical assistance: “Dementia and mental disease are very low in priority in the Vietnamese community…they prioritize more of cancer, heart, stroke.” (Informant 3). “They don’t see that [dementia or Alzheimer’s disease] as a disease. They see that as an aging process.” (Informant 1) “They’re just like, “Oh, we’re getting old. It’s senior.” And then, ‘We’re just forgetful and that’s it. So, to them, it’s not a sickness.” (Informant 2) “So, I think that because of the old age, everybody get it.” (Informant 9)
The stigma associated with dementia
Many key informants noted how stigma is still attached to Alzheimer’s disease and related dementias, making community dialogue all the more difficult. That is partly due to Alzheimer’s disease and related dementias being mistaken for mental illness and evoking the same negative connotations associated with psychiatric conditions. “It is still a cultural shame and taboo” (Informant 11) and “is a very tough topic to talk about” (Informant 12). Older adults have expressed their resistance to discussing dementia with their doctors as they feel it is important in Vietnamese culture to “save face” (Informant 1). “They wouldn’t be even reaching out to ask for help” (Informant 11), saying things like, “Oh, no, not that me, that’s not me. I’m not gonna sit down and talk to the doctor about because that not me. I don’t have that problems” (Informant 14). Because the term dementia connotes mental illness in general, it is important to fully understand the community’s attitudes and discomfort with the topic. Psychiatric treatment is not socially acceptable in the Vietnamese American community, lest patients admit they have a mental disorder or “something wrong with your mind” (Informant 1). However, it is acceptable to discuss one’s problems with non-medical personnel: “You talk to a Buddhist monk, a Catholic priest or a friend, but seeing a psychiatrist mean that you have something wrong with your mind” (Informant 1).
It was suggested that greater awareness of the disease would reduce some of this stigma by acclimating the community to the terminology and correcting misconceptions: “the more they hear, the more familiar they get used to the terms” (Informant 1). Much of the negative response to the topic could be avoided through greater awareness “so they don’t get, you know, sad or upset or shocked about it” (Informant 11). Furthermore, dementia was perceived as less socially taboo when compared to addressing other mental illnesses, as it was suggested that its association with natural aging and common occurrence ameliorates some of the shame and discomfort surrounding the topic. For instance, several informants reported “Forgetful is a lighter term… And people accept it easily. They always said, “Oh, I – I start forgetting doing things.” Things like that.” (Informant 1) “Cognitive health less stigmatized than mental health.” (Informant 9)
Barriers to seeking medical care for dementia
Numerous barriers were identified as reasons for not seeking medical care for dementia. Foremost was due to fear, subsequent avoidance, and outright denial of the condition. “A lot of people are – well, not wanting to know because they are afraid” (Informant 12). This prevents them from going to the doctor’s office since “it will be something like telling them something that they are afraid of” (Informant 2). Older adults “doesn’t want to admit that they have some problem” (Informant 2). Even for those who know they have the condition, denial is a common response with parents dismissing the diagnosis or preferring to ignore it completely. “If they do find out that they have it, there is a denial” (Informant 12). This applies to the community’s sentiment in general as some Vietnamese Americans are resistant to learning more about the disease. “I think somehow fear is there…people may not want to learn about it” and “living in America, we hear often enough, but not want to learn about it” (Informant 12).
Cost, as well as not knowing about insurance coverage for dementia treatment were mentioned as another barrier. In Vietnam, mental health conditions are not commonly covered by insurance and can be expensive to treat out of pocket. Even in the U.S., the Vietnamese American community might be unaware that Medicare and Medicaid cover part of the cognitive assessment (Centers for Medicare & Medicaid Services, 2023). It was suggested that if this fact was informed widely to the community, that would result in more patients seeking Alzheimer’s disease and dementia-related services. But the issue of cognitive health is a new concept to the community and if the coverage of health insurance for any assessment or diagnosis is unknown, it is a barrier: “It’s still very new. They don’t know how much they’re gonna get help with payment or how much the bill is gonna be” (Informant 11).
The decision of the family members, especially adult children who are caregivers of their aging parents, also influenced whether or not the older parent received medical attention. Some adult child caregivers were occupied with their work obligations during normal business hours and could not afford to take time off from work for doctor’s appointments. Others dealt with their parents’ cognitive decline by hiring in-home healthcare workers if they were too busy. Other children with a sense of filial piety noted how they wanted to respect their parents’ wishes and not trouble them in their later years. “They’re gonna die soon. So, just let it be and then it’s gonna pass. So, they don’t want to stir it up or do anything more to it” (Informant 11). Even if the adult children encourage their parents to see a doctor, they might be met with resistance from the parent and choose to honor their wishes. “You can see daughters that really want to take their mom to see the doctor but her mom says, ‘I’m fine…I don’t think I need it,’” (Informant 2).
Culturally and linguistically tailored community-specific design considerations
All key informants agreed that the community was in need of education and were eager to promote greater discussion around dementia. However, dementia remains a sensitive subject in the Vietnamese American community. Therefore, how the topic is broached relies heavily on the nuanced perspective of the key informants, and their advice on navigating sensitive areas of conversation. The theme of culturally-sensitive and community-specific design considerations emerged and recommendations were made based on their experience in the local community.
Special care would need to be taken in the wording and design of the one-pager due to the education level of the target audience. Given the low education level and traumatic background of many community members, it was suggested that the one-pager refrain from using clinical terminology such as “testing” and “cognitive impairment” and, instead, employ more informal language. For example, replacing the word “dementia” with “short-term memory loss” would be more comprehensible for an audience unfamiliar with Alzheimer’s disease and related dementias. Yet, the wording should not be so elementary that it could be perceived as condescending. Overly simplistic wording would be ill-received, therefore, “you have to do it where they don’t get offended but they’ll accept it…Above all else, the design must “reflect the community and who they are.” (Informant 11).
“Visuals are important. Include more pictures than words; friendly to everybody no matter their education level; little words. Target the population that has fear about the illness. To limit their barrier, start with talking about, just like diabetes.” (Informant 12). They wanted to include information that would dispel common misconceptions, increase awareness about the warning signs of Alzheimer’s disease and related dementias, and provide ways they could combat the disease. 14 informants agreed that there should be an eye-catching message such as “Do you think you have dementia?” or “Are you aware that dementia is a silent disease?” at the top of the one-pager in order to pique readers’ curiosity. It should be simple and concise, yet informative. It was recommended to include facts, statistics, and information about the disease with symptoms (e.g., warning signs), as well as solutions: “there are ways to prevent dementia or slow down the progress [so that we are not just leaving them hanging but give them somewhere to see the solutions to feel better].” (Informant 2). “[First, we need to explain] the difference between mental illness and “being forgetful” or “losing your mind.” The term, “forgetful” is more accepted. But be careful while using these terms [due to stigma and shame.]” (Informant 1) “People might be drawn away from the term, “dementia.” We have to use another word that describes it but doesn’t say it straightforward.” (Informant 13)
Suggestions for dissemination
The last topic was focused on suggestions for future interventions: implementing and disseminating the information in the community. They agreed that printed material such as a one-pager should be made available at doctors’ offices, pharmacies, and social service agencies. “Disseminate [the one-pager] at the doctor’s office and educate caregivers and their loved ones.” (Informant 3)
Doctor’s offices are good places to distribute because “the community strictly listens to their doctors.” (Informant 5) and with “my dad and my mom generation, the doctor is the boss.” (Informant 14). Therefore, information is likely to be considered when dispensed from a physician’s point of authority within the community. “If coming out from provider, it’s increase the value and the meaning of that.” (Informant 9). Similar to doctors, religious leaders in the community are highly regarded and were mentioned as authority figures that people would listen to and heed their advice. Training community health workers by recruiting local residents was suggested, along with utilizing telehealth services and in-home healthcare workers during house calls.
Other ideas included having a cognitive/brain booth at community events, churches, temples, and adult daycare centers. Social media such as radio and TV channels were also mentioned as a means to reach a wider audience. Creating a website, YouTube videos or short films about stories of families caring for their loved ones with dementia were suggested as engaging ways to appeal to audiences across generations. Texting as a means of notifying and mobilizing the community was recommended with one informant stating that “We notice when we use texting to get people to go out and vote, they respond.” (Informant 12).
Likewise, word of mouth was recommended as the most effective means of spreading information within the community. “Word of mouth is what really gets information out. Sometimes people think it’s advertising, but over the years…I found that we still do the advertising, but word of mouth beats it.” (Informant 12).
A multi-faceted approach (social media and health fairs) and reinforcement with a conversation with healthcare professionals were highly recommended by all informants.
Focus group meetings
Two focus group meetings were planned (first meeting in person and second meeting virtually via Zoom). Due to the informants’ work schedule, two separate focus group sessions for each meeting were conducted (5 informants in each group). Both focus group discussions were facilitated by the Principal Investigator, and Research Assistant 1 took extensive notes during the meetings. The first discussion meetings were held in June and the second one took place in July 2022. The last member checking with all the key informants (Birt et al., 2016) was completed in August 2022. All the discussion meetings took 1–1.5 hours and were compensated by a $30 store gift card.
The goal of the first two focus group meeting
As the next step, the research team hired a Vietnamese professional designer to create sample one-pagers. The designer and the research team met and shared the outcomes of the first focus group meetings. The designer searched for relevant images on the front page, inserted the content, and developed several versions of the one-pagers. We shared those draft versions with the key informants during the second focus group meetings. At the end of the meetings, the key informants and the research team finalized the front-page images and the content of the one-pager and sent it to the designer to develop the final version. Once the final versions (in English and Vietnamese) were made, they were shared with the key informants for final review. Approval of the document was then obtained from all key informants (see Supplementary material).
Discussion
The VACS 2 data revealed the high prevalence of mild cognitive impairment and dementia in older Vietnamese, however, seeking medical care from primary care physicians or specialists remains an uncommon practice in the Vietnamese American community. Time constraints, work schedules, and other obligations seem to prevent caregivers from taking loved ones to the doctor. Most caregivers are aware of memory loss, mood changes, or other signs of cognitive decline in their loved ones, but often attribute these changes to natural aging. Because dementia symptoms are expected and seen as normal in the older population, caregivers are often resigned to handling it on their own, even at great cost and inconvenience. Moreover, there is a stigma attached to cognitive impairment, and a sense of shame attached to the loss of functioning. This prevailing attitude dissuades adult children from dishonoring their parents and they attempt to keep their struggles private or within the family.
Based on the key informants’ assessment, the Houston Vietnamese American community’s health literacy level on dementia was between Stages 2 and 3: the denial/resistance to vague awareness stages. Han et al. (2015) conducted a similar study with a Vietnamese American community in Northern California regarding their mental health awareness. Their readiness level was assessed using the same model, and the result was between Stages 2 and 3. But after introducing a mental health awareness pilot project utilizing ethnic-specific social media, key informants (N = 7) believed that the community’s awareness of mental health issues improved. Our key informants all agreed to utilize their ethnic radio and TV programs to advertise the one-pager in addition to disseminating the one-pagers from other venues (e.g., doctor’s offices). Ethnic radio, TV stations, and newspapers are an integral part of Vietnamese people’s lives as they rely on these media as daily sources of information (National Association of Broadcasters, 2022). A group of Houston-based psychiatrists (Bui, 2016) initiated a mental health awareness project and utilized Houston’s local media channels. After broadcasting several segments of recorded programs, the stations received more mental health inquiries from across the nation. Thus, ethnic media outlets appeared to be the appropriate way to reach out to the local Vietnamese American community.
A pilot survey about the knowledge level of dementia was conducted with 102 Vietnamese immigrants in Southern California (Nguyen et al., 2016). Similar to our study, their literacy level on dementia was low. The respondents misunderstood that dementia was a treatable disease, and similar to the Houston Vietnamese American community, they believed that the pathological decline was an unavoidable, natural part of aging. It was suggested that offering education and community outreach programs may increase the community’s health literacy and lead to more patients seeking cognitive evaluation and treatment. Haralambous et al. (2018) conducted dementia education programs to improve the health literacy of older Chinese and Vietnamese in Australia and concluded that “health literacy is an evolving process” (2018, p. 8) and requires ongoing education and consideration of the culture of the community. Several ethnic-specific and culturally tailored interventions for caregivers of people living with dementia have been developed, successfully implemented, and helped caregivers’ mental health issues (Meyer et al., 2020; Miyawaki et al., 2020b; Ta Park et al., 2019a, 2019b). Therefore, tailoring and developing a program specific to the target population may be the best way to impact change and improve outcomes.
The strength of the CEDEP was that we leveraged the involvement of the key informants from the very community that we are trying to learn from and assess. Key informants included professionals who have worked for and/or lived in the Houston community for an average of 30 years, and thus, possess the most accurate insight. Four members of the key informants were also dementia caregivers who provided essential input directly from the one-pager’s target population. However, this one-pager was developed exclusively for the Houston Vietnamese American community. All the contents and components were developed and appropriate for the health literacy level of the Houston Vietnamese American community (i.e., language, details, etc.), and were approved as the final product for dissemination to the Houston Vietnamese American community, and thus, the product is geographically limited. Although it is not unusual for this type of community participatory study, the sample size of key informants was not large (N = 14). Other key informants, such as Vietnamese neurologists, could have been included. However, there were no known Vietnamese neurologists in the area at the time of the study despite that Houston has the largest medical center in the world (Texas Medical Center, 2022). This fact may reflect the resistance to and unfamiliarity with mental and cognitive assessment in the Vietnamese American community (Gordon et al., n.d).
Conclusion
Negative health consequences of low health literacy have been well-documented regardless of race and ethnicity (Hickey et al., 2018; Shahid et al., 2022; United Health Group, 2020). The Vietnamese American population, and more specifically the Vietnamese refugees/immigrants in the U.S., have been considered to be a community with one of the lowest health literacy (Lee et al., 2015; Sentell & Braun, 2012). They are especially vulnerable to health disparity because they tend to be older with low socioeconomic, low education levels, and low English proficiency, and they are unaware of preventive care, available services, and need for health care, and may not have health insurance (Lee et al., 2015; Sentell & Braun, 2012; Xiao et al., 2020). We have developed educational material in the form of a dementia one-pager, that is culturally and linguistically tailored specifically for the Houston Vietnamese American community based on the Cultural Exchange Model. By utilizing previously proven outreach methods such as local ethnic radio and TV stations, collaborating with key informants and their network of affiliated venues, as well as involving university students in their co-curricular activities, and offering a cognitive booth at various Vietnamese health fairs, our next step is to disseminate the one-pager throughout the community, measure, and evaluate the effectiveness of the outreach. In spreading this information, we hope to improve health literacy on dementia in the Houston Vietnamese American community.
Supplemental Material
Supplemental Material - A culturally and linguistically tailored Community-Engaged Dementia Education Program (CEDEP) for the Houston Vietnamese American community
Supplemental Material for A culturally and linguistically tailored community-engaged dementia education program (CEDEP) for the Houston Vietnamese American community by Christina E. Miyawaki, Angela McClellan, Kim N. Nguyen, and Tuong-Vi Ho in Dementia.
Footnotes
Acknowledgements
The authors appreciate the enthusiasm of the following stakeholders who dedicated their time and energy to creating the one-pagers for the Houston Vietnamese American community. Ms. Jannette Diep (BPSOS-Houston), Dr. Tram Ho, Ms. Quynh Thi Hoang (VieTV), Ms. Myle Jones (Golden Bamboo Village), Dr. Anhlan Nguyen (Lyceum Global), Mr. Mike C. Nguyen (VN TeamWork), Ms. Nina P. Nguyen, Ms. Susie Nguyen, Ms. Thien-An Nguyen (Houston Unity Lions Club), Ms. Vicky Nguyen, Dr. Tri Pham (MD Anderson & Texas Woman’s University), Ms. Loan Tran, Ms. Thuy Vu (Radio Saigon Houston) (Listed alphabetical order by last name).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Miyawaki was supported in part by a pilot grant from the Engaging Communities of Hispanics for Aging Research (ECHAR) network (NIH/NIA R24AG0065170; L.D. Medina, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (NIH).
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author, CEM, upon reasonable request (Data for Original Cultural Exchange Model taken from Haralambous et al., 2014).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.