
Abstract
Introduction
Recent estimations have projected a threefold increase in dementia prevalence in Aotearoa New Zealand (NZ) by 2050, particularly in Maori and Pacific peoples. However, to date, there are no national data on dementia prevalence, and overseas data are used to estimate the NZ dementia statistics. The aim of this feasibility study was to prepare the groundwork for the first full-scale NZ dementia prevalence study that is representative of Māori, European, Pacific and Asian peoples living in NZ.
Methods
The main feasibility issues were: (i) Sampling to ensure adequate community representation from the included ethnic groups, (ii) Preparing a workforce to conduct the fieldwork and developing quality control, (iii) Raising awareness of the study in the communities (iv) Maximizing recruitment by door-knocking, (v) Retaining those we have recruited to the study and (vi) Acceptability of study recruitment and assessment using adapted versions of the 10/66 dementia protocol in different ethnic groups living in South Auckland.
Results
We found that a probability sampling strategy using NZ Census data was reasonably accurate and all ethnic groups were sampled effectively. We demonstrated that we were able to train up a multi-ethnic workforce consisting of lay interviewers who were able to administer the 10/66 dementia protocol in community settings. The response rate (224/297, 75.5%) at the door-knocking stage was good but attrition at subsequent stages was high and only 75/297 (25.2%) received the full interview.
Conclusions
Our study showed that it would be feasible to conduct a population-based dementia prevalence study using the 10/66 dementia protocol in Māori, European and Asian communities living in NZ, utilizing a qualified, skilled research team representative of the families participating in the study. The study has demonstrated that for recruitment and interviewing in Pacific communities a different but culturally appropriate approach is required.
Keywords
Background
The World Health Organisation (WHO) has classified dementia as a global public health priority (World Health Organisation, 2012) (1). Advocacy, awareness-raising, developing specific dementia policies and plans, supporting caregivers and research are some of the actions needed to improve dementia care and services. The WHO recommends these actions to be context-specific and culturally relevant (World Health Organisation, 2012). It also encourages countries around the world to include dementia on their public health agendas and to coordinate these actions across national, regional, and local levels. The extent and impact of dementia in Aotearoa New Zealand (NZ) is not completely understood as there are no community-based national dementia prevalence data available. The NZ estimated total resident population is over 5 million (Statsistics New Zealand-Tatauranga Aotearoa, 2018a; 2018b), and by extrapolating data from other countries (with similar development levels), the prevalence of dementia in NZ has been projected to increase from 60,000 cases in 2015 to 170,000 cases in 2050 (Deloitte Report for Alzheimer’s New Zealand, 2017).
NZ is officially recognised as a bicultural country comprised of Māori and non-Māori populations. Non-Māori populations include NZ Europeans, Asian (the majority being Chinese and Indian), Pacific Island (the majority being Samoan, Cook Island, Tongan and Fijian), and Middle Eastern, Latin American and Africans (MELAA). Statistics NZ (Tatauranga Aotearoa) allows people to self-identify with more than one ethnic group and reports that in 2018 70.2% of the NZ population self-identified as NZ Europeans, 16.5% as Māori, 15% as Asian, 8% as Pacific Island, 2% as MELAA, and 1% as other ethnicities (Statsistics New Zealand-Tatauranga Aotearoa, 2018a; 2018b). Māori, Asian and Pacific Island populations are growing and ageing at a faster rate than NZ-Europeans, and thus the prevalence of dementia is expected to increase more rapidly in these communities (Ma’u et al., 2021). Accurate community-based dementia prevalence information for Māori, Asian and Pacific peoples living in NZ is unavailable. The calculated dementia prevalence based on administrative data in 2019-2020 was 5.8% for Māori, 6.4% for Pacific, 3.7% for NZ European, and 3.4% for Asian in the age 60+ population; and 18.8% for Māori, 22.7% for Pacific, 13.6% for European, and 13.3% for Asian in the age 80+ population (Cheung et al., 2022). These data are based on diagnostic coding and therefore do not include people with unidentified and/or undiagnosed dementia in these communities. Access to diagnostic services may differ across ethnic groups, for example, it has been reported that Asian peoples living in NZ are more likely to have undiagnosed dementia compared to NZ Europeans (Martinez-Ruiz et al., 2020). Older adults in some ethnic groups may be at a higher risk of dementia, due to increased prevalence of the cardiovascular and metabolic risk factors associated with dementia (Feigin et al., 2015; Joshy & Simmons, 2006; Simmons et al., 1999; Thornley et al., 2011). A study using routinely collected data at a memory service in South Auckland has shown that Māori and Pacific people are diagnosed with dementia at an earlier age compared to NZ–Europeans (Cullum et al., 2018), which could be a result of earlier onset and higher rates of obesity, hypertension and type 2 diabetes mellitus (Feigin et al., 2015; Joshy & Simmons, 2006; Simmons et al., 1999). The life-course social determinants may also play an important role in increasing the risk of developing dementia in these communities (Dudley et al., 2019). An example of such social determinants in the Māori community is the on-going effects of colonisation, such as difficulties accessing health care services, low levels of education, and discrimination (Ellison-Loschmann & Pearce, 2006; Graham & Masters-Awatere, 2020).
To develop culturally appropriate and responsive services for dementia in NZ the true extent and impact of dementia in all the major NZ ethnic groups must be accurately estimated. This will provide a foundation to measure “the full impact of dementia, raise public awareness, reduce stigma and inform policy development regarding the implementation of evidence-based prevention, treatment and support services for people with dementia and their families” (Martinez-Ruiz, Yates, et al., 2021).
The aim of this study was to assess the feasibility of (i) sampling a multi-ethnic population to ensure adequate representation of the major NZ ethnic groups and (ii) using adapted versions of a standardised dementia diagnostic assessment tool, the 10/66 dementia protocol (Prince et al., 2007), to measure dementia prevalence as well as the psychological and economic impact of dementia on families in those communities.
Methods
Feasibility Questions, Used Methodology and Outcome Variables.
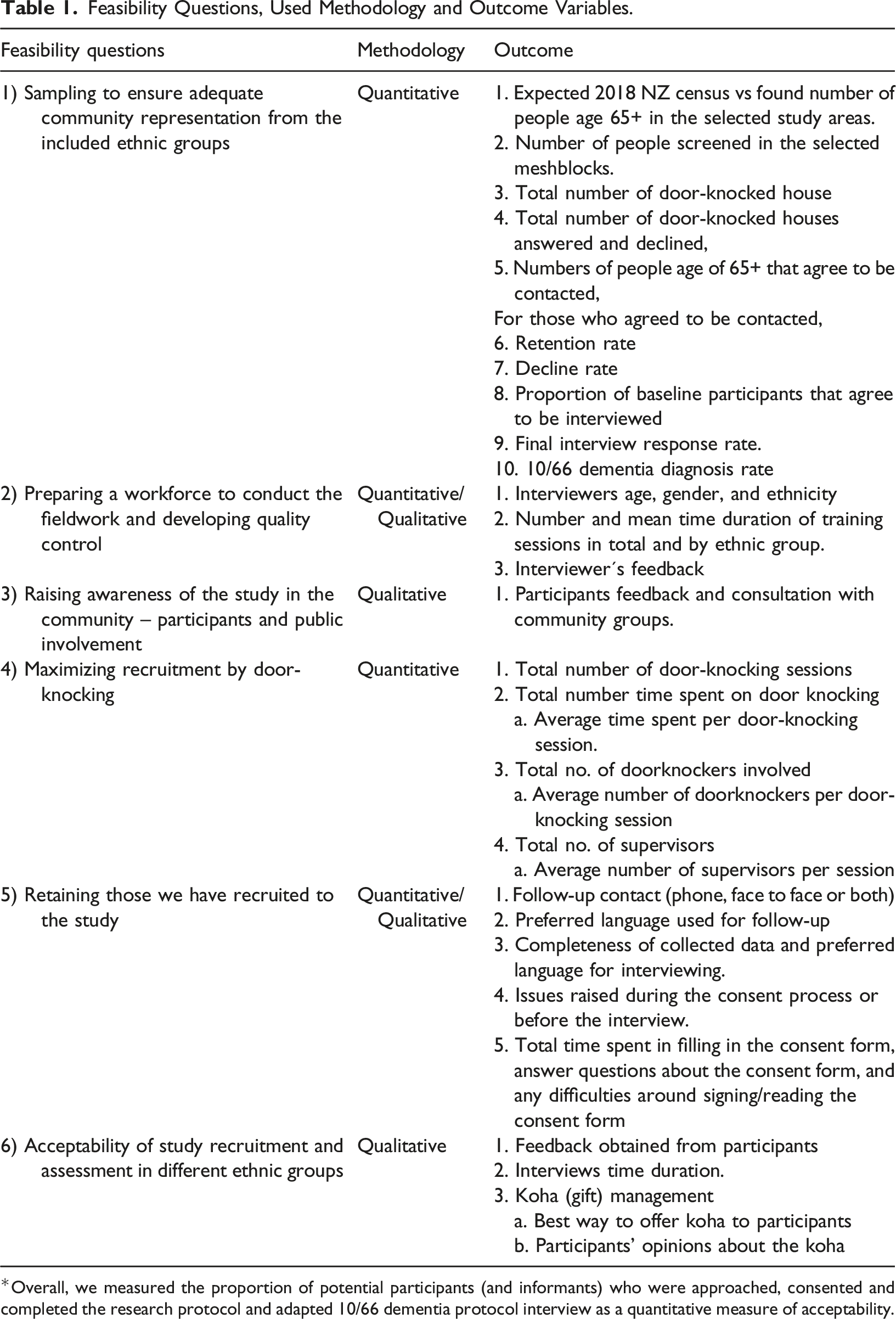
*Overall, we measured the proportion of potential participants (and informants) who were approached, consented and completed the research protocol and adapted 10/66 dementia protocol interview as a quantitative measure of acceptability.
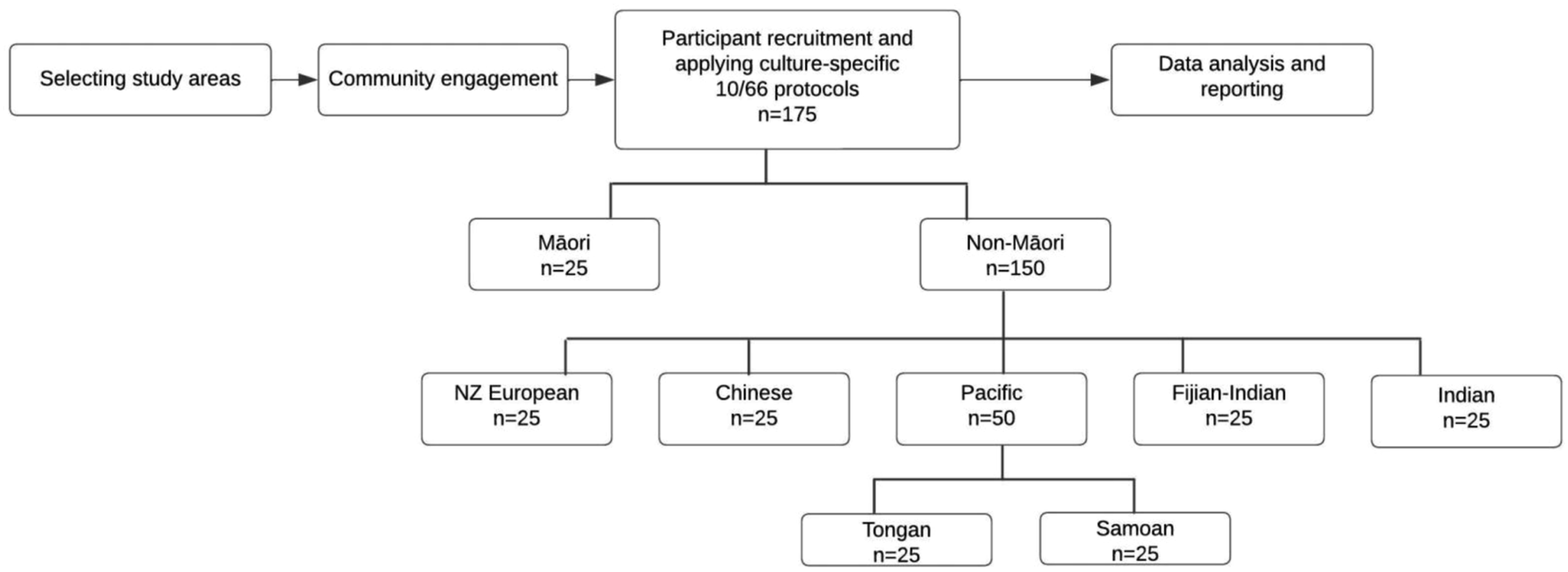
LiDiA feasibility study design.
This study was approved by the New Zealand Northern A Health and Disability Ethics Committee – New Zealand Government/Ministry of Health (ref number: 18NTA176).
Study Setting and Population
We selected South Auckland as our study site because of its ethnically diverse population. The demographic profile for the 65+ population living in South Auckland is 7% Māori, 12% Pacific Peoples, 20% Asian, and 60% NZ European (Winnard et al., 2015). This contrasts with the national 65+ population of 6% Māori, 3% Pacific Peoples, 6% Asian and 83% NZ European (Statsistics New Zealand-Tatauranga Aotearoa, 2018a; 2018b). Door-knocking was used to identify and recruit potential participants. The inclusion criteria were people who (i) self-identified as one of the seven included ethnic groups; (ii) were aged 65 years or over; (iii) were living in private residences; and (iv) had an informant willing to participate in the study. People living in long-term care facilities or retirement villages were excluded. Written consent was obtained from all participants and informants.
Instruments
10/66 dementia assessment sections.
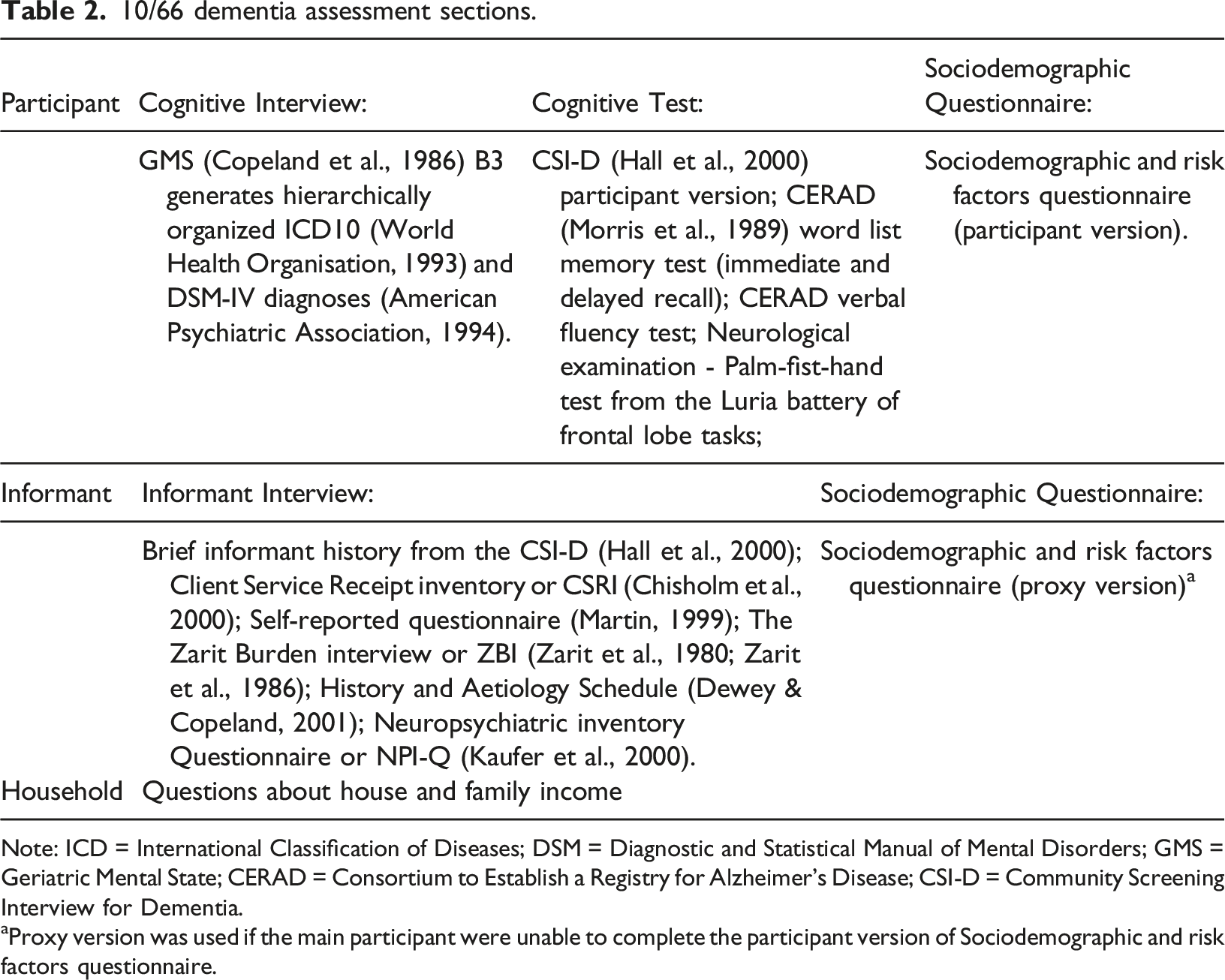
Note: ICD = International Classification of Diseases; DSM = Diagnostic and Statistical Manual of Mental Disorders; GMS = Geriatric Mental State; CERAD = Consortium to Establish a Registry for Alzheimer’s Disease; CSI-D = Community Screening Interview for Dementia.
aProxy version was used if the main participant were unable to complete the participant version of Sociodemographic and risk factors questionnaire.
Six feasibility questions were addressed in this study (Table 1) and the methods for each are described below:
Sampling to ensure adequate community representation from the included ethnic groups
A standard population-based sampling procedure (meshblock sampling and door-knocking) was used to identify and recruit a representative sample of participants from the seven ethnic groups. The expected number of dementia cases and the probabilities of finding them in adults aged 65+ in each of the main ethnic groups were calculated using sociodemographic data from the NZ Census information for every Statistics NZ statistical area in South Auckland (Statsistics New Zealand-Tatauranga Aotearoa, 2019a; 2019b; 2019c). We selected geographical areas with the highest probability of finding people aged 65+ for each ethnicity, and then selected meshblocks within those areas that maximised the probability of finding older people from the main ethnic groups when door-knocking in that neighbourhood. Meshblocks are defined as “the smallest geographic unit for which Statistics NZ has demographic information” (approximately 100 people) (Statsistics New Zealand-Tatauranga Aotearoa, 2016a; 2016b). We selected two study areas each comprising up to 10–20 meshblocks (defined as Study Area 1 and Study Area 2) and door knocked all houses included in those areas. All older adults who met inclusion criteria (including those within the same household) were invited to participate in the study. Study Area 1 had a high probability of finding age 65+ adults from Māori, Samoan, Tongan and Indian backgrounds; while Study Area 2 had a higher probabiliy of finding people from Chinese background. Both study areas had a moderately high NZ European population. We aimed to recruit 25 participants per ethnic group included in the study to test the accuracy of the sampling methods.
Table 1 lists the outcomes to be reported which include 2018 NZ Census expected vs found number of people in the selected areas, total number of people screened in the selected meshblocks, numbers of houses door knocked and answered, numbers of people who accepted and declined door-step interview, numbers of people aged 65+ in each ethnic group that agreed to be further contacted and their response rates.
Preparing a workforce to conduct the fieldwork and developing quality control
Lay interviewers were recruited using electronic resources such as university website or email or through contacts from people/students/health professionals known to the study’s lead investigator or co-investigators. Interviewers were bicultural and bilingual, identified with at least one ethnicity of Māori, NZ European, Chinese, Indian, Fijian-Indian, Tongan and Samoan. Non-European interviewers were able to speak English and at least one ethnic group language fluently. For practical and safety reasons, the interviews were to be conducted by pairs of interviewers in which one interviewed the participant and the other the informant. The interviewers were fully trained by following culture-specific protocols for each ethnic group and the specific steps of the training process have been thoroughly described elsewhere (Martinez-Ruiz, Yates, et al., 2021). Quality control was carried out as part of the training. For example, interviewers practiced the 10/66 dementia protocol interviews with each other and with older volunteers, and constructive feedback was provided by the study’s principal investigator and/or lead co-investigator and a dementia specialist. In addition, the first three 10/66 dementia protocol interviews with study participants were conducted also under their supervision.
For the purpose of the feasibility study, we report the interviewers’ gender and ethnicity as well as the number and mean time duration of training sessions. The interviewers’ feedback regarding the training, participant engagement and interviewing process are also reported. Interviewers’ feedback was obtained via scheduled videoconference meetings for each ethnic group. The questions asked included: 1) are there any changes that you would recommend for the training? 2) are there any changes you would recommend for the interviews? 3) any things that worked well? 4) any things we need to add or do differently? 5) any specific cultural and/or language issues that arose during the process? 6) any issues we need to approach differently for cultural and/or language reasons? Additionally, feedback was obtained from interviewers throughout the process, both on an individual level and at regular update meetings. These meetings took place once per week throughout the duration of the data collection study phase. The interviewers’ feedback was collected by a research assistant, transcribed verbatim and handed to the lead investigator or lead co-investigator. This allowed for specific issues to be raised and resolved during the period that the interviews were being conducted.
Raising awareness of the study in the community – participants and public involvement
We aimed to gather information that would inform the co-design of a study launch strategy for the main study. Therefore in the feasibility study we engaged with communities through local non-governmental organisations serving older people in different ethnic groups, to raise awareness three to four months before the start of recruitment, and to devise a launch event for the feasibility study. These activities would aid strategy development for the main study.
Maximizing recruitment by door-knocking
Door-Knocking Initial Questionnaire.
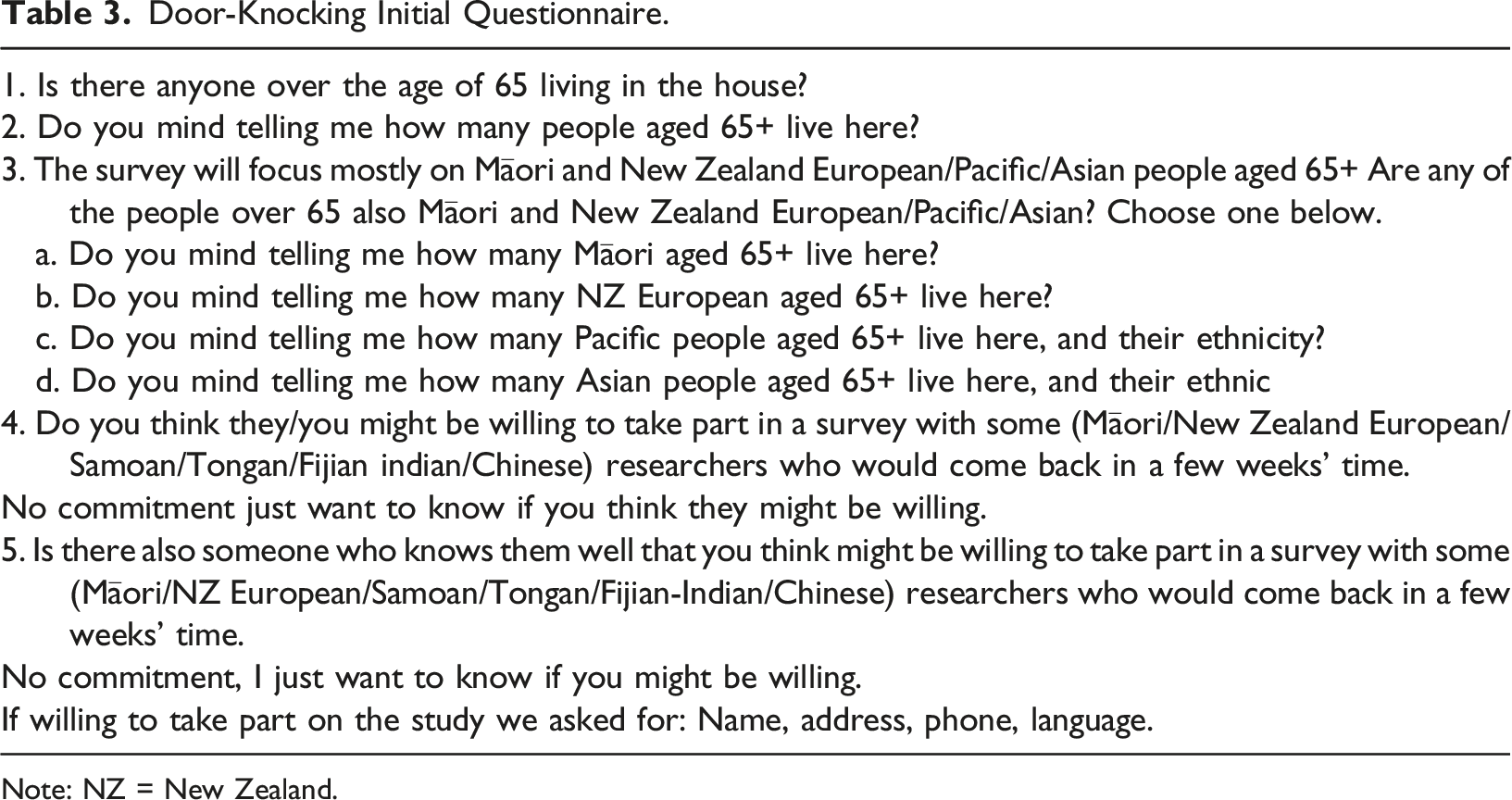
Note: NZ = New Zealand.
Retaining those we recruited to the study at the door-knocking stage
After the potential participants and informants agreed to participate in the research, they were contacted to set up an appointment for the interview. The appointment was organized by one of the ethnic-specific lead co-investigators or someone designated by them. Taking into consideration what was most culturally appropriate, participants were contacted either face-to-face (preferred by Māori for example), by telephone, or both. In addition, and depending on the participant preferences, the communication was made either in their native language (te reo Māori, Mandarin/Cantonese, Hindi, Fijian-Hindi, Tongan or Samoan) or in English. We reported, in total and by ethnic group, the number of people contacted either by phone, face-to-face or both, preferred language used for contact and for interview, and completeness of interview data. Feedback was obtained from the interviewers regarding any issues raised during the consent process or pre-interview cultural protocols. A gift of $100 (NZD) was given to each family that participated in the full 10/66 interview as recognition and appreciation of the time involved.
Acceptability of study recruitment and assessment in different ethnic groups
Feedback from the participants was obtained after the 10/66 dementia protocol interview, and included the following questions: (i) Did the interview go okay? (ii) Were there any things you really enjoyed about the interview? (iii) Was there anything that worried you? and (iv) Do you have any other comments? The questionnaire administration, and gift management were also assessed to evaluate the acceptability of the study recruitment and assessment. The feedback was obtained either immediately following the interview or via a follow up phone call or by a follow-up face-to-face visit. The responses were recorded verbatim by the interviewers and the main issues identified were summarised and reported in the results.
Data Analysis
Descriptive analysis was used to report the overall findings and by ethnic groups. Means, standard deviations are reported for continuous variables, while rates, percentages and proportions were reported for categorical variables. Dementia diagnosis was made using the 10/66 dementia diagnostic algorithm described previously (Martinez-Ruiz & Krishnamurthi et al., 2021). Deductive thematic analysis was used for textual data.
Results
Sampling to Ensure Adequate Community Representation From the Included Ethnic Groups
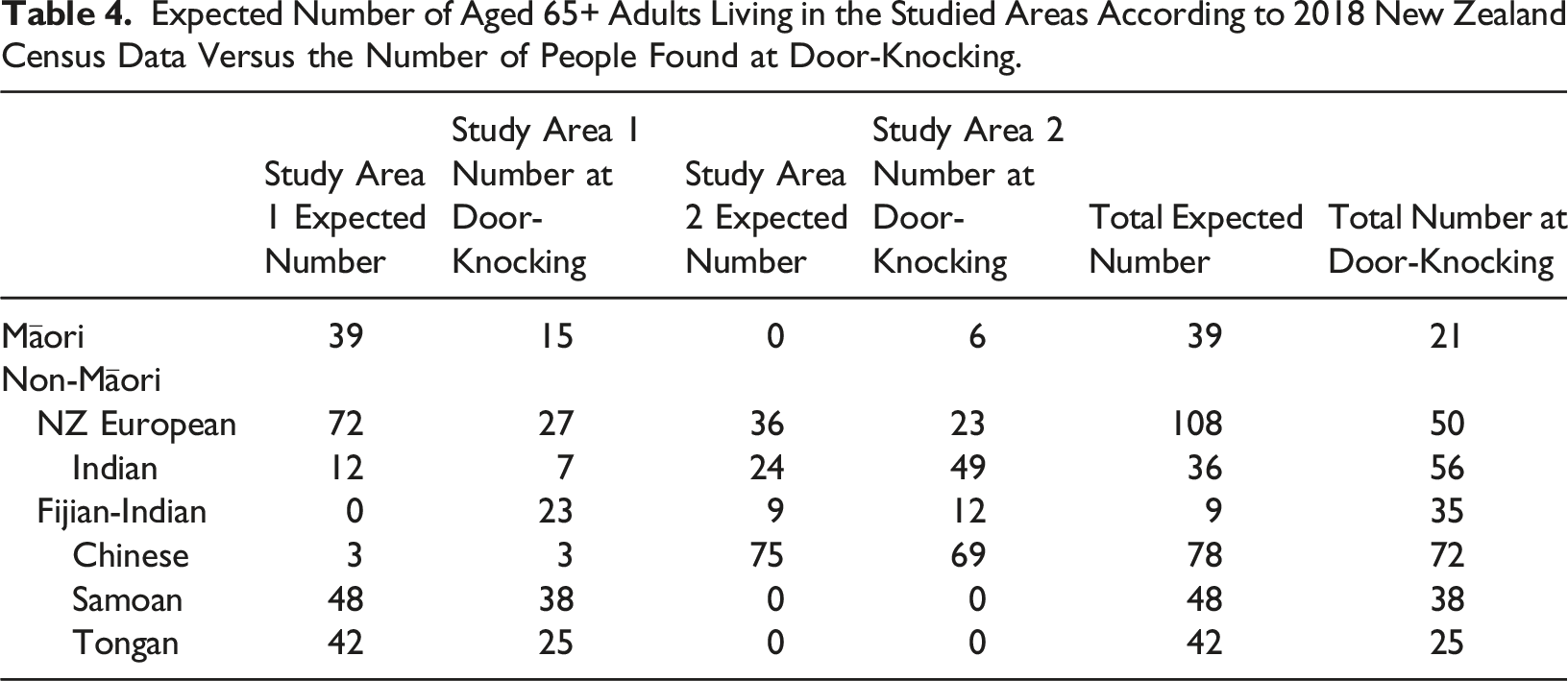
Expected Number of Aged 65+ Adults Living in the Studied Areas According to 2018 New Zealand Census Data Versus the Number of People Found at Door-Knocking.
A total of 1,607 houses were door-knocked in the selected areas. Of these, 297 potential participants met the inclusion criteria in the 1278 (89.1%) houses that answered, and 224/297 (75.5%) agreed to be further contacted. The retention and decline rate at follow-up, proportion of baseline participants that agreed to be interviewed, final interview response rate as well as the 10/66 dementia rate are described in Figure 2. Recruitment processes. hh = number of houses, p = number of participants.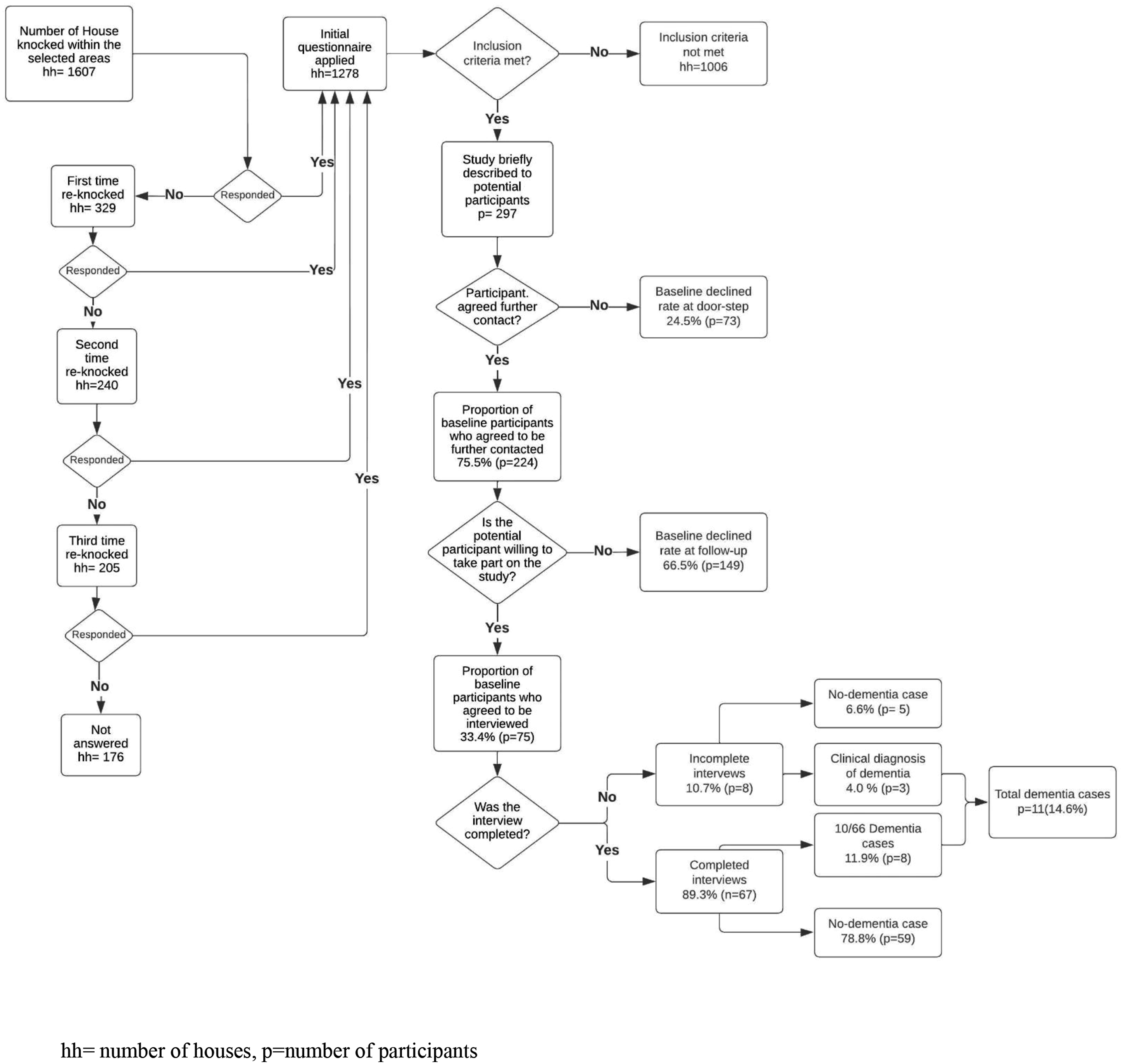
Preparing a Workforce to Conduct the Fieldwork and Developing Quality Control
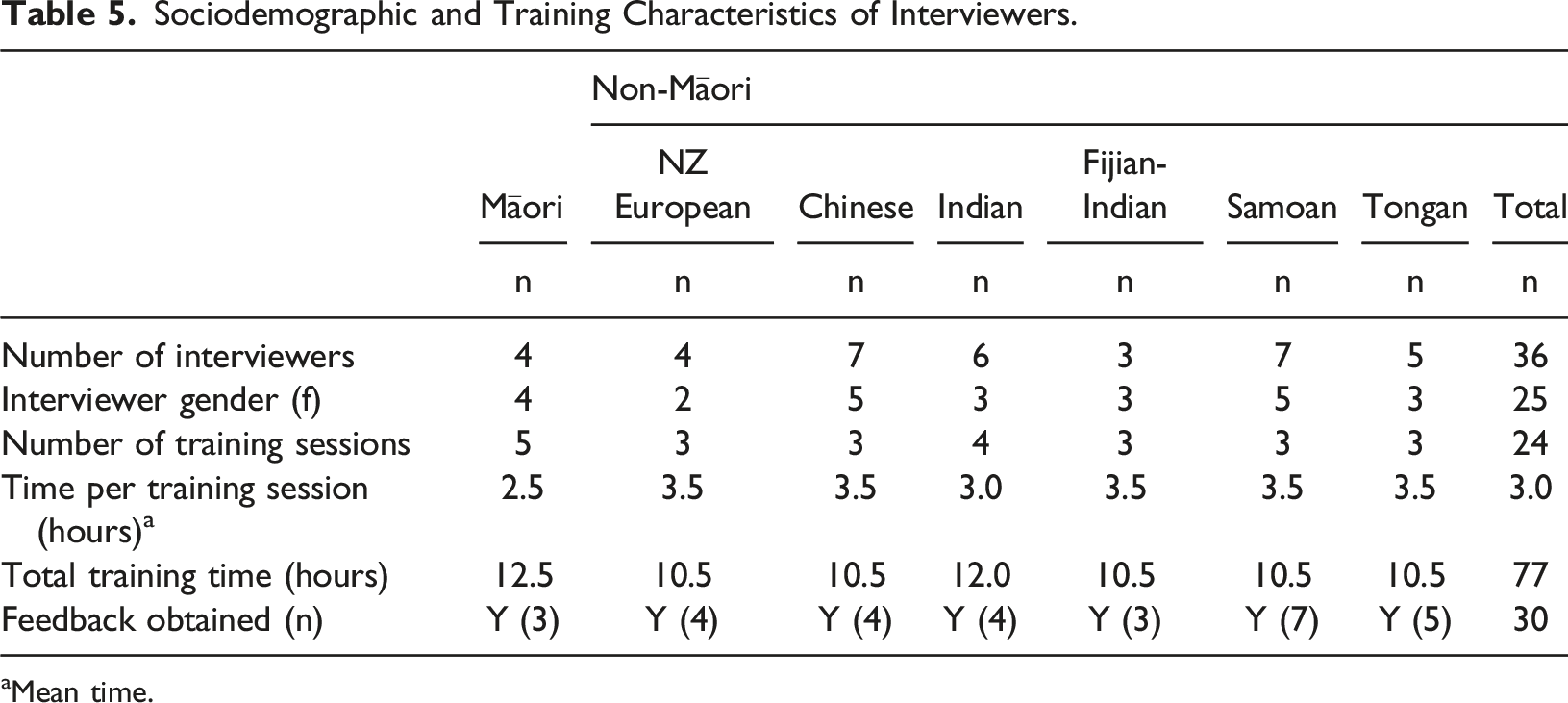
A total of 36 interviewers were recruited for the feasibility study, and 25 (69.4%) were female. We initially recruited Tongan medical students to interview in Tongan communities however the Pacific expert advisory group felt that this would not be culturally appropriate because younger people should not interview older people about sensitive subjects. They advised that well-respected older women in the community were recruited as interviewers instead. Consequently, we outsourced the Samoan and Tongan arms of the study to a local Pacific research group, Moana Connect (https://www.moanaconnect.co.nz), in order to maximise recruitment and retention.
Sociodemographic and Training Characteristics of Interviewers.
aMean time.
Feedback from the interviewers was classified into five main topics: a. Translation, adaptation and administration of the questionnaires: (i) The appropriateness of some of the topics in the questionnaires might be taboo in some cultures, for example, suicidal ideation and questions regarding sexuality, (ii) Continuing concerns about stigma around dementia in some of the communities and whether this would affect recruitment. b. Interviewers’ dementia knowledge: Some study participants wanted to learn more about dementia and available support but interviewers were unable to provide this information. Interviewers would benefit from some basic dementia training and be provided with translated written information about dementia which could been given as a “gift” to thank the participants. c. Interviewer and study participant safety: The importance of interviewing in pairs for safety reasons was acknowledged but was sometimes inconvenient for arranging interviews due to conflict in availability of interviewers (who were employed on a casual basis). The participants’ time commitments and their own conflict with time schedules of interviewers was also raised. d. Engagement with participants: There was a need to provide more training to the doorknockers and interviewers on how to present the research as friendly and time-efficient to potential participants because (i) some participants/families were concerned about being “scammed” by doorknockers; (ii) there were concerns about confidentiality such as how the research results will be used and shared; (iii) some potential participants were concerned about time commitments and perceived the interview as too long. e. Improving logistics and follow-up: Interviewers made suggestions to improve logistics regarding scheduling and follow-up on interviews, interviewers, and participants' availability. Some of the potential participants may have lost interest in the study if they were not followed up promptly (however we were also limited by a lengthy COVID-19 lockdown in this respect).
Raising Awareness of the Study in the Community – Participants and Public Involvement
We initially raised awareness and informed older people in the selected ethnic groups about the study by offering dementia education sessions through organisations providing care for older people in those groups, e.g, Dementia Auckland (www.dementiaauckland.org.nz), Chinese Positive Ageing Charitable Trust, Shanti Niwas Day centre for Indian elders (https://shantiniwas.org.nz/day-programmes), and Vaka Tautua (https://www.vakatautua.co.nz/). We also organised a multi-ethnic feasibility study launch at the University marae (sacred Māori meeting house) and invited members from the different communities to contribute with traditional music and dance from their own cultures. The study launch was very popular and generated much enthusiasm, but we also found that it caused some confusion about who was eligible for the study, and there was disappointment for some who were not eligible to participate because we were targeting specific geographical areas. We addressed this by making leaflet drops (which included all the languages of the study) to mailboxes in the selected areas which was much more effective in targeting the appropriate sampling frame. The leaflets were produced in English and the other major languages of each area (te reo Māori, Samoan, Tongan, and Hindi in Study Area 1; Chinese and Hindi/Fijian-Hindi in Study Area 2). The leaflet content included introducing the principal investigator, an outline of the study and an invitation to participate. Most study participants that we spoke to on the doorstep told us they knew about the study beforehand due to the leaflet delivered to their mailboxes by the study team. Feedback sessions about the study were conducted in the same local non-governmental organisations serving older people in different ethnic groups and a cross-cultural interest group was conducted with Asian health professionals regarding the best ways to conduct dementia research in their communities (Cheung et al., 2019).
Maximizing Recruitment by Door-Knocking
Door Knocking Sessions Characteristics.
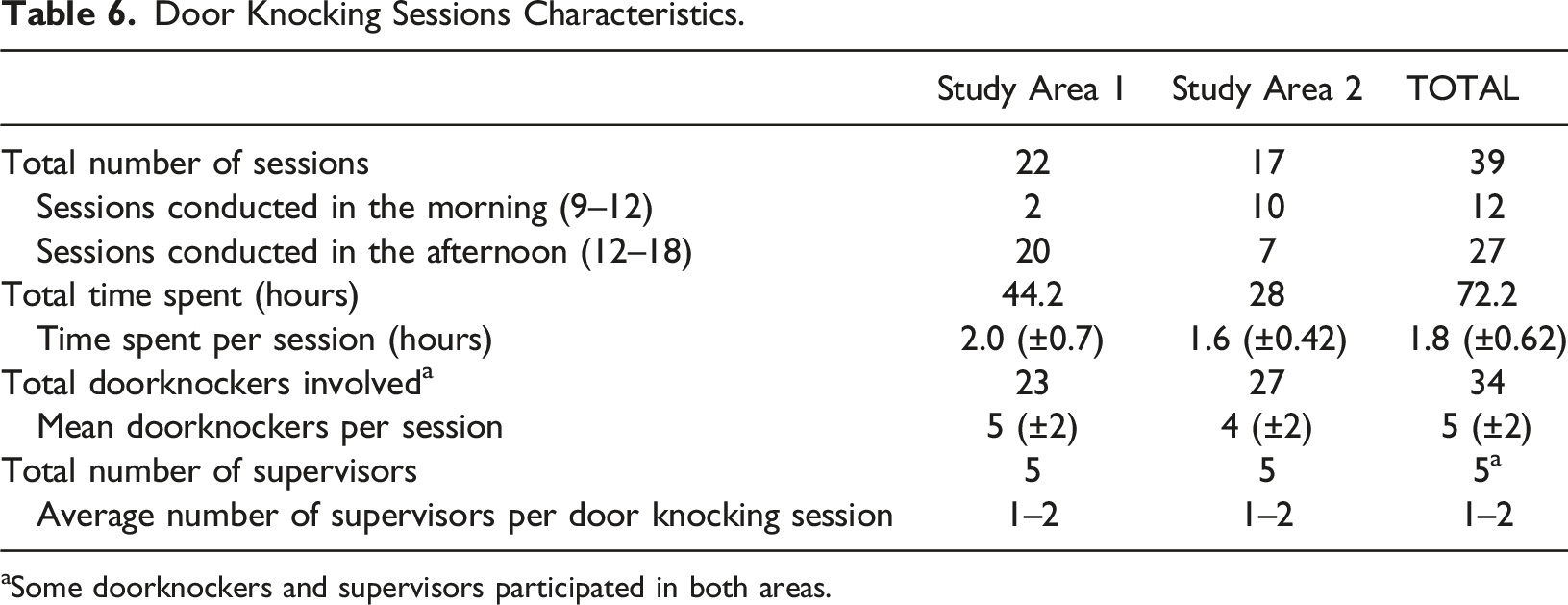
aSome doorknockers and supervisors participated in both areas.
Retaining Those Recruited to the Study
Out of 224 potential participants who agreed to be followed up after the door-knocking, 194 were followed up by telephone, 25 by face-to-face contact, and 5 required both telephone and face-to-face approaches. Sixty-six participants selected English as the preferred follow-up language, and 158 participants preferred follow-up in their own (non-English) language.
Number of People Over 65 and Outcome of Initial and Follow-Up Contact by Ethnic Group in Answered Houses.
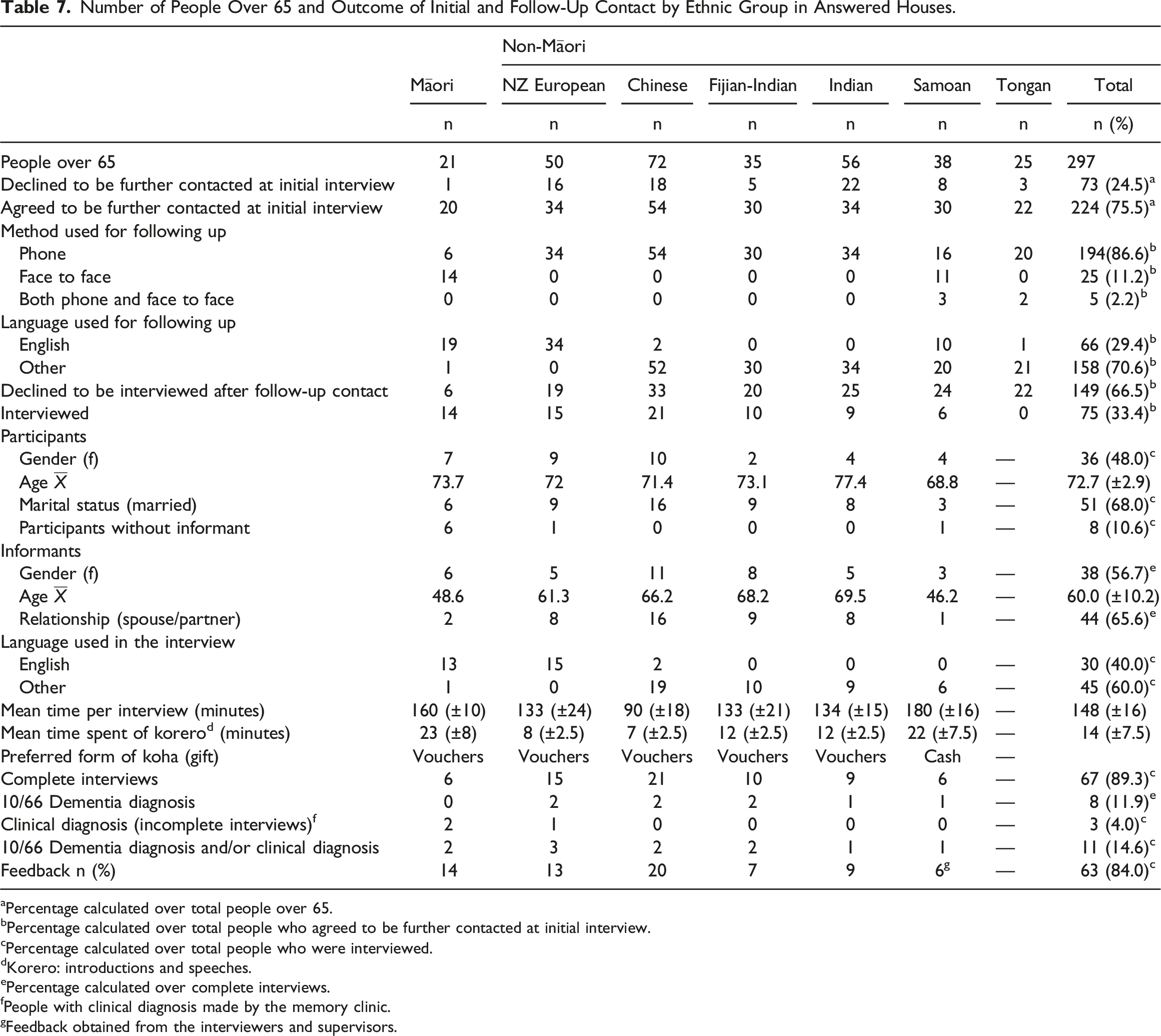
aPercentage calculated over total people over 65.
bPercentage calculated over total people who agreed to be further contacted at initial interview.
cPercentage calculated over total people who were interviewed.
dKorero: introductions and speeches.
ePercentage calculated over complete interviews.
fPeople with clinical diagnosis made by the memory clinic.
gFeedback obtained from the interviewers and supervisors.
Acceptability of Study Recruitment and Assessment in Different Ethnic Groups
All participants responded in the affirmative to the feedback question: “did the interview go okay?” To the question, “were there any things you really enjoyed about the interview?” two participants in the NZ European group said they did not enjoy the interview but did not elaborate further on the reasons. To the question “was there anything that worried you?” four Māori participants expressed being worried about their final cognitive test score, one NZ European participant responded that it was “a long interview,” and another was “worried about being able to answer the questions.” Most of the non-European participants expressed their appreciation for having the opportunity to be interviewed in their own language. Most expressed gratitude for the supermarket voucher given at the end of the interview, but some of the Pacific participants expressed a preference for cash instead as they did not use the supermarket. Feedback response rate by ethnic group is summarized in Table 7.
Discussion
Our results showed that a dementia prevalence study is feasible in NZ, however there are significant challenges conducting such a study in a multi-ethnic community. We found that the probability sampling strategy using NZ Census data was reasonably accurate and all ethnic groups were sampled effectively. We demonstrated that we were able to train up a multi-ethnic workforce consisting of bi-cultural bi-lingual lay interviewers who were able to administer the 10/66 dementia protocol in community settings. The response rate (224/297, 75.5%) at the door-knocking stage was good but attrition at subsequent stages was high and only 75/297 (25.2%) received the full interview. The low response rate might result in selection bias, so recruitment methods would need to be adjusted in a full study to maximise data collection. The decline rate at first contact (24.5%) and at follow-up (66.5%) suggests that we need to maximise data collection at first contact. For example, this might include a short cognitive test at the door-step in those who consent, which, although not providing a diagnosis, might indicate sources of bias and/or potential prioritisation for further stages.
Our findings mirrored other studies in which ethnic minorities are less likely to participate in clinical and epidemiological studies (Fisher & Kalbaugh, 2011; Konkel, 2015; Milani et al., 2021; Patel et al., 2020). For example, a systematic review of barriers and facilitators to minority research participation in the US (George et al., 2014) found that the key participation barriers faced by ethnic minority groups are mistrust and consequent fear of participation, stigma related to research participation, and competing demands. Another study found that Hispanic individuals were less willing to participate in studies that may be seen as invasive or demanding (Milani et al., 2021). It has been also reported that due to lack of trust in research and language barriers, Asian Americans were less willing than other racial groups to participate in health research (Liu et al., 2019). Similar to our study, the Cognitive Function and Ageing Study I and II (Gao et al., 2015), that included older people aged 65 years and over, found that at follow up the decline rate was higher (45.3%) compared to the first phase of the study (18.3%), and reported that deprivation status and female sex were more likely to predict decline in the follow up phase. Occupation, education, health, and attitudes to medical science and belief have been also described as factors influencing the participation willingness of ethnic minorities in research (Smart & Harrison, 2017).
High rates of attrition in our study were partly due to unavailability of informants living at the same residence. Statistics New Zealand have reported that, along with NZ Europeans, Māori have the highest rates of people over the age of 65 living alone (Statsistics New Zealand-Tatauranga Aotearoa, 2016a; 2016b), thus making it more difficult to find an informant. A cross-sectional study amongst older adults living in NZ reported that Māori and NZ Europeans had the highest rates of people living alone by 38% and 52% respectively, when compared to Pacific Peoples (16%) and Asians (18%) (Jamieson et al., 2018). The Health, Work, and Retirement Study conducted in NZ found that older Māori were more likely to feel lonely, and had weaker perceptions of social support when compared to non-Māori (Stephens et al., 2010). A recent study on frailty in older people were referred for home care services in NZ, reported higher rates of Māori participants who were widowed, separated, never married, and divorced compared to other ethnic groups included in the study (Abey-Nesbit et al., 2021). A more flexible approach might be required to gather informant information and maximise participation, for example re-visiting homes at alternative times, accepting alternative informants, and/or interviewing the informants by telephone.
Although Pacific participants were more likely to have an informant living at home, attrition was highest amongst the Samoan and Tongan communities. The feedback received from the Pacific interviewers and their supervisors’ included concerns about stigma around dementia in these communities, participants and relatives having other time commitments, and avoiding interviewers (despite multiple attempts to contact them). It was also reported that the method of recruitment was not culturally appropriate for Pacific communities and that more work was required to co-design effective recruitment strategies in these communities. The Samoan and Tongan interviewers highlighted the importance that, in future studies, engaging community leaders (e.g., church leaders) and identifying other sources for disseminating information about the research to give the study more credibility in the Pacific communities. In addition, the length of the interview and some questions included in the interview were considered taboo and not culturally appropriate. Interviews lasted for over 3 hr in some cases, and the time reported to finish the interviews in the Samoan group was the longest of all ethnic groups. This was due to an increased time required to i) develop relatedness and trust before the interview commenced, ii) further elaborate on terminology and explain terms in the appropriate languages. Due to the lengthy interviews, participants often would feel tired or unable to answer questions and expressed their wishes not to continue with the interview. Also, some difficulties were identified during the interview regarding Samoan and Tongan translations used in the 10/66 interview. For example, there is no Samoan term for ‘depression’. There is stigma associated with some topics, for example, the negative transliteration of the term “mental” – even when it means “mental wellbeing”. The Samoan Expert Advisory Group (SEAG) emphasised the need for interviewers to elaborate on certain questions that may not be immediately clear to participants to prevent confusion among participants and informants. These issues have been identified in other studies requiring cross-cultural adaptation of similar surveys (Farina et al., 2022). Providing consistent context across the interview process would ensure responses captured by the families are as accurate as possible. The issues found in the Samoan and Tongan groups might be mitigated by raising awareness (and reducing stigma) around dementia in Pacific communities, developing culturally appropriate tools and models of care to assess cognitive decline in those families, and further Pacific-led research with regards to dementia.
Although our over-sampling for non-European ethnic groups was successful, we found a larger than expected number of Māori, Chinese, Fijian-Indian and Indian participants in one of the study areas, and a larger than expected number of Fijian-Indian participants in the other study area, compared to the predicted numbers calculated using the 2018 NZ Census data (Statsistics New Zealand-Tatauranga Aotearoa, 2016a; 2016a). These findings are important for future studies as the accuracy of the NZ Census is essential for sample calculation by area. The discrepancies found between our results and the 2018 NZ Census might be explained within intrinsic factors in 2018 NZ Census such as response rate (2018 NZ Census 83.3% compared to 92.2% for the 2013) (Statsistics New Zealand-Tatauranga Aotearoa, 2019a; 2019b; 2019c), or extrinsic factors such as the rate of residential mobility among the studied populations, (e.g. the 2018 CM Health Census reported that only 39% of CM Health residents were living in the same house as they were 5 years before the census, which in term can indicate a high rate of residential mobility)(Lees et al., 2021).
Regarding awareness-raising we found that targeting the specific geographical areas was likely more effective than a broader approach through local organisations, radio or social media, but the latter methods may be more suited to a fully powered dementia prevalence study. In particular our interviewers fed back that dementia knowledge about dementia was poor (for both interviewers and participants) so an overall strategy to improve dementia education might be beneficial and would help the interviewers to collect complete data and encourage continued participation (Lavrakas, 2008).
There are some other limitations that need to be acknowledged: (i) The study was designed to address feasibility issues and was not a pilot study designed to provide data for subsequent sample size calculation for a larger fully-powered study (Browne, 1995; Julious, 2005; Sim & Lewis, 2012), however our finding that approximately 14.6% of people met diagnostic criteria for dementia (see table 7) is aligned with previous similar studies (Prince et al., 2003). (ii) Due to the unavailability of bilingual bicultural researchers and interviewers, and budget constraints, not all of the major ethnic groups in New Zealand were included in the study, thus the findings may not be applicable to the overall NZ population. (iii) We only included people aged 65 years or over but we know that future studies will need to include a younger population as there is some evidence that certain ethnic groups (e.g. Māori and Pacific peoples) are at higher risk of developing dementia at a younger age due to higher prevalence of modifiable risk factors (Cullum et al., 2018). (iv) This study only included people recruited from people living in the community, but a fully powered dementia prevalence should also include populations from different settings (e.g. long-term care facilities and retirement villages). (v) Our study was carried out in a multi-ethnic urban area, but different strategies may be required to recruit participants in rural areas in NZ. (vi) The Samoan and Tongan versions of the 10/66 dementia protocols used in this study were not adequately validated due to spectrum bias, as the participants in the (unpublished) validity studies had more severe dementia and very few had mild dementia, causing spuriously high sensitivity and specificity. Further research is required if the 10/66 dementia protocol is to be used for a prevalence study in the NZ Pacific communities.
Conclusion
Overall, our study showed that it would be feasible to conduct a population-based dementia prevalence study using the 10/66 dementia protocol in Māori and some non-Māori communities (NZ Europeans, Chinese, Indian and Fijian-Indians). The study has demonstrated that recruitment and interviewing in the Samoan and Tongan communities will require an alternative more culturally appropriate approach. Our study has demonstrated the benefits of recruiting a qualified, skilled research team that is representative of the families participating in the study. NZ-specific robust evidence regarding the number of people affected by dementia, as well as its risk factors, caregiver distress, and financial implications on families are needed to develop culturally informed policies. A national prevalence study will help to address those issues and to raise public awareness about dementia. It will also help to develop culturally appropriate services that support families living with dementia in all NZ communities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Brain Research New Zealand, Health Research Council of New Zealand.
Ethical Approval
The Living with Dementia in Aotearoa (LiDiA): a feasibility study for a dementia prevalence study in Māori and Non-Māori living in New Zealand was approved by the Northern A Health and Disability Ethics Committee, Number: 18NTA176. The findings will be disseminated through peer-reviewed academic journals, national and international conferences, and public events.