
Abstract
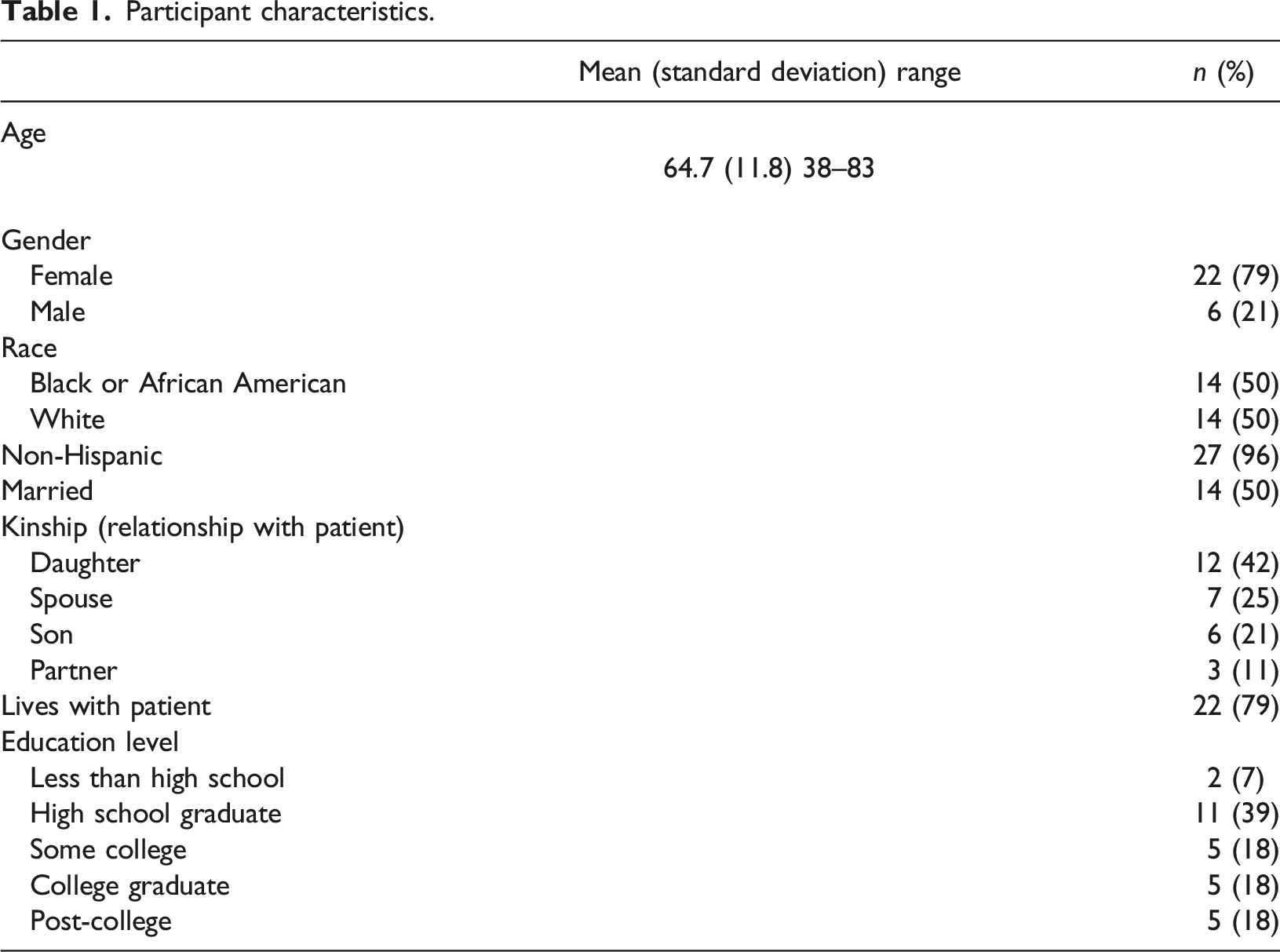
The Family-centered Function Focused Care (Fam-FFC) intervention, is a nurse-family care partnership model aimed to improve the physical and cognitive recovery in hospitalized persons living with Alzheimer’s Disease Related Dementias (ADRD) while improving the care partner’s experiences. Discussions of patients’ needs and preferences between nurses and the patient’s close family members have been found to be useful in preventing excessive stress in persons with dementia, while lessening the anxiety of care partners. However, the efficacy of dementia-specific interventions is influenced in part by the degree to which the interventions are flexible and sensitive to the patient’s and care-partner’s condition, needs, and preferences, including cultural preferences. Therefore, the purpose of this study is to assess the cultural appropriateness of Fam-FFC using the Ecological Validity Model (EVM). This qualitative, descriptive study included 28 consented care partners drawn from a sample of 455 dyads enrolled in the Fam-FFC intervention. An interview guide was created based on the EVM. Participants provided demographic data. Thematic analysis was conducted to analyze transcribed interviews. The majority of the sample was female (79%), Non-Hispanic (96%) and half were married. One-half of the sample represented Black care partners and one-half were White. Seventy-nine percent lived with their family member with ADRD. Three major themes were identified from the thematic analysis including Care Partner Identity, Care Partner Preferences, and Goals of Care for functional recovery of their family member living with dementia. In this study care partners wanted more social services as well as home care that supported not just physical needs but also social and recreational needs. Findings from the study offer guidance on improving the Fam-FFC intervention including strengthening education and resources on partner self-care.
Background
Over six million people in the United States (US) and over 50 million worldwide are currently living with Alzheimer’s disease and related dementias. Persons living with Alzheimer’s disease are about two times more likely to be hospitalized than their peers who are cognitively healthy accounting for 3.2 million hospital admissions per year (Alzheimer’s Association, 2022). Prior to the acute care stay, approximately 80% of hospitalized patients with Alzheimer’s disease in the US are living at home and receiving care from the over 16 million family members or friends who are acting as unpaid caregivers, also known as care partners (CDC: Centers for Disease Control and Prevention, 2019). Over fifteen billion hours of caregiving at a value of over 250 billion dollars are provided per year in the US (CDC, 2019).
Although the rewards of caregiving are well documented, including enactment of values, skill attainment, and emotional reciprocity (McGillick & White, 2016; Yu et al., 2018), the demands take their toll. Care partners of persons living with dementia face compromises to their time, finances, health, quality of life, and even productivity in the workplace (National Academies of Sciences, Engineering, and Medicine, 2021). The progressive cognitive and functional decline and associated neuropsychiatric symptoms places a large burden on family members providing care (Connors et al., 2020) and the demands are associated with increased psychological and physical morbidity and mortality (Gilhooly et al., 2016; Karg et al., 2018; Koyama et al., 2017). The mechanism of action for negative physiologic changes are attributed to the emotional demands of caregiving, sustained vigilance, poor sleep, and inability to attend to the care partner’s health promoting behaviors (Jiménez-Gonzalo et al., 2021). Sources of psychological strain are due to role changes within the family, competing demands at home and the work setting, and insufficient information sharing and engagement in decision-making with health care providers (Rowe et al., 2016).
While hospitalization of a family member with dementia may be expected to provide respite for care partners, the experience is often associated with increased stress for these individuals (Shankar et al., 2014). The greater presence of troublesome symptoms including neuropsychiatric symptoms and delirium, increases care partner distress. The pre-existing, chronic strain borne by care partners of persons with dementia is also compounded by anxiety about the comfort and safety of the patient during their hospital stay and the potential for increased care needs at discharge that they feel unprepared to meet (Keuning-Plantinga et al., 2021; Kuzmik et al., 2021; Shankar et al., 2014).
When engaged to do so, care partners of hospitalized persons with dementia provide essential information on the baseline cognitive and functional statuses of patients, which is necessary to guide care delivery and track treatment response (Boltz et al., 2015a). Although not typical practice in the acute care setting, discussions of patients’ needs and preferences between nurses and the patient’s close family members have been found to be useful in predicting and preventing excessive stress in persons with dementia, while lessening the anxiety of care partners. Further, family members can play a positive role by motivating and encouraging patients during the hospitalization and subsequently at home (Boltz et al., 2015b, 2021).
The Family-centered Function Focused Care (Fam-FFC) intervention, a nurse-family care partnership model, aims to improve physical and cognitive recovery in persons living with dementia during hospitalization and the 60-day post-acute period, while also improving the care partner’s experience during the inpatient encounter. Fam-FFC provides a function-focused care pathway that individualizes care during the hospital and post-acute timeframe and includes caregiver education and engagement in assessment and decision-making, as well as unit-based environmental and policy modifications, and staff education. Post-acute education and coaching is provided to care partners via telephone for eight weeks then monthly for four months after discharge, to support continuity of a plan to address potential complications, promote functional recovery, and improve the quality of life in the person living with dementia and their care partner. More detailed information on the Fam- FFC intervention can be found elsewhere (Boltz et al., 2018).
The efficacy of dementia-specific interventions is influenced in part by the degree to which the interventions are flexible and sensitive to the person’s condition, needs, and preferences (Karrer et al., 2020). Cultural factors influence preferences, values, beliefs, behaviors, and language which can affect engagement with and success of interventions (Parra Cardona et al., 2012). Thus, an important goal of the Fam- FFC work is to explore the cultural responsiveness of the intervention, considering the need to avoid preconceived ideas and biases regarding age, gender, dementia diagnosis (i.e., “ableism”), race and ethnicity. Cultural responsiveness takes a strengths-based approach to clinical interactions and is defined as the ability to respectfully learn from, relate to, and build on own as well as other cultures (New York State Education Department Board of Regents, 2017: Williams et al., 2003). Thus, the purpose of this study is to examine perceptions of the cultural responsiveness of Fam-FFC among a sample of care partners of persons living with dementia.
Guiding framework
The Ecological Validity Model (EVM), originally developed by Bernal et al. (1995) was used as a framework to assess the cultural appropriateness of the Fam-FCC intervention, and to refine Fam-FFC for future studies. The EVM highlights eight cultural dimensions that may impact how an intervention is deployed for a given cultural group. This framework includes language used; attributes of persons, incorporation of metaphors; consideration of content (i.e., cultural values and traditions) and concepts (i.e., theoretical orientation and intervention conceptualization); culturally-adaptive intervention goals; methods/procedures of intervention; and context of the intervention (Bernal et al., 1995).
Methods
This qualitative descriptive study included 28 consented care partners drawn from a sample of 455 dyads enrolled in the Fam-FFC intervention which took place in six medical units in three hospitals (two units per hospital) all located in Pennsylvania. The full protocol for the Fam-FFC intervention has been published elsewhere (Boltz et al., 2018). Approximately 10 percent of families from each ethnic group represented in the study were randomly sampled and approached for consent for participation in interviews. The demographics for the parent study included 64% white, 34% black and 2% who identified as other races. Our final sample yielded 28 care partners,50% Black and 50% White, who agreed to participate. Theoretical saturation of themes was established before closing the interview recruitment process.
An interview guide (Figure 1) was created based on the EVM and participants provided descriptive data. Interviews were conducted after the completion of the intervention (approximately six months after discharge from the hospital). Project staff conducted the interviews in a private room either in-person or telephone and participants provided written consent. Project staff who conducted the interviews and subsequent analysis of interview transcripts were not involved in delivering the Fam-FFC intervention. Interview guide.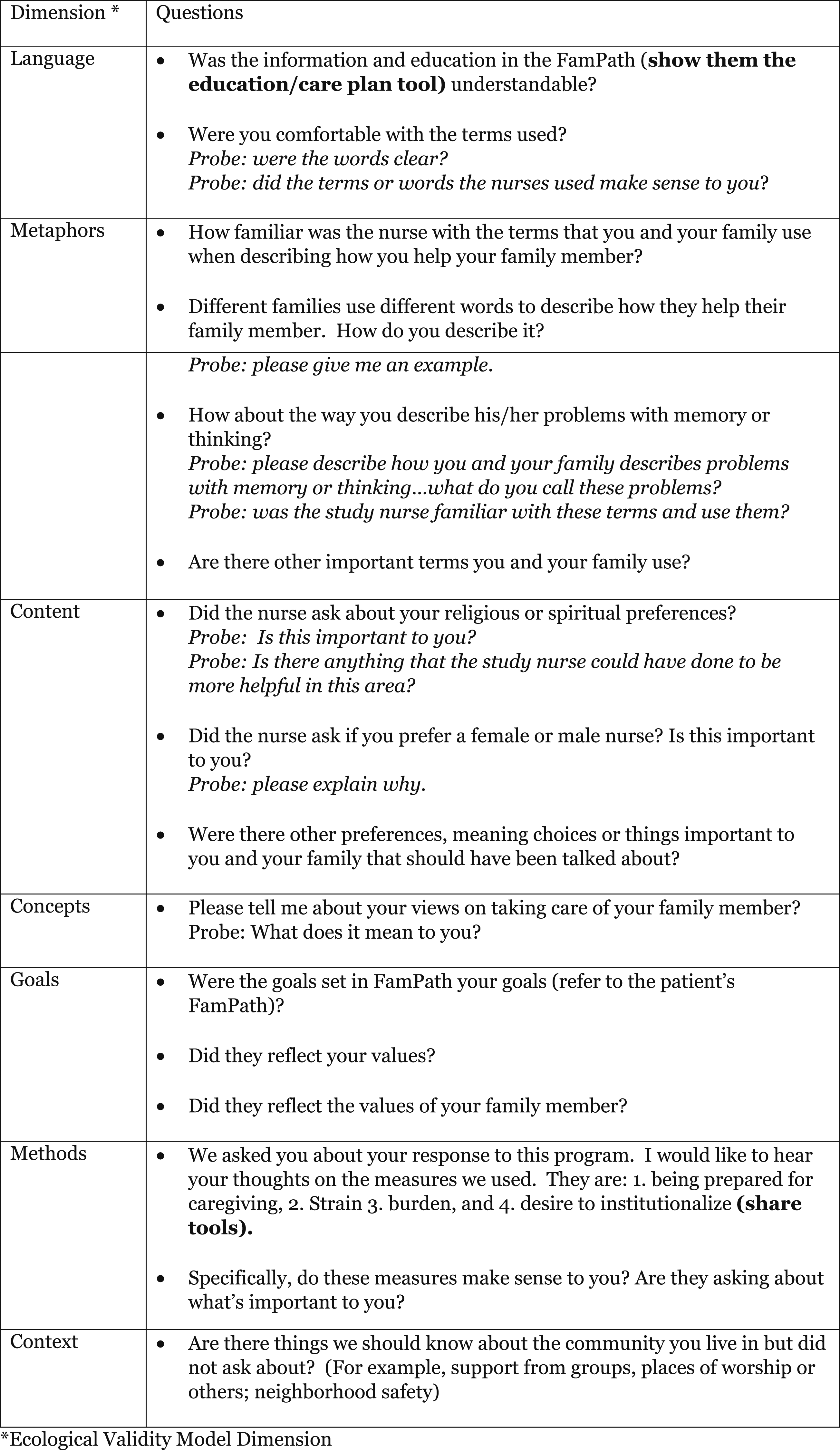
Interviews were recorded and transcribed verbatim using Dragon software (Dragon, 2023) then transcriptions were verified for accuracy. Recordings and descriptive data were stored in a secured REDCapTM site (Harris et al., 2009).
Ethical considerations
The Fam-FFC study was approved by the Pennsylvania State University Institutional Review Board on 9 February 2017 (Study #:00006201). This research complied with the ethical principles for medical research described in the Declaration of Helsinki. All participants provided written informed consent prior to data collection.
Data analysis
Thematic analysis was conducted according to the approach offered by Clarke and Braun (2013) and included familiarization with the data, then coding by two researchers individually who compared findings. The codebook was refined and iterative double-coding meetings were conducted until agreement was reached. Descriptive statistics for care partners were also analyzed. The codes were evaluated by two additional members of the research team, organized into themes and sub-themes by the primary coders, and validated by the research team. The trustworthiness of the data were fulfilled as follows: (1) credibility (i.e., confidence in the ‘truth’ of the findings) was enhanced by the team’s methodological expertise; rigorous analytic approaches; use of a detailed audit trail; and (2) dependability (i.e., application of methods that can be replicated) was based on our detailed methodological approach, use of a codebook, audit trail, and code verification (Guba, 1981; Shenton, 2004).
Results
Participant characteristics.
Three major themes congruent with domains of the Ecological Validity Model (EVM-see Figure 2 below), were identified from the thematic analysis as follows: Identified themes and corresponding EVM domains.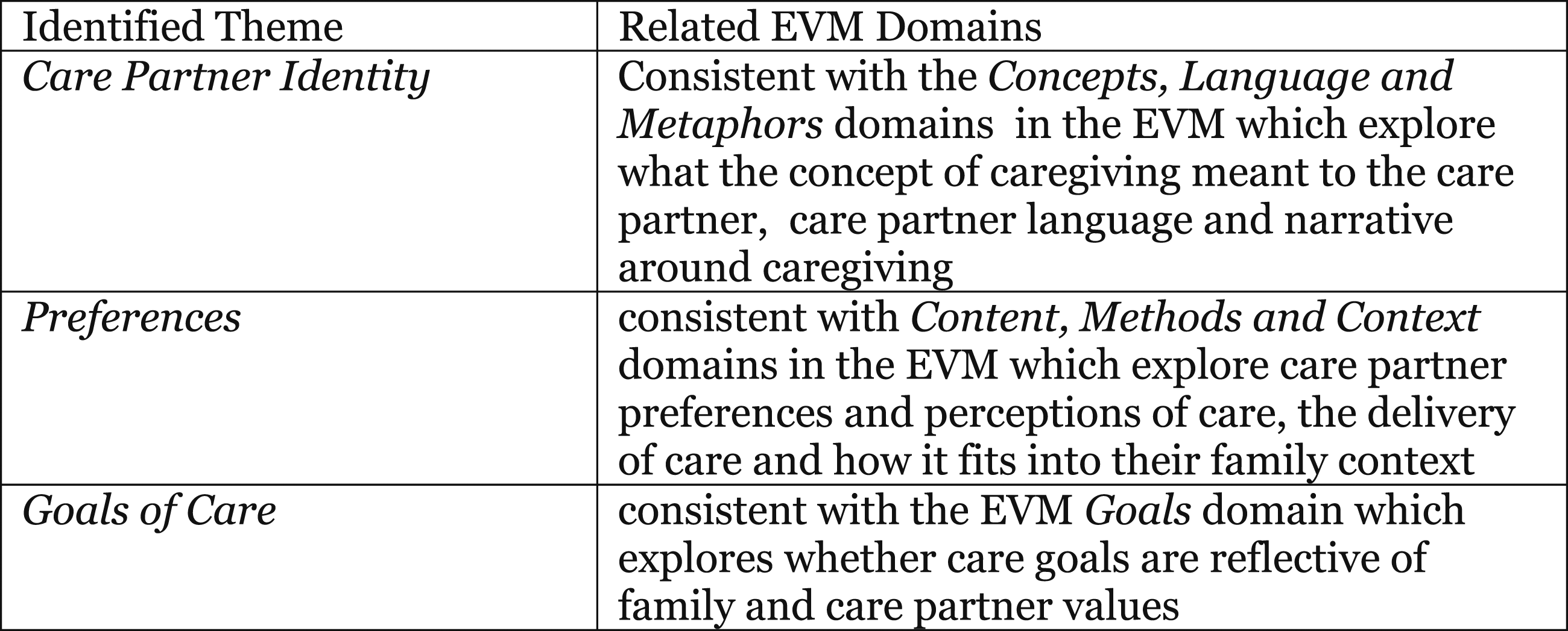
Theme 1: Care partner identity
The care partners offered three sub-themes describing the dimensions of their identity as care partners: the meaning that they ascribed to being a care partner, their activities as a care partner, and the language they use to describe the person living with dementia and their role.
Meaning of the care partner role
Care partners consistently described their role as an enactment of their values, what they believed was the right thing to do. A daughter who has two sisters, reported that she has “always considered myself to have been there for mom.” Care partners described themselves as passionate and committed, and acting as a care partner was integral to their identity (“who I am”). Another daughter reported that she has been a caregiver almost her whole life as she has been a nursing assistant for over 20 years; she has taken care of other family members as well. She stated that she doesn’t “see why I would not do it for someone I love so much, especially a family member.”
Care partners valued familial structure and found it important to care for their family members. In fact, care partners expressed joy and privilege in taking care of their family members, and do not feel they need to be labeled as care partners for their duties, as it is expected of them. Relationships between patients and care partners reflected biological connections, as well as those made through marriage.
“I was raised to take care of my elders…..you take care of your elders because they take care of you, it goes full circle, you must take care of them because if you don’t, whose there to take care of them.
Other comments noted that though there is a sense of familial connection and duty, these feelings can co-exist with stress and strain. Some care partners reported times of fatigue and exhaustion, preventing the opportunity for a social experience. For care partners married to the patient, a theme of commitment and time investment was identified as the reasoning for taking care of the patient. A husband care partner said it was part of the vows that included “for better or for worse.” Several spousal care partners described that they grew accustomed to their caring activities and they developed long-standing routines.
“We’ve been married for 47 years so I feel like it’s my responsibility to do it. Most of the time it doesn’t bother me, but sometimes it’s not the way I envisioned my retirement, but things happen. I’m happy he’s doing so well…… but like I said it’s a routine.”
Everyday care
When asked how they describe the help they provided to their family member living with dementia, care partners described “everyday care” as attending to physical needs, ensuring safety, as well as considerable attention to emotional needs and helping the care receiver enjoy life. Care partners found importance in reminding the patient of experiences they had during adolescence and earlier years, helping them relate back to family ties. This was found to be helpful when reducing the severity of the patient’s cognition skills, as it allowed them to be more settled, comfortable, and lucid in thought when reminded of impactful experiences. At moments, it seemed as if a patient’s memory improved.
Care partners also reported their value in being the repository of information regarding the preferences, needs, and situation of the person living with dementia. Consequently, they need to provide information to health care providers on an ongoing basis, and be alert for subtle changes in condition, which clinicians may not detect. For example, one care partner reported,
“Her (mother’s) left eye was not coordinated enough with the right to see the stuff on the
left. If you don’t pay attention….nobody really caught it, I actually had to look at my mother and study her for a little while and then I had to say to the therapist, ‘Listen, this is what I see, go check it out’…. he said, ‘you’re absolutely right’.”
Another aspect of everyday care is acting as an advocate with health care providers. Examples included advocating for rehabilitative care to help the care receiver be as functional as possible and convincing a medical provider to reduce the number of medications prescribed or changing a medication that the care partner believed to be harmful or ineffective.
Care partners’ use of language
Care partners described the impact of dementia and associated symptoms including memory loss, trouble recognizing people’s faces, needing help with basic care needs, and repeating themselves. Some care partners describe the challenges to communication and at times their relationship with their family members. One care partner described her father as “a shell of what her used to be.” Other care partners attempted to normalize manifestations of cognitive changes and accept them, as one described her father’s repetitive questions as “dad just being dad.” Care partners in general avoided diagnostic labels such as dementia and Alzheimer’s disease. Additionally, they described other issues that can confound the presentation of these symptoms. For example, difficulty recognizing faces was reported to be possibly due in part to vision loss; language issues (Spanish as primary language) may have contributed to difficulty understanding and remembering information.
Care partners felt that the educational materials, care planning materials, and measures were understandable. However, notably, care partners did not identify as caregivers and did not want to be referred to as such. They felt as though it was a normal part of life and did not relate to the label “caregiver,” instead preferring to be called by their familial role (e.g., son, wife, etc.), and similarly having their family member living with dementia referred in the same manner.
“I enjoy taking care of him, he’s my father, and I like him to have the best life he has left. I like to do whatever I can to keep him involved.”
Theme 2: Preferences
Three types of preferences were discussed by care partners: gender preferences for the nurse, spiritual preferences, and preferences related to “what matters” to the care partners.
Gender preferences
Gender preferences varied. While there were no strong gender preferences based on cultural norms, some families expressed practical reasons for wanting a male or female nurse. This includes a male nurse’s ability to physically assist their family member, or previous history that indicates that their family member reacts better to male authority.
“My mom responds better to male authority.”
“I don’t have a preference, but I think my dad would prefer a male nurse. I think he would get the care he needs with either one.”
Otherwise, families had no gender preference related to nurse gender and just wanted a well-qualified and kind nurse.
“……. if the nurse has credibility and went to schooling, it doesn’t matter if they are male or female” or “No, it wouldn’t matter if male or female. Just be a kind nurse!”
Spiritual preferences
Spiritual preferences were either deemed important by the care partner, or not important at all. In some families, engaging their family member who is living with dementia in spiritual activity helped the care partner navigate stress-related situations. Some types of activities associated with spiritual support included prayer, music, and attending church services, but often they were not specified. Some care partners believed spirituality was important because it provided a positive outlook for persons living with dementia and their family. Finally, there were some families that had no preference for discussing spirituality and indicated that they were not even asked questions about it by health care staff during patient encounters. Several reported that professional boundaries limited this type of discussion.
“….as a care provider you’re not really supposed to talk about religion with the people you care for unless you really knew them.”
“What matters” preferences
Care partners described their preferences and the degree to which they were addressed by Fam-FFC. They did not describe explicitly any cultural factors associated with these preferences but were clear about “what mattered” to them. They wanted to improve the mood of their family members, and help them to be mobile, to prevent medication related problems, and deal with medical problems (e.g., diabetes and infections). Care partners described the Fam-FFC nurse’s attention to meaningful activities as valued and appreciated their connecting the care partners to local resources such as arts and social programs. Care partners described preferences for information that addressed positive communication and strategies to enhance a positive relationship.
Preferences identified as needing more attention included education and resources to develop advance directives. Also, some care partners identified the need for services to provide more in-home support to provide respite and assistance (e.g., volunteers to help with activities such as gardening) and access to support programs for the care partner. Those care partners who were receiving support from their places of worship, senior centers, and adult day care agencies described them as helpful in relieving care partner burden and improving the function and well-being of the person living with dementia.
Many care partners reported that preference congruence was supported by the approach of the Fam-FFC nurse that treated them as experts in the care of person living with dementia. This was demonstrated by obvious and consistent attention to the care partner’s views and perspectives and helping include them in the daily plan. As one care partner reported, she felt like she:
“….was being heard and understood….would discuss with nurse about concern of (family member) not wanting to exercise and the nurse would listen to mention of the exercises she would not do and discussed other potential exercises (I) thought she would do- felt “heard correctly.”
Theme 3: Goals of care
Care partners were asked about the goals set in the hospital and updated at discharge and throughout the post-acute follow-up. Goals that were identified as successfully met included those that focused on increased mobility, ability to use the stairs, engagement in games, self-feeding, and being engaged socially. Care partners did not report that cultural norms played a significant role in effective goal setting. However, many care partners did report that the goals did reflect the values of their family member with dementia.
“We tried to have them (goals) reflect her values, as I said there are four of us, and we mostly agree and understand where my mom is coming from in the past and we try to project that into the future to make sure she is comfortable.”
Ongoing discussion of goal attainment was helpful in keeping the dyad focused on the goals, and following through the daily plan.
“The nurse seemed to be very familiar with the goals… and discussed our goals and seeing how I was doing….. and explored with us the dynamic of how the person living with dementia affects the family and vice versa.”
Discussion
This study aimed to engage care partners in an exploration of the cultural appropriateness of the Fam-FFC intervention to help inform clinical encounters and guide refinement of Fam-FFC based on the EVM. The three major themes identified from interviews illuminate care partners’ perceptions of their identity as a care partner, their preferences, and goals developed to support the well-being, health, and functional recovery of their family member living with dementia.
Caregiver identity was identified as a major theme which highlighted the Concepts, Language and Metaphors domains in the EVM. Some of the care partners describe their role as enactment of their values; this finding as well as the rewards of providing care to family members is consistent with other research (McGillick & Murphy- White, 2016). Moreover, there were descriptions from some participants that providing care to a family member was intrinsic to who they are, an essential dimension of their personalities and life.
The description of the helping activities of the care partners is conceptually aligned with salient, early family research that describes providing care (e.g., direct care) and coordinating care as two major caregiving roles (Archbold, 1979). The care partners also underscored the importance of other role dimensions including assessment, monitoring, information sharing, and acting as advocates for their family members living with dementia. These role dimensions are particularly important to supporting person-centered care in persons living with dementia (Gillick, 2013), who are compromised in their ability to identify their needs, communicate their preferences, and self-advocate. A study by Prato and colleagues (2021) found that care-partner interaction with health and social services is an important part of care partner identity development. Interactions that acknowledge care partner needs and well-being support their identity as an advocate for the person living with dementia. Care partners described strategies to support the emotional comfort of their family members, such as reminiscence, reminding clinicians of the need to view families as experts when intervening to promote a sense of wellbeing in the person living with dementia.
Care partners strongly stated their objections to being called “caregivers,” a term that is pervasively used in health care and research. Use of this term may pose as barrier to developing a therapeutic relationship with care partners and engaging them in scientific inquiry, and thus needs to be further explored for acceptable alternatives that are culturally acceptable. The Fam-FFC educational, care planning tool, and measures were otherwise acceptable and understandable by the care partners. However, we recognize that the measures used in the study were deficit- oriented and not aligned with care partners’ positive views of their role and their goals that focus on optimizing the capabilities and social engagement of the family member. Research is needed to further develop, test, and use strength-based measures, for both care partners and persons living with dementia. Such work is underway in both Europe and the United States (Clarke et al., 2020; Zimmerman & Fazio, 2022) consistent with the research and policy priority to enable people living with dementia and their care partners to “live well.”
The preferences and goals themes identified through care partner interviews highlighted EVM domains, Content, Methods & Context and Goals. Preferences and goals that were established by families reflect expectations and hope that their family members with dementia will ‘live well’. They also offer a multi-faceted view of quality of care that is function-focused (considers physical, emotional, and social function), manages medical problems competently, and supports the well-being and relationships within the family unit. In this study care partners wanted more social services as well as home care that supported not just physical needs but also social and recreational needs. Findings from the study offer guidance on improving the Fam-FFC intervention including strengthening education and resources on advance directives and care partner self-care.
The Ecological Validity Model was helpful in exploring the cultural appropriateness of Fam-FFC. It would be useful to integrate the model into trials that test Fam-FFC in distinct cultural groups, beginning in the early stages of the research.
Study limitations
Study limitations included the potential social desirability associated with interview questions, the use of a non-random sample, and care partners that were limited to those caring for patients with mild to moderate dementia, not severe. Additionally, the participants were recruited from only three hospitals in Pennsylvania and the study lacked inclusion of racial and ethnic groups other than Black and White participants.
Suggestions for future research on culturally responsive interventions
Culture was identified as a relevant factor for care partners in several ways. First, the identity of the care giver is an important aspect of culture that should be considered when working with care partners. Dilworth-Anderson et al. (2020) list caregiver identity as a cultural factor that helps explain how care partner ways of “being and doing” relate to caregiving and receiving preferences. Findings suggest that additional research is needed that examines care partner identity and its relationship to help-seeking as well as interventions that support the advocacy role of care partners. Further, individualized family-centered care may benefit from support for family spiritual preferences. For hospitalized patients, healthcare providers should be cognizant of the pre-existing stress faced by care partners, compounded by the stress related to an acute hospitalization. An assessment of care partner needs, preferred terms regarding their role, and what matters to them and the person living with dementia are a high priority. Providers also need to ensure that care partners are in the position to receive information, in an effective form and have an opportunity to follow-up at a later time with questions about caring for their family member. Finally, post-acute care needs to expand beyond medication management and medical treatments to include care that optimizes physical, emotional, and social function.
Footnotes
Declaration of conflict of interest
The author(s) declare no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Foundation National Institute of Aging (NIA), Grant: R01AG05445.