
Abstract
When dealing with the challenges of dementia, spousal relationships have a central role to play in outcomes such as quality of care and emotional wellbeing. Dementia places strain on these relationships and so it is important to develop interventions to support them. This review maps out what interventions have been employed in this context. Searches of PsycInfo, PsycArticles, CINAHL, Embase, MEDLINE, and Web of Science were conducted to find studies describing interventions that aimed to improve some aspect of the relationship. Thirty-four studies were identified. A wide range and diversity of interventions were described, including life review, psychotherapy and ones focused on communication or creative activity. Reported benefits included meaningful interaction, emotional connection, reduced conflict and negativity, an increase in mutual support, and greater equality in the relationship. However, these can only be considered as potential rather than proven benefits because of the lack of methodological rigour of most of the studies. Future research on this topic would benefit from a closer links with research on the impact that dementia can have on spousal relationships, and from the use of stronger methodology.
Introduction
The importance of family relationships in dementia is increasingly recognised. Dementia can have a major impact on these relationships and, in turn, the quality of those relationships can impact on how well those involved cope with the challenges posed by the dementia (Ablitt et al., 2009; Edwards et al., 2018; Quinn et al., 2009). Spousal relationships may be particularly important in this context because of the closeness of the relationship (‘spousal’ is used in this paper to refer to both marriages and partnerships). Dementia can often have a negative impact on the quality of this relationship. Spousal caregivers have frequently reported reductions in communication and companionship, in empathy and reciprocity, and in affection and intimacy, leading to an overall increase in dissatisfaction (Ablitt et al., 2009; Evans & Lee, 2014; Quinn et al., 2009). Some caregivers also report changes in their feelings towards their partner; a perception that the person with dementia feels like a stranger to them; and a perception that the relationship has changed from a marriage to a relationship characterised by the giving and receiving of care (Evans & Lee, 2014; Riley, 2019; Riley et al., 2013). Similarly, people with dementia have also described reductions in physical and emotional intimacy, and in communication and companionship (Alsawy et al., 2020; Clark et al., 2019; Harris, 2009; Wawrziczny et al., 2016), along with an increase in friction within the relationship, and feelings of being side-lined and ignored as the caregiver takes over (Clare & Shakespeare, 2004; Svanström & Dahlberg, 2004).
The quality of this relationship is, in turn, associated with the emotional well-being of the caregiver (Ablitt et al., 2009; Chunga et al., 2021; Riley et al., 2018) and the quality of the care they provide (Riley et al., 2020; Williamson & Shaffer, 2001). A good spousal relationship is also associated with less cognitive and social deterioration on the part of the person with dementia (Burgener & Twigg, 2002; Nordheim et al., 2009) and a reduced likelihood of moving to institutional care (Wright, 1998). Good relationships are also, of course, of intrinsic worth to those involved.
Given the value of the spousal relationship, it is important that interventions are developed to help couples maintain a good relationship as they deal with the challenges of dementia. The research literature contains a wide diversity of interventions intended to support spousal couples. Several scoping and systematic reviews of this literature have been published (Bielsten & Hellström, 2019a, 2019b; Moon & Adams, 2013; Rausch et al., 2017). These reviews have focused on any intervention involving the couple, not just on those that aimed to sustain or improve the relationship. Consequently, much space in these reviews is taken up with considering other outcomes such as cognitive function or emotional wellbeing rather than relational outcomes. A review focused more narrowly on relational outcomes would enable a more detailed consideration of this issue. Another issue about these reviews is that they operated with relatively strict inclusion criteria (e.g. both members of the couple had to attend the intervention together and both had to be living together in the community) and this resulted in a relatively small number of studies being reviewed. There is some merit in operating with looser inclusion criteria to gain a broader perspective on what interventions have been developed.
The current study builds on these previous reviews by operating with looser inclusion criteria and by focusing on literature describing interventions that were intended to improve some aspect of the spousal relationship. A scoping review was selected because the main purpose was to map the extent and nature of the literature on the topic (Grant & Booth, 2009; Peters et al., 2020). Consistent with the broad review purpose, dementia was taken to include a broad range of dementias (Alzheimer’s Disease, Vascular Dementia, Dementia with Lewy bodies, frontotemporal and mixed dementias) and all stages of the disease were included (mild, moderate and severe). Similarly, interventions were broadly defined to include any intervention that used a psychosocial activity with the intention of facilitating some aspect of the couple’s relationship. The review was therefore not confined to psychological therapies derived from some theoretical perspective (e.g. cognitive-behavioural therapy). Finally, all research designs were included. This inclusive approach aligns with scoping reviews which are well placed to answer broad descriptive questions about complex and heterogenous literature (Arksey & O'Malley, 2005; Peters et al., 2020; Pham et al., 2014). The diversity of the literature reviewed made it less appropriate to conduct a systematic review or meta-analysis focused on conclusions about therapy effectiveness.
The objectives of the scoping review were to: • To describe and categorise the psychosocial interventions that have been used to enhance some aspect of the spousal relationship. • To describe in general terms the designs and methodologies that have been used. • To summarise the benefits from these interventions that have been reported.
Method
Arksey and O’Malley’s (2005) framework for conducting scoping reviews, updated by Peters et al. (2020), guided the review. The first stage, defining the research questions, has been outlined in the Introduction. Details of the other three stages are outlined below. The scoping review was planned and conducted by a team consisting of a PhD researcher working academically in the field of dementia (first author) and two clinical psychologists (second and third author) one of whom has experience of working with dementia clinically and in a research capacity (third author).
Search strategy and identification of potential studies
Search terms.
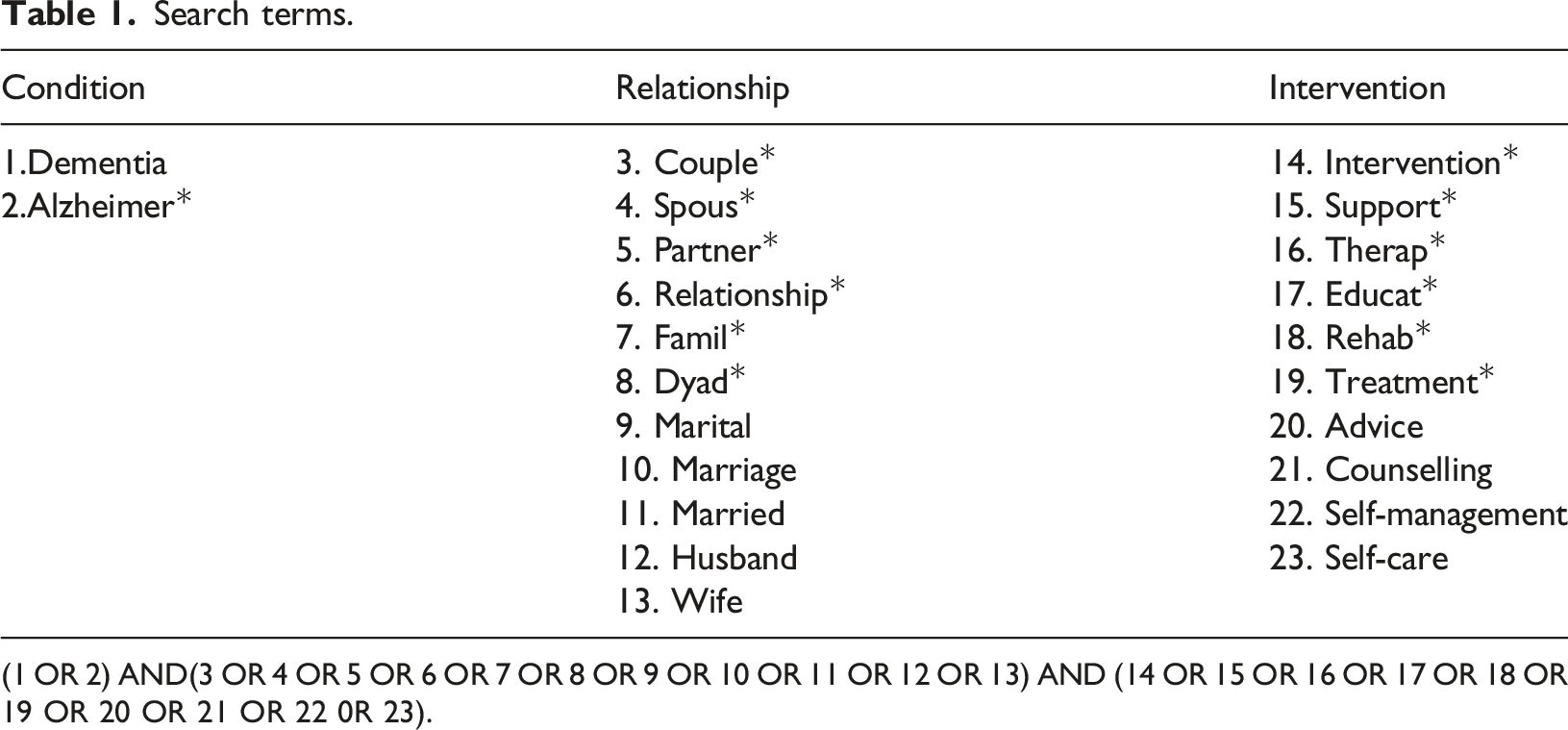
(1 OR 2) AND(3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 OR 11 OR 12 OR 13) AND (14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 0R 23).
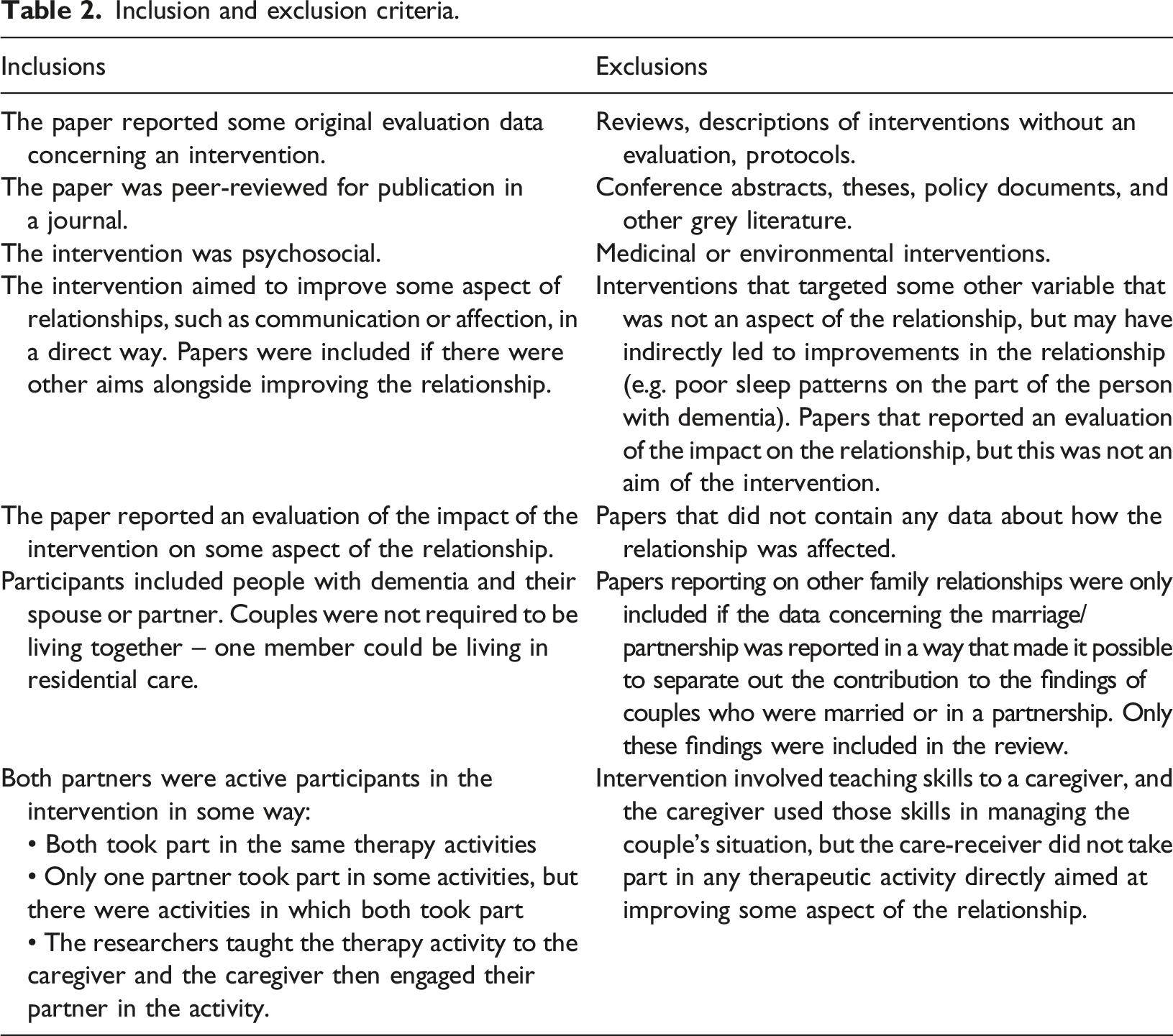
Inclusion and exclusion criteria.
Study selection
Study selection was conducted by screening all papers against the criteria outlined in Table 2. Papers were exported into Endnote and, at the first step, all duplicates were removed. At the next step, titles and abstracts were screened for eligibility. Finally, the full text was retrieved for papers that could not be excluded at the screening phase and they were read to enable a decision about whether they met the inclusion criteria. Due to limited resources, the screening was conducted by the first author. Any papers about which there was uncertainty of their eligibility, were discussed with the third author and decisions resolved by consensus.
Extracting and summarising the data
Summary of included studies.

Results
The search of the databases yielded a total of 90,235 papers. After 52,703 duplicates were removed, 37,532 titles and abstracts were screened for eligibility. Of these, 37,291 were excluded, with 241 retrieved for the full text screening. At this stage, 207 were excluded for the reasons presented in Figure 1, leaving 34 papers to be included in the review. Prisma chart showing selection strategy.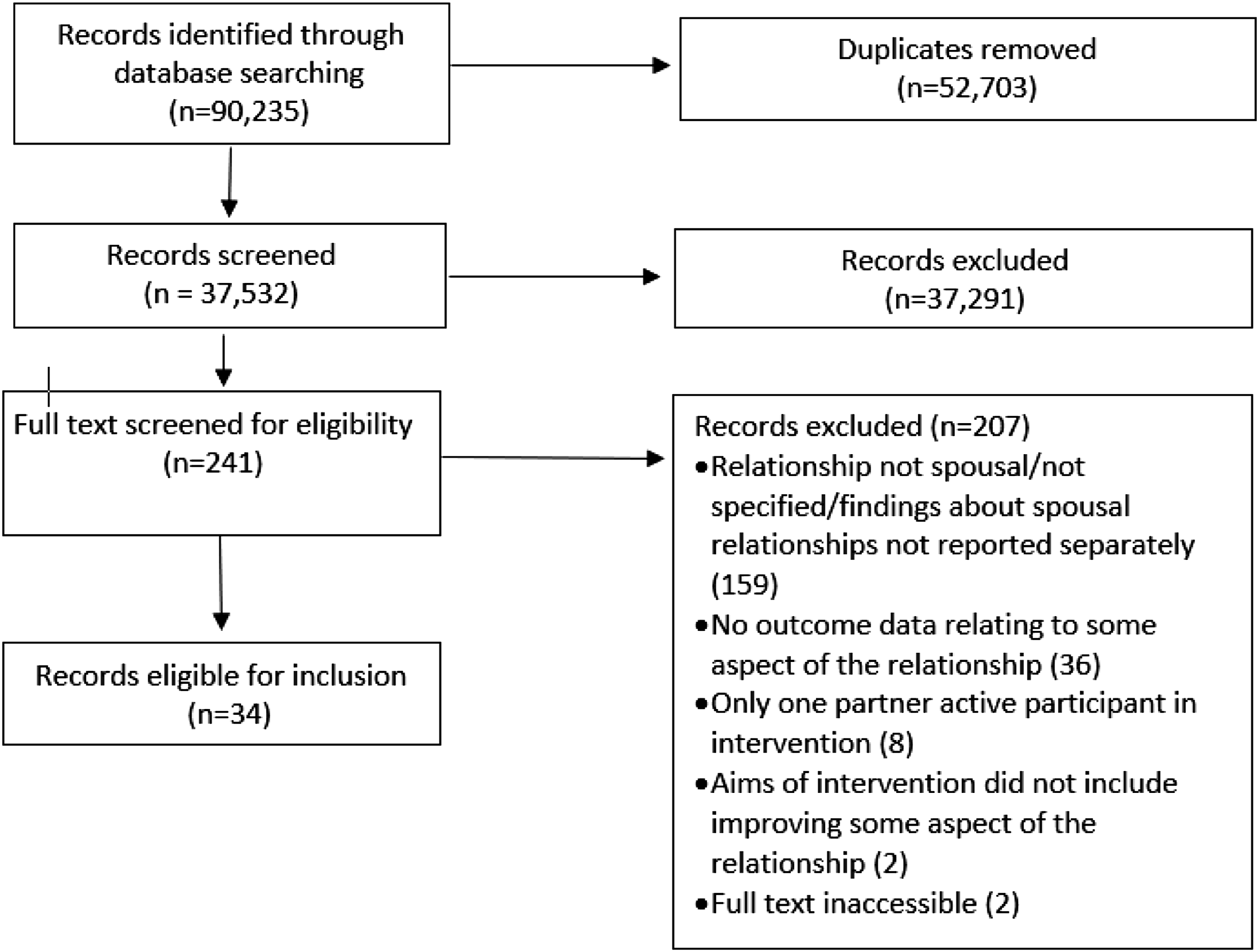
Table 3 gives a summary description of each included paper. One study (Quayhagen et al., 2000) compared the outcomes of four interventions, three of which were eligible for inclusion. These three interventions are entered separately in Table 3. The papers by Williams et al. (2018 and 2021) report different evaluations of the same study; and the paper by Kindell et al. (2019) reports on the same case study that was described in the study by Kindell et al. (2018). Again, these papers are entered separately in Table 3. Thus, there were 34 papers, 36 entries in Table 3, but only 32 studies.
Table 3 provides the following information about each of the included studies: • The type of intervention. • The number of participants. • The stage of dementia they had reached and the location of the study. • A description of the intervention, the aims of the intervention that addressed the relationship, and how it involved the couple (i.e. whether it was delivered to both together, separately etc.). • The design and methodology of the study, including whether there was any follow-up assessment of outcome and whether the outcome of the follow-up was reported separately in the findings section. • The outcomes concerning the relationship, including whether any limitations to the intervention had been noted in the paper.
Only those aspects of the study that were relevant to the aims of this review are included in the table (e.g. there is no information about aims not directly related to the couple relationship, and no details about outcome measures unrelated to the relationship or associated findings). Papers are grouped in Table 3 according to the type of intervention they evaluated.
Participants
Fifteen of the 32 studies failed to report on the stage of the dementia process reached by the care-receiver (defined in terms of scores on the Mini-Mental State Examination or an equivalent). In the remaining studies, the full range was represented, from severe to mild, but those with severe dementia were participants in only five studies. Unsurprisingly, the studies that provided some form of verbal psychotherapy did not involve people with severe dementia. Most of the studies were conducted in North America or Europe, with the remaining being from Australia (3), South Korea (2), China (1) and Japan (1).
Interventions
A wide range of interventions were evaluated in the included studies. To summarise these, they were divided into several broad categories based on their central therapeutic element: • Narrative (10 entries in Table 3): The primary aim of these interventions was to guide couples to reflect on their life together through reminiscing about the past or through creating a story of their life together. • Creative (8 entries): These interventions involved some form of imaginative, expressive, or artistic activity, such as painting, dancing, or singing. • Communication (11 entries): The aim of these interventions was to improve communication between the couple. Some of them focused on developing communication skills, but others were focused on the use of aids to facilitate conversation, such as a digital camera that recorded events of the day and thereby enabled conversation about those events (Karlsson et al., 2014). • Psychotherapy (4 entries): These interventions were based on the application of established psychotherapeutic approaches to identify and resolve issues that challenged the relationship. The approaches included counselling psychology, cognitive-behaviour therapy, and a psychoanalytic couples therapy. Two of the studies were linked, in that one was a pilot for the other (specifically, Epstein et al., 2007 was a pilot for Auclair et al., 2009). • Miscellaneous (3 entries): It was difficult to classify these studies under any of the above categories, either because they used several different components and no component appeared to be the central therapeutic component (e.g. Chung, 2001), or because the intervention was not similar to that used in any of the other studies (e.g. Bielsten et al., 2020).
These categorisations are somewhat artificial because there was often an overlap. For example, the creative interventions frequently involved some element of reminiscence, such as singing songs that had personal meaning (Unadkat et al., 2017); and the Couples Life Story Approach that was used in several studies classed as narrative also involves teaching communication skills.
Although all the studies aimed to improve the relationship and reported relational outcomes (as per the inclusion criteria), enhancing aspects of the relationship was not the exclusive aim of many of the interventions. For example, the intervention described by Nordheim et al. (2019) also aimed to maintain the independence of the care-receiver and the mental wellbeing of the couple through interventions such as relaxation exercises and adaptations to the home environment.
Perhaps due in part to the fact that enhancing the relationship was not the exclusive or primary aim of some of the studies, many of them did not provide a detailed theoretical rationale for how the intervention could be expected to benefit the relationship. For example, Melhuish et al. (2019) discussed the potential benefits of music therapy in dementia, but the benefit for the relationship was only one of several benefits listed and was not considered in detail. Some studies, however, stated the supposed benefits for the relationship without any account of how the intervention might bring about these benefits (e.g. Chung et al., 2021; Hamill et al., 2012; Sweeney et al., 2021). Others did provide a more detailed rationale (e.g. Balfour, 2014; Clark et al., 2021, Ingersoll et al., 2013). However, even in these more detailed accounts, there were often some gaps. For example, Ingersoll-Dayton et al. (2013) in their account of the Couples Life Story Approach state that one of the aims of the approach is to highlight the adaptability and resilience of the couple in their past lives together, but they do not explain the value of doing this.
In 26 of the 36 table entries, both members of the couple took part in the same intervention together. Five entries involved training the caregiver to engage in the therapeutic activities with the care-receiver, while the remaining five entries involved the couple receiving some components of the intervention together, but some separately.
Study design and methodology
In terms of study design, only three of the 32 studies were randomized controlled trials. Nine studies did not have a control group but took measures before and after the intervention (labelled in Table 3 as ‘pre-post-intervention’). The remaining 20 studies had no control group and only took post-intervention measures. Uncontrolled studies, particularly those that do not take any pre-intervention measures, do not provide a firm basis for drawing conclusions about the effectiveness of an intervention.
A range of data collection methods were used. Quantitative methods primarily involved the use of questionnaires, but some studies used quantitative coding of recorded interactions between the couple (e.g. Williams, et al., 2018). In most cases, the questionnaires were established measures of satisfactory reliability and validity, but in a few cases questionnaires or rating scales with untested psychometric properties were used (e.g. Melhuish et al., 2019). Qualitative methods primarily involved interviews or open-ended questions, but data was also gathered from notes taken by the therapist or an observer during the session; notes completed by the therapist after the session; team discussions; recordings of the couple interacting with one another; and diaries and logs kept by the caregiver. Quantitative methods were used in the minority of studies (11 in total).
Apart from four studies that quantitatively evaluated recorded interactions between the couple, and two studies that logged observations made during session, all the other studies relied on self-report, either from the therapist or the participants. Self-report is more prone to bias.
The description of qualitative methods often lacked sufficient detail. Some studies that used interviews or open-ended questions did not provide any information about what questions were asked (e.g. Ekström et al., 2017). For other methods of collecting qualitative data (e.g. caregiver diaries, therapist notes, observations), it was often not specified whether these followed a structured format or it was left to the person completing them to decide what was worth recording (e.g. Karlsson et al., 2014). Unsystematic data collection is also prone to bias.
In terms of analysis, of the 11 studies that used quantitative methods, five provided only descriptive statistics and did not analyse the data (e.g. Ekstrom et al., 2017) and two (Bourgeois, 1992; Epstein et al., 2007) failed to report the data from questionnaires they had used. Failing to complete statistical analysis means that it was not possible to eliminate the explanation that any changes were due to chance. Numerous qualitative studies failed to indicate whether the data were analysed using a systematic method such as conversational analysis or grounded theory. Not using systematic methods of data analysis places the findings of these studies at risk of researcher bias.
Finally, only three studies collected follow-up data in a systematic manner, with a further four studies reporting a follow-up but failing to state whether the data were collected in a systematic manner. In three of these seven studies (Dassa, 2018; Dupuis & Pedlar, 1995; Hill et al., 2020), findings from the follow-up were not reported separately from the main findings and so it was not possible to determine what information was obtained at follow-up.
Relational outcomes
In terms of the reported benefits for the relationship, a different picture emerged from the qualitative and quantitative studies. Whereas all the studies using a qualitative approach reported benefits for at least some participants, quantitative methods provided mixed evidence of benefit.
Eight studies used questionnaires to evaluate outcome. Two of these (Bourgeois, 1992; Epstein et al., 2007) failed to report the outcome data and three provided only descriptive statistics (Baker et al., 2012; Melhuish et al., 2019; Quayhagen et al., 2000). These descriptive statistics provided no convincing evidence that the intervention had been beneficial (see Table 3). Two of the remaining three papers reported that the intervention did not have a statistically significant impact (Ha et al., 2021; Nordheim et al., 2019). The remaining paper (Quayhagen & Quayhagen, 2001) provided inconsistent evidence. The intervention group showed significantly less decline than a waiting list control in the first study, but not in the second study; and, in the first study, there was no significant benefit relative to a placebo group, suggesting that any benefit may not have been due to the specific nature of the intervention. The three randomised controlled trials included in this review are all among these papers that used questionnaires (Nordheim et al., 2019; Quayhagen et al., 2000; Quayhagen & Quayhagen, 2001). There was therefore no quantitative evidence from these trials that the interventions had any specific therapeutic effect.
Four studies extracted quantitative data from recorded interactions between the couples. This method provided some evidence of benefit. Three of the studies reported improvements, but did not statistically analyse the data (Bourgeois, 1992; Ekstrom et al., 2017; Troche et al., 2019). Williams et al. (2018) reported statistically significant improvements in communication across sessions (apart from those living with more severe dementia) and, in an analysis of different findings from the same study, Williams et al. (2021) also reported significant improvements in some aspects of communication, but other aspects appeared to deteriorate.
The relational outcome data collected using qualitative methods primarily came from participants reporting on their experience of the therapy sessions, therapists reporting on progress in the sessions, or recorded conversations between the couple that were set up as part of the study. Consequently, most of the evidence relates to benefits occurring within the therapy sessions themselves and there was relatively less information about what impact the intervention may have had on the lives of the participants outside the sessions. Some studies did ask participants about the broader impact of the intervention (e.g. Bourgeois, 1992; Dupuis & Pedlar, 1995; Kwak et al., 2018), although it is difficult to determine how many did this because of the failure of numerous studies to specify what questions had been asked (see Table 3). For example, the interview described by Kwak et al. (2018) (who used the Couples Life Story Approach) included questions about participants’ intentions to use the life story book after the intervention had ended and their ongoing use of the communication advice they had been given.
Related to the lack of information about the impact on everyday life, there is even less evidence about long-term benefits. As noted earlier, only four studies reported follow-up data separately from post-intervention data. Two of these did not collect the data in a systematic way and reported longer-term benefits (Dassa et al., 2020; Kindell et al., 2018). Two collected the data systematically and one found longer-term benefit (Bourgeois, 1992) but the other did not (Nordheim et al., 2019).
To summarise the benefits reported by the studies, a list of potential topics was made from the research described in the Introduction about the relationship changes that occur after dementia and from the constructs measured by the relationship questionnaires, that were used to guide the selection of studies. Each finding for each paper was then allocated to one of these topics. If the finding did not fit an existing topic, then a new topic was created; and the label of some of the topics was changed to better reflect the benefits reported. This resulted in the following categories of benefits that were reported or observed for some participants: • Enjoyment: Participants reported that the intervention provided the opportunity for the couple to enjoy one another’s company by taking part in the activities associated with the intervention. • Meaningful interaction: Related to this, participants reported that the activity provided an opportunity to connect and relate to one another in a meaningful way, something which could otherwise be relatively absent from their lives together. • Communication: The skills of the caregiver in managing communicative interactions with the care-receiver were improved. The contribution of the care-receiver to conversations was increased, as was the length of those conversations. Some interventions also facilitated communication with one other about thoughts and feelings relating to the other and to their situation. • Emotional connection: Some interventions created an emotional connection between the couple, allowing them to feel greater intimacy, affection, and closeness to one another. Associated with greater understanding (see below), participants could also feel more compassion and empathy for their partner. Interventions involving life review could create a sense of gratitude for the other person and their life together. • Reduced negative feelings: Conversely, greater understanding could reduce feelings of resentment and blame that the caregiver felt towards the care-receiver. • Reduced conflict: Interventions that increased the caregiver’s understanding could also reduce conflict in the relationship, as could interventions focused on reducing anxiety and improving mental wellbeing. • Mutual support: Some interventions allowed couples to be more supportive of one another, increasing their collaboration in facing the challenges of living with dementia and their sense of togetherness. • Appraisals of other person: Interventions could provide the caregiver a better understanding of the communication needs of the care-receiver, their emotions and their behaviour – leading to reduced conflict and negative feelings, and greater empathy. Interventions could also help the caregiver appreciate the residual strengths and abilities of the care-receiver. This could enhance the sense that they have an identity separate from the dementia, and help strengthen the relationship by helping the caregiver appreciate that the care-receiver was still the same person. • Appraisals of the relationship: Similarly, interventions could strengthen the relationship by reconnecting with its past form and escaping from the caregiver and care-receiver dynamic. They could also help participants appreciate their strength and resilience as a couple. • Equality: Associated with appraisals of the other person and the relationship, some studies reported a greater balance and equity in the relationship. Working together on an activity that revealed residual strengths in the care-receiver meant that the relationship felt more equal. In one study, a caregiver reported feeling a reduced need to control their partner.
Table 3 shows which of these outcomes were reported by each study. As an aid to appreciating the frequency of these outcomes, they are depicted as a word cloud in Figure 2, which was generated using online software (https://www.freewordcloudgenerator.com/). To construct this, a frequency count of the relational outcomes was conducted based on the entries in Table 3. The word cloud presents more frequently identified outcomes in larger font, and those less frequently identified in smaller font. Word cloud depicting frequency of reported relational benefits.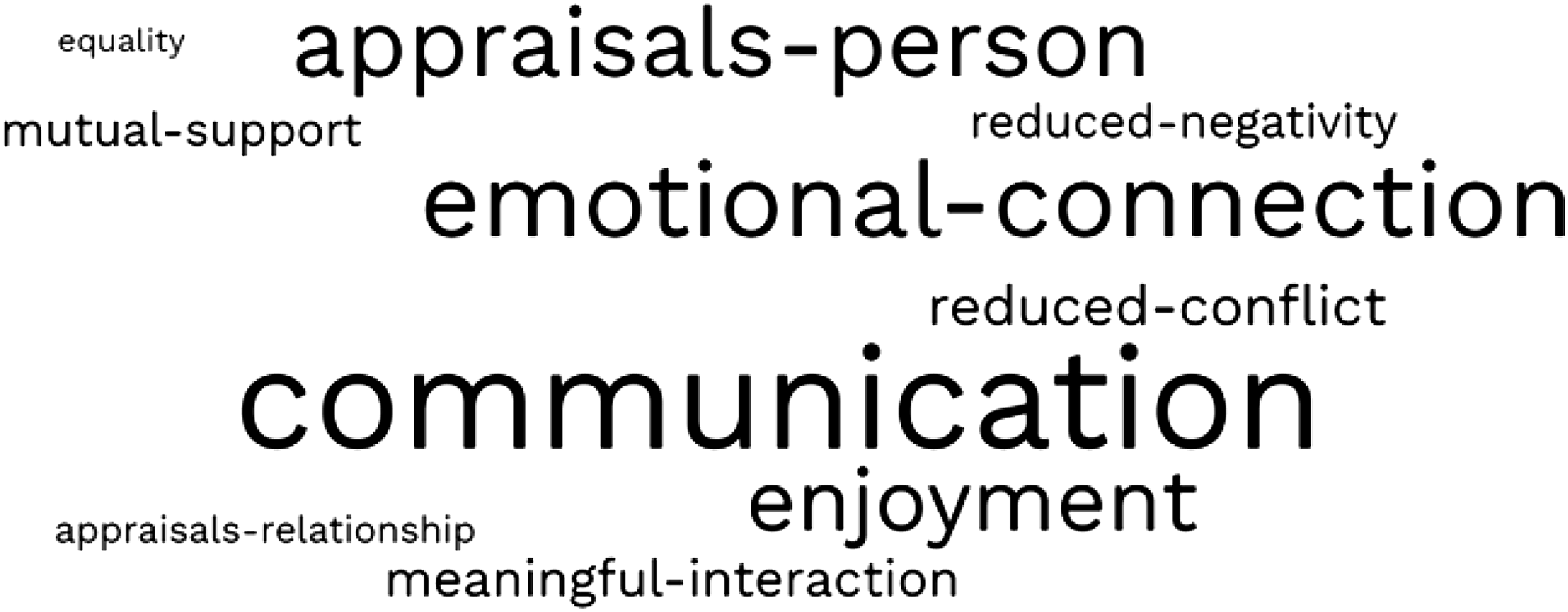
Some of the studies highlighted possible limitations and challenges to using the interventions (Table 3). Reminiscence and life review may be upsetting at times because it can serve as a reminder of what the care-receiver has lost (including not being able to recall significant events from their past) and how the relationship has changed. Some participants highlighted the burden of attending intervention sessions and being asked to do intervention-related activities at home. Frustration and conflict could also occur when the care-receiver was unwilling to participate or unresponsive to the efforts of the caregiver to implement the intervention.
Discussion
Improving the quality of research
It is difficult to draw any firm conclusions about the benefits of these interventions for the couple relationship because of the poor quality of the evidence. Although exploratory studies serve a useful purpose, the commissioning of services to provide interventions of this nature relies on a strong evidence base. The methods of data collection and analysis need to be more systematic. For example, studies that ask participants about their experience of the intervention need to follow a set interview schedule and the data need to be analysed using an appropriate qualitative methodology. More studies are needed that use control groups. Control groups are particularly important in this area of research because of the need to take account of decline in the variables of interest due to the advance of the dementia. For example, Quayhagen et al. (2000) reported a pre-post intervention decline in scores on a measure of marital satisfaction for their treatment groups, but an even greater decline for their control group (although this was not statistically analysed). A pre-post intervention design without a control group would have suggested that the intervention was ineffective. Self-report measures need to be supplemented by more objective evaluations to avoid the bias associated with self-report. A promising example of such evaluation is the quantitative analysis of recorded interactions between the couple described by some of the reviewed studies (Bourgeois, 1992; Ekstrom et al., 2017; Troche et al., 2019; Williams et al., 2018).
Future studies also need to explore more rigorously the wider impact of the intervention. Much of the focus of the reviewed studies was on the benefits occurring within the session. There was less investigation of whether it benefited the everyday life of the participants beyond the session, and whether the benefits were sustained over time. This is not to suggest that within-session benefits are not valuable. There is intrinsic worth, for example, in the opportunities for meaningful interaction and emotional connection within the session afforded by creative interventions such as music therapy (e.g. Dassa et al., 2020). Nevertheless, the case for commissioning these interventions within resource-limited services would be strengthened by evidence that there are long-term carry-over effects to everyday life. Control groups are again an important consideration when exploring long-term effectiveness to account for deterioration due to the dementia.
It is worth considering that when the research employed control groups (i.e. the three randomised controlled trials) and when it used standardised measures that addressed the wider impact of the intervention (i.e. the eight studies that used standardised questionnaires about the relationship), there was no quantitative evidence that the interventions were effective. It would be premature to conclude from this that the interventions were, indeed, ineffective or that any benefits were entirely within-session. The three randomised controlled trials all used standardised questionnaires to measure the outcome, but, in all three cases, it is questionable whether the questionnaires would have been sensitive to any relational benefits that occurred. Thus, the component of the intervention described by Nordheim et al. (2019) that was relevant to the relationship was communication training, but the questionnaire measured mutual support. Quayhagen and Quayhagen (2001) provided communication skills, but the questionnaire evaluated marital satisfaction. The different treatment groups in Quayhagen et al. (2000) received training in conversational skills, a discussion about family and social relationships, and cognitive behaviour therapy. The sensitivity of the marital satisfaction questionnaire they used to changes brought about by these interventions is questionable. Similar concerns can be raised about other studies that used questionnaires. For example, in the study by Baker et al. (2012) it is not clear questionnaires measuring the provision of mutual support and the benefits experienced by the caregiver from their caring role were an effective way of measuring the effects of music therapy. Future research needs to use quantitative outcome measures that will be sensitive to any changes brought about by the intervention. For example, quantitative coding of recorded couple interactions is likely to be sensitive to the benefits of communication training. Indeed, all five studies that used this method reported some benefits (Bourgeois, 1992; Ekstrom et al., 2017; Troche et al., 2019; Williams et al., 2018; Williams et al., 2021), although these were uncontrolled studies.
An appropriate overall conclusion about the effectiveness of the interventions reviewed in this paper is that they show promise, but they need to be more rigorously tested before they can be recommended for use in resource-limited services.
Embracing diversity
A positive aspect of the reviewed studies is the breadth of the interventions employed. They included different kinds of life review and reminiscence, a wide range of creative activities, verbal psychotherapies, and interventions directed at developing communication skills or using various aids to facilitate communication. As will be apparent from Table 3, there was some considerable overlap in terms of the potential relational benefits from these different kinds of intervention. For example, benefits in terms of Communication were reported for the narrative, creative and psychotherapy interventions as well as those that specifically focused on communication. This diversity in the interventions and the diversity in how relational outcomes can be achieved are valuable because they provide the opportunity to match an intervention to the needs, preferences, and abilities of the couple. For example, creative interventions enabled the involvement of couples living with severe dementia (Clark et al., 2021; Hamill et al., 2012; Unadkat et al., 2017). Future research should embrace this diversity and aim to ensure that, for each particular relational need, there is a range of interventions available.
As part of this future diversity, there needs to be more investigation of the use of verbal psychotherapies that have been implemented to improve relationships in the general population. The small number of studies that evaluated their use (four – see Table 3) is surprising given that such therapies have been reported to be effective in improving the relationships of those living with other kinds of neurodegenerative disease (e.g. Beasley & Ager, 2019; Ghedin et al., 2017). Unwarranted assumptions about lack of insight, understanding and reasoning on the part of the person with dementia may have contributed to this lack of interest. More recent studies indicate that many people in the earlier stages of dementia are aware of changes within their relationship (Alsawy et al., 2020; Clark et al., 2019; Harris, 2009; Wawrziczny et al., 2016).
Developing the theoretical rationale for interventions
Some of the reviewed studies did not provide a detailed account of the processes whereby the intervention was expected to benefit the relationship. To advance the development of interventions that support the relationship, and to understand for whom and in what circumstances they are effective, a more comprehensive understanding is needed of their mechanism of effect. In large part, this could be achieved by a closer connection with the research on the impact of dementia on the relationship that was summarised briefly in the Introduction. Taking into consideration what effects the dementia has had on the relationship could help to shape existing interventions and to suggest new developments or new interventions. Two examples are given to illustrate this possibility.
Some qualitative research on the experience of the person with dementia suggests that they can feel side-lined and ignored as the caregiver takes over, leading to some resentment of the caregiver (e.g. Clare & Shakespeare, 2004; Svanström & Dahlberg, 2004). Two of the reviewed papers mentioned greater balance and equity in the relationship as a product of the intervention. Epstein et al. (2007) evaluated the benefits of psychotherapy and noted that, as a result of the therapy, one of the caregivers felt less need to control the life of the care-receiver. In the study by Bielsten et al. (2020) that used a problem-solving approach, both members of some couples reported that their relationship felt more balanced. There is clearly scope for enhancing this effect of interventions. Greater attention could be paid to increasing the agency of the person with dementia, taking advantage of the fact that several of the interventions led caregivers to an appreciation of the fact that the care-receiver still retained some abilities they were unaware (e.g. Melunsky et al., 2015). This greater appreciation of retained abilities could also be used to address the tendency of some caregivers to over-control the lives of their partner.
A second example is based on work suggesting that dementia can undermine the caregiver’s experience of continuity in the relationship (Evans & Lee, 2014; Riley, 2019). The relationship no longer feels like a marriage, but as one characterised by the giving and receiving of care. This process is facilitated by perceptions that the person with dementia feels like a stranger. Both changes, in turn, contribute to changes in the feelings the caregiver has for their partner, as spousal love is replaced by feelings of care and protectiveness. Retaining a sense of continuity in the relationship is associated with a range of benefits for the couple (Riley, 2019). A rationale offered for the effectiveness of individual life review work with people with dementia is that it helps the individual to maintain a sense of identity and personal continuity by reminding them of their past (Kasl-Godley & Gatz, 2000). Some of the included studies that used life review highlighted that this intervention can have a similar impact on the caregiver. For example, caregivers in the study by Kindell et al. (2019) reflected that the intervention gave them an opportunity to reflect on the personhood and identity of the care-receiver and understand them for who they are. This suggests that it may be beneficial to explore how life review interventions might be used to highlight aspects of the person with dementia, and aspects of the relationship, that are relatively continuous with the past – thereby counteracting the experience of discontinuity. Other categories of intervention brought an appreciation of the residual strengths of the person with dementia, and this also offers an opportunity to counteract the sense of discontinuity. Indeed, participants in the music therapy intervention of Baker et al. (2012) reported that participation had strengthened the relationship by helping the caregiver appreciate that the care-receiver is still the same person.
Limitations of the scoping review
The review excluded studies in which the findings for spousal couples could not be clearly identified from those of other dyadic relationships. This resulted in the exclusion of some studies that are relevant to the topic addressed by this review. For example, this criterion resulted in the exclusion of two randomized controlled trials that evaluated the effectiveness of reminiscence groups for people with dementia and their family carers, (Charlesworth et al., 2016; Woods et al., 2016). In neither trial did the intervention have any significant impact on the relationship.
Another potential limitation of the review relates to the criterion of including studies in which improving the relationship was not the exclusive or primary focus of the intervention. Papers with a range of aims that included a relational aim may have been more likely to be missed in the initial screen that involved inspection of the title and abstract only.
Conclusions
Dementia can have a negative impact on marriages/partnerships. Maintaining a strong relationship helps couples deal more effectively with the challenges of living with dementia. Developing effective interventions to help couples maintain a strong relationship should therefore be a priority for research focused on living well with dementia. Existing research on this issue has some strengths, notably the diversity of the interventions that provides the opportunity to match the intervention to the needs, preferences, and abilities of the couple. Going forward, a closer connection needs to be made between intervention development and research that has been conducted about how dementia can affect the relationship. More attention also needs to be paid to the methodological rigour of future evaluations of the effectiveness of the interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.