
Abstract
In recognition of the often poor experience of people living with dementia in general hospitals and the lack of dementia curricular content for health and social care professionals, the Scottish Government commissioned a dementia workforce development programme (Dementia Champions) for qualified health and social care professionals in 2011. This constructivist grounded theory study aimed to construct a theory of the learning experienced by the dementia champions before, during and after the programme. The reported experience of change in the champions' professional and personal perspectives about people with dementia was the focus of this study. The findings contribute to a deeper understanding of the long-term negative impact of knowledge and skills gaps in dementia education and on people living with dementia and health and social care professionals. This negative impact has implications for individual professionals, service leaders and health and social care systems internationally. Data was co-produced through intensive interviewing, a focus group and email interviewing with nineteen Dementia Champions. Construction of the theory emerged from direct engagement with the data using the constructivist grounded theory approach. The findings illuminate how, before the programme, professionals were educated, socialised and defined to fail people with dementia. On the programme, multiple learning interventions in which interacting with the lived experience of people living with dementia, their families and colleagues became the stimulators of change. These learning interventions stimulated a disrupted self-definition and actions to resolve this disruption. Once the self-definition was restored, the participants faced the complexity of working with people living with dementia with passion, pride and new thinking. These findings further illuminate the importance of expert facilitation and the inclusion of people with dementia and their families as peer educators in health and social care dementia education. Further research on the negative outcomes of gaps in initial professional education is important.
Keywords
Introduction and background
Globally, around 55 million people have dementia; it is expected to rise to 139 million by 2050 (World Health Organisation, 2021). In the UK, about 40% of the people over 70 admitted to the hospital have dementia (Gwernan-Jones, Lourida, Abbott et al., 2020, The Royal College of Psychiatrists, 2019). The experience of people living with dementia and their families of general-hospital services has frequently fallen well below expectations (Alzheimer's Society, 2009; The Royal College of Psychiatrists, 2011; Boaden, 2016). A range of factors can influence their hospital experience, including co-morbidities of physical and mental ill-health, longer lengths of stay, avoidable complications such as dehydration and falls and the ability of people with dementia to cope with the admission and care provision (The Royal College of Psychiatrists, 2019; Prince et al., 2016). One key element of international dementia strategies is the education and upskilling of the dementia workforce, for example, in the UK, to prevent or lessen the impact of hospital admissions on people with dementia and their families. This paper presents a substantive grounded theory of health and social care professional participants' learning experience and impact on participants of a national workforce dementia education and change agent development programme.
Education and skills development for the current and future health and social care workforce to deliver high-quality care for people with dementia are international concerns (Collier et al., 2015; Mustafa et al., 2013). Current predictions indicate that an additional 40 million new health and social care jobs will be required globally by 2030, including 18 million new health workers (World Health Organisation, 2017). There is a lack of a solid evidence base for the impact of staff training in caring for people with dementia in the general hospital setting (Elvish et al., 2014, 2016; Surr & Gates, 2017). In the most recent round of the National Audit of Dementia Care in General Hospitals (England & Wales), only 53% of hospitals were able to provide figures on the proportion of staff dementia care trained at a level appropriate for their role (The Royal College of Psychiatrists, 2019).
For many years, the UK’s first professional education of health and social care professionals has not included working with people with dementia and their families (Collier et al., 2015; Pulsford et al., 2007). Pulsford et al. (2007) found pre-registration education about dementia care was often brief and dependent on the priorities of the curricula of individual Higher Education Institutions. And this content was influenced by the presence of lecturers interested in dementia. Despite increasing pressure over 10 years from academics and people with dementia, the situation has changed only marginally (Collier et al., 2015). The World Health Organisation has identified the essential need for dementia education and competencies across undergraduate and postgraduate health and social care workers (World Health Organisation, 2018). The implications of the current gap in dementia education have not been researched.
This paper presents the research approach and findings of a study into the learning experience of health and social care registered professionals who participated in Scotland’s National Dementia Champions Programme. Scotland’s National Dementia Champions are registered health and social care professionals prepared through the programme to become leaders and agents of change to improve the care and treatment of people with dementia and their families in the general hospital setting (Brown et al., 2018). The 6-month programme, developed in partnership with people with dementia and their families, has a blended learning approach, including five face-to-face study days and three assignments. The learning activities focus on a human rights-based approach to dementia care and is at the Enhanced Level of the Promoting Excellence Scottish Knowledge and Skills Framework (Scottish Government, 2021). The assignments facilitate reflection on knowledge, attitudes and practice, with the final assignment being an action plan for the Dementia Champions to lead change in their area of practice. A detailed description of the programme and ongoing evaluation is in Banks et al. (2014) and Jack-Waugh et al. (2018). These studies demonstrated that the Dementia Champions Programme significantly improves attitudes and knowledge of dementia and increases participants’ feelings of self-efficacy in delivering person-centred dementia care.
However, there is no research to explore the learner experiences and social learning process in this programme to understand how the reported positive outcomes are achieved. This study aimed to understand the learner experiences and the educational interventions that stimulated the reported positive shift in attitudes, knowledge and self-efficacy. Describing, sharing and replicating effective educational interventions can contribute to creating high-quality dementia education in global care settings where people with dementia are present.
Methods
Theoretical perspectives
The Constructivist grounded theory approach of Charmaz (2014) forms the methodology for this study. An underpinning philosophical subtle realist perspective and a theoretical symbolic interactionist lens were used to generate data, analyse, and present the findings and recommendations for future work. Symbolic interactionism and constructivist grounded theory share the research intentions to explore the worlds of the research participants and provide a deeper understanding of those social worlds (Blumer, 1969; Charmaz, 2008, 2014). By attending to the participants' experiences, a sense of ‘what is happening here was co-produced and represented in the data generation, analysis and findings.
The third space researcher positionality adopted for this study is an approach of being neither an outsider nor an insider to the social setting of the research (Corbin Dwyer & Buckle, 2009). As a qualitative researcher using a constructivist approach, the third space was occupied by being together with participants within a range of teaching and learning experiences as part of the Dementia Champions education team and meeting separately to co-construct their reality and seek meaning. The researcher’s positionality, the constructivist grounded theory methodology, and a symbolic interactionist lens required a pre-planned integrated approach to rigour. Researcher actions for rigour included adherence to methodological approaches, ethical procedures and engaging in and recording reflexivity, as discussed by (Blythe et al., 2013) and (Gentles et al., 2014).
Participants
Summary of study phases, sampling and data generation methods used and the number of participants.
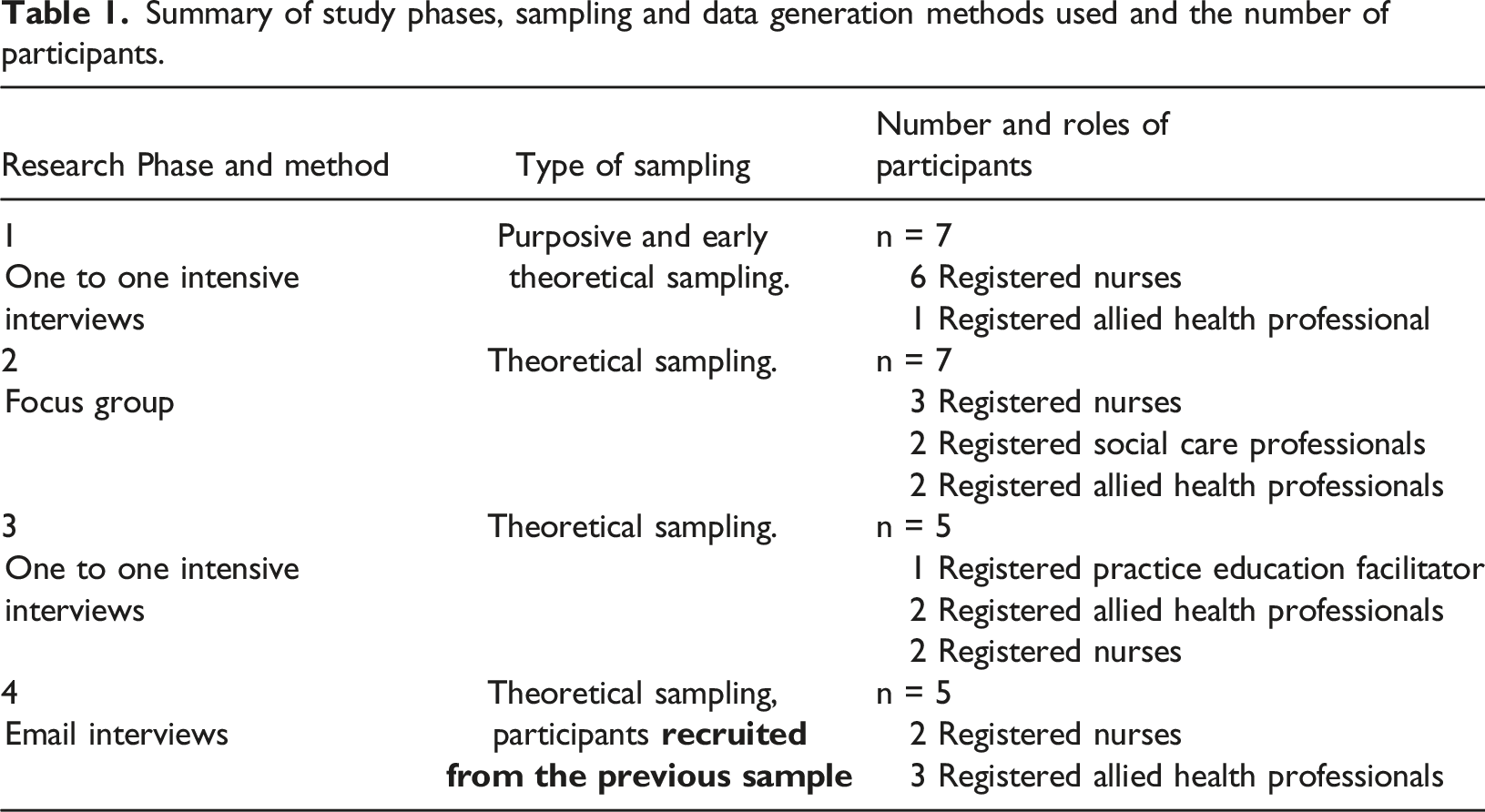
Gatekeepers for NHS Dementia Champions across Scotland sent out the participant information packs, and Dementia Champions were invited to participate by contacting the researcher directly if the statement below applied to them, Decide if you feel that you experienced a change in yourself OR your professional role, OR your perceptions of people with dementia due to the Dementia Champions Programme.
Procedure
Twelve Dementia Champions participated in intensive face to face interviews in two phases. Dementia Champion Programme evaluations had demonstrated the most significant positive change in attitude towards people with dementia was from nursing participants, therefore providing the richest data from which to develop initial categories; thus, sampling and recruitment in phase 1 were directed at nurses.
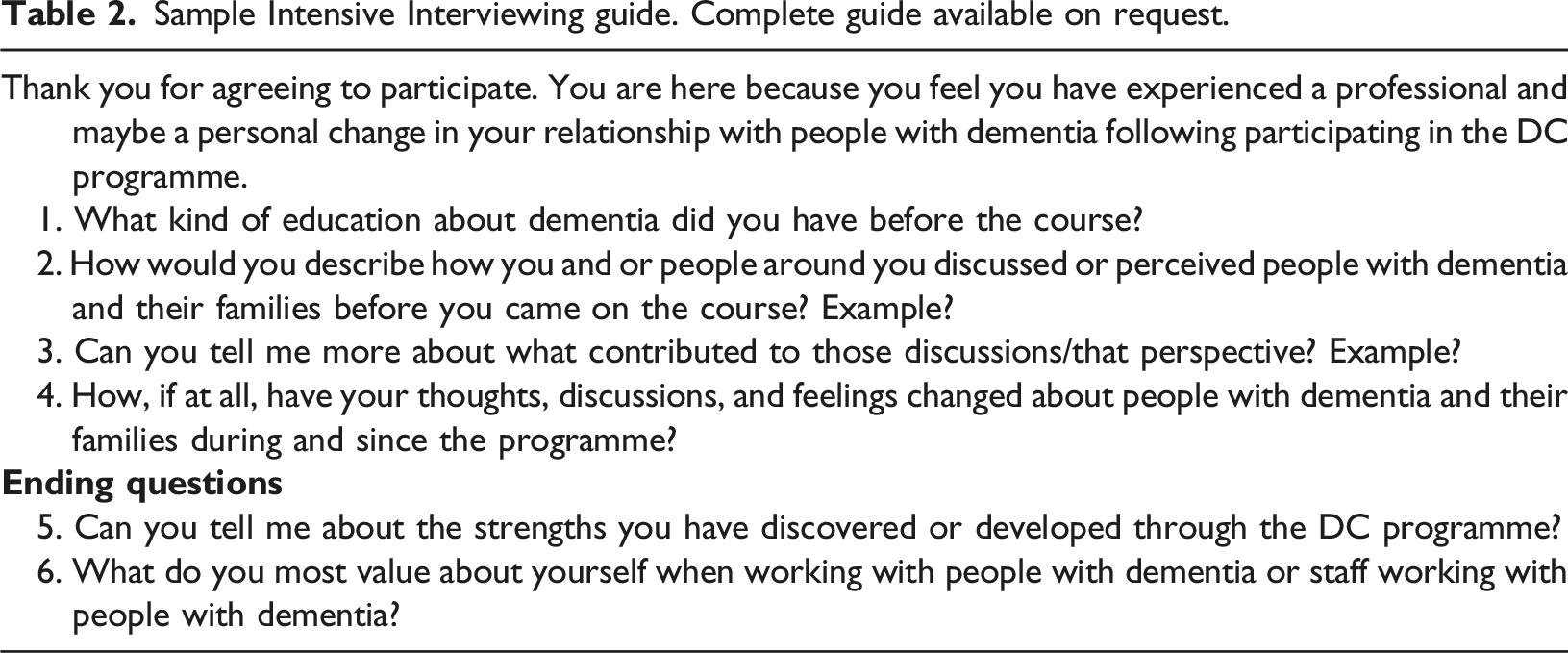
Intensive interviewing, where the interviewer listens to the participants’ interpretation of events and pays close attention to language, definitions and actions, was the face-to-face interview approach using a semi-structured method (Charmaz, 2014). The one and a half hour interviews were conducted in a private area of the interviewees choosing with the principal researcher. Each interview was recorded on a digital recorder, and after reflective field notes were recorded. A semi-structured interview guide was developed from the study literature review as recommended by Charmaz (2014); this formed the initial focus of the interviews.
Analysis of the interviews in phase 1 illuminated an emerging conceptual category of educational gaps. The experience of student placements with people with dementia was unpleasant and left participants with a pervasive negative perspective towards people with dementia; these findings became the primary analytical and theoretical sampling direction. Theoretical sampling is participant sampling undertaken to pursue early theoretical direction from ongoing analysis (Charmaz, 2014). Phase two data were generated with seven Dementia Champions in an hour-long focus group. The focus group participants were recruited at a national event for Dementia Champions. Before the event, they were recruited by selecting the workshop, and consent was gained before the focus group started. The researcher presented emergent theoretical categories from the intensive interviews for consideration. Two members of the education team conducted the group and data generation through field notes of the discussions and emergent shared perspectives. Participants discussed issues they had experienced in relation to proposed emerging codes and theoretical categories. They developed a shared perspective of these; an advantage of using focus groups as a data generation and collection method (Acocella, 2012; Carey, 2016).
Phase 3 was five further intensive interviews with two nurses, two allied health professionals and one nurse practice educator. This phase was concerned with following the analytical and theoretical direction indicated by the codes and theoretical categories resulting from the analysis of intensive interviews 1–4 and the focus group.
As the theory-building was nearing completion, email interviewing for data generation (phase 4) was conducted by revisiting five previous participants. These questions elicited views on the developing theory and if and how theoretical categories represented their experience. The use of email in qualitative research enabled remote access and expanded participation of the potential sample, allowing people time to consider responses to afford the researcher more open responses from the participants (James, 2016).
Ethical approval was sought in the four stages of the study through the university and NHS Research Scotland (ref GN15AM100) for interviews, the focus groups and email interviews. Ethical consent was gained by sending the participants information before the data gathering by email and then going back over the participant information sheets and the consent forms just before each interview and the focus group. Written and verbal consent was sought and given at each study stage.
Analysis
Sample Intensive Interviewing guide. Complete guide available on request.
The development of the interview framework and the inclusion of non-nursing professional groups of Dementia Champions became the critical method of enacting theoretical sampling; a process where data is sought to develop the emerging theory (Charmaz, 2014; Sbaraini et al., 2011). Memo-writing was the principal activity for moving theoretical sampling forward. The symbolic interactionist lens, memo-writing, constant comparison of memos with memos, and theoretical sensitivity described by Hernandez (2009) and Charmaz (2014) were the methodological approaches to generating and analysing data and developing the theoretical categories. Inclusion of the non-nursing health and social care professionals in the phase 2 focus group and phase 3 interviews allowed the theoretical categories to be further developed and analytical memos to be written questioning whether the early categories were dependent on the professional group membership.
The end of the constructivist grounded theory process is suggested by Charmaz (2014) to be when the data does not stimulate new theoretical insights, also known as saturation. Repeated engagement in the analytic processes after interview 12 illustrated no new insights in the data focusing upon the aim of the study.
Findings
The integrated theory of the experience of the Dementia Champions on the programme is the appraisal of the existing and the construction of a new self-definition and definition of others through learning, interaction, and relationships on the programme was a result of the educational interventions and their participation in them. The learning experience was grounded in the Dementia Champions' educational and professional histories. A timeline of experiences before, during and after the Dementia Champions programme provided the context of the Dementia Champions experiences. The evolution of positive and negative perspectives towards people with dementia resulting from interaction in workplaces, educators, people with dementia, families and fellow professionals provides an overarching and integrated understanding of the social and learning experiences of the Dementia Champions.
Three core theoretical concepts present the learners’ experiences before, during and after the programme. These being, Professionals were educated, socialised and defined to fail people with dementia is the learner experience before the programme. Being close up: taking the role of the other for learning represents the learner experience of educational interventions while on the programme and Holding a Mirror up to ourselves represents the evolution of the self through the redefinition of themselves and people with dementia experienced by the learners in response to the educational interventions. The detailed findings of this study are presented as an integrated, interpretive theoretical rendering, as recommended by Charmaz (2014). Figure 1 below provides a visual illustration of these processes. The learning experience of being a Dementia Champion.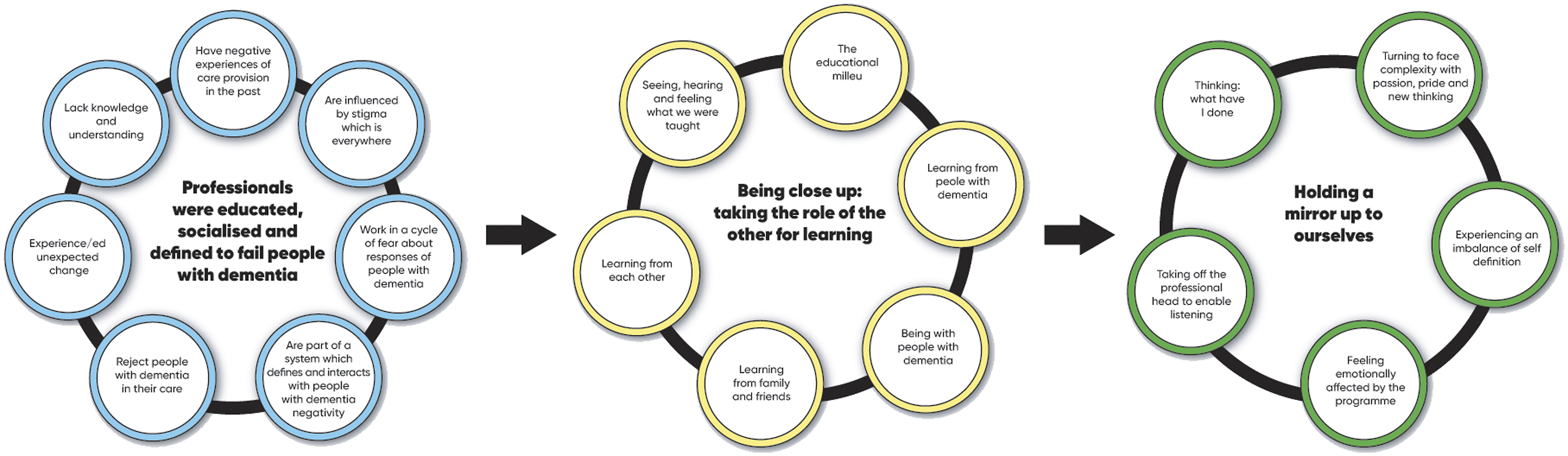
Professionals were educated, socialised and defined to fail people with dementia
In their education and professional past, Dementia Champions in this study were educated, socialised and defined by themselves and others to fail people with dementia Figure 2.
All the Dementia Champions reported they had little or no education about dementia during their pre-registration education. …….. I qualified in 1992, …… I don't think we did do stuff specifically on dementia. I mean, I can remember doing essays about rheumatoid arthritis, and we did mental health. We would have had something on elderly care, but I don't think there was much specifically on dementia. I don't think so, no. DC4 Nurse
Despite this lack of underpinning knowledge, many stated they had practice-placement experiences with people with dementia which were predominantly negative and shaped their early definition of people with dementia and working with people with dementia. They never saw themselves working with people with dementia and felt the care they had observed lacked humanity. ….. I had one placement caring for older adults, and I didn't enjoy the experience at all. Because of the way the care was delivered, …. … there were people restrained in chairs, constant toilet rounds and a lack of humanity. You know people, heavies, beddies, all the language that was used around caring for people, feeders. DC 12 Nurse
Stigma towards people with dementia was experienced and observed in people’s verbal and behavioural actions around the Dementia Champions. A cycle of fear featuring the combination of a lack of understanding of distressed behaviour and the neurobiological and environmental causes of distressed behaviour emerged from the data analysis. This cycle of fear resulted in staff descriptions of being fearful and withdrawing from or not approaching the person with dementia. How afraid they [staff] sometimes felt in engaging with people with dementia, and it was all because they didn't understand what was going on and why they were so anxious, and the big fear that they would upset them more, they would say something wrong. DC6 Allied Health Professional
The Dementia Champions experienced a lack of positive perspectives from which to view people with dementia, stemming from a lack of knowledge and understanding, stigma and the culture of the systems they worked in. Dementia Champions reported that they defined the care of people with dementia as not part of their job or professional role before undertaking the Dementia Champions programme. However, they recognised that the number of older people they care for has increased in a way they did not expect nor were prepared for. …….. it was a gradual process – we just suddenly found ourselves taking more and more patients that were in the older age group. So it wasn't a case of ‘You're going to now be accepting patients, so here is some training.' We didn't get that, that was not available, and so we had to be self-taught, self-aware, self-critical in a sense of our own environment and how we were managing our patients with particular needs and how we were perceived by other patients to manage patients who had specific needs, particularly with dementia. DC2 Nurse
How the Dementia Champions defined themselves and their work in relation to people with dementia evolved in the context that they worked in. This negative perspective contributed to the negative experience people with dementia and family carers had in care areas before the programme. Dementia Champions asserted that the absence of education led to retention and strengthening of actions that promoted cooperation of the hospital system and survival of the professionals. These actions, however, were not appropriate for people living with dementia.
Being close-up: taking the role of the other for learning
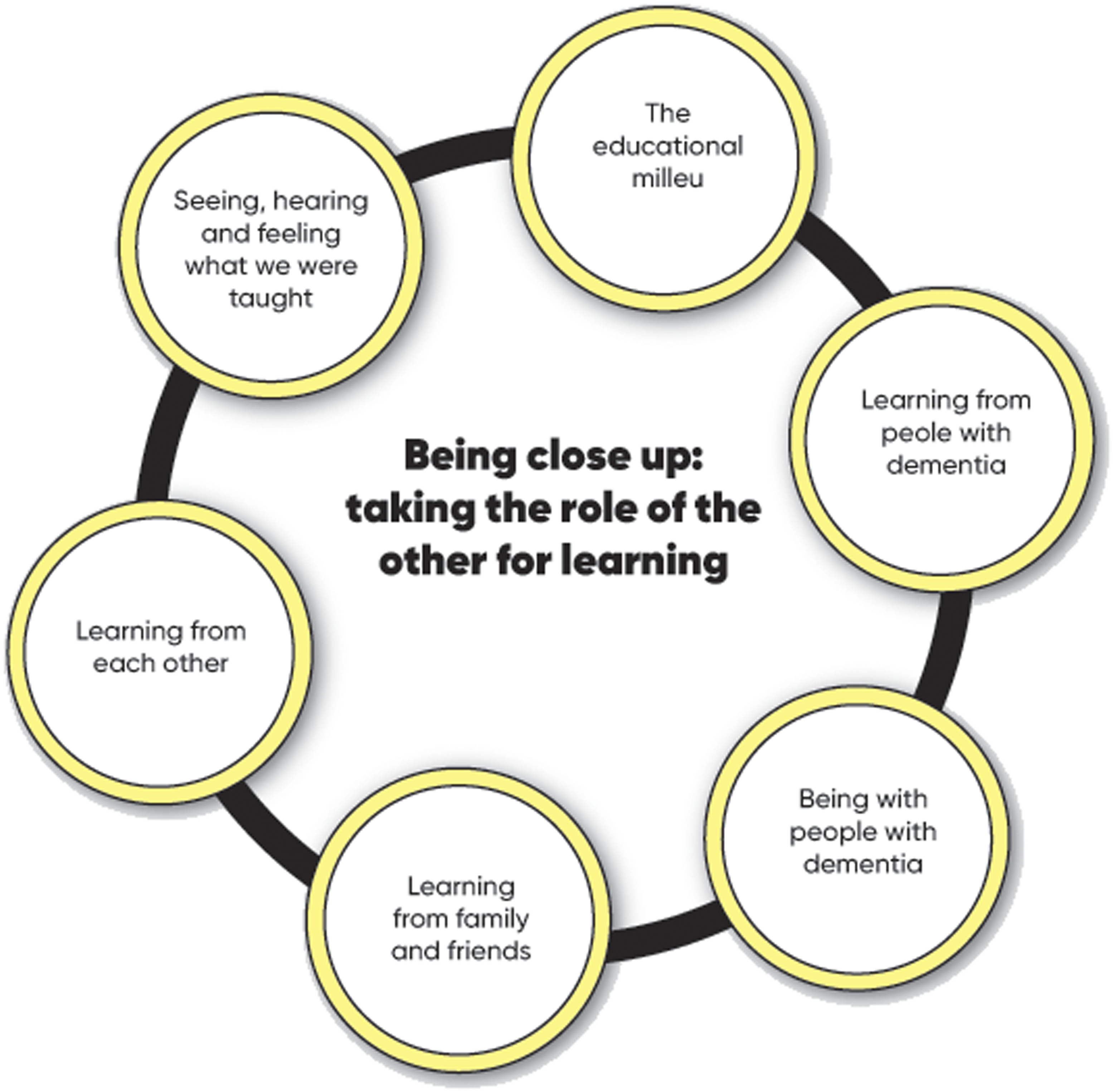
The learning experience on the Dementia Champions programme challenged participants’ prior education, socialisation and definition of themselves and people with dementia and family carers by bringing the experience of people affected by dementia up close in a range of learning activities. The core theoretical concept of this part of the substantive theory is ‘being close-up: taking the role of the other for learning’. The educational milieu created on the Dementia Champions programme, which supported actions for change, and specific standout learning moments emerged as stimuli for the evolution in self-definition and the definition of people with dementia (Figure 3).
The input of people with dementia and family carers in the Dementia Champions programme provided the most substantial and most sustained educational impact on self-definition and the definition of people with dementia by the Dementia Champions. Participation of people with dementia in the programme and seeing people with dementia living well in their communities provided interaction that changed how the Dementia Champions viewed themselves in relation to people with dementia. I particularly remember Tom ……..he is very moving because there's always this assumption that once you have dementia, you don't have a voice anymore. Having time to see and, I think, it's also we do so much sometimes in practice by proxy: you get the carer's views on things, rather than the person's own words. I think it's taking the time sometimes to get that first-hand perspective, isn't it, which is harder; it takes a bit more effort. This is a real authentic person with all their warts and all, all the unglamour as well. DC11 Allied Health Professional
Interactions with other Dementia Champions resulted in learning about other services and specialisms, with Dementia Champions gaining a deeper understanding of how services intersected (or not) for people with dementia. A socially defined group of Dementia Champions was created by being close-up to their peer group; with accepted understandings of their self-definitions and definitions of people with dementia, participants became and defined themselves as Dementia Champions. I thought they were a fabulous group, really supportive. I knew nothing about lots of things that they knew heaps about and already had good ideas about how to manage people and support people with dementia, and it was all completely new to me. I just learned so much from every single person on it, and I engaged with everybody, and it just gives you a real buzz feeling. DC6 Allied Health Professional
A suite of simulated educational activities called Care Empathia facilitated reflexivity and meaning-making. The process was unique to each champion at the deepest intrapersonal level resulting in Dementia Champions appraising their practice and the practice of others.
I can remember most things we did (on the programme). I remember feeding each other.
INT: How did you find that?
Oh, it was terrible.
INT: Right, okay, in what way was that terrible?
Oh, I don't know; it was just that lack of control, isn't it, when you're getting fed. That's why I'm very mindful. DC 5 Nurse
Each element of the programme described in Figure 3 contributed to the reappraisal of the champion’s experience, definition and perception of working with people with dementia in the context of Being educated, socialised and defined to fail people with dementia. This reappraisal, outlined next, was challenging. Professionals were educated, socialised and defined to fail people with dementia. Being close up: taking the role of the other for learning.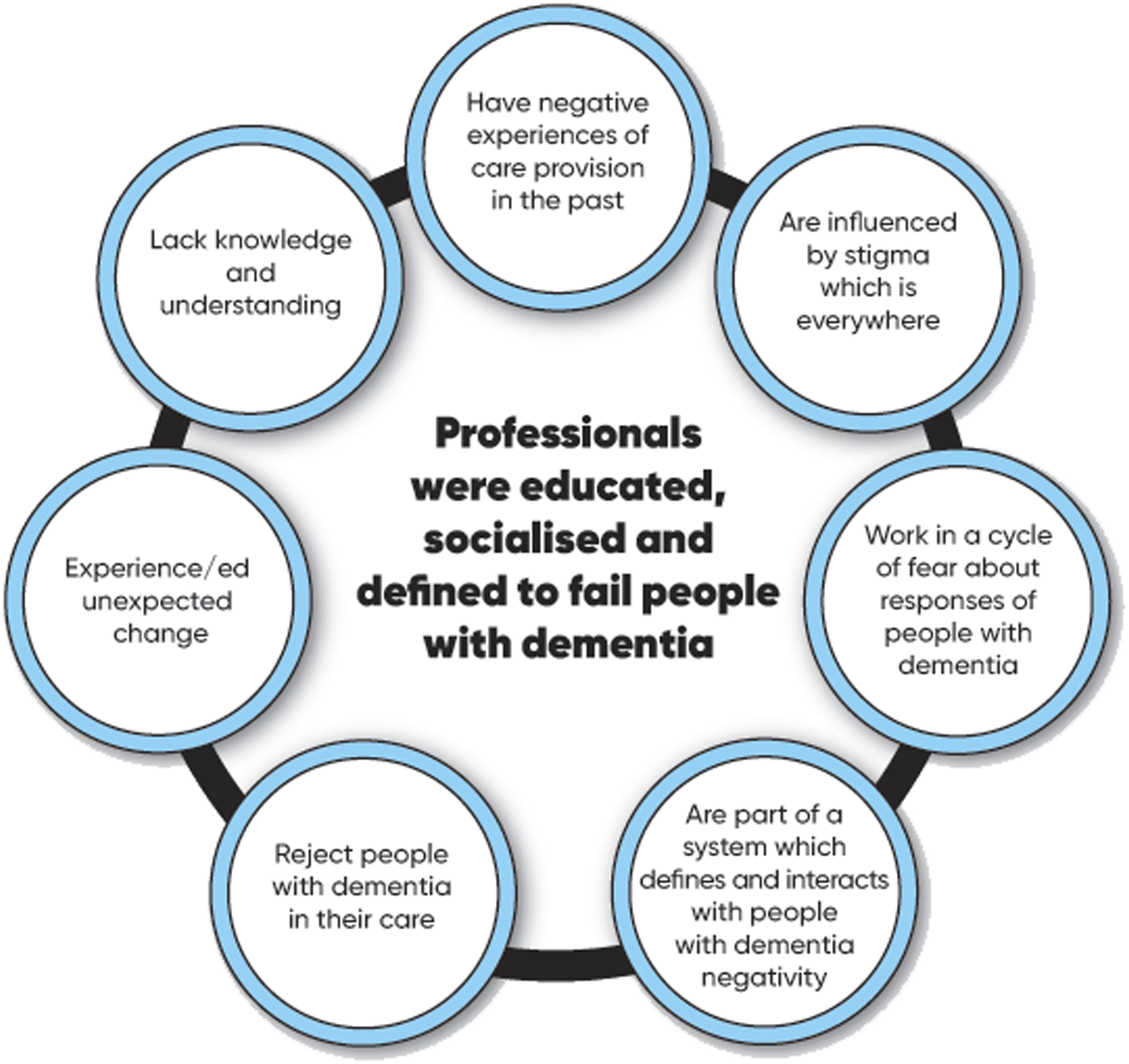
Holding a mirror up to ourselves
The benefit of hindsight supported the Dementia Champions to move from a position of unconscious incompetence to a place of conscious incompetence and an understanding of the gap between best practice and the care they delivered. The evolution of the self was consolidated through these directly experienced moments of being close-up: taking the role of the other for learning (Figure 4).
This evolution was emotionally painful as a metaphorical mirror was held up to their self-definition and self-concept of being a ‘good’ professional. Holding a Mirror up to ourselves. The course made you reflect. ‘What have I done?' made it difficult, emotionally draining. The course made me reflect on my practice, acknowledge my emotions and particularly a strong sense of guilt about how I had treated people with dementia in the past. FG 1 Nurse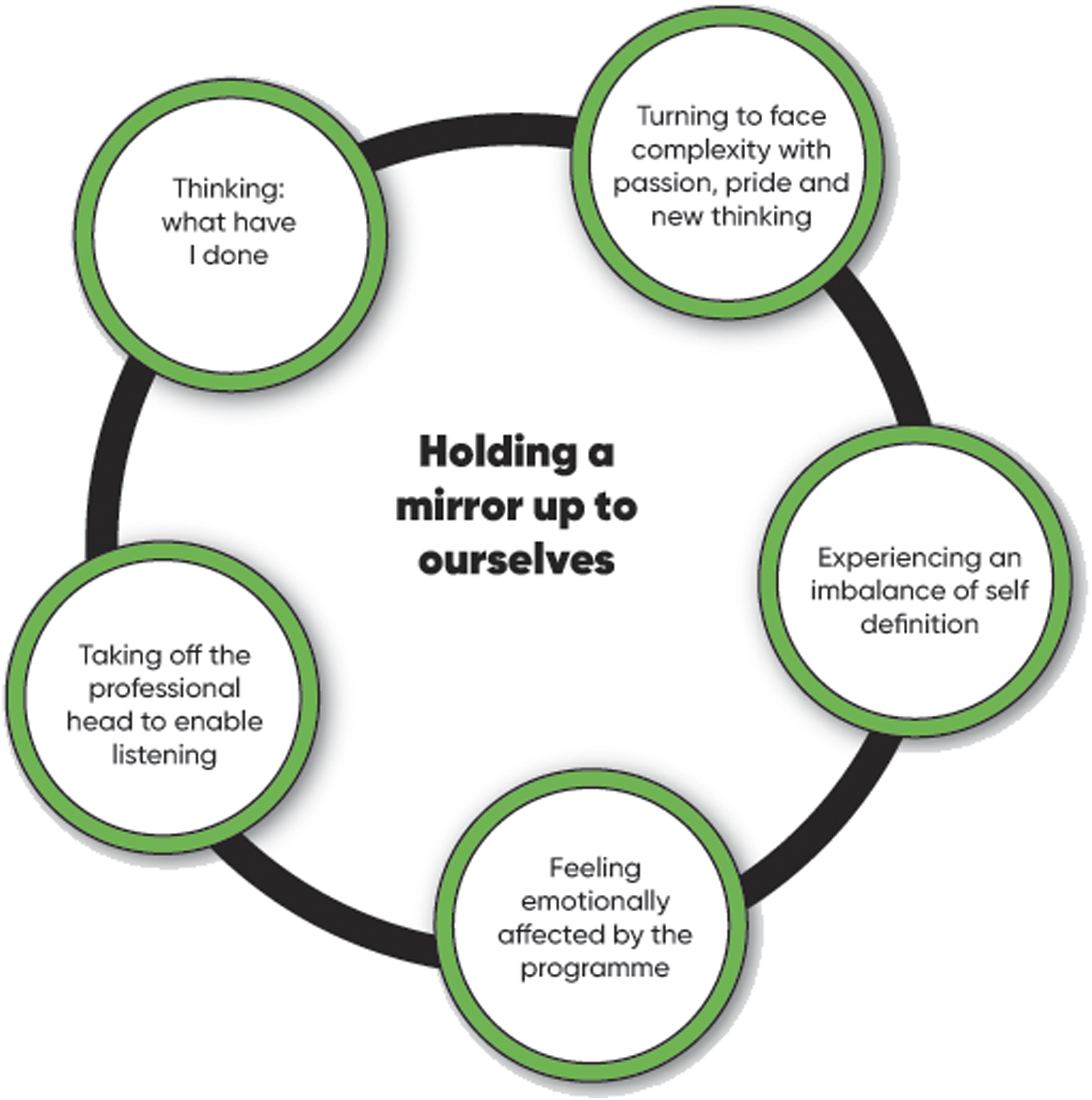
Efforts to resolve this disruption included remaining on the programme and removing aspects of their professional socialisation to engage with learning on the programme deeply. This emotion highlighted that they had to ‘remove their professional head’ to listen to the experience of others and to learn. … sometimes we make quite a lot of assumptions, or we sometimes have that professional hat on, and we assume that we have to act in a certain way or be all-knowing, and I think sometimes it's like, just take that hat off for a minute. I'll say to teams, 'If this was you or your mum, how do you think it would feel to you?' DC10 Nurse
A new self-definition evolved, with the Dementia Champions turning to face the complexity of working with people with dementia with passion, pride and new thinking. So, it definitely increased my confidence as an AHP and as an individual and as a healthcare professional to be able to participate in discussions about people with dementia confidently and not think when I'm on a ward with nursing staff that they know it all and I can't help them. But actually, you know, from a hands-on point of view with a patient, I would have stepped right back. Whereas now I would be so much more comfortable and do it all the time and I think I wouldn't have gone to help people in the past. I would have helped people immediately and then gone and got a nurse or somebody else to come and help, but now it would never cross my mind to walk by somebody. It's my duty and responsibility, and I'm happy with that now. DC6 Allied Health Professional
Three core theoretical concepts of the substantive theory told of the Dementia Champions who were educated, socialised and defined to fail people with dementia in their first professional preparation and subsequent socialisation into their workplace. As new entrants in their profession, they vowed never to work in those setting again. On the programme, multiple educational interventions in which interacting with the lived experience of people living with dementia, their families and colleagues became the stimulators of change. The change the champions experienced was how they defined their professional identity and self-concept concerning people with dementia and their broad definition of people with dementia. The change process was painful; while on the programme, the champions understood how they defined themselves as proud, competent professionals was flawed. They reflected and experienced pain when they thought about what they had done in the past. They found they had to drop their professional identity to engage in the programme, so profoundly had they been socialised into a perspective that rejected people living with dementia. Once, through continued learning on the programme, self-definition was restored. The participants faced the complexity of working with people living with dementia with passion, pride and new thinking.
Discussion
This discussion demonstrates how the Dementia Champions’ experiences and the findings of this study are reflected in, extend and highlight gaps in contemporary literature on dementia education for health and social care professionals. Like the Dementia Champions, hospital staff expressed a lack of knowledge and skills, particularly in managing stress and distress, and felt anxious, helpless or uncertain (Digby et al., 2017; Hynninen et al., 2015; Moonga & Likupe, 2016; Pinkert et al., 2017; Turner et al., 2017). Efforts to overcome the negative experiences included using existing routines for security and control or working flexibly to fulfil the needs of the person with dementia (Pinkert et al., 2017). Some worked flexibly but felt like lone champions (Brossard Saxell et al. 2021). Others retreated into routines focused on fulfilling the system’s needs and keeping themselves safe as a professional (Digby et al., 2017; Pinkert et al., 2017; Teodorczuk et al., 2015). Some nurses had made active choices not to work with people with dementia by choosing care areas that were highly medically focused (Pinkert et al., 2017). As experienced by Dementia champions, the literature reflects systematic stigma present in a range of healthcare settings, including negative perceptions of people with dementia which prevented nurses from seeing a person’s holistic needs (Digby et al., 2017; Houghton et al., 2016; Turner et al., 2017). Stigma was not limited to people with dementia, impacting health professionals creating poor pay, poor education, low job satisfaction and peer invalidation, also raised by Digby et al., (2017). As in this study’s findings, people with dementia were defined as low priority and treated according to the general-hospital focus, bureaucracy and hierarchy concerned with acute medical care reinforcing findings from Digby et al., (2017), Gkioka et al. (2020) and Gwernan-Jones, Lourida & Abbott et al. (2020). Additionally, so embedded is the low status of dementia care and the importance of physical healthcare routines and safety in general hospitals that for person-centred care for people with dementia to become routine, a change in hospital culture is needed Gwernan-Jones, Lourida & Abbott et al. (2020).
All studies on dementia in general hospitals assert the need for further education to help staff work with people with dementia. However, staff in these studies who had received education felt it was too theoretical and lacked transferability to direct care (Teodorczuk et al., 2015; Turner et al., 2017). Where possible, the education should be mandatory for all staff in the areas where they will be caring for people with dementia (Houghton et al., 2016; Moonga & Likupe, 2016) and should be accessible in terms of time and facilities to access this education (Gkioka et al., 2020; Houghton et al., 2016; Pinkert et al., 2017; Surr & Gates, 2017.). Additionally, staff may require awareness-raising to value and pursue education about dementia (Pinkert et al., 2017).
In the ‘What Works' studies, Surr and Gates (2017), Surr et al. (2017) and Surr et al. (2020), the characteristics of effective dementia education were described as, directly relevant to the practitioners, classroom-based, delivered by expert educators and with the participation of people with dementia and their families. The Dementia Champions programme has all these characteristics in its design and delivery. It represents an integrated, evidence-based approach to dementia education, with this study illuminating the positive lasting impact on participants.
In the educational milieu of the programme, Dementia Champions valued the ability of the facilitators to bring the experience of people living with dementia alive in the classroom setting, being a member of a group and the learning resulting from the group membership. Surr and Gates (2017) highlighted positive attitude change when engagement with facilitators was prolonged and described short programmes as ineffective for attitude change. The necessary characteristics to support attitude change include being an expert in education and dementia care and responding skilfully to learner concerns and attitudes that are viewed as essential (Surr et al., 2017).
On the programme, Dementia Champions had four opportunities to learn by listening to and being with the people with dementia and their families who receive care, including a community placement where they worked alongside people with dementia who lived with their diagnosis in the community and 24-hour care. Family carers of people with dementia were co-facilitators of one afternoon dedicated to their experience. These learning interventions were reported to have the highest impact on the Dementia Champions’ knowledge, the definition of people with dementia, and their definition as professionals. These findings have implications for all education of people within the current and future dementia workforce.
Education should be informed by the experiences of people with dementia and be directly applicable to practice, focusing on working with stressed and distressed people with dementia (Houghton et al., 2016; Surr et al., 2020; Turner et al., 2017). Dementia Champions reported being with the people with dementia, their peers, and the other learning partners within the learning environment supported their change. No other programme in this field involves people with dementia directly in the room as part of the education of general-hospital staff. On the Dementia Champions Programme, people with dementia and their families are the most influential in this apprenticeship relationship, rather than artefacts through which to construct new meanings socially. No previous studies into general-hospital staff education implemented a learning strategy that enabled learners to be with people with dementia where the people with dementia were hosting the learners. General-hospital staff see people with dementia when they are ill or in crisis, potentially providing a one-dimensional perspective of the experience of dementia. Unsurprising then, general-hospital staff continue to hold the views and definitions illuminated in this study.
Seeing, hearing, and feeling what we were taught refers to learning experiences on the programme that used Care Empathia, a low-fidelity simulation of sensory and cognitive changes for people with dementia and supported the practice of fundamental skills. The Dementia Champions reported developing an understanding of the ‘bigger picture of the experience of dementia and reflecting upon why people with dementia became stressed and distressed. The Dementia Champions in this study described reflecting upon their previous care experiences and feeling guilt and shame about how they may have made people in their care feel. Then they reflected upon what it may be like for them to receive care in the future. Enabling learners to be close-up requires skilful facilitation and the development of skills for this group of staff. Such facilitation should occur in a trusting educational relationship and have a structured debriefing process (Surr et al., 2017) that resonates and links with the importance of the educational milieu.
The programme’s reported emotional and psychological processes and impact require particular attention, demonstrating the importance of the interaction between the educational milieu and learning from each other. Dementia Champions found their previously held self-concept did not promote learning, listening and acting as a Dementia Champion. For Dementia Champions, the social environment in the educational milieu of the programme failed to validate their shared understanding of people with dementia and their self-concept of being an excellent professional. A disruption of self was experienced as the Dementia Champions understood that their previously held definition of dementia was not an accepted norm within the social environment of the programme. This discrepancy between self-concept and relevant new information results in self-concept change (Gore & Cross, 2014). It became more rewarding for them to evolve from their previous definitions and develop a self-concept in relation to people with dementia which aligns with their self-concept of being an excellent professional and the social environment of the programme. Self-concept change with regard to people with dementia developed through shared experiences and the formation of relationships on the programme are actions observed in work by Besta et al. (2016). The Dementia Champions developed a social identity of ‘being a Dementia Champion’. The programme became an in-group to be part of, especially after the first two cohorts. Being part of an in-group includes assimilating self-concepts to fit into the characteristics of the identified social group (Gore & Cross, 2014).
However, this self-concept evolution was painful, provoking guilt and shame at how they had treated people with dementia in the past and how they continued to see people with dementia treated in their setting. The Dementia Champions reported an emotionally and psychologically difficult self-concept change. The programme directly contradicted their previous education and socialisation. No available literature considers how general-hospital staff receiving education about working with people with dementia may experience a self-concept change or how to support this process. This study, however, demonstrates the need for psychological and emotional safety and support integrated into programmes where self-concept change is a possibility.
The findings of this study have produced both a timeline of health and social care professionals’ experiences of intensive dementia education and an evidence-based approach to future dementia education based on their experiences and the education gap illuminated by this study. The next phase of our work is to examine and report on lessons from the Covid-19 pandemic, where each pedagogical component of the programme was delivered digitally.
Limitations
A limitation of this study is the inclusion of only Dementia Champions who had a positive experience of change on the programme. Searching for Dementia Champions who had a negative or no experience of change may have further developed the theory or been useful as negative cases to ‘identify new variables or different explanations in the developing theory’ (Charmaz, 2014, p. 199).
Conclusion
The Dementia Champions' commitment to the study enabled an in-depth exploration of their history, educational experiences, and the emotional and psychological impact of the programme, bringing about personal and professional change. The substantive theory illuminates how gaps in education intersect with hospital systems to create an environment where staff and people with dementia experience significant difficulties. Close-up experience of people living with dementia and their families is the central educational intervention that stimulated their change in perspective and subsequent relationship to working with people with dementia. This theory could enable current and future actions for education programmes and educational research internationally that support the development of health and social care staff to provide care to people with dementia, underpinned by an appreciation of the lives of all people affected by dementia.
The study findings contribute to a deeper understanding of the long-term impact of stigma on learning about and working with people with dementia and their families. The findings describe the complex evidence-based educational interventions required to support all health and social care staff to learn and work in partnership with people with dementia and their families.
Footnotes
Acknowledgements
Deepest gratitude for support for the study and the publication goes to the Alzheimer Scotland Centre for Policy and Practice team, all Dementia Champions across Scotland, the National Dementia Carers action group, and the Scottish Dementia Working Group, in particular, Henry and Anne Rankin.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was sought in the four stages of the study through the university and NHS Research Scotland (ref GN15AM100) for interviews, the focus groups and email interviews. Ethical consent was gained by sending the participants information before the data gathering by email and then going back over the participant information sheets and the consent forms just before each interview and the focus group. Written and verbal consent was sought and given at each study stage.
Dr