
Abstract
Objectives
This systematic review examined the effectiveness of Montessori-based programmes for individuals with dementia living in residential aged care.
Methods
Nine databases were searched between January 2010 to October 2021, including Scopus, CINAHL, MEDLINE, Web of Science, SocINDEX with Full Text, PubMed, PsycINFO, Cochrane library and Cochrane Registry. Publications were included if they used Montessori-based programmes as interventions for individuals with dementia living in residential aged care and were qualitative, quantitative, mixed-method, or pilot studies. The quality of eligible studies was assessed using Joanna Briggs Institute critical appraisal instruments and the Mixed Method Critical Appraisal Tool. The findings were tabulated and narratively synthesised.
Results
Fifteen studies were included in this review. The quality scores of the 15 studies ranged from 62 to 100 out of 100. Four key categories of outcomes were observed: (1) significantly improved engagement; (2) significantly improved mental health outcomes, including affect, depression, agitation, excessive eating and psychotropic medication prescriptions; (3) significantly improved feeding difficulty but mixed results regarding nutritional status; and (4) no significant changes in the activities of daily living and quality of life of individuals with dementia.
Conclusion
Cognitive capacity, personal preferences, individual care needs and the design of Montessori-based activities are pivotal to tailoring personalised Montessori-based activities for individuals with dementia in residential aged care and to maximise intervention outcomes. The synergistic effect of integrating Spaced Retrieval with Montessori-based activities in improving the eating ability and nutritional status of individuals with dementia was also noticed. The study summarised evidence about the effectiveness of Montessori-based programmes for individuals with dementia and informed healthcare professionals about how to implement individualised Montessori-based programmes.
Keywords
Introduction
Montessori-based programmes in dementia care are non-pharmacological interventions that reflect the person-centred approach to engaging individuals with dementia (Dementia Australia, 2019). The principles of Montessori-based programmes encompass respect, dignity, autonomy and equality, and the activities are tailored to match the cognitive capacity of individuals with dementia (Camp, 2010; Camp et al., 2017; Dementia Australia, 2019). By using familiar materials, task breakdowns and guided repetition from simple to complex, Montessori-based programmes enable individuals with dementia to adapt to self-paced learning and achieve success (Camp, 2010). The Montessori-based programme denotes that individuals with dementia be perceived as living with a disability rather than a disease (Camp, 2010). In addition, Montessori-based programmes encourage individuals with dementia to engage actively and connect within a social and physical environment through purposeful and meaningful activities (Camp, 2010; Camp et al., 2017).
Dementia has a significant impact on individuals' cognition, behaviour, psychology, functionality and quality of life (Alzheimer’s Society, 2022b; Bessey & Walaszek, 2019; Gale et al., 2018). As the worldwide incidence of dementia increases at an alarming rate, its impact on individuals, families and the care burden must be addressed (World Health Organisation, 2022). In Australia in 2022, it is estimated that there are 487,500 individuals living with dementia with a projection of 1,076,000 by 2058. (Alzheimer’s society, 2022a). Additionally, in 2018, three billion dollars of the Australian health budget were allocated to dementia care (Australian Institute of Health and Welfare, 2021). A study by Cohen-Mansfield et al. (2015) identified the top three unmet needs of individuals with dementia in residential aged care to be loneliness/need for social interaction, boredom/sensory deprivation, and need for meaningful activities. Especially for those who are in the advanced stages of dementia and needed assistance to meet their physical, psychological and spiritual needs, such as safety, food, physical well-being and physical activities are most intense (Schmidt et al., 2018). Consequently, healthcare practitioners have a significant role to play in promoting the health and well-being of individuals with dementia in residential aged care. In addition, the ramifications of ignoring these unmet care needs of individuals with dementia do not support person-centred care and may also be associated with depression, responsive behaviours and increased dependency on caregivers and result in caregiver burden (Carvacho et al., 2021). Thus, understanding the care and support needs of individuals with dementia is crucial for enabling individuals with dementia to enjoy a meaningful life and to feel fulfilled and accomplished.
The World Health Organisation recently recognised the need for all countries to develop strategies that will improve the health and well-being of individuals with dementia and their family caregivers in their Global action plan on the public health response to dementia 2017-2025, mDementia handbook, WHO’S iSupport programme (World Health Organisation, 2022). Over many years in Australia, various attempts have been made to improve dementia care, such as the Clinical Practice Guidelines and Principles of Care for People with Dementia that provide recommendations for care. These recommendations include providing a person-centred approach, improving quality of life and using dementia-friendly language (Guideline Adaptation Committee, 2016). Therefore, prioritising the needs and preferences of individuals with dementia is a crucial way of achieving person-centred dementia care (Guideline Adaptation Committee, 2016). Most recently, the Royal Commission into Aged Care Quality and Safety (2021) emphasised the right of older Australians to receive high quality, safe and timely care from service providers. To achieve this, the national peak body of dementia care (Dementia Australia) advocated for the use of Montessori-based programmes in aged care to improve the engagement and quality of life for individuals with dementia (Dementia Australia, 2021).
Montessori-based activities are evidence-based practice that have been adopted for individuals with dementia for decades and has shown many benefits. For instance, positive effects on feeding difficulty, engagement, affect and cognition (Sheppard et al., 2016). Other aspects of dementia care such as verbal communication, quality of life, behaviour changes, relationships with family visitors and staff are also mentioned. Montessori-based activities have also been shown to reduce agitation and, therefore, reduce psychotropic medication utilisation (Booth et al., 2020; Ducak et al., 2018; Lin et al., 2009; Orsulic-Jeras et al., 2000; Runci et al., 2012). Montessori-based activities combined with Spaced Retrieval (a memory training technique) have been shown to enhance the eating abilities of individuals with dementia (Wu and Lin, 2013; Wu et al., 2014). Despite there being many studies that highlighted the value of Montessori-based programmes, there are few studies that have examined the effectiveness of Montessori-based programmes in residential aged care, including nursing homes, dementia care units and memory care units. Therefore, this systematic review aimed to synthesis the evidence from published research that focused on determining the impact of Montessori-based programmes on individuals with dementia in residential aged care.
Methods
The study design was a systematic review with narrative synthesis. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Checklist was used to guide the review process and report results (Page et al., 2021). The review protocol was registered and published in PROSPERO (registration number CRD42021291129).
Eligibility criteria
The inclusion criteria for eligible studies were: (1) written in English; (2) published in a peer-reviewed journal between January 2010 to October 2021; (3) sample included individuals with dementia (all types and all stages) in residential aged care, such as nursing homes, dementia care units and memory care units; (4) study outcomes were relevant to the usage of Montessori-based programmes on individuals with dementia in residential aged care; and (5) qualitative, quantitative, mixed-methods and pilot studies that met the objectives of this review. The exclusion criteria included studies that only explored the effects of Montessori-based programmes on outcomes for caregivers, studies not conducted in residential aged care, review articles, case studies, study protocols, commentary articles and studies with a high risk of bias. The search was limited to abstracts and full-text available.
Information sources and search strategy
Nine databases were searched: Scopus, CINAHL, MEDLINE, Web of Science, SocINDEX with Full Text, PubMed, PsycINFO, Cochrane library and Cochrane Registry. The keywords searched were: “dementia” OR “Alzheimer*” OR “cognitive impairment” OR “cognitive decline” OR “memory loss” AND “Montessori”. The primary author (ZMY) used these keywords after multiple pilot searches to test their accuracy. The university librarian was also consulted to ensure that the keywords and the target databases would generate a comprehensive search. Additional sources were searched, including Google Scholar, industry websites such as Dementia Australia (https://www.dementia.org.au/) and Alzheimer’s Association (https://www.alz.org/), as well as organisations such as Bupa Aged Care (https://www.bupaagedcare.com.au/), Uniting Care Australia (https://unitingcare.org.au/) and Anglican care (https://anglicancare.com.au/residential-care/). In addition, the citations of potentially eligible studies were also examined.
Data collection process and methodological quality assessment
The primary author (ZMY) screened the titles and abstracts from the databases and saved potentially eligible studies in Mendeley. Four authors (ZMY, IA, HCC and VT) independently assessed the methodological quality of the selected papers after retrieving the full text of eligible studies. The Joanna Briggs Institute critical appraisal instruments were used to review the papers (Aromataris, & Munn, 2020In Aromataris & Munn, 2020) for randomised control trials (RCT), quasi-experimental and qualitative research, and the Mixed Method Critical Appraisal Tool was used for mixed-method studies (MMAT; Hong et al., 2018). Questions were answered with ‘yes’ (score 1) and ‘no’ (score 0) for the Joanna Briggs instruments. Scores were converted to percentages to allow for comparison across different study designs. A score of 100% indicated the highest possible score. Low-quality papers were excluded based on an agreed quality threshold of the mean minus one standard deviation (Aromataris, & Munn, 2020In Aromataris & Munn, 2020). Questions from the Mixed Method Critical Appraisal Tool were answered only as ‘yes’ or ‘no’ because the instructions for using this tool do not recommend calculating a score, and thus no percentage score was possible for the mixed method studies appraised. Discrepancies between the two reviewers were resolved through discussion with the other authors.
Data extraction
Two reviewers (ZMY and VT) worked together to extract the key data from the original empirical studies. The extracted data were tabulated to answer the research question for this study. Details such as the name of the first author, year of publication, country, aim, method, sample size, setting, characteristics of participants, intervention, measurement tools, and outcomes were extracted from the original studies. Additionally, details of the Montessori-based programme intervention were extracted, including the format, content, frequency, duration, and the role of the individual(s) who implemented the intervention. The outcomes from the included studies were grouped using the recommendations from the Health Categories of the UK Clinical Research Collaboration (n.d.). The details of the measurement tools, data collection time and method, and the presentation of key findings with statistical significance were also included.
Data synthesis
Studies varied greatly in terms of the study design, interventions and populations. Due to the heterogeneity of the studies included, meta-analysis was not the best choice for data synthesis (Munn et al., 2014). The majority of the studies in this review were observational studies and varied in terms of their study design, and included RCTs, quasi-experimental and mixed-methods. There were variations in the Montessori-based programme design and data collection, such as the duration of the programme, frequency and duration of the Montessori-based activities, role of the implementers, data collection tools and data collection points. The participants were in different stages of their dementia and thus the impact of their dementia on the intervention outcomes differed. To manage these heterogeneities, narrative synthesis was adopted to tabulate the data and outcomes from the review. According to the JBI systematic review guideline on effectiveness review, the essence of a narrative synthesis is to summarise the results of included studies using words and tables without meta-analysis, which provides a reliable source to facilitate an understating of the summarised results and enhances the robustness of the synthesised results (Aromataris, & Munn, 2020). The findings from the 15 included studies were classified into four categories: (1) engagement; (2) mental health outcomes; (3) feeding difficulty and nutritional status; and (4) activities of daily living and quality of life. The areas addressed were included study selection, critical appraisal results, characteristics of included studies, details of the intervention, measurement tools, data collection methods and the impact of Montessori-based programmes in residential aged care.
Results
Study selection
Details of the study selection are presented in Figure 1. PRISMA 2020 flow diagram (Page et al., 2021). A total of 281 records were retrieved from databases and registers, out of which 230 records were excluded after screening the titles and abstracts. After full-text retrieval, 51 records were assessed, out of which 36 were excluded for various reasons, leaving 15 studies that were eligible for inclusion. Five records were not retrieved because they did not meet the inclusion criteria. ‘Other’ sources were five citations from organisational websites. The 86 citations related to Montessori-based activities that were retrieved from the 15 eligible studies were all excluded, with reasons provided as shown in the PRISMA 2020 flow diagram.
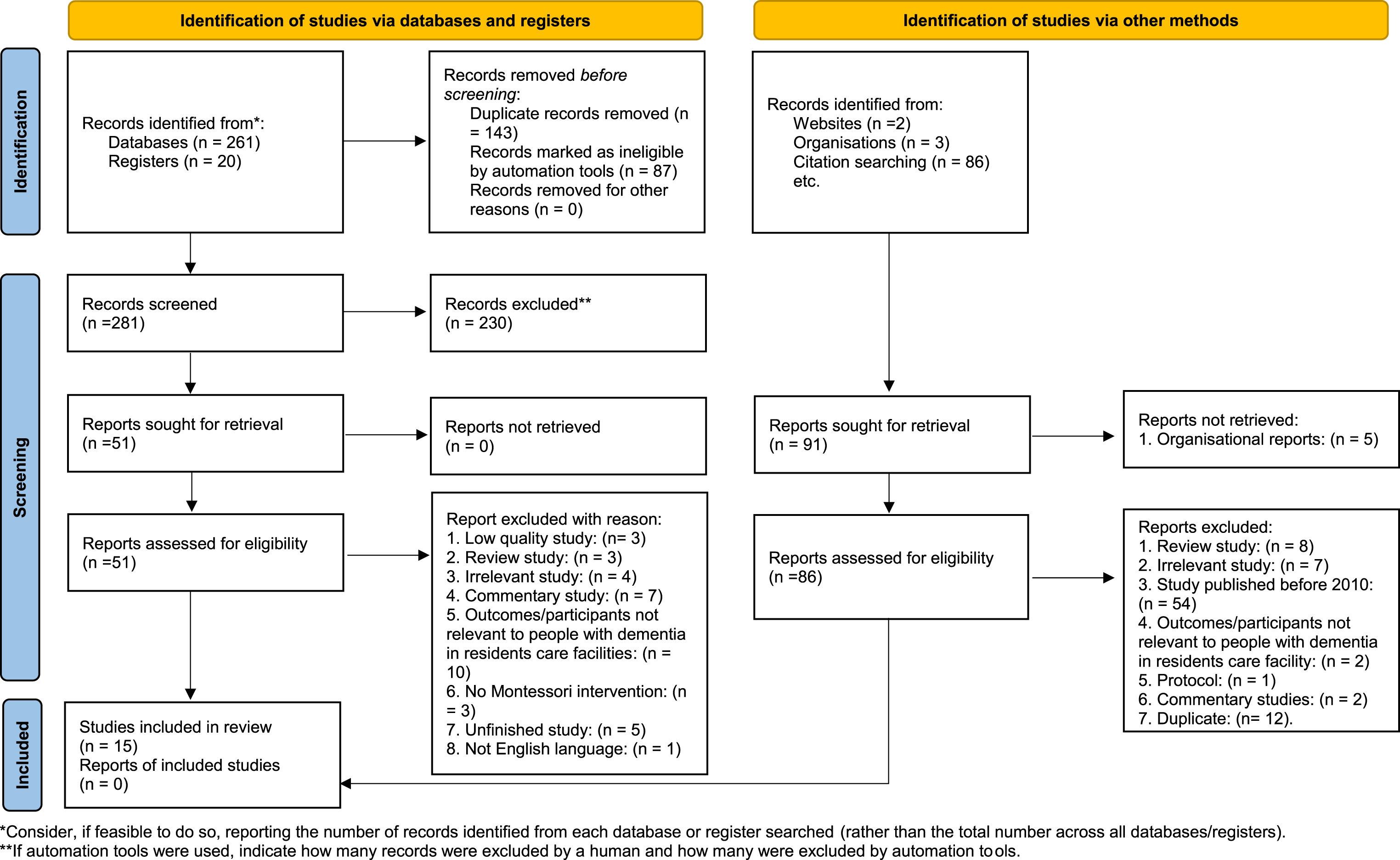
*Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/
Critical appraisal results
Eighteen studies met the inclusion criteria and were appraised for methodological quality. Of these, six were RCTs, eight were quasi-experimental studies, two were qualitative studies, and two were mixed methods studies (for which the tool recommended scores could not be calculated). The mean (M) quality score for the 16 studies appraised was 70.69 out of 100 (Standard Deviation [SD]: 16.44). The threshold for excluding low-quality papers was determined as ≥ 54.25 (70.69–16.44 = 54.25). Of the 18 studies appraised, three studies (one RCT and two qualitative studies) were excluded due to low methodological quality, leaving 15 studies for this literature review. Of the 15 included studies, except the two mixed methods studies, the quality scores across the remaining 13 studies ranged from 62 to 100 (M ± SD: 76 ± 13.77). Details of the critical appraisal results are showed in Supplement file 1: Critical appraisal results of the included studies.
Characteristics of included studies
Characteristics of included studies.

A total of 885 individuals with dementia participated in the studies included in this review. The participants’ mean age ranged from 63.6 (Mbakile-Mahlanza et al., 2020) to 89 (Skrajner et al., 2014) years. Regarding gender, 12 of the studies reported 409 females and 251 males as participants (Chan et al., 2021; Chaudhry et al., 2020; Gaspar and Westberg, 2020; Kao et al., 2016; Lin et al., 2010, 2011; Mbakile-Mahlanza et al., 2020; Roberts et al., 2015; Skrajner et al., 2012, 2014; Wilks et al., 2019; Yuen and Kwok, 2019); while three studies omitted gender (Giroux et al., 2010; Wu and Lin, 2013; Wu et al., 2014). More than half of the included studies’ participants (n = 8, 53.3%) were experiencing moderate to severe dementia (Chaudhry et al., 2020; Giroux et al., 2010; Kao et al., 2016; Lin et al., 2011; Roberts et al., 2015; Skrajner et al., 2014; Wilks et al., 2019; Yuen and Kwok, 2019). Three studies (n = 3, 20%) focused on participants experiencing mild to moderate dementia (Lin et al., 2010; Mbakile-Mahlanza et al., 2020; Skrajner et al., 2012) and four (n = 4, 26.7%) on mild to severe dementia (Chan et al., 2021; Gaspar and Westberg, 2020; Wu and Lin, 2013; Wu et al., 2014). Five studies (Gaspar and Westberg, 2020; Kao et al., 2016; Lin et al., 2010, 2011; Mbakile-Mahlanza et al., 2020) reported the length of time the participants had been living in residential aged care, which ranged from 21 (Gaspar and Westberg, 2020) to 36 months (Kao et al., 2016).
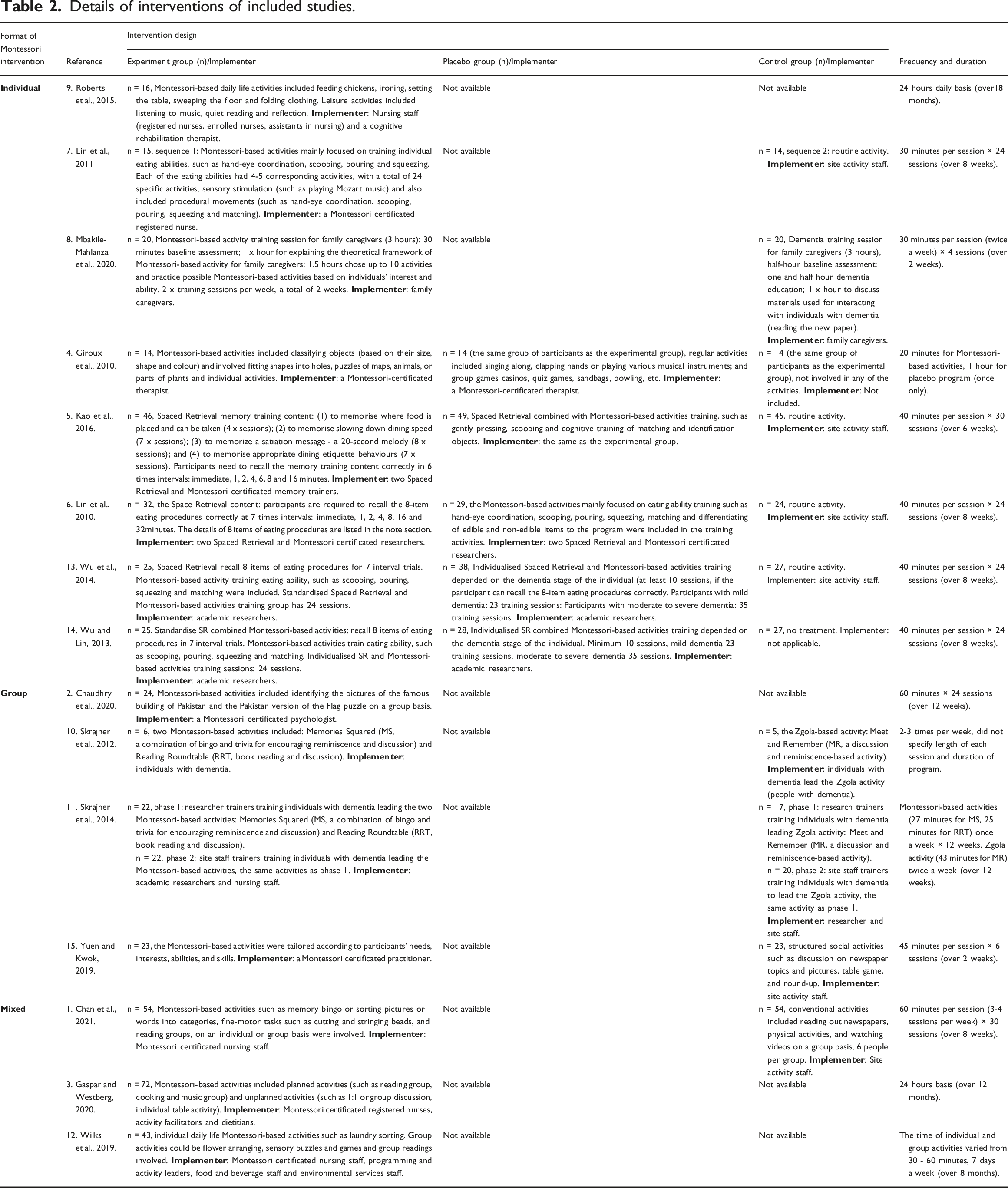
Details of the intervention
Details of interventions of included studies.
Measurement tools and data collection
Summary of variables, measurement tools, data collection and key findings with statistical significance.
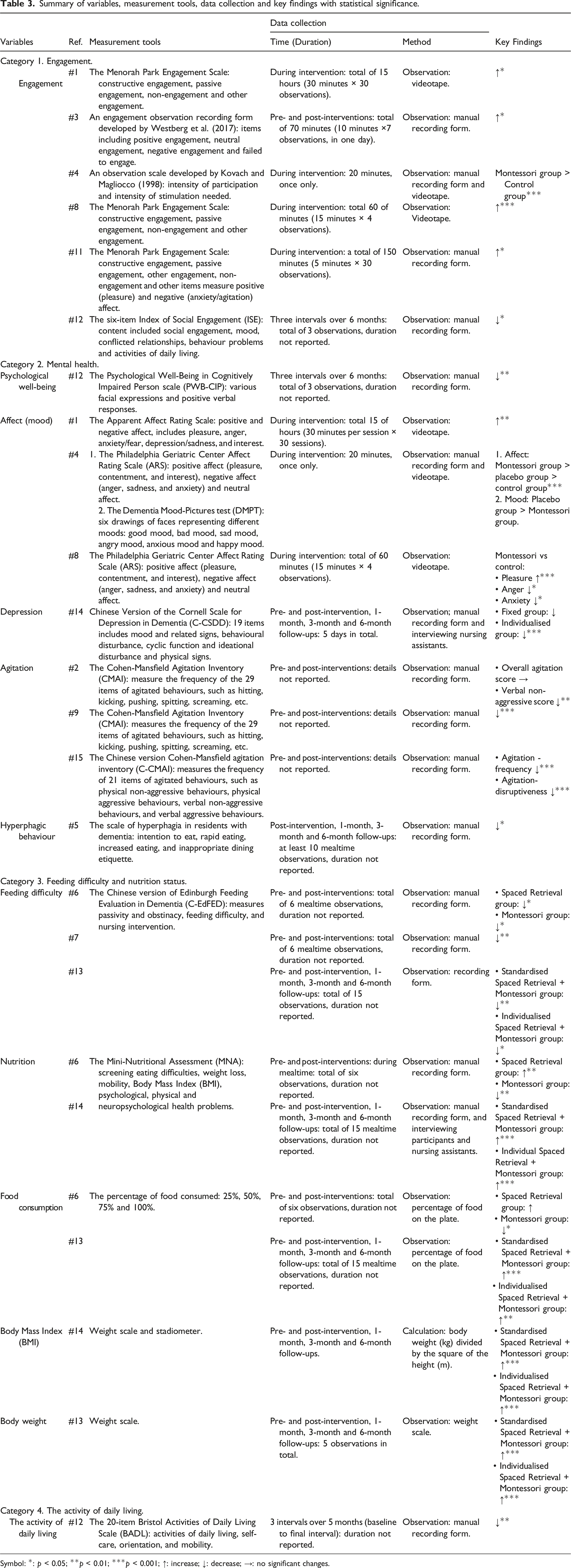
Symbol: *: p < 0.05; **p < 0.01; ***p < 0.001; ↑: increase; ↓: decrease; →: no significant changes.
The impacts of montessori-based programmes in residential aged care
Category 1: Engagement
Eight studies investigated the engagement, feasibility and acceptability of Montessori-based programmes (Chan et al., 2021; Chaudhry et al., 2020; Gaspar and Westberg, 2020; Giroux et al., 2010; Mbakile-Mahlanza et al., 2020; Skrajner et al., 2012, 2014; Wilks et al., 2019). Four studies showed significant improvement in engagement scores post-intervention (p < 0.05) (Chan et al., 2021; Gaspar and Westberg, 2020; Mbakile-Mahlanza et al., 2020; Skrajner et al., 2014). Mbakile-Mahlanza et al. (2020) reported a large effect size (Cohen’s d = 1.33) on constructive engagement post-intervention. Giroux et al. (2010) showed the Montessori-based programme had a significantly higher overall engagement score than the control group (2.9 ± 0.8 vs. 2.5 ± 0.5, p < 0.001). However, Wilks et al. (2019) illustrated a significant decrease in engagement scores post-intervention (M ± SD: 3.0 ± 2.19 in the pre-test versus 2.6 ± 2.24 in the post-test, p < 0.05). Additionally, Chan et al. (2021) and Chaudhry et al. (2020) confirmed that overall engagement was acceptable and feasible in Chinese and Pakistanis communities. Skrajner and colleagues (2012) pilot tested the feasibility of a Montessori-based programme led by the residents (individuals with dementia) in the United States also generated positive outcomes in engagement.
Category 2: Mental health
Ten studies examined the mental health outcomes of participants (Chan et al., 2021; Chaudhry et al., 2020; Gaspar and Westberg, 2020; Giroux et al., 2010; Kao et al., 2016; Mbakile-Mahlanza et al., 2020; Roberts et al., 2015; Wilks et al., 2019; Wu and Lin, 2013; Yuen and Kwok, 2019). These mental health outcomes, include but are not limited to psychological well-being, cognition, affect (mood), depression, anxiety, agitation, behavioural and psychological symptoms of dementia, hyperphagic behaviour, prescription rates of antipsychotic and sedative medications (Gaspar and Westberg, 2020; Roberts et al., 2015). Prior studies showed significantly positive outcomes (p < 0.05) on affect (mood) (Chan et al., 2021; Giroux et al., 2010; Mbakile-Mahlanza et al., 2020), agitation (Chaudhry et al., 2020; Roberts et al., 2015; Yuen and Kwok, 2019), hyperphagic behaviour (Kao et al., 2016) and psychotropic and sedation medication rates (Gaspar and Westberg, 2020; Roberts et al., 2015). Whereas there was a significant reduction in psychological well-being score post-intervention (p < 0.01) (Wilks et al., 2019) and a varying impact on depression post-intervention, with one Montessori-based programme reported a strong significant positive outcome (p = 0.001) (Wu and Lin, 2013) and another reporting no significant changes (Chaudhry et al., 2020). There was no significant change in cognition (Chaudhry et al., 2020), anxiety and responsive behaviours of individuals with dementia (Wilks et al., 2019).
Category 3: Feeding difficulty and nutritional status
Four studies explored the feeding difficulty and nutritional status of participants (Lin et al., 2010, 2011; Wu and Lin, 2013; Wu et al., 2014). Two studies examined the effectiveness of Montessori-based programmes and Spaced Retrieval alone (Lin et al., 2010, 2011), while the other two studies combined Spaced Retrieval with Montessori-based activities (Wu and Lin, 2013; Wu et al., 2014). Overall, Spaced Retrieval combined with Montessori-based activities, regardless of standardised training or individualised training, yielded better results than Montessori-based activities alone or Spaced Retrieval alone in feeding difficulty, nutritional status, body mass index, body weight and food consumption. Although Spaced Retrieval or Montessori-based activities alone can significantly reduce the feeding difficulty of individuals with dementia post-intervention (p < 0.05) (Lin et al., 2010, 2011; Wu et al., 2014), significant reductions in food consumption (mean difference = −10.08, p < 0.05) and nutrition (mean difference = −2.58, p < 0.01) were observed with Montessori-based activities alone, and there were no changes in body mass index and body weight (Lin et al., 2010). In contrast, significant improvements in nutrition (slop increase: 0.94, p < 0.001), food consumption (mean difference = 5.80, p < 0.001), body mass index (slope increase: 0.39, p = 0.001) and body weight (mean difference: 0.99, p < 0.001) were observed when Spaced Retrieval was combined with Montessori-based activities (Wu and Lin, 2013; Wu et al., 2014). Furthermore, improved nutritional status was associated with a significant reduction in depression among participants, and the effects on nutrition lasted six months after the intervention (R2 = 0.44, p < 0.001) (Wu and Lin, 2013).
Category 4: activities of daily living and quality of life
Two studies reported the activities of daily living and quality of life of participants (Chaudhry et al., 2020; Wilks et al., 2019). Wilks et al. (2019) found a statistically significant reduction in activities of daily living post-intervention (M ± SD: 1.2 ± 0.79 in the pre-test versus 1.0 ± 0.76 in the post-test, p < 0.01). While Chaudhry et al. (2020) discovered a slight increase in activities of daily living score but it was not significant. When the impact on the quality of life for individuals with dementia was measured, two Montessori-based programmes reported positive changes but these effects were not significant (Chaudhry et al., 2020; Wilks et al., 2019).
Discussion
The purpose of this systematic review was to fill a knowledge gap and summarise the evidence on the effects of Montessori-based programmes on individuals with dementia in residential aged care. The findings from this systematic review identified 15 studies and reported on four main categories of impacts for Montessori-based programmes: (1) engagement; (2) mental health; (3) feeding difficulty and nutritional status; and (4) activities of daily living and quality of life. In the discussion section, suggestions for improving the design of Montessori-based programmes and research in this area are presented. Furthermore, when considering the format of Montessori-based activities and their intended outcomes, the individual format is best suited for specific training purposes such as reducing feeding difficulty and addressing individual mental health concerns like agitation, hyperphagia behaviours and depression. On the other hand, the group and mixed formats of Montessori-based activities have shown to be more effective in enhancing engagement and emotional well-being among individuals.
Engagement
Generally, almost all studies that are relevant to engagement reported significantly positive outcomes (Chan et al., 2021; Gaspar and Westberg, 2020; Giroux et al., 2010; Mbakile-Mahlanza et al., 2020; Skrajner et al., 2014). The only exception was Wilks et al. (2019) that showed a significant reduction in engagement due to participants being in their late-stage of dementia and requiring significant assistance with activities of daily living, including mobilisation and incontinence care as well as relying on non-verbal communication. Our findings regarding the impact of Montessori-based programmes on engagement were consistent with those from a systematic review conducted by Sheppard et al. (2016). Some helpful tips from previous studies include the duration of the programme, the timing of each training session and the format of the intervention (Chaudhry et al., 2020; Gaspar and Westberg, 2020; Giroux et al., 2010). Specifically, Gaspar and Westberg (2020) noticed a negative association between the length of the programme (more than one year) and the engagement of participants; the longer participants were exposed to the Montessori-based programme, the less positive engagement was observed. Chaudhry et al. (2020) also suggested that each training session should be less than one hour because participants can easily get tired. Future studies should monitor the duration of the programme and each training session to ensure that Montessori-based activities do not exhaust the participants. Gaspar and Westberg (2020) emphasised the importance of training staff about Montessori principles to ensure that it becomes a sustainable and commonplace intervention in dementia care. Giroux et al. (2010) argued that the individual format of Montessori-based activities would be more appropriate for those in moderate to severe stages of dementia in terms of individual cognition and personal preferences as well as more easily modified as needed. Therefore, future Montessori-based programmes design should consider the duration of the programme and the timing of each training session as well as integrating person-centred care in Montessori-based programme design that aims to generate interest among participants and actively engage them in the activities.
Choices regarding data collection tools and the timing of data collection are crucial when designing a plan to evaluate the impact of Montessori-based programmes. Data collection tools measure variables from different perspectives, so selecting the appropriate ones is essential to determine the effectiveness of the Montessori-based programmes. Some tools measure engagement characteristics and intensity, while others measure mood, relationship, and participant behaviours (Chan et al., 2021; Giroux et al., 2010; Wilks et al., 2019). It is important that researchers carefully select measurement tools to ensure that their research questions are answered accurately and precisely. Additionally, collecting data at multiple time points to measure longitudinal outcomes is beneficial. For example, in the studies reviewed, there was a focus on measuring the engagement of participants during Montessori-based activities, but details about the general engagement of participants is unknown. Therefore, increasing the diversity of data collection points could help better understand the impact of Montessori-based programmes. Two longitudinal programmes integrated Montessori-based activities into the daily life activities of participants, but they only used limited data collection points, ranging from three observations at three-month intervals (Wikis et al., 2019) to seven observations in one day (Gaspar and Westberg, 2020). Future studies should consider carefully selecting measurement tools and expanding follow-up data collection points.
Mental health
Over the past two decades, Montessori-based programmes have been applied to address mental health problems in dementia care (Zhou et al., 2021). Our review found that Montessori-based programmes had significantly positive outcomes on affect (mood), agitation, hyperphagic behaviour and prescribing rates for antipsychotic and sedative medications, but had varying impacts on depression. Our review findings were similar to a previous review study (Sheppard et al., 2016) that found Montessori-based programmes generated positive affect (mood) on individuals with dementia. In our review, none of the included studies found significant changes in cognition and anxiety, although it is important to note that many factors could influence the mental health outcomes of individuals with dementia, making it difficult to attribute causation or isolate specific variables. These factors include the format of the intervention (Chan et al., 2021); the cognitive ability of participants (Wilks et al., 2019); the competency of implementers (Mbakile-Mahlanza et al., 2020) and the person-centred care model (Roberts et al., 2015). For instance, our review found that when Montessori-based programmes were conducted in a small groups, individuals with dementia exhibited more social interaction with peers and achieved significant improvements in positive affect (Chan et al., 2021). Additionally, positive affect and engagement had a significantly positive correlation, with more active engagement being positively correlated with more positive affect (Giroux et al., 2010). However, for individuals with late-stage dementia, our review found no significant effects on mental health outcomes like anxiety and responsive behaviours, or even worse, a significant negative effect on the psychological well-being (Wilks et al., 2019). When person-centred care was combined with Montessori-based activities there were notable significant improvements in agitation and prescribing rates of anti-psychotic and sedative medications (Roberts et al., 2015). Furthermore, studies have shown that when both formal (healthcare professionals) and informal (family caregivers) carers with Montessori training implemented Montessori-based activities, there were significant benefits in generating positive affect (Chan et al., 2021; Mbakile-Mahlanza et al., 2020). When individuals with dementia lead Montessori-based activities, with proper training and assistance from staff, they could effectively lead the activities and yield significant positive outcomes in engagement and affect, which can be even better than staff-led activities (Skrajner et al., 2012, 2014). Therefore, when designing Montessori-based programmes, it is important to acknowledge multiple factors and consider their influence on the mental health outcomes of individuals with dementia. To optimise the benefits of Montessori-based activities on the mental health outcomes of individuals with dementia, an ideal Montessori-based programme design should reflect the cognitive and physical capacity of individuals with dementia, be delivered by competent implementers and be integrated within person-centred care programmes.
Feeding difficulty and nutritional status
The review found that the combination of Spaced Retrieval and Montessori-based activities produced significantly better results in nutritional status, body mass index, body weight and food consumption than either Space Retrieval or Montessori-based activities alone (Lin et al., 2010, 2011; Wu and Lin, 2013; Wu et al., 2014). This finding is inconsistent with a previous review that found a significant reduction in eating difficulty after Montessori-based programmes training but insufficient evidence to support an improvement in the nutritional status of participants (Sheppard et al., 2016). A possible explanation for this inconsistency is that the Montessori-based activities training, which lasted 30–40 minutes per session, three times a week for eight weeks, aimed to train the eating abilities such as scooping, squeezing and pouring. This purposeful and repetitive training was more successful in improving feeding difficulty (Lin et al., 2010, 2011; Wu and Lin, 2013; Wu et al., 2014). Interestingly, Montessori-based activities or Space Retrieval alone also had significant improvements in eating difficulty but had no impact on nutritional status, body mass index, body weight and food consumption (Lin et al., 2010, 2011). However, when Spaced Retrieval was combined with Montessori-based activities, significantly improvement in feeding difficulty, nutritional status and food consumption were observed, whether in standardised training sessions or individualised training sessions (Wu and Lin, 2013; Wu et al., 2014). Therefore, it is recommended that Montessori-based activities can be combined with spaced retrieval in future Montessori-based programmes that aimed at improving the feeding difficulty and nutritional status of individuals with dementia in residential aged care.
Activities of daily living and quality of life
Our review found that Montessori-based activities had no impact on activities of daily living and the quality of life of individuals with dementia (Chaudhry et al., 2020; Wilks et al., 2019). Chaudhry et al. (2020) suggested that the small sample size (n = 24) may have contributed to the lack of significant change in activities of daily living and quality of life. It is recommended that future studies use a larger sample size, as the recommended minimum sample size for preliminary studies is 30 (Serdar et al., 2021). Furthermore, it is common for individuals in the late stages of dementia to experience a significant deterioration of activities of daily living or quality of life after Montessori-based training (Wilks et al., 2019). It is essential to consider this when interpreting research findings. Researchers should also consider the potential impact of continuing cognitive decline on the effectiveness of Montessori-based programmes. As individuals with dementia experience ongoing cognitive decline, the effectiveness of Montessori-based programmes may be reduced. Therefore, it is crucial to develop programmes that are appropriate for individuals at different stages of dementia to ensure maximum effectiveness.
The synergistic effect of integrating Spaced Retrieval with Montessori-based activities
Four studies explored the impacts of Spaced Retrieval on the eating ability of individuals with dementia in residential aged care and three of them blended Spaced Retrieval with Montessori-based activities (Kao et al., 2016; Wu and Lin, 2013; Lin et al., 2010; Wu et al., 2014). The synergistic effect of integrated Spaced Retrieval with Montessori-based activities was previously highlighted in the mental health outcome (excessive eating behaviours), feeding difficulty and nutritional status of individuals with dementia. Spaced retrieval is an evidence-based practice that has been used for decades to train the memory of people with dementia (Camp & Schaller, 1989). It achieved positive outcomes in remember simple information (names of people or objects) and verbal cues and behaviours to improve their functional skills. For example, visual cues for safe swallowing for participants with dysphagia, and verbal cues combined with visual cues for participants with toilet orientation difficulty (Bird et al., 1995; Brush & Camp, 1998). Two recent literature reviews discovered that many factors, including the severity of dementia, design of the Spaced Retrieval training (frequency, duration and time intervals between each test), familiarity with the training content and length of staying in the organisation, could influence the outcome of Spaced Retrieval (Creighton et al., 2013; Oren et al., 2014). Specifically, the authors indicate that the earlier the individual with dementia receives Spaced Retrieval training, the better the outcome of the intervention. Similarly, participants who are more familiar with the training content performed better during the training. Furthermore, the authors stated that participants in an increased time interval group (e.g., 1 minute, 2 minutes, 4 minutes, 8 minutes) had better outcomes than those in a fixed time interval group (e.g., 10 minutes time gap in each test). Additionally, participants in continuous days of Spaced Retrieval training (Monday through Friday) performed better than those in interrupted days of training (Monday, Wednesday, and Friday) (Creighton et al., 2013; Oren et al., 2014). To summarise, Spaced Retrieval is recommended for improving the memory, behaviours and functional skills of individuals with dementia and the synergistic effect of combining Spaced Retrieval with Montessori-based activities is also emphasised.
Limitations
There are a few limitations to this review. Firstly, the focus was on the outcomes of Montessori-based programmes for individuals with dementia, while the outcomes of care staff, family members and organisations were excluded. Future research should address these areas to provide a more comprehensive understanding of the impact of Montessori-based programmes. Additionally, some of the included studies did not report effect size or outcomes of dropouts, which reduces the quality of evidence presented in this review. Future research in this area should address these issues to enhance the quality of evidence. Lastly, due to the diversity of methodologies, interventions, and measurement tools used in the included studies, the heterogeneity prevented the possibility of a meaningful meta-analysis.
Conclusion
The systematic review with narrative synthesis summarised the impact of 15 Montessori-based programmes for individuals with dementia living in residential aged care. Of the 15 included studies, three types of Montessori-based activities were observed, conducted in three different formats. The design of Montessori-based programmes, measurement tools and data collection points varied across programmes. The findings showed that Montessori-based programmes significantly improved engagement, mental health outcomes and feeding difficulty. However, there were mixed results in nutritional status, and the synergistic effect of integrating Spaced Retrieval with Montessori-based activities in improving eating ability and nutritional status of individuals with dementia was also emphasised. There were no significant changes in activities of daily living and quality of life. Future Montessori-based programmes designers would highly recommend tailoring personalised Montessori-based activities to individual care needs, cognitive ability and personal preference. Practitioners also need to consider the purpose of their Montessori-based activities to determine whether a group or individual format will be most appropriate. More research into Montessori-based activities is needed for recreational purpose and to improve the health care outcomes of individuals with dementia living in residential aged care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author Ms ZMY is a fully funded PhD student who receives tuition fees from The University of Wollongong and stipends from the China Scholarship Council.
Ms.
Professor
Dr
Dr
Dr