
Abstract
Many people living with dementia are ‘on the margins’, not accessing services and support, despite policy and care advancements. The COVID-19 pandemic exacerbated this, with the closure of face-to-face support during lockdowns in the UK and globally. The aim of the ‘Beyond the Margins’ project was to develop, implement, and evaluate a face-face programme of support with, by and for people with direct experience of dementia who are on the margins of existing services and support. In March 2020 the project was interrupted by the outbreak of the COVID-19 pandemic and it changed to an online format. The three-phase participatory action research project included 40 people living with dementia, 26 care partners and 31 health and social care practitioners. A seven-week online personal development programme called Getting On with Life (GO) was developed, delivered, and evaluated. This paper focuses on the participatory approaches used to develop and implement the GO programme, and the resulting aspects of its approach to facilitation and content. Key features include the GO Programme’s principles of providing a safe and a respectful space, and the programme’s values of: Everyone who comes already knows things, can learn things and can teach things; Doing things ‘with’ each other, rather than ‘for’ or ‘to’ each other; Personalised goals—led by the needs of participants rather than an imposed agenda. A key finding was the importance of developing post-diagnostic programmes as a ‘sandwich’, providing a safe space for learning that is preceded by understanding pathways to access the programme and followed by explicit consideration of the next steps in increasing social engagement.
Keywords
Background
Post-diagnostic support is the cornerstone of dementia care in the community and much of this relies on social engagement through support groups and peer networks (Bamford et al., 2021; Levin et al., 2018; Mansfield et al., 2022; Wiersma and Denton, 2016). However, not everyone welcomes this level of social engagement or can navigate the complexity of services. Despite advancements in policy and care, many people are ‘on the margins’ and not accessing existing services and support: ‘The evidence we have taken has made it clear that improving diagnosis alone is not sufficient: people living with dementia and their carers need appropriate post-diagnostic support throughout the rest of their life. We are clear that there should be no gap between receiving a diagnosis and providing both immediate support and planning longer-term care for someone with dementia. People with dementia and their carers should not be left to fall through the cracks of an uncoordinated and complex pathway across the health and social care system.’ (UK House of Commons Health & Social Care Committee Inquiry, 2021 p. 21 p. 21)
In response to this unmet need, the ‘Beyond the Margins’ project aimed to develop and implement a Personal Development Programme (PDP) for people living with dementia. This programme became known as the GO programme (Getting On with Life). PDPs aim to place people in control of their own support, valuing the empowerment that can bring and acknowledging that there is no ‘one size fits all’ approach to defining and delivering support.
PDPs are known to be feasible and beneficial health/social care interventions for long-term conditions but have not been explored in relation to dementia (Quinn, Toms, Anderson, & Clare, 2016). However, self-management programmes in dementia have evolved over the last decade and evidence for the effectiveness of self-management interventions includes participants reporting: • Enjoyment and benefits (Martin et al., 2015) such as anxiety reduction (Clare et al., 2019; Mountain et al., 2022); • Increased confidence and self-efficacy, (re)engagement in activities, fun and friendships (Sprange et al., 2015), • Enhanced self-management techniques (Toms et al., 2015), • The potential to bridge the “care gap” often experienced in the early stages of dementia (Martin et al., 2013), • Empowerment of people living with dementia, fostering independence, reciprocity and the desire for social support (Clare et al., 2019; Mountain et al., 2022; Quinn, Toms, Jones, et al., 2016), • Cost effectiveness (Laakkonen et al., 2016).
The development of the GO programme builds on recommendations to work with people living with dementia to co-produce and identify the most appropriate outcomes to test efficacy (Mountain, 2017; Mountain et al., 2022) and qualitative process evaluations (Clare et al., 2019; Quinn, Toms, Anderson, & Clare, 2016). Also recommended are the integration of self-management interventions into care pathways (Quinn, Toms, Jones, et al., 2016) and research that measures change in social support and networks (Mountain et al., 2022; Sprange et al., 2015).
With these recommendations in mind, the GO programme built on four prior strands of work by the project team: 1. ‘Give and Take’—National Institute of Health funded research in the UK, which demonstrated that people living with dementia have information and experiences to share with others (Clarke et al., 2011). 2. ‘Talking Dementia’—Economic and Social Research Council funded research in the UK, which developed methods of working with people with dementia as co-researchers and developed a model of relationship-based care (Clarke et al. 2018, 2020, 2020). 3. ‘Taking Control of our Lives’—Canadian Institute of Health Research and Alzheimer’s Society of Ontario funded research (Hickman et al., 2015; Wiersma, Mcainey, et al., 2016), which developed a programme for people with dementia that was underpinned by adult learning principles, recognising that every person engages as a learner, teacher and knower (Vella, 2008). 4. ‘A Good Life with Dementia’—a programme developed by Innovations in Dementia.
This groundwork was used as a starting point in developing the GO programme content and approach, a critical aspect of which was the focus on the person living with dementia and their involvement, whilst recognising the important role of care partners.
Research Aims
• To refine, in collaboration with people living with dementia, the format, content and sustainability of a programme for people on the margins of support. • To deliver the programme on four occasions, focussing on a process evaluation of the intervention by the participants and facilitators. • To prepare the organisational environment and resources of the programme to facilitate its spread and sustainability.
Research Design
An action research approach was central to the research process, locating action as rooted in social relationships and optimising collaboration and action. The research team included a member living with dementia and we worked closely with many other people living with dementia as co-researchers as well as research participants. In total, the research worked alongside 40 people living with dementia and 26 family carers as well as 31 health and social care practitioners.
The Donabedian model of structure, process and outcome (e.g., Heckman et al., 2016) was used to identify key features of implementation to ensure that the GO programme was optimally developed, refined and implemented. Horton et al. (2018) suggest that the spread of innovations depends on codifying interventions in ways that support ‘adopters’ to adapt them to their own environment e.g., identifying the core key ingredients to making the intervention work and scope for adaptations. Horton et al. (2018) describe the importance of a ‘loose’ description of an intervention where the focus is more on the adopters’ ability to formulate their own versions of the components appropriate to their own setting, and responsive to the participants’ needs.
Phase One
Phase One focussed on the development of the PDP - it’s content and its mechanisms for delivery and sustainability. Key research and implementation questions asked in Phase One were: • What factors will hinder or enhance engagement with people ‘at the margins’ in participating in the PDP? What are the pathways of engaging people as PDP participants? • What factors in the environment will enhance the PDP? • How are people with experience of dementia optimally supported as co-facilitators? • What ways will best communicate the key messages of the PDP? • How does the PDP interact with existing services and support activities, and how can we ensure that it complements rather than competes with these to optimise sustainability?
Ethical approval was granted by the University of Edinburgh Research Ethics Committee to recruit people living with dementia with capacity to consent and non-NHS staff. HRA and local Research and Development Approval was granted to recruit NHS staff (REC reference 19/HRA/2782).
Phase One Data Collection
Over a 9-month period, a series of six in-person co-production workshops were run with three groups of people living with dementia. The purpose was to explore post-diagnostic support in relation to: a) Structure (e.g., factors in the immediate environment that are important to consider), b) Process (e.g., ways of engaging those ‘on the margins’) c) Outcome (e.g., the learning objectives of the PDP).
Firstly, eight people living with dementia and two care partners participated in a series of six workshops. Workshops were audio-recorded and detailed notes kept when the group worked in sub-groups. The topics covered in the six weeks are shown in Box 1.
Box 1. Phase 1 Co-Production Workshop Topics
Workshop one: Building relationships and explaining the research. Workshop two: Understanding pathways to engaging in post-diagnostic support. Workshop three: Understanding the different roles people living with dementia play in groups and the factors which enable these roles to be taken (e.g., facilitation styles). Workshop four: Developing potential content of a PDP programme. Discussion of readability of materials, accessibility, visual impact and messaging. Workshop five: Understanding what shows that support after a diagnosis has been successful. Workshop six: Understanding how best to engage people after a programme ends.
Secondly, a further three workshops were run with two groups to achieve greater clarity and depth of the topics above, involving 15 people living with dementia and 11 care partners in Scotland and England. Data extracts from the first series of workshops were used to prompt discussion and all of the workshops were digitally recorded and transcribed.
These groups were pre-existing peer groups of people living with dementia rather than formed solely for the purpose of this research. As a result, there were established group dynamics and all participants were known to each other. This benefitted the research because people felt comfortable and had a sense of security with each other, though it may have meant that some concerns were well-rehearsed in the group leading to some ‘group-think’. Participant engagement was maximised by using ‘I Want To Speak’ cards, name badges, and a mid-workshop break. Communication and enabling people to keep track was supported by using visual prompts and writing on paper tablecloths to visually record participant comments. All groups were reimbursed for their time by payment to group funds in accordance with guidance for Public Patient Involvement in research https://www.nihr.ac.uk/documents/centre-for-engagement-and-dissemination-recognition-payments-for-public-contributors/24979.
In addition, 11 interviews with community, voluntary sector, health, and social care staff were undertaken. The interviews focussed on current locality services, pathways of identifying and recruiting potential programme participants, and possible outcomes of the programme such as added value in relation to existing services.
Phase One Data Analysis
All interviews were transcribed, and all workshop notes and transcripts were reviewed and discussed in monthly research team meetings. The qualitative software package NVivo (www.qsrinternational.com) was used to assist data coding. The analyses were used to develop the content of the seven-week GO programme and the guide for facilitators and to inform the recruitment pathways in Phase Two.
At the end of Phase One, the UK went into the first national lockdown because of the pandemic. As a result, the GO programme was developed as an on-line programme. Moreover, everyone suddenly became ‘beyond the margins’ of being able to access post-diagnostic support.
Phase Two
During Phase Two, over a 20-month period (including a no-cost extension because of the pandemic), the GO programme was implemented with four groups of people living with dementia across the NE of England. Key research questions asked in Phase Two were: • How effective was the pathway of engaging people as PDP participants in identifying, recruiting and retaining participants? • How do the participants and the facilitators describe their experience of the PDP in relation to the environment and the content and the tools of communicating those messages? • What do people feel they have learnt by participating in the PDP, and how have they used this in furthering personal outcomes in their lives? • How do the participants and the facilitators describe the distinctive contribution of the PDP within their lives, and where does it duplicate other activities and messages?
The GO programme was delivered four times via Zoom by two facilitators employed by Innovations in Dementia with a total of 15 people living with dementia. Participants were not members of a pre-existing peer group and were mostly unknown to each other prior to the GO programme. They were nominated for the programme by service providers and community networks, including the DEEP and dementia research networks.
The inclusion criteria for research participants to take part in the GO programme were as follows:
People With Dementia
• Diagnosis of dementia • With or without capacity to consent to a seven week programme participation and evaluation • If without capacity to consent, has a consultee who can provide consent on their behalf • Speaks English • Be able to access a weekly session either online via Zoom or by telephone or contribute and receive information via telephone/post for the facilitator to feed into the group.
Care Partner of a Person With a Diagnosis of Dementia
• Care partner of a person with dementia who is participating in the seven week programme • Be able to access a weekly session either online via Zoom or by telephone/post for the facilitator to feed into the group • Speaks English
GO programme facilitators liaised directly with prospective participants so that they had one point of contact. This was to reduce any confusion resulting from different members of the research team being in touch. Participants were sent an information sheet, including a summarised version, and consent was recorded verbally using digital technology.
This paper focuses on data collected on the processes which were used to develop the GO programme through cycles of action and reflection and further action and evaluation and to codify the approach to facilitation.
The NHS Health Research Authority Oxford C REC (Ref 20/SC/0023) granted ethical approval in February 2020 with approval for a non-substantial amendment to deliver the programme online granted in May 2020. NHS Research and Development approval was granted for recruitment through NHS routes.
Phase Two Data Collection
The following data was collected in each of the four deliveries of the 7-week GO programme: • Fieldnotes from researcher weekly meetings with facilitators (total of 28 meetings), • Weekly reflections by facilitators on processes and individual participants’ issues (two facilitators at each of the 28 sessions), • Fieldnotes from observations of recorded weekly GO programme sessions (28 sessions in total).
Phase Two evaluation data (which is not presented in this paper) included video recordings of 14 evaluation interviews at week 7 and at three months post programme.
Phase Two Data Analysis
It was through this iterative process of writing fieldnotes and reflection with researchers and GO facilitators that an understanding was gained of the processes of engaging people in the GO programme, the day-to-day running of the programme, and issues that needed to be changed between the first two rounds of running the programme and the second two rounds. As such, the writing of fieldnotes is indistinguishable from analysis as the process of writing these identified gaps and issues to be followed up as well as contributing to the process of sense making (Sanjek, 1990). The fieldnotes and reflective notes were all archived in NVIVO.
Phase Three
The aim of the 4-month Phase Three was to prepare the organisational environment and resources of the GO programme to facilitate its spread and sustainability. In keeping with the participatory design of the study, the researcher team worked with co-researchers living with dementia to refine the GO programme.
Key research and implementation questions asked were: • How can the GO programme processes and resources be optimally developed for adoption beyond the life of the Beyond the Margins project? • How are localities optimally prepared for introducing the PDP: relationship with other supports in the area, optimal environments and facilitator preparation, and pathways of engagement?
Ethical approval was granted by the Sociology Research Ethics Committee, Durham University (Reference: SOC-2021-07-20T14_54_22-mqnt16).
Data Collection
Eight people living with dementia were invited to take part as co-researchers. Each co-researcher was remunerated with vouchers at a rate of £20/hour for their time and expertise.
The eight co-researchers worked together in two groups of four, each group meeting three times on Zoom, and facilitated by two members of the research team. Sessions were video-recorded, and detailed notes taken by the researchers. Six of the co-researchers living with dementia had taken part in either Phase One workshops, or as participants in the GO programme in Phase Two and therefore had prior knowledge and familiarity with the GO programme, making their analysis grounded in their experiences of the project.
Short vignettes were written of issues from Phase Two to capture the themes and questions in an accessible way. These were prepared for readability with input from two people living with dementia. Topics addressed were the role of care partners, enabling a safe emotional space online, navigating different types of relationships, talking about rights, and assessing the benefits of the GO programme.
The vignettes were used as the starting point for a discussion at workshops and were sent to all co-researchers by email and as hard copies in the post. In keeping with learning in Phase Two of the importance of preparing in advance to enable people to contribute to the best of their ability online, each co-researcher was offered a preparatory meeting the day before the workshop. Five of the eight co-researchers requested preparatory sessions, and these proved valuable during workshops with those who had trouble with memory or word finding as the researchers could support the individuals by prompting.
Data Analysis
Workshops were video-recorded and fieldnotes maintained. An agreed position on each of the topics addressed was reached with co-researchers during the workshops. Observation of video recordings of workshops and reading of fieldnotes taken during preparatory sessions were undertaken to check the conclusions reached during workshops for accuracy in relation to the issues being clarified.
Findings
The findings of the research presented in this paper focus on the structure and process of the development of the GO programme. These developed through interaction between the three phases of the research and include issues critical to the GO programme but that stretch beyond the programme itself, such as routes to engaging with such a programme and a non-existent ‘Week 8’ in which participants were encouraged to plan for what they would do after completion of the GO programme. We considered this as the GO Sandwich, with the work ahead of and following the 7-week programme being essential (Figure 1) The GO sandwich.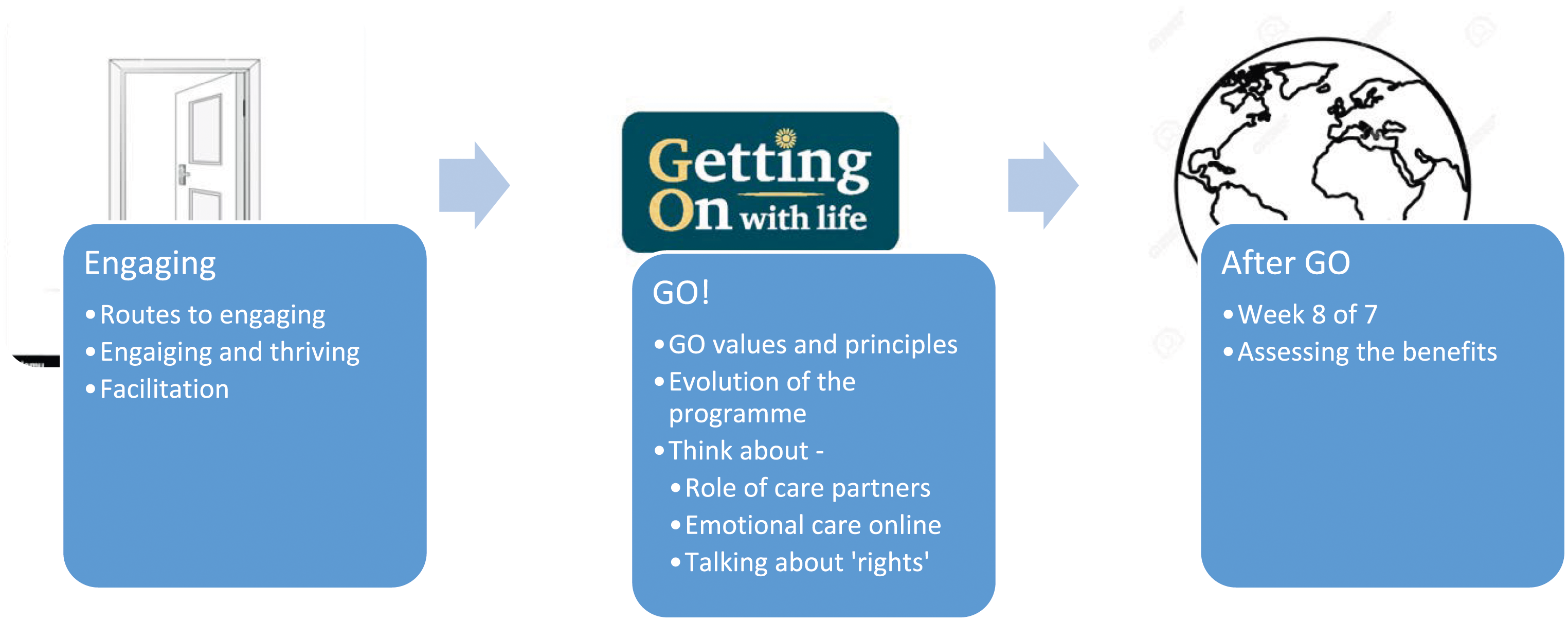
Participants were invited to be identified by a pseudonym or their own name and this is reflected in the following presentation of the findings.
Engaging—Routes to Engaging
In Phase One, participants identified key challenges in joining a post-diagnostic group and why many might be unwilling to do so. This included assumption of what a dementia group would be like. The reason I was reluctant to come to a group at the beginning was because I, like other people, imagined lots of people just sat in a room at the end stages, so I didn’t want to be part of that. It was very difficult to step through that door the first time. When you don’t know what is at the other side of the door. (Sandra – living with dementia, Phase One)
Serendipitous ‘bumping into’ encounters were a common way that people found their way to getting support. Suggestions for overcoming this included the grassroots mobilisation of people living with dementia who have a role to play at the beginning of the dementia care pathway, such as people in memory clinics who could invite participation in post-diagnostic support. If somebody phoned and said to me “come along”, I would quite happily do that…I bumped into (group facilitator) and she said “come on, we’ll go for a coffee”. And it was just then, I thought, right, I’ll start coming to the meetings. (Betty—living with dementia, Phase One)
Engaging—Engaging and Thriving
Participants identified a tension between ‘just get on with your life’ after diagnosis and the losses associated with dementia, signalling the importance of the GO programme to reflect and respect the range of emotions that people might be experiencing. Actually sometimes it’s impossible to just get on—.She can’t drive, that’s a massive impact on our lives, on everything, so dementia has really…perhaps we are still both grieving.’ (Abbey—care partner, Phase One)
Acknowledging and working with this tension was critical to whether people engaged with support. I have had a couple who have asked me to go [to other dementia groups] but I have declined because I had heard that you don’t come away feeling better. You come away learning about problems rather than getting encouragement. (Mark—living with dementia, Phase One)
Engaging—Facilitation
Preparation by facilitators and participants in advance of commencing the GO programme was essential for it to be successful in achieving its values and principles. At least three weeks were required to prepare participants to take part, to support people to access Zoom sessions, to consider personal goals and to build relationships with facilitators so that the facilitators could provide bespoke support to enable people to engage to the best of their ability. For example, the facilitators learned how to support those with word finding difficulties by bringing them into the conversations with gentle prompts. The facilitators made individual calls between weekly Zoom sessions to follow up on any issues and prepare the participant for the following week.
GO!—Values and Principles
People living with dementia told us that an enabling approach which sees the potential in each person rather than focussing on problems is preferred and is key to encouraging people to engage and flourish. Therefore, in Phase One, we developed a set of values and principles to guide the facilitation of the GO programme (see Box 2).
Box 2. GO programme Values and Principles
• Everyone who comes already knows things, can learn things and can teach things • Doing things ‘with’ each other, rather than ‘for’ or ‘to’ each other • Personalised goals – led by the needs of participants rather than an imposed agenda
• A good welcome • Have fun but we need to be serious about some things too • Allowing us to express emotions and grief for the things we have lost • Everyone helps each other
• Don’t treat us like children • Don’t talk over us • We’ve got dementia but we’ve got a life to live • Friendliness, and being accepted as we are, are the most important things – no judgement • Sessions need to run in a way that enables everyone to contribute • Time for talking and asking questions
GO!—Evolution of the Programme
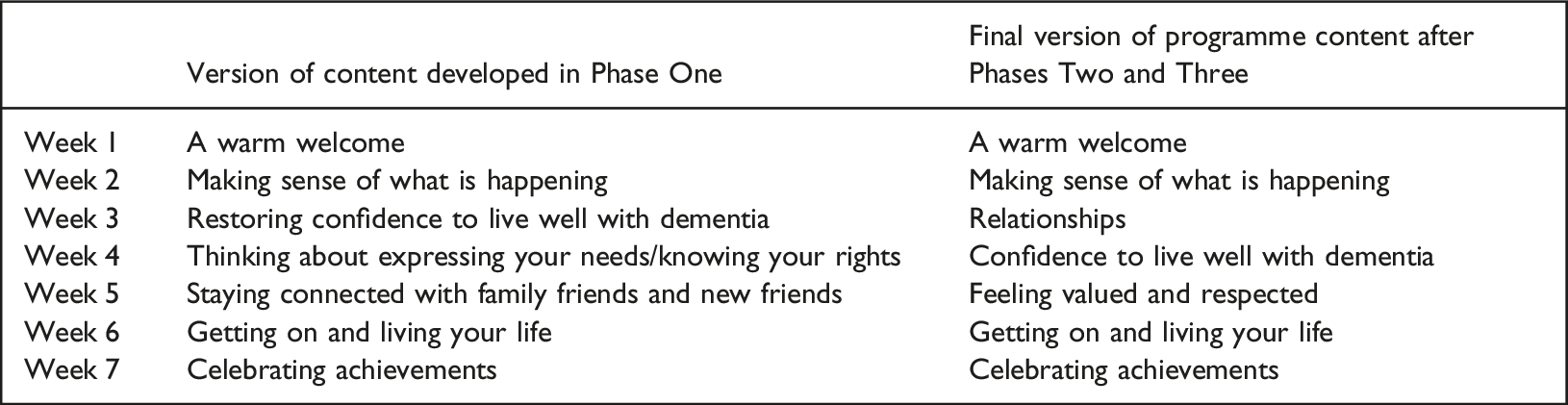
The workshops of Phase One developed the weekly programme content of the GO programme, which was refined during Phases Two and Three (see Box 3).
Weekly guest appearances of people living with dementia were a key ingredient. Guests shared their experience of how they have adjusted to a diagnosis and this peer support was transformational for some of the participants. Guests were identified by the facilitators through Innovations in Dementia networks.
GO!—Role of Care Partners
There were a number of complex issues that were considered and reflected on alongside people living with dementia in the refinement of the GO programme—one such issue concerned the role of care partners.
Co-researchers in Phase Three agreed that the voice of the person living with dementia was central during the weekly online GO programme sessions and that they should be free to speak. Having a care partner on screen could be an added distraction but was also identified as sometimes necessary and helpful so long as it was managed through good facilitation (see Box 4). We want to hear what the person with dementia has got to say but sometimes they do need their partner. So, in order to get the whole of what the person wants to say they do need their partner and so does the group, otherwise the group won’t hear what the person with dementia has got to say. (Jacqui—living with dementia, Phase Three)
Box 4. Steps to including care partners on screen
• Preparation—ensure that at the outset the care partner understands that the focus is on the person living with dementia and the aim is to support them to have their say. • Explain in advance to other participants that a care partner will be present on screen in a supportive role. • The care partner should sit slightly behind the person living with dementia when on screen so that visually the focus is on the person living with dementia. • Facilitator uses the person living with dementia’s name when inviting them to speak. • Care partner holds up a yellow ‘I Want To Speak’ card and only speaks when the facilitator invites them to do so. • If the care partner is speaking too much, the facilitator needs to step in and ask them to allow the person with dementia to speak. • There should be no conferring out loud between couples. When the care partner and the person with dementia want to speak with each other they should show their yellow card to each other and then mute Zoom. The facilitator needs to make the decision about whether to wait for them or move the conversation on. • It is acceptable for the facilitator to use their authority to mute a couple who are talking to each other on screen. The noise can be difficult, especially if some participants experience hyperacusis (sound sensitivity). • Care partners may be unaware that they are taking over. The facilitator’s role is to raise their awareness and therefore asking them to stop talking and allow others to speak is acceptable. • If a facilitator is inexperienced, they should shadow an experienced facilitator and practice through role play with an experienced facilitator.
Care partners played a vital role off-screen too: • Supporting people to get online and join a Zoom call, • Supporting the person with dementia afterwards with difficult emotions raised by the discussion and their memory of the discussion, • Giving their perspective on how the person with dementia is benefiting from the GO programme, • Providing a sense of security when the person living with dementia is meeting new people,
It can also be useful for care partners to see a group of people interacting, supporting each other, and sharing experiences: ‘Even today I’ve noticed (my wife) was thinking more for herself with me off screen’ (Colin - care partner, Phase Three).
The GO programme is designed specifically for people living with dementia but supporting care partners is clearly central to this. In future delivery of the programme, we recommend some additional strategies for supporting care partners as an integral part of the GO programme: • Run at least one separate session where care partners can meet together and share contact details, if they wish, for ongoing peer support, • Be aware of local support for carers and signpost, • Encouraging care partners to continue to engage with activities they enjoy was felt to be important by people living with dementia as a strategy to lift any sense of despair and hopelessness and bring some joy, • Refer couples to other supports to address deeper relationship issues in relation to dementia.
GO!—Emotional Care Online
One of the core principles identified in Phase One was of providing a safe space to allow (and perhaps expect) the expression of emotion including sadness. The week about relationships, in particular, raised emotional issues for participants. There was a recognition that it is acceptable to speak about emotions and it is not something facilitators should be avoiding. It was the facilitator’s role to create an atmosphere of comfort and belonging for everyone, irrespective of varying ages between participants and that some participants may live alone and without a care partner. Nobody is going to judge…everybody is going to be sympathetic because we have all had some problems of some kind that we have had to contend with. (Anita – living with dementia, Phase Three)
There was a consensus that people living with dementia are the best people to support others as they understand what they are going through, and people will open up to each other as a result. The facilitators gently bring in other participants when someone is upset, asking if there is anything anyone would like to say that would support the person with their issue. Jacqui explained why she felt more comfortable on Zoom than face-to-face meetings: Zoom for me is a safer place than face-to-face because if I get upset on Zoom, I can leave the meeting if it’s so bad I want to go and have a good cry. Or I can get support from the people on the Zoom meeting because they will be people who understand and are patient and get what I’m feeling so I’d be very happy with that. (Jacqui—living with dementia, Phase Three)
These discussions with co-researchers indicated that there was nothing inherently unsafe about expressing emotions in an online space. An online environment can be created where it is safe to express difficult emotions and be supported by others in a way that is helpful in adapting to a diagnosis of dementia. In the preparatory stages, facilitators can explain how the person living with dementia will be supported during and after the sessions since some of the discussion may be emotional. The preparation period is also the opportunity for facilitators to identify any issues that might be emotional for each person. If someone becomes emotional on the Zoom call, a facilitator needs to follow up with a phone/Zoom call, but the second facilitator may need to make the call and support them one-to-one during the session. Box 5 outlines the steps to creating an emotionally safe space online.
Box 5. Steps to create an emotionally safe online space
• Preparation—weekly preparatory sessions are important for anticipating and preparing for emotional issues that may arise when online and reassuring that there is no shame in sharing emotions. • Active listening to ensure the person feels heard • Acknowledge the emotion, don’t ignore it • Body language—lean forward. • Gently bring other participants into the conversation so they can support the person—people living with dementia are the best people to support others with dementia. • Pause and ask the person who is upset or who has shared something painful if they would like to take a break. • Offer a phone call right away from the co-facilitator. • Finish the session on a positive or light-hearted note. • Follow up after the session with a phone/Zoom call.
GO!—Talking About ‘Rights’
During Phase Two of the project, dementia ‘rights’ was difficult for participants to grasp and this was explored further with co-researchers in Phase Three. Participants often spoke about dementia as a condition that ‘you can’t see’ and understanding dementia as a disability was what they thought of when talking about rights. If facilitators speak more explicitly about dementia as a disability this might be helpful. For example, if someone is in a wheelchair, it is their right to have access to buildings made easier for them. Similarly, it is a person living with dementia’s right to have things that are made difficult by dementia made easier for them. We do have rights to have things made easier for us, for example, written information. (Jacqui—living with dementia, Phase Three)
However, using the word ‘rights’ was seen as problematic: ‘Rights can be viewed negatively, and people get fed up hearing it.’ (Paul—living with dementia, Phase Three)
Navigating ‘having your rights met’ was complex and in the GO programme the preferred term was ‘being valued and respected by others’ (Reilly et al., 2020). While co-researchers saw the issue of ‘rights’ as important, there was some discomfort which indicated that sensitivity is required to avoid making people feel burdensome or guilty when their families do a lot to help them. I don’t want people to think ‘oh no here she comes’. This makes me stay quiet sometimes when people give me more help than I feel I sometimes need. I stay quiet as I don’t want to offend them.’ (Barbara—living with dementia, Phase Three)
After GO—Week 8 of 7
Participants spoke of what would happen after the programme ended and the importance of it leading onto something else. As a result, the GO programme was explicit in having a (non-existent) ‘week 8’, which was the first week post-programme. If it is a good course, it depends on the tutor of course. I find it puts me further into what it’s all about. We find out there’s other groups, it just seems to expand, we all become one big family. You learn more and more about it. (Eddy—living with dementia, Phase One)
After GO—Assessing the Benefits of the GO Programme
Co-researchers advised that getting to know people before the GO programme starts is key to knowing if it benefits them. Here, Billy urges a focus on feedback from participants: The people that will tell you whether it’s good or not are the people who are on the programme, because you review with them, how did that work for you? Would you rather have had …and then you improve and you improve and you improve. (Billy—living with dementia, Phase One)
While it was felt that the person living with dementia was the most important person to ask about benefits of the GO programme, it was agreed that asking care partners also has a place, although with some caveats: Carers can’t speak for me. As a patient, I want my voice to be heard with them backing me up. A carer can’t speak for me. They can speak about me. That makes the difference. They can see how my moods change. And the wider perspective. They can certainly have a very big role to play. (Michael–living with dementia, Phase One)
Some indicators of success were considered to be signs of people looking after each other and becoming ‘like family’ and changes in what people are doing, such as being more confident to tell others about dementia. I came off (Zoom) every DAY feeling that I’d achieved something, feeling uplifted, feeling energised, and just feeling so happy. I feel sort of more, I don’t know, part of the world. (Sophia—living with dementia, Phase Two)
Discussion
The far-reaching effects of the global pandemic have shaken the lives of people across the world, and this project is no exception. The original proposal focussed on those people living with dementia ‘on the margins’ which we defined as those not accessing existing services and support. The pandemic and the closure of all face-to-face support within the statutory sector, the third sector and peer networks during lockdowns, meant that those living with dementia who could be classified as ‘on the margins’ expanded dramatically in ways which could not have been foreseen at the outset of this project. Our understanding of ‘on the margins’ has changed and shifted throughout the project.
The rapid switch to online communications created new barriers but also new opportunities for reaching those on the margins not accessing support. Digital equity is important so that new barriers are not erected for people living with dementia - not everyone has access to laptops/tablets or wi-fi or a care partner who can support them to log on so some people will be excluded from online approaches. Giebel et al. (2021) found that online support groups can be helpful for some but often not those with more advanced dementia or visual problems associated with some types of dementia. On the other hand, Talbot and Briggs (2021) in an interview study with people with dementia during the pandemic found that for some people living with dementia, staying at home because of COVID restrictions reduced the anxiety of venturing into the outside world, gave them a break from the stresses of everyday life and provided opportunities for achievement. Liu et al. (2021) suggest that further research is needed to assess the success of remote interventions for people living with dementia to improve well-being.
Essential to translating research into practice is knowing the barriers and facilitators to promoting change in behaviour (Zapka et al., 2004) including a clear understanding of the influences on human behaviour and the contexts in which they can occur (Atkins et al., 2017). Döpp et al. (2013) suggest that resolving possible individual and organisational barriers should be a precursor to programme implementation. In developing the GO programme through the Beyond the Margins project, the different stages of creating and implementing the programme have been described and analysed. This is consistent with Zapka et al.’s (2004) recommendation that the following should be considered: the programme conception and its organisational context; the planning and implementation process; the participation of the providers and the interactions of all concerned throughout the process of implementation; the impact and the outcomes of the programme. Careful and multiple ways of evaluating the process and the outcome are also essential as failure can occur at any level: conceptual, implementation or evaluation (Zapka et al., 2004). Peters et al. (2013) comment that the effects of changes over time, the complexity of systems and unintended consequences of an implementation should also be considered.
In addressing these considerations, the Beyond the Margins project has worked together with people living with dementia (as co-researchers involved in part or all of the project and as participants in the GO programme) to develop an evidence base of approaches to evaluating the GO programme that reflect its learning outcomes in relation to: empowerment in action, identity, communicating with confidence, resilience strategies, wellbeing and getting the most out of life. Co-production with people living with dementia gives the GO programme a strength and distinctiveness, including specific guidance on avoiding harms, identifying priorities and strategies to improve health outcomes in the online environment (as advised by Hrincu et al., 2021). Through detailed analysis of the processes of running the programme, we codified the approach to facilitation by embedding it in the underlying values and principles (Box 2). Fidelity to our approach to facilitation, and particularly the underlying values and principles, is crucial and is enabling scalability while retaining flexibility in the weekly content which is responsive to the needs of those participating.
At the service delivery level, the GO programme can be commissioned locally and delivered by anybody who works with people living with dementia who adheres to the values and principles of the programme. A range of organisations are developing and delivering courses for people living with dementia, for example Recovery Colleges (Lowen et al., 2019) and our partner organisation Innovations in Dementia. The GO programme is continuing to be implemented through AgeUK. The GO programme facilitator’s manual can be accessed at: http://www.innovationsindementia.org.uk/resources/our-publications/. If it is tailored to what local support is available, it will ensure fewer people fall through the net of service support. It could enhance the support that is currently provided and provide a different way of working.
One of the key organisational routes to implementing the GO programme is social prescribing, which is the practice of linking patients in primary care with support within their community to help improve their health and wellbeing (Bickerdike et al., 2017). In recent years, it has been widely promoted to enhance social inclusion and community wellbeing (Chatterjee et al., 2018), although referral mechanisms, target groups, range of activities, and intensity and duration of support may vary (Drinkwater et al., 2019). Social prescribing is specifically targeted at people who require a greater level of social and emotional support than is available through routine care, such as people with long term physical and mental health conditions, as well as frail and older people. Though robust evidence regarding its success and cost effectiveness is lacking, most current evaluations of social prescribing point to positive results (Bickerdike et al., 2017). Several of the professional people we interviewed during Phases One and Two of this project believed referrals to the GO programme could be embedded in the services of social prescribers. Referral to a social prescriber delivering the GO programme could also take place within memory clinics.
Strengths & Limitations
One of the key strengths of this research is that people living with dementia were involved at every stage of development of the GO programme, which means it can make a distinct contribution to the post-diagnostic support landscape. The multi-phase and multi-method research design provides strength through the triangulation and reflexive considerations of each aspect. The programme has been developed as a ‘loose’ intervention (Horton et al., 2018), allowing it to be adopted and adapted for local circumstances and needs but providing a very clear set of values and principles and ways of working.
The limitations of the research arise from the need to adapt to the pandemic part-way through the project—though we hope that we have made a virtue of necessity and been able to produce a programme and associated facilitator guide that is able to be adapted between being in-person and on-line. Recruitment into Phase Two was challenging during the pandemic and we would have preferred to have recruited a larger sample and one with more cultural diversity.
Conclusion
The Beyond the Margins project has led to the development of the very innovative GO (Getting On With Life) programme for people living with dementia. Importantly, the programme is best understood as not a stand-alone programme but as the middle of a sandwich of support, in which attention is given to the routes and facilitation into joining peers on the programme and the explicit attention given to what happens following the end of the programme. The programme is a launchpad into another stage of engagement for people in their lives despite a diagnosis of dementia.
Footnotes
Acknowledgements
We are extremely grateful to all of the people living with dementia who contributed in a variety of ways to the research, and to all of the care partners who played an important part in enabling this. Activism comes in many forms but everyone has played a part in shaping the next steps in this programme of work. We also thank the many health and social care practitioners who contributed their time generously.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ‘Beyond the Margins’ project was funded by the Alzheimer’s Society.
Ethical Approval
All aspects of this research have secured the necessary ethics and governance approvals: Phase 1—Ethical approval was granted by the University of Edinburgh Research Ethics Committee to recruit people living with dementia with capacity to consent and non-NHS staff. HRA and local Research and Development Approval was granted to recruit NHS staff (REC reference 19/HRA/2782). Phase 2—The NHS Health Research Authority Oxford C REC (Ref 20/SC/0023) granted ethical approval in February 2020 with approval for a non-substantial amendment to deliver the programme online granted in May 2020. NHS Research and Development approval was granted for recruitment through NHS routes. Phase 3—Ethical approval was granted by the Sociology Research Ethics Committee, University of Durham (Reference: SOC-2021-07-20T14_54_22-mqnt16).