
Abstract
There is a need in South Africa to understand the status of available care and support to strengthen responses to dementia. This study provides a situational analysis of the current provisions of health, care and support for older persons, people living with dementia and their families in South Africa. It is a first step towards describing the landscape of needs and services available, and provides an evidence base to inform priority-setting for strengthening responses to dementia in South Africa. This situational analysis was conducted in three phases: (1) a desk review guided by a comprehensive topic guide which includes the WHO’s Global Dementia Observatory indicators; (2) multi-sectoral stakeholder interviews to verify the secondary sources used in the desk review, and to identify gaps and opportunities in policy and service provisions; and (3) a SWOT-analysis examining the strengths, weaknesses, opportunities and threats in current care and support provisions in South Africa. Our findings highlight the gaps and opportunities with current service provision and show how structural factors create barriers to diagnosis, support, and care. There is an urgent need for intersectoral policy responses to support and strengthen current health, social care, and long-term support systems so that people living with dementia and their families can live and age well. This paper forms part of a larger study on strengthening responses to dementia (The STRIDE project).
Keywords
Background
In South Africa, there is a need for evidence to understand the landscape of available care and support for older persons, people living with dementia and their families to strengthen its responses to dementia. Despite limited or absence of regional and national data, the Global Burden of Disease (GBD) forecasts a 181% increase in dementia prevalence between 2019 (241 937) and 2050 (680 045) for South Africa (Nichols, 2022). As populations age and people live longer, the need for care and support increases as the prevalence of chronic conditions increases. Older persons in South Africa are defined as 60 years and older and comprise 9.15% of the population (i.e. 5.5 million people) (StatsSA, 2021), and projected to increase to 15.4% in 2050 and 27.8% in 2100 (United Nations, 2015). With competing public health concerns and social care priorities such as HIV/AIDS, gender-based violence (GBV) and limited early childhood development services, dementia and long-term care (LTC) for older persons have not received adequate attention in South Africa. The lack of research and policy focus on geriatric health and dementia (Lloyd-Sherlock, 2019) has significant consequences for health and social care system preparedness. There is a growing need for culturally appropriate responses to support ‘ageing-in-place’ or ‘active ageing’, promoting the protection and inclusion of older persons in daily living and decision-making at home and within communities (Jordan, 2009; WHO, 2002).
As a start to addressing these needs in South Africa, this study presents a situational analysis of existing provisions of health care, social care and support for older persons, people living with dementia and their families in South Africa. This situational analysis provides an evidence base to inform priority-setting for strengthening responses to dementia in South Africa. The STRIDE project includes a number of components of which the situational analysis is one of the first. The other components (not described in this paper) complement the data gaps, leading to modelling of human and financial resources needs for improving dementia care services.
Evidence for the situational analysis was generated via three phases: (1) a desk review guided by a comprehensive topic guide (Comas-Herrera, 2021) and including WHO’s Global Dementia Observatory indicators (WHO, 2017); (2) multi-sectoral stakeholder interviews to verify secondary sources used in the desk review, and identify gaps and opportunities in policy and service provisions; and (3) a Strengths, Weaknesses, Opportunities and Strengths (SWOT) analysis in current care and support provision for older persons and their families in South Africa. The purpose of this paper is to present key findings from these three phases, with an emphasis on the insights derived through stakeholder interviews.
Methodology
The STRIDE project, funded by the Global Challenges Research Fund GCRF)aimed to contribute to improving dementia care, management and support for people living with dementia and their families (see shttps://stride-dementia.org/).
Phase 1: Desk Review
A desk review was conducted following a detailed topic guide developed by STRIDE investigators. It covered ten 10 areas: (1) overall country context (population, demography); (2) health system; (3) LTC system; (4) policy context; (5) dementia awareness and stigma; (6) epidemiology and information systems for dementia; (7) the dementia care system; (8) unpaid care and other informal care; (9) social protection; and (10) dementia research (see Comas-Herrera, 2021). The topic guide also included WHO’s Global Dementia Observatory (GDO) indicators and resulted in a detailed, in-depth situational analysis of care and support arrangements for older persons in South Africa. The full situational analysis includes a SWOT-analysis to inform other dimensions of the (STRIDE project), modelling the current and future costs for each participant country (see www.stride-dementia.org/).
Evidence sourced for the desk review included official government policies, legislation and reports, country-specific statistical releases, academic peer-reviewed journal publications, grey literature, and institutional reports obtained through university and/or public repositories. The desk-review was additionally guided by an overall cross-country desk-review guide (Comas-Herrera, 2021). In cases where official sources were not available, we included media and organisational websites and available online resources.
Phase 2: Multi-stakeholder engagement
Phase 2 focused on multi-sectorial stakeholder consultations with key decision-making and topic experts, and experts by experience (i.e., people living with dementia and their carers). We conducted in-depth, semi-structured interviews with stakeholders from (a) the public healthcare sector; (b) the social care and support sector; (c) government officials; (d) civil society and non-governmental organisations (NGOs); (e) traditional healing; (f) the private LTC and support sector; and (g) people living with dementia and their carers.
Topic Guides
Semi-structured interview topic guides were generated separately for decision-making and topic experts and for experts by experience, a priori. Following completion of Phase 1, these topic guides were adapted for relevance to both the interviewee(s) and the identified gaps in the evidence base. Broadly, the interviews with experts by experience included questions about their experiences of and perspective on diagnostic and care services, social support and care, and elder abuse. Interviews with decision-makers and topic experts were tailored to their experience with and expertise on dementia, where questions broadly focussed on (i) health services; (ii) prioritisation concerning detection and management; (iii) data and surveillance; (iv) awareness and prevention; (v) LTC services; (vi) policy prioritisation, development, and progress; and (vii) elder abuse. The final topic guide(s) are available through the supplementary appendices.
Participant Recruitment
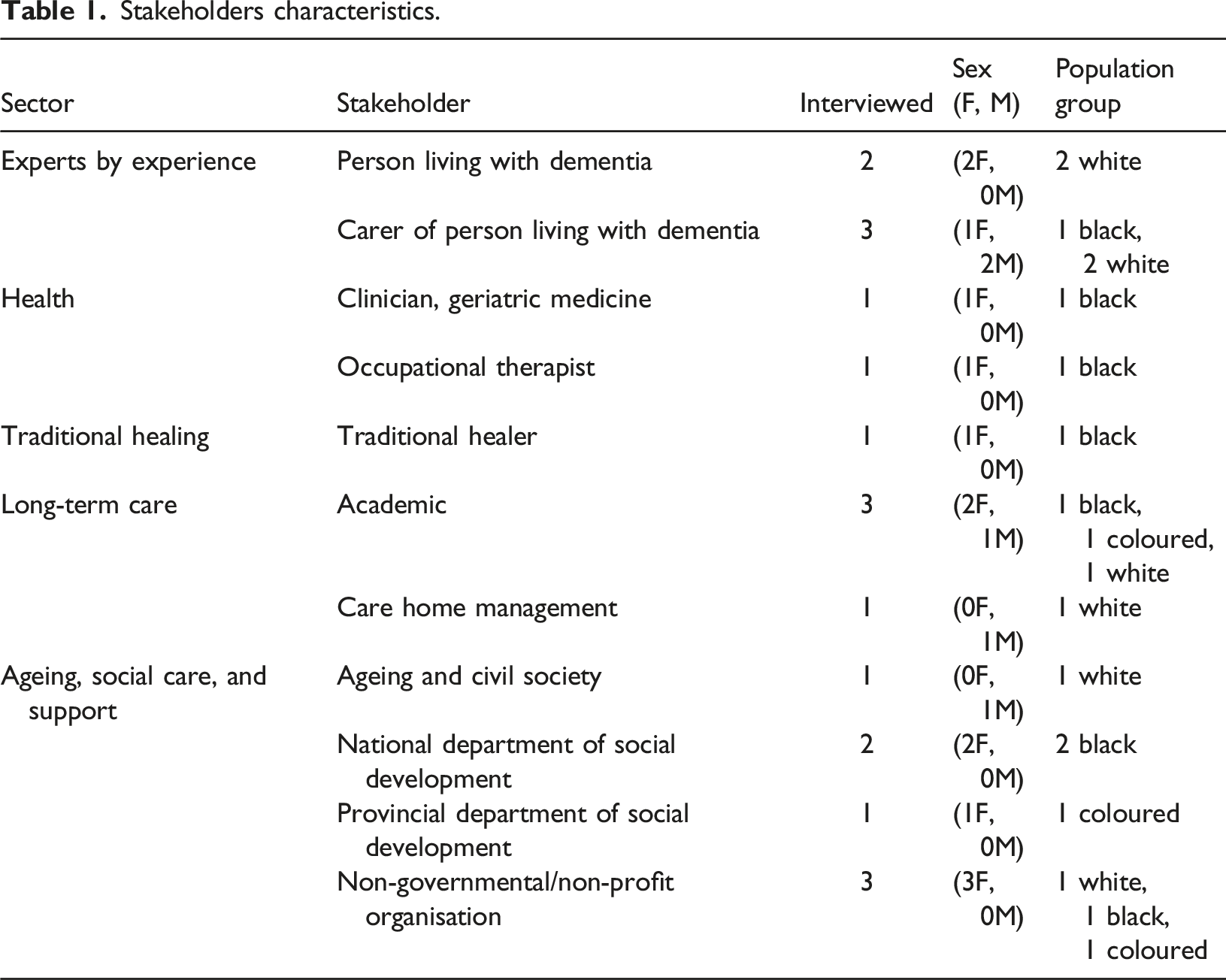
A total of 12 stakeholders were interviewed across six predefined sectors, namely health, social care, ageing and civil society, traditional healing, LTC, and experts by experience. We purposively selected stakeholders to include both national and provincial level officials, and across geographic regions. People living with dementia and their carers were included as experts by experience because they have personal experience in seeking help and accessing services and provide valuable insight to the experiences of dementia care service users. We recruited participants in collaboration with members of the STRIDE South African Advisory Group (SAAG) 1 or identified via information freely available on official government websites. We used snowballing techniques, asking enrolled participants to share our project information letter with their contacts. For inclusion, stakeholders were required to have a minimum of two years’ experience in their sector. Experts by experience were included if they had received a formal diagnosis of dementia or have been living with or caring for a person diagnosed with dementia for at least two years. While this sample of stakeholders was relatively small, the focus was on depth of information obtained rather than breadth.
Procedure
Stakeholders were interviewed virtually to accommodate COVID-19-related restrictions. Interviews ranged between 40 and 90 minutes and were led by one interviewer (RJ or MS) and either one or two co-interviewers (RJ, MS, PDT, or SD). One interview was done jointly because a person living with dementia and carer felt most comfortable to be interviewed together. Informed consent was obtained from all participants, with precautions taken to explain information letters and consent forms verbally, via a virtual platform. The consent process was documented either digitally (where both audio and visual recordings of the consenting procedure were transcribed verbatim and filed securely and separately to the interview content); or via signed consent forms returned to the researchers via email. Participants were provided the option of being interviewed in English, Afrikaans, or isiXhosa. However, all interviews were conducted in English, based on the language preference of the participants, with no translation required.
Analysis, Rigor and Reflexivity
All interviews were digitally recorded (audio and visual), transcribed verbatim for quality and analytic purposes, and entered into NVivo 12 (NVivo, 2022). Inductive thematic analysis was conducted to interpret the complexity and richness of the information collected, and sorted into dominant themes (Nowell, 2017; Thomas, 2006). The lead author analysed the transcripts following Braun and Clarke (2006)’s approach to thematic analysis, in the following steps: (1) familiarising with the data; (2) generating first-level codes; (3) identifying themes; (4) reviewing themes; (5) refining themes; and (6) generating the findings and report (Braun & Clarke, 2006). Our study employed various strategies that determine the validity of qualitative, inductive analysis such as peer debriefing, member-checking, triangulation and thick description (Creswell & Miller, 2000). The lead author led on the coding, with debriefing discussions with co-interviewers (MS, PDT, SD). Follow-up discussion with participants (member-checking) allowed for the validation of interpretations as well as enhancing the positionality 2 of participant insights, especially when presenting information on traditions, beliefs, and cultural practices (as researchers are situated outside of some of the cultural belief systems that participants described). This exercise (member-checking) was especially relevant where interviewers with participants could not be matched in terms of cultural background and we relied on the explanations of participants themselves to verify interviewer interpretations of beliefs and cultural practices. We include detailed narratives (thick description) to provide readers with an understanding of the context of the account and make decisions about the transferability of findings to other similar conditions (Creswell & Miller, 2000). In addition, we reflect on the cultural diversity of participants and their service populations. Most stakeholders interviewed in this study work within the public sector and reflect on their insights of working with culturally diverse populations, with whom they often share similar cultural backgrounds. Their insights therefore include the voices of historically disadvantaged groups.
Ethical Considerations
Precautions were taken by the lead interviewers (RJ and MS) to ensure participants living with dementia understood the purpose and expectations of the study (Lee, 2010), retained and engaged with the information to make a decision, and were able to clearly communicate that decision (Gilbert, 2017). People living with dementia and their carers in this study were existing service users of our NGO partner, Alzheimer’s South Africa (ASA). An ASA social worker, and co-author (PDT), provided support to participants with dementia and their carers during the interviews. No people with severe dementia and without capacity to consent were interviewed. Special precautions to de-identify stakeholder narratives were taken to protect the anonymity and confidentiality of participants and the specific organisations they represent. Participants are positioned in terms of the broader sector they represented.
Phase 3: SWOT-analysis
We performed a SWOT-analysis to further inform priority-setting, and identify weaknesses and threats to provide insight to managing risks that undermine priorities (Gurel & Tat, 2017). Four steps were followed: (1) collect data and information (desk review); (2) critically evaluate data and sort factors across the four SWOT components; (3) populate the SWOT matrix, categorising factors as they relate to the health system, LTC, economic context, political context, legal and social protection context, and cultural and societal context; and (4) incorporate inputs from the multi-stakeholder interviews (Docrat, Lorenz and Comas-Herrera, 2019bDocrat, Lorenz, & Comas-Herrera, 2019). Factors were listed in four-quadrant SWOT-tables.
Findings
Phase 1: Desk review findings
Healthcare System
South Africa’s health system is divided into two: the public and private sectors. The public sector offers free healthcare for 84% of the population (Mahlathi & Dlamini, 2015) who cannot afford private medical insurance and the out-of-pocket payments. Public health services are rationed by queuing systems and long waiting lists. Despite active redresses by government, the health sector is still characterised by unequal access to services and resources (including human, financial and technological), with an urban bias despite most of the population (64.7%) living in rural areas (Mahlathi and Dlamini, 2015; South African Government, 2017; Competition Commission SA, 2018). State sources estimate that rural populations are serviced by only 12% of doctors and 19% of nurses in the country (DOH, 2011), with an estimated 79% of physicians in the private sector (Rawat, 2012). Access to private medical care is contingent on having medical insurance, which few South Africans can afford (16%) (Mahlathi and Dlamini, 2015; StatsSA, 2019). Escalating private rates are the result of an unregulated pricing environment, lack of integrated care models and solo practices that incentivise practitioners to provide more services than needed through their own activities, and through referral for further investigations and hospitalisation (Competition Commission SA, 2018).
There are no dementia-specific services at the primary healthcare level, with fewer than ten geriatricians and five geriatric psychiatrists (Kalula & Petros, 2011) to serve the entire country of over 5.5 million older persons (StatsSA, 2021). The poorest South Africans live furthest from healthcare facilities (Mclaren, Ardington and Leibbrandt, 2013), with time and travelling costs to the nearest centre posing significant barriers to access and health (Fusheini & Eyles, 2016). Diagnostic pathways for dementia are weakened by common misperceptions amongst primary healthcare staff that dementia is a natural part of ageing, not requiring referral for further assessment, diagnosis and management of care (Jacobs et al., 2022; Kalula, 2010; Kalula & Petros, 2011). Therefore, most people living with dementia in South Africa remain undiagnosed and cared for without professional or other formal support. South Africa has standard treatment guidelines for the pharmacological management of dementia (DOH, 2020; Emsley et al., 2013), but the public sector has a general shortage of available pharmaceutical supplies (South African Government, 2017).
South Africa is a multi-cultural country with twelve official languages and a myriad of customs, beliefs, and practices. Traditional healing among some cultures is a way of life, with diseases, misfortune, and especially mental or emotional conditions understood as being social in origin (Mkhonto & Hanssen, 2018). Traditional healers often live amongst the people in communities, speak the local languages and provide a rich source of support for the whole family (Audet et al., 2017). Cultural beliefs play an important role in understanding dementia, where symptoms are often viewed with suspicion and fear, and where stigma sends families into hiding and avoiding help-seeking (Mkhonto & Hanssen, 2018; Mukadam & Livingston, 2012).
Social Care and LTC sector
Social care and support services, including LTC, vary greatly across South Africa. Access to LTC services is largely limited to those who can afford out-of-pocket payments as medical insurance companies do not support LTC and residential care services. Available LTC services (including home care, residential care facilities, respite care) are skewed towards the private sector with many being unregistered with the Department of Social Development as required (Mahomedy, 2017).
Community-based services for people living with dementia are limited and based within the NGO-sector, with two dementia-specific NGOs in South Africa: Alzheimer’s South Africa (national coverage), and Dementia-SA (Western Cape province). Government relies heavily on the NGO sector to provide psychoeducation and support to people living with dementia and their families, and to link service users to home-based care, counselling groups and legal advice. There are no nationally representative data available in South Africa on caregiving arrangements specific to dementia care, although a small study in Cape Town showed that 79% of persons living with dementia were cared for at home either by a spouse or an adult child (Kalula, 2010).
Policy Environment
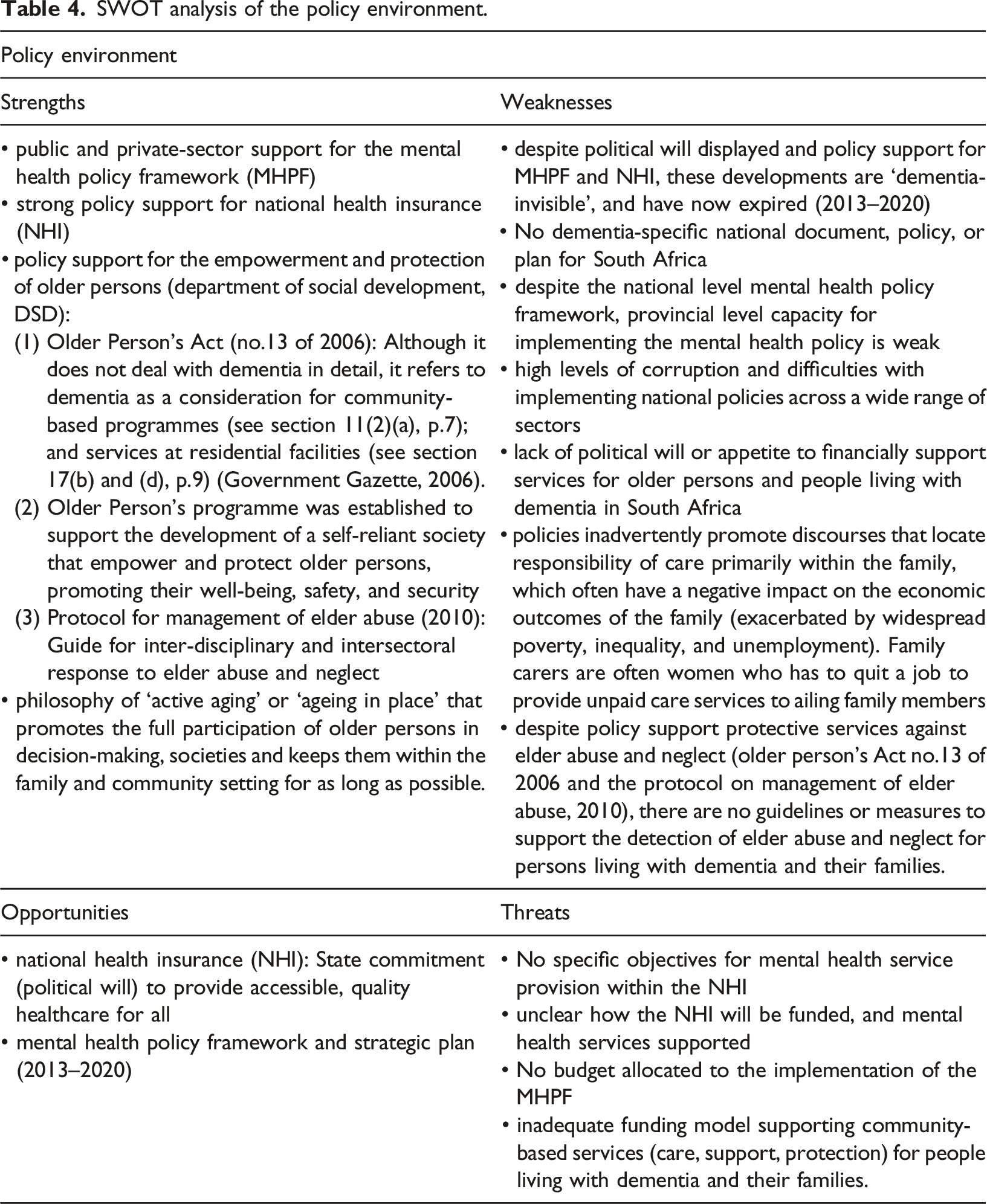
South Africa currently has no national dementia policy or health plan. The Department of Social Development (DSD) is the custodians of the Older Person’s Act (no.13 of 2006) that broadly promotes the rights, protection and care provision for older persons and ageing in general, while the Older Person’s Programme is responsible for coordinating services to older persons and includes awareness, educational and communication programmes, and residential care services (Jordan, 2009). The Older Person’s Act recognises the State’s responsibility for developing home-based care and providing information, education and counselling services, and includes care for Alzheimer’s disease and other dementias (amongst other conditions) (see section 11 (2)(c) of the Older Person’s Act, p.13) (Government Gazette, 2006). The Older persons’ programme (Jordan, 2009) and the Protocol on management of elder abuse (DSD, 2010) were established by the Department of Social Development to support the development of a ‘self-reliant society’ that empowers and protects older persons, while promoting their well-being, safety and security (Jordan, 2009). Current policies support services for older persons and are embedded in an ‘active ageing’ philosophy that promotes the full participation of older persons in their societies, their own decision-making and keeping them in their families and communities for as long as possible (Jordan, 2009). The shadow side of this philosophy is that the absence of adequate community-based support services for dementia locates care primarily within the family, where women often adopt care roles without support, resulting in excessive burden (Lloyd-Sherlock, 2019).
South Africa has strong policy support for moving toward universal healthcare through the development of the National Health Insurance (NHI). The objective of the NHI is to provide quality healthcare regardless of a person’s economic status and ability to contribute to the fund (DOH, 2019). However, despite these plans for redress of widespread inequality in South Africa, implementation of the NHI has been slow, with unclear funding modalities and lack of plans for how this scheme will be fully implemented and sustained. In 2013, the National government adopted the Mental Health Policy Framework and Strategic Plan (MHPF) (2013–2020) that promotes an integrated care model for mental health in South Africa, supporting the decentralisation of primary care to home- and community-based services (DoH, 2013). However, like the NHI, these policies are largely ‘dementia-invisible’ with no provisions articulated for dementia care and support services for persons living with dementia and their families. South Africa faces many challenges with policy implementation and corruption across a wide range of sectors. An evaluation of the health system costs of mental health services and programmes in South Africa showed that (i) despite the national policy agenda promoting the decentralisation of services, 86% of mental health service costs remain directed at inpatient services, with the majority of this spending occurring within specialised psychiatric hospitals, (ii) significant disparities exist between provinces on resource allocations, and (iii) there is limited evidence of community-based reforms being initiated (Docrat, Besada and Lund, 2019aDocrat, Besada, & Lund, 2019).
Phase 2: Stakeholder Interviews
Stakeholder Characteristics
Stakeholders characteristics.
Thematic Map of Stakeholder Interviews
The multi-stakeholder interviews largely corroborated the findings of the desk review and provided valuable insight to existing diagnostic services, post-diagnostic support, socio-cultural factors, LTC and support provisions in South Africa. Findings showed how these fragmented systems largely leave people living with dementia and their families with poor diagnostic, referral, and support outcomes, and at risk of elder abuse and neglect. Figure 1 provides a thematic overview of these findings. Thematic map of stakeholder interviews.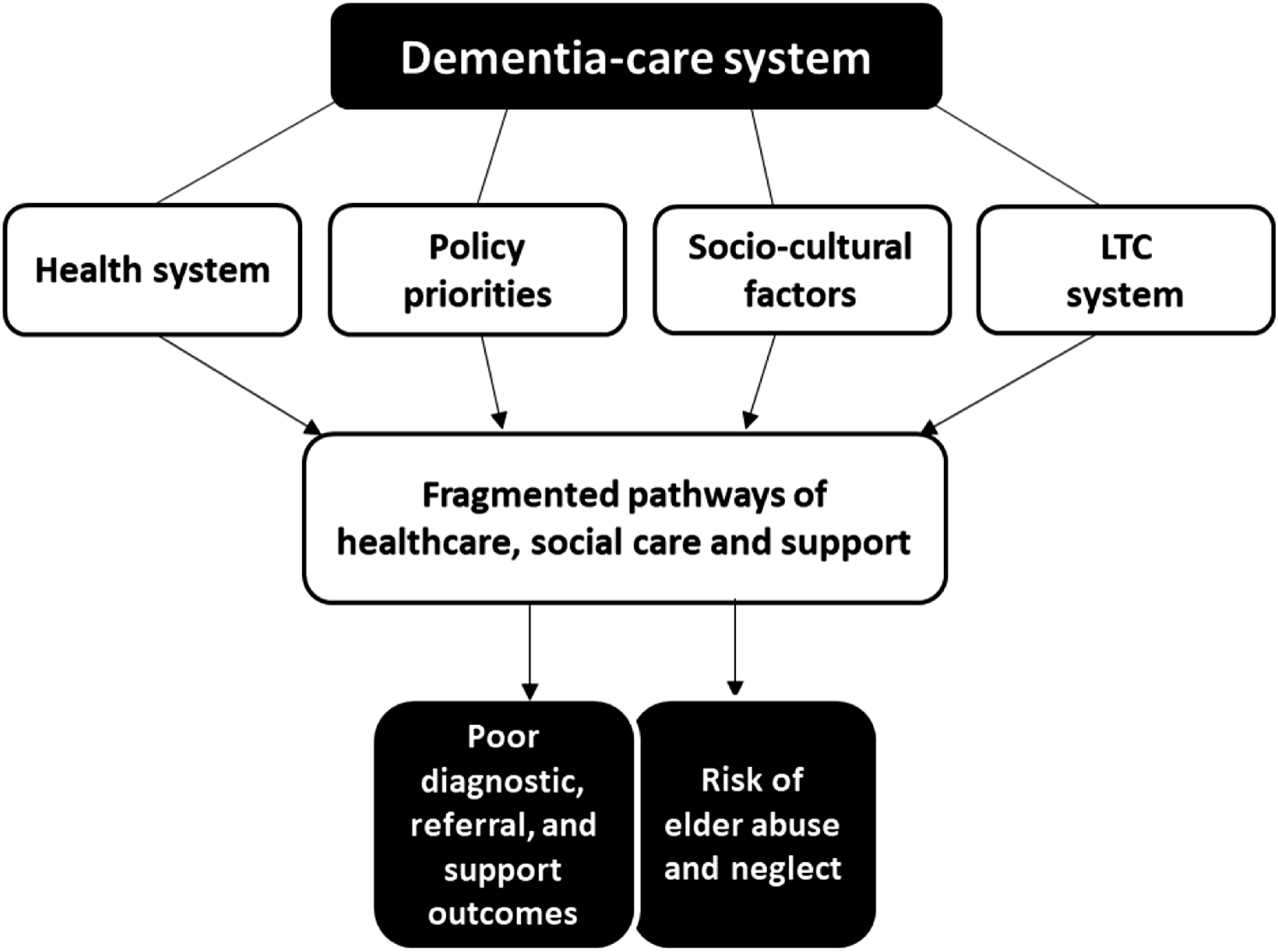
Access to Diagnostic Services
Lack of Training of Health Care Workers
There are many factors influencing access to a dementia diagnosis in South Africa. Referral and diagnostic pathways were described as fragmented, with no specific dementia services at primary healthcare level. Variations in the medical training of primary healthcare doctors and nurses were highlighted as a serious gap in the health system, affecting the identification, diagnostic capacity, and management of dementia.
For example, training nurses on dementia is not prioritised, with reluctance from both nursing schools and the regulating nursing council to include geriatrics in the curriculum: “… for nurses to train in geriatrics, we have tried that, but they say that, that has to be on a postgraduate level, and they are not sure about how much intake there would be…Nursing and geriatric training is a national issue which, over many years, we have tried to motivate for it, but the nursing council haven't really agreed to have it incorporated. We worked together with the Department of Health, the geriatric sector, to try and talk to the nursing council, but for some reason they seem not to have room for that up to now…” (Participant 11, Clinician, Public health service).
Nurses were seen as the backbone of the South African public healthcare system. The low prioritisation of geriatrics and dementia training in nursing curricula limits healthcare provided for people living with dementia. One carer shared about the devasting effect of dementia being unacknowledged in a healthcare setting. She describes the care her mother received by the health care system when she was admitted to hospital after experiencing a stroke, despite she (the carer) informing nurses that her mother had dementia: “I found my mother [restrained] with bandages after she had a stroke. Legs and arms…And the next week she got discharged without the nurse consulting the doctor. So, she walked…being disorientated and not knowing who she was…her feet had blisters and she fell over the bridge from [suburb name], trying to get to [name of suburb she lives in]. And people that recognized her, brought her home…” (Participant 10, Carer and Healthcare professional).
A clinician described how the skill and knowledge of qualified general practitioners (GPs) differ since medical training and exposure to geriatrics vary considerably across the country. Some also believe that nothing can be done for someone with dementia. These factors therefore discourage the identification of dementia and referring patients for formal assessment and diagnosis: “…at the community level regarding health services…there’s not much specific in the management of dementia…What is unfortunate is that the medical schools within the country, not all of them have any exposure to geriatrics at all, so probably only half the medical schools, so that some practitioners finished their training without much exposure to how older people differ [and] their management differs from younger adults. So unfortunately, it's not just the layperson, it’s even the qualified practitioner…for them to say, ‘maybe this is dementia, probably this needs a further referral’…or if they decide to say ‘oh, you know what can be done about it anyway’? ‘What's the point of me referring?’ So that's how it is that not everybody is picked up and not everybody…finds it essential or necessary to refer someone on for further assessment” (Participant 11, Clinician, Public health sector).
Participants living with dementia confirmed this reality and shared their experiences with private GPs that dismissed dementia based on their (younger) age. The first participant described a long journey of yo-yoing between a series of general practitioners and neurologists with poor outcomes: “Then we went to this neurologist [Dr A]. And…he said that…he suspected that I have early onset dementia, Alzheimer but he wasn’t sure…he just suspected. I went back to work. Then, I went back to the GP and…suggested that I see [Dr B, another neurologist]. I went to him, and he then diagnosed me…I think it was a year after he diagnosed me, I went to the GP, the first GP and then he said no, I’m too young and he doesn’t think so. So, he made go off all the tablets…which I did…I carried on working…he didn’t believe me because of my age…he thinks I should go off all the tablets and carry on with my life. And then that’s when I went back to Dr B [2nd neurologist] and I said to him what the GP said…And he said he can do is do all the tests and things again. Which he did. And then apparently, he sent a new report back to the GP to say you know, that this is the situation. I then left that GP I didn’t go back to that GP again” (Participant 4, Person living with dementia).
Delays in diagnosis due to understanding symptoms as ‘natural ageing’
Delays in diagnosis and help-seeking were evident. An experienced clinician linked delayed help-seeking to beliefs of dementia as ‘natural ageing’, also creating risk for elder abuse when families cannot cope with advanced care needs and when changes in behaviour are not understood as a symptom of dementia: “But what we see mostly is that, even for those[families] who are knowledgeable, they don't feel the need of referring someone in the early stages. So, you find that the only time they are prompted to seek any help is when some behavioural or some either feeding or incontinence or something has developed that they are having challenges to cope with, at that point then that's when they feel ‘I think we need help’. So, in the early stages when it's…mild things that they can manage…families don't feel they need to consult anyone about it mostly in the early stages it’s regarded as ‘this happens when you get old’… sometimes there is no understanding of certain behaviours, you know this might be due to dementia. Unfortunately, abuse might even set in at that point because they…cannot live with this change, the challenge” (Participant 11, Clinician, Public health sector).
Lack of Referral Services
Even when awareness and understanding of dementia are good, the reality is often that there are no services available to refer patients to, adding to the belief amongst practitioners that nothing can be done to support people living with dementia: “…family members who have the knowledge, they will say something like ‘I live in the Eastern Cape, do you know anyone in this area who can see my mother or my father…who can give a proper assessment? We think she has dementia.’ So that is a well-informed family, but then they don't have a service to go to” (Participant 11, Clinician, Public health sector).
Lack of Awareness on Dementia
All participants agreed that current responses to dementia in South Africa are inadequate and that there is a need for awareness amongst the general public, as well as education and training on dementia for healthcare staff. One participant summarised these views and talked about the inadequacy of current responses to dementia, noting how education and training are critical tools for awareness and understanding: “…firstly, I think there needs to be a general societal awareness…community clinics in all the areas that have staff that are equipped to see the early warning signs, to start doing some psychoeducation around healthy ageing…we're not even out of the starting blocks in many respects of people understanding dementia…I'm not talking about in rural remote areas. I'm talking about urban areas. I'm talking about educated people…basic understanding in the community is still lacking. There's lots of misconceptions…that escalates people's fear...in rural and remote settings there's lots of suspicion around symptomatic behaviour of dementia patients. I think services are completely inadequate.” (Participant 6, Ageing, Social Care and Support sector).
Post-Diagnostic Support
While there remain many barriers to a timely diagnosis for people living with dementia, as described above, a further challenge (if a diagnosis is obtained) is inadequate post-diagnostic support in South Africa.
Limited Post-Diagnostic Interventions
One of the main challenges reported by experts by experience in this study was that after diagnosis, there was no information or support on how to manage dementia beyond pharmacological responses. One couple shared their post-diagnostic experience in the private sector: “…she’s[neurologist] never even sat with me. When we came there, I said to [husband’s name], what now? What now? I think if you are there for the time with your doctor, whose given you this thing[diagnosis], surely you would like…[to be] more clearer about things which didn't come from my neurologist.” (Participants 1, Person living with dementia).
Post-diagnostic support is, however, offered in pockets by healthcare staff that have more understanding of dementia. A clinician reflected on a strength of the public (tertiary) health system where patients are linked to their community practitioners to co-manage care when re-entering the community: “…we advise families to consult the practitioner who sees them so that we can get full medical background. Also, the reason why we insist that there should be a practitioner involved in the community is that the management has to be bi-directional. After assessment we need to send them back to somebody in the community who can co-manage…we do refer family members to contact [NGO name] to join the groups to support families [and] the patients themselves.” (Participant 11, Clinician, Public health sector).
Medications that support dementia symptom management are not freely available and come at a considerable cost. The minority who can afford medical insurance and/or out-of-pocket payments are able to secure long-term use of medications via private pharmacies: “There’s three that’s quite expensive…but the medical aid is quite good. But the last three months of the year we normally had to pay out of[pocket], then the fund is finished” (Participant 1, Carer).
For the majority of South Africans that rely on free public health services, dementia largely goes unmanaged: “Cholinesterase inhibitors are not on the code for the public healthcare services. So…we do inform them about their availability in the private pharmacies. But again, due to cost most of the people we see, they are on old age pensions and their families cannot afford to buy those medications for year in, year out...there are so many demands on that income…The public healthcare sector has a list of medications that's on code that you are permitted to use, there has been over the years motivation to include the cholinesterase inhibitors on the public service code, but because of the costs and the and they are not 100% effective, there has been resistance to include those on codes, saying it would be very costly nationally…” (Participant 11, Clinician, Public health service).
Need for Multi-sectoral Responses
Participants frequently expressed a need for multi-disciplinary, home-based services for people living with dementia: “Dementia is a challenge, it's not just the medical part…Its a multi-disciplinary management that is lacking. Especially in the public service…if someone is very confused, you take them out of their home to see a day hospital for how many hours and maybe be told that sorry we have run out of medication, or we don't have…I think those are the challenges that there isn't much provision of people going out to people's homes and manage them there. Everyone has to come and line up with everybody else. And for someone who is disoriented, that wait, I mean it's a challenge to sit there with lots of people, a lot of noise going on…someone with dementia can’t filter out [or] block out things so to them [it]is an experience. They go home then they are worse off than they were before. So, we don't have community services that support people within their homes.” (Participant 11, Clinician, Public health service).
As a culturally diverse country, many families seek support from the health system as well as faith-based or spiritual communities, and traditional healing. These pathways of care are not mutually exclusive and reflect the complexity of help-seeking behaviour in South Africa.
Socio-Cultural Factors: Traditional Healing vs. Western Medicine
Traditional Healing
Accessing traditional healers is an important help-seeking resource. One participant summarised how traditional healers are often the first port of call for many families, and especially for older persons: “…they [older persons] will start by getting a traditional healer before the western medicine and sometimes things go well, and sometimes things don't go well and when people are too sick, as traditional healers, there are things we can heal and there are things we can’t heal. And that’s why we have to really understand” (Participant 10, Traditional healer).
Therefore, for dementia awareness and understanding to be meaningful, it is critical to understand how traditional healing approaches include the family system in their consultations (where western medical approaches tend to focus on the individual/disease). Family systems reflect generational norms that are conflicting and create friction within families about care pathways to follow. Insights from a traditional healer with experience and training in dementia illustrated how (often juxtaposed) western and traditional practices could bridge gaps between these ‘worlds’ to serve the needs of people living with dementia and their families (irrespective of where they first access care): “…our [Western, medical] care is not family-centred. It’s looking at individuals, it’s not looking at the whole family…But the traditional healers would talk to a person and the whole family…it’s the family that is suffering and that our [western] care or help that we get, is not family centred. Because the person lives within the family and the family lives within the community…The most important thing is communication with the families, to also say this is how dementia presents itself. So, when you see the symptoms in your family, please go to the clinic or come to [place’s name]” (Participant 10, Traditional healer).
Often dementia is confused with an ancestral calling,
3
a belief where ancestors call an individual through spiritual means to become a traditional healer. A traditional healer explained how this phenomenon compares to dementia arguing that there are key differences in how these two manifest that would help traditional healers make choices about their response (i.e., a ritual for a true ancestral calling versus a referral to a primary healthcare system for dementia): “…a person with ancestral calling will get a repeating or consistent dream. It's like watching a movie when things are happening, and you are able to tell that story. But once you go to a person with dementia, they tell you 20 stories in one story…that's why if you are [a]traditional healer you must listen very carefully…You can't on that first instance say that [the] person has an ancestral calling…this person must…come to you for maybe four times for you to actually ascertain if it’s an ancestral calling or it's related to an intellectual or psychiatric illness and to be able to refer…It’s very rare when people are older that they get ancestral calling. It can happen. But it doesn’t happen a lot. So, most of the time it’s dementia. But you can’t just diagnose without considering the stories” (Participant 10, Traditional healer).
Integrating Traditional and Western Medicine Approaches
It is critical that health staff and traditional healers understand the full patient history, and what is consumed or ingested, especially if prescribing treatment responses. Participants noted that it was common when visiting a medical facility for patients to hide that they consulted a traditional healer, for fear of judgement. People are reluctant to reveal that they may be using alternative interventions before, or alongside pharmacological interventions prescribed by health practitioners: “If they go to a traditional healer, they get asked why did you go there? If the person goes to see a traditional healer sometimes it’s seen as a crime when they go to the western doctors. So, they have to hide that they’ve gone to a traditional healer. So there's no understanding…people get scared to reveal where they’ve been, where they’ve seeked help…” (Participant 10, Traditional healer).
Traditional healing and the needs of families are important considerations when strengthening culturally acceptable responses to dementia. The evidence presented above shows that there are many valuable and under-used resources like primary healthcare nurses, doctors and traditional healers that can be drawn on to strengthen acceptable responses to dementia in South Africa. Support of families is critical, with an emphasis on long-term care and support provisions.
Long-Term Care and Support Provisions
Family Locus of Care
Participants interviewed from the social care and long-term care sectors described dementia care in South Africa as largely family-centred, where the dominant culture in caring for older persons is situated within families and their larger communities: “…a residential facility...that's the last resort and it depends also on the culture of the older persons. You know as [black] Africans, most older persons would want to remain in their homes and taken care of by their families,” (Participant 9, Social care sector).
Specialised dementia LTC services are skewed to the (largely unaffordable) private sector. Community-based services are therefore critical to support families caring for people living with dementia. Unregistered facilities respond to this growing need for LTC provisions in communities, as family members desperately try to balance employment with meeting care needs. Stakeholders talked about their challenges with the mushrooming of unregistered, often predatory, care facilities that do not comply with minimum norms and standards of care for older persons: “…some of our older persons or the families end up taking an older person to an unregistered facility because a registered facility, you'll find that the waiting list…they will tell you we don't have space until maybe another older person dies. So, it's quite a challenge in terms of space. And that is why we have a lot of mushrooming residential facilities which are not registered which do not even comply [to norms and standards]. They would close one here…and after some few weeks they would open in another area. So, it's a money making [enterprise]. I think they are making money out of older persons because family members become frustrated. If I'm the only one looking [after] and there's no other person who can take care of my mom. I would look for an alternative…The need is there.” (Participant 9, Social care services sector).
Stakeholders recognised the need for community-based services but explained that current services were fractured and severely threatened by a failing funding model, even before the COVID-19 pandemic. The needs of older persons were simply not a priority for the country: “You know what, I don't think it's the pandemic. It talks to the priority of the country, we have to start there…services to older persons unfortunately is very critical, but it has never been on the top of the agenda of the country…That's why it's so unfunded both at National[level] and at provinces, because provinces are struggling to increase their funding to NGOs, not because they don't want to, but because there are no funds available. The funds are not increasing at all. If you look at the ECD [early childhood development], they have a lot of money. They have that what we call the grants straight from Treasury so that they can be able to top up when they have [to]. If you look [at] gender-based violence [GBV], everybody's talking about it. Everybody is contributing towards GBV. Everybody is funding even the donors. But when you go to older persons is like ‘why should we waste money?’ as if you are over 60 then you don't have a life anymore. So funding is quite a challenge. And we normally say it’s because it lacks a political buy in. They don't see it as an important service. Unfortunately. We can't fund our organisation[s] properly.” (Participant 7, Ageing, Social Care and Support sector).
Formal care in South Africa is expensive and unaffordable to most of the population who need long-term care solutions. One participant argued that dementia care is broader than medical understanding and approaches to the condition, and that there is a need to ‘de-medicalise’ care in South Africa to make it more accessible to families that need this type of long-term support: “We are too prone to think that you
Carers: Training and Career Pathways
Despite the critical need for formal carers to support service provision in the broader long-term care system (i.e., beyond institutions and including home/community services), there is no formal career path or appropriate salary structure in place to promote philosophies of ‘ageing in place’ that encourage the participation of older persons and promote their quality of life in their communities for as long as possible: “…carers in our country are one of the most underappreciated professions and under paid. These people take the responsibility of that older person on their shoulders. They’re the primary contact in many instances for that older person and that the scales on which they are paid are simply horrendous. I don't know if in fact there is really career pathing for people that wants to take up a career in caring for people with Alzheimer's and dementia, but also whether there is accredited training for care workers…” (Participant 5, Ageing sector, Civil society).
Families with unmet home-care needs are struggling to manage care when a care facility is not an option. Participants noted that unsupported families with long-term care needs are ideal environments for elder abuse and neglect to flourish: “I don't think institutionalisation is necessarily in the future. We don't have the resources as a country to build more residential care facilities, [or] to provide more subsidies. Subsidies are not adequate [in]most cases, which is why, as a result of covid-19 also, many of the residential care facilities have opted to close. If you have a person with dementia in a residential care facility, and that facility closes, where does that older person go? Most likely back to family. And that can be an ideal recipe for abuse and neglect…sometimes people just don't have the capacity to deal…and they try to make do…sometimes it's just an issue of desperation…if there's nowhere to send grandma that has dementia and you can hardly deal with your children, now you have to deal with an older person as well, [and] you don't really know dementia...How do you deal with that? (Participant 5, Ageing sector, Civil society).
Phase 3: SWOT-analysis
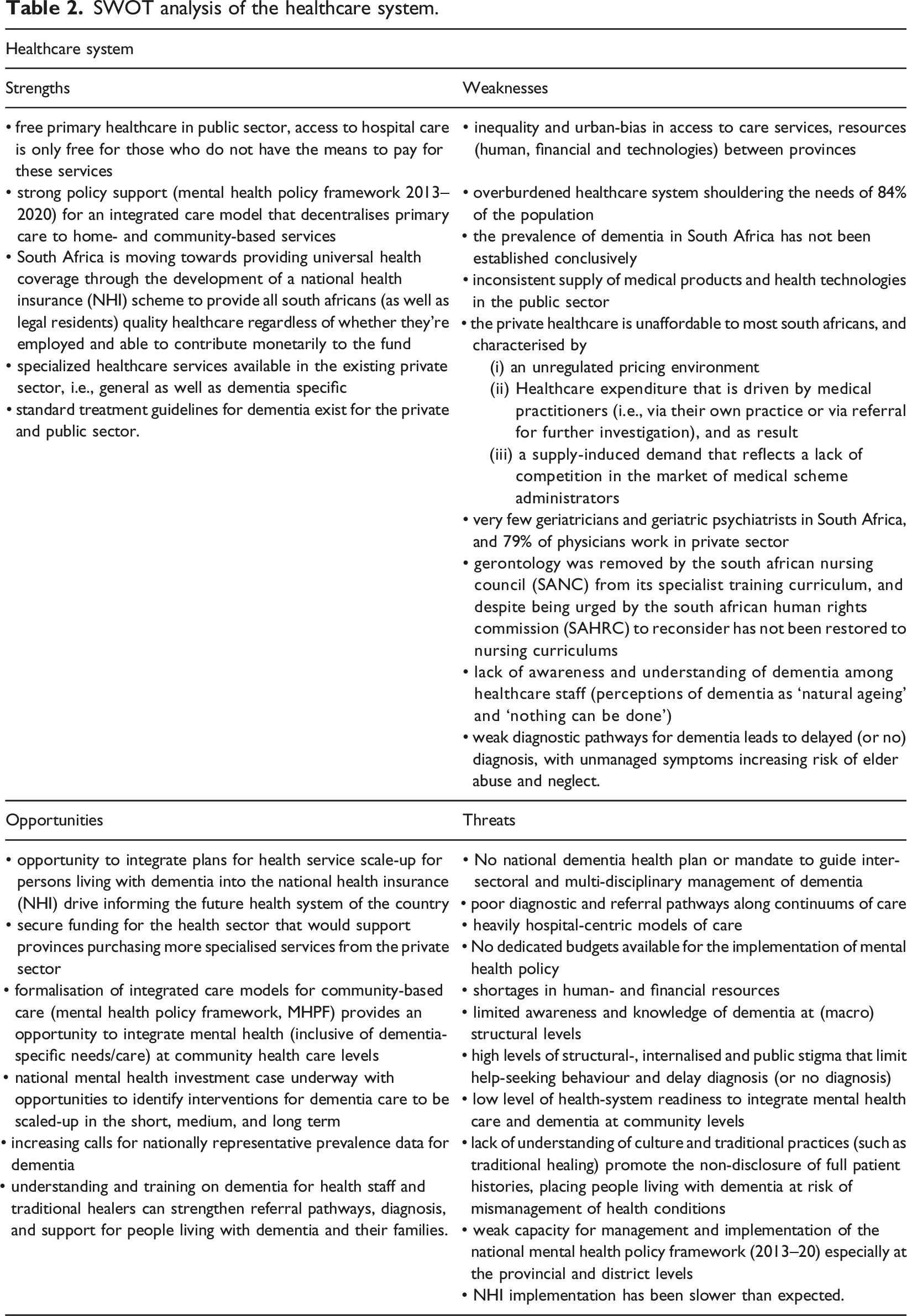
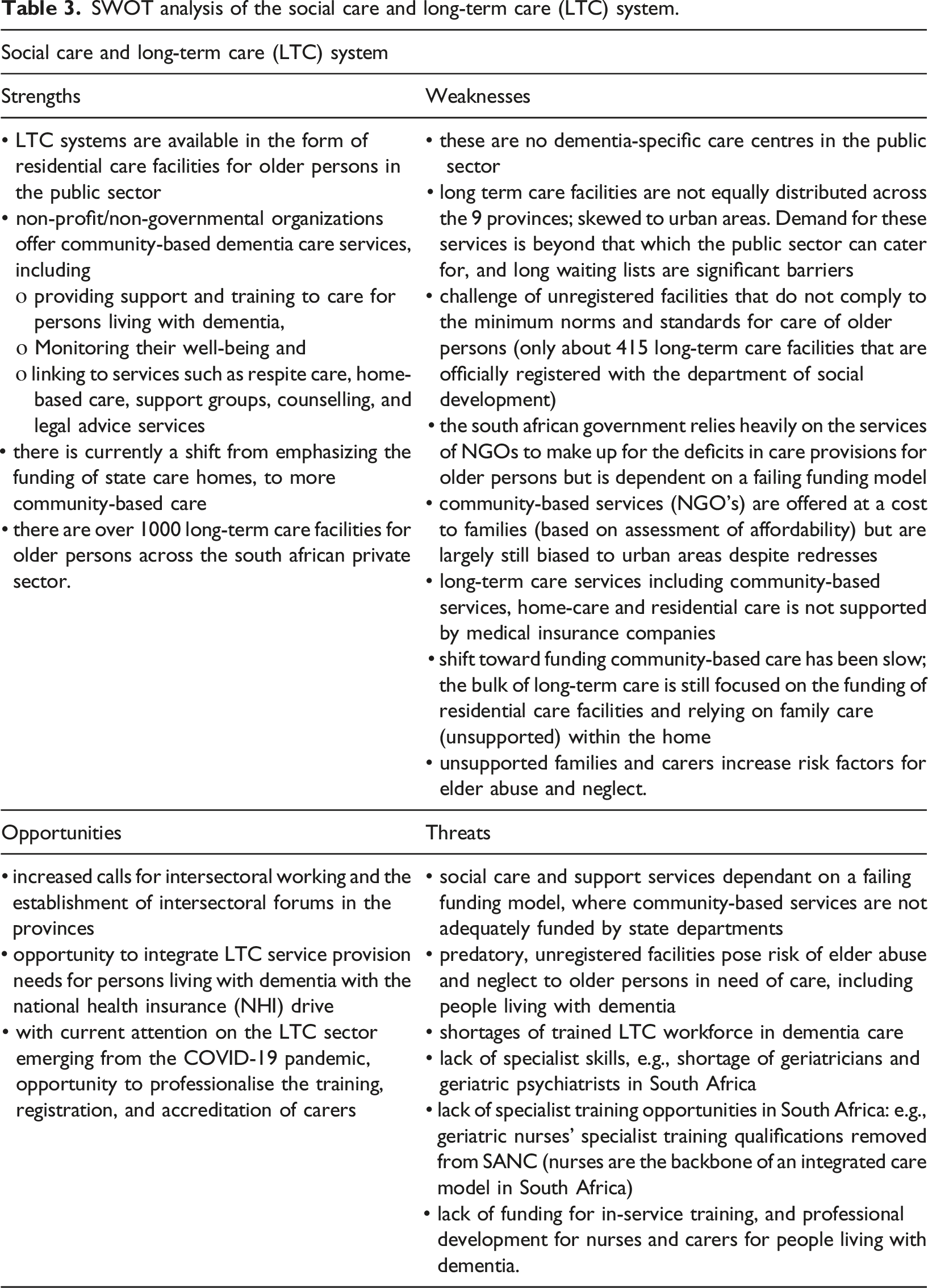
Despite strong policy support for decentralised care to home- and community-based services, the healthcare system in South Africa is still skewed to hospital-centric models of care, with low readiness to integrate mental healthcare and dementia at community levels. Provision of home- and community-based services for people living with dementia rests heavily on a struggling NGO-sector, which, through inadequate funding from the State, is unable to meet the demands for care and support. Unregistered care facilities respond to these community needs for care and support. However, these facilities’ lack of compliance to prescribed norms and standards that guide the appropriate care and support of older persons in South Africa (DSD, 2011) increase risk of elder abuse and neglect to older persons in need of care, including people living with dementia. The NHI articulates no specific objectives for mental health and dementia-related services but, with further development, could offer the opportunity to integrate plans for the scale-up of health- and long-term care services for people living with dementia. Despite strong policy support for the 2013–2020 MHPF, now expired, there was no budget allocated to its implementation. This reflects a common threat to policy and implementation in South Africa, leaving older persons, including people living with dementia and their families, unsupported at a structural level, within their homes and communities.
SWOT analysis of the healthcare system.
SWOT analysis of the social care and long-term care (LTC) system.
SWOT analysis of the policy environment.
Discussion
This study provided an in-depth situational analysis of available care, support and treatment provisions for older persons, people living with dementia and their families in South Africa. We presented the findings from three phases: (1) desk review; (2) multi-stakeholder interviews; and a (3) SWOT-analysis synthesising phase 1 and 2 data. We described current provisions for dementia diagnosis, post-diagnostic services, LTC and support, and the role of traditional healing and culture in dementia care in South Africa. Interviews and quotes from stakeholders provide nuance and context to a complex and fragmented system, while a SWOT-analysis provides a summary of the factors to inform priority setting (strengths and opportunities), as well as to identify risks to achieving these priorities and goals (weaknesses and threats).
We found that dementia diagnostic services were highly fragmented at primary healthcare level, and that most GPs and nurses were not formally trained in geriatrics and dementia. Training in geriatrics and gerontology is limited across the country, with only eight geriatricians registered in 2010 (Lloyd-Sherlock, 2019). In the outcomes of the ‘Investigative hearing into the systemic complaints relating to the treatment of older persons’, the South African Human Rights Commission (SAHRC) urged the South African Nursing Council (SANC) to reinstate gerontology as a requirement in nursing curricula (SAHRC, 2015), with no response to date.
Experts by experience and public health participants indicated that there are various factors (other than training) that delay diagnosis, including stigma and beliefs that ‘nothing can be done’ or ‘you’re too young’; and the unavailability of care and support services to which to make referrals. Most people in South Africa rely on the public sector for free healthcare (Mahlathi & Dlamini, 2015). Another study highlighted that existing health structures do not support the management of dementia, with structural stigma resulting in a ‘dementia-blind’ healthcare system that negatively impacts both help-seeking behaviour and the health system’s preparedness to meet the needs of people living with dementia and their families (Jacobs et al., 2022).
Carers that feel supported are less likely to abuse care recipients (Serra et al., 2018). Our findings suggested that there might be a link between delayed help-seeking and diagnosis, unmet home- or community-based support needs, and the risk for elder abuse. As dementia and functional dependence increase, the family’s ability to cope and provide adequate support is diminished in a context where no formal support services are accessible. Lack of post-diagnostic support, high levels of care burden, and poor knowledge of how to care for someone living with dementia are known risk factors for elder abuse and neglect (Downes, 2013). These realities are amplified in a country characterised by widespread poverty, crime, inequality and unemployment (The World Bank, 2018) and emphasise the need for adequate diagnostic and post-diagnostic support and care.
Existing community-based care services are urban-biased and divided across two tiers: (1) private, profit-based care that is accessible only to the minority who can afford it; and (2) the non-governmental sector (NGO) that is non-profit, severely underfunded and resource-constrained (Prince, 2016). The NGO sector is currently the only source of dementia-specific care and support for the majority of South Africans who cannot afford private care. Therefore, most people living with dementia live at home and are supported by an unpaid, informal carer who is (usually) a female family member (Lloyd-Sherlock, 2019). Despite the government’s reliance on the NGO sector for care and support, our study showed that these essential community-based services are grounded on a failing funding model where the need substantially outweighs investment by the State. The large number of unregistered facilities reflect the magnitude of this unmet need at community level, leaving people living with dementia and their families unsupported and at risk of isolation, increased financial hardship, elder abuse, and neglect.
Our study has shown that the family system is an important resource in health decision-making, support and the care of people living with dementia. Traditional healing is often the first port of call for many, and an important source of support for families at community level. It is vital that people feel safe to inform health staff about treatments accessed, especially when using traditional substances in conjunction with pharmacological interventions. Health staff sensitisation and understanding of traditional practices are important to understand patient histories holistically, and crucial to create safe spaces for families to communicate freely.
Our study also showed that education and training are powerful tools for dementia awareness and could potentially bridge the often juxtaposed western and traditional healing practices. Traditional healers, together with trained general practitioners and primary health nurses, are largely unused resources for the identification, referral, and management of dementia in culturally acceptable ways.
Limitations
Our study is not without limitations. First, the findings are derived from a small number of stakeholders, with different backgrounds and expertise. The fact that there were common themes despite the heterogeneity in the sample, however, strengthens the likelihood that these experiences are commonplace, and this is further confirmed from data collected in other components of the project. However, our interviews do not represent dementia stakeholders from all backgrounds and regions, and as such we should be cautious about assuming generalisability. Selection bias may also lead to certain views being more prominent in the study, thus confirmation of findings in a larger cohort would be beneficial. Second, we had limited participation from the health sector because of unanswered applications for formal permission to interview national health government officials. Third, we adopted a pragmatic solution of completing a dyadic interview with a person with dementia and their carer. Whilst this helped make the person with dementia feel more at ease, it is important to consider that interview responses may have been influenced by the presence of a family member within the room. Finally, it is important to note the timing of data collection – the heart of the COVID-19 pandemic – when the health sector was largely unavailable and involved in managing the national health crisis and people were feeling the effects of even more limited access to healthcare. We also acknowledge that our understanding of participant experiences is limited to the explanations of cultural beliefs provided by the stakeholders themselves.
Conclusion
Our findings provide an important contribution to inform priority-setting for health, social care, and support services and to highlight gaps and opportunities within current provision for people living with dementia and their families in South Africa and potentially also in other low-and-middle-income settings. We have shown how structural factors (weaknesses and threats) create barriers in accessing a timely diagnosis, post-diagnostic support and care. We have also shown how current structures locate dementia care within households that are, for the most part, unsupported, and thereby fuelling known risk factors for elder abuse and neglect. Post-diagnostic support described by our stakeholders living with dementia tended to centre around pharmacological interventions. We need more research to explore the contributions that non-pharmacological approaches can make to support care practices at family and community level.
There is an urgent need to prioritise adequate responses at policy, structural and community levels as the general unavailability of services drive stigmatising beliefs that ‘nothing can be done’ for people living with dementia. This study highlighted an opportunity to support broader employment initiatives by developing career pathways for formal carers and in doing so, strengthen community structures to support ‘ageing in place’. Supporting people living with dementia is everyone’s responsibility and cuts across sectors, disciplines, and traditions. Ageing in South Africa is hard for older persons and people living with dementia. This hardship could be mitigated through implementing intersectoral policy responses to support the strengthening of current health, social care, and support systems so that people living with dementia and their families can live and age well. Ultimately, maintaining and improving the quality of life of people living with dementia and their families should be a priority.
Footnotes
Acknowledgments
We would like to thank Klara Lorenz-Dant, Wendy Weidner, Chiara De Poli, and the South African Advisory members for their support. We thank all our stakeholders and experts by experiences for sharing their time and expertise. We also like to thank the National Department of Social Development and the National Department of Health for their ongoing support and insights in strengthening responses to dementia in South Africa.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the support of the STRIDE project and funding from the United Kingdom Research and Innovation’s Global Challenges Research Fund (GCRF), through the Economic and Social Research Council (grant number ES/P010938/1). The funders had no direct input to the formulation or creation of the protocol, results, and their interpretation.
Ethical Approval
This study has ethical approval from the University of Cape Town’s Human Research Ethics Committee (HREC reference 021/2019). This study was approved by the Human Research Ethics Committee (HREC) of the Faculty of Health Sciences, University of Cape Town (HREC reference 021/2019) and the London School of Economic and Political Science’s Research Ethics Committee (REC reference 000834b).