
Abstract
Objectives
The experience of providing/receiving intimate continence care between family members can be difficult and emotive. Often, for people living with dementia this seems an area of care overlooked by professionals. This study investigated the experiences of intimate continence care for people living with dementia and their family member (the family dyad), and whether they viewed this as impacting on their relationship.
Method
Face-to-face interviews were conducted at 6 monthly intervals over a 12-month period with 13 carers (all family members) and one person living with dementia (13 family dyads) in England. Interviews were recorded and transcribed. Analysis of the data was achieved using a descriptive phenomenological method.
Findings
Carers’ attitudes towards providing intimate continence care revealed a task-focused approach for some but feelings of disgust and distress for others. Four participants (including the participant living with dementia) reported that intimate continence care had strengthened their dyad relationship. However, some carers perceived the care and support received from health and social care practitioners to be insufficient, which placed extra stress on them and adversely affected their family dyad relationship.
Conclusion
Implications of the study suggest that integrated and effective continence care and support for people living with dementia and their carers could (1) maintain the quality of the family dyad relationship, (2) help keep the person living at home, delaying an unwanted move to a care home and (3) consequently improve overall quality of life for individuals in the family dyad. Assuring integrated and effective continence care should be a priority for service funders and quality assurance regulators.
Introduction
Many people living with dementia experience problems with using the toilet and managing continence. Incontinence, that is the leakage of urine or faeces (excreta) (Abrams, Cardozo, Khoury, & Wein, 2013), may occur due to symptoms of dementia (e.g. not recognising the physiological signs of needing to use the toilet) or an additional medical condition (e.g. Crohn’s disease). However, for people living with dementia, ‘incontinence’ may also be due to difficulties with using the toilet effectively (Drennan, Manthorpe & Iliffe, 2017), such as not being able to find the toilet in time (Hutchinson, Leger-Krall, & Skodol Wilson, 1996), or resisting support or assistance (Kyle, 2012; Drennan, Cole & Iliffe, 2017).
In England, a study of general practitioner (family doctor) records found that older people living with dementia at home had double the rate of urinary incontinence and triple the rate of faecal incontinence compared to those without dementia (Grant et al., 2013). The presence of incontinence is thought to influence a move to a care home (Luppa et al., 2008; Young, Kalamaras, Kelly, & Hornick, 2015) but what aspect of the incontinence precipitates a move to a care home is not known. One possibility may be that carers find it difficult to support their relatives living with dementia who have problems using the toilet or containing urinary or faecal incontinence.
Gaining advice and support from health and social care agencies to manage continence for people living at home with dementia is problematic. In an article that examined United Kingdom (UK) policy documents in these two areas (continence and dementia care), Drennan and Cole concluded, ‘those (policies) concerned with people with dementia at home do not mention incontinence, and those concerning incontinence do not mention people with dementia’ (Drennan & Cole, 2009, page 20). In 2014, Alzheimer’s Europe produced a report and expert driven guidelines on the management of continence problems for people living at home with dementia. It recommended that people living with dementia, carers, and health and social care professionals work together to conduct a continence assessment and implement a management plan, such as changes to the environment (e.g. signs, handrails), products to contain the incontinence (e.g. absorbent pads, commodes) and support for the carer (e.g. respite) (Alzheimer’s Europe, 2014).
The most intimate of all caring tasks has been argued to be the management of body fluids and excreta (Cambridge & Carnaby, 2000). As such, this study uses the definition of ‘intimate continence care’ to refer to the intimate management of excreta, an aspect of bodywork. Twigg argued that much of care work was ‘body work’, an aspect that is often overlooked in research, and policy related to carers (Twigg 2000), possibly due to this type of care work breaching social norms and being hidden from society (Twigg, 2006). Consequently, incontinence and toilet-related difficulties can negatively affect an individual’s sense of self and identity, creating feelings of shame and fear of being stigmatised (Elstad et al., 2010; Olsson & Bertero, 2015). Carers supporting a family member living with dementia at home were found to try to conceal their family member’s incontinence in an attempt to preserve their dignity (Drennan et al., 2011). Similarly, people living with dementia tried to keep their incontinence hidden from their family member to shield them from their problems (Cole & Drennan, 2019).
Receiving or providing care at home whilst maintaining familial bonds can be challenging for families (Clark et al., 2019). Family caring emerges from the context of pre-existing relationships (Montgomery & Kosloski, 2000), and as such, the relationship between those receiving care and those providing care is a social interaction that may lead to changes in power dynamics (Tronto, 1993) and levels of satisfaction with the relationship (e.g. Sanders & Power, 2009). Relational approaches to care, such as ‘an ethic of care’ (Tronto, 1993), are important to dementia and continence care as they include the perspectives of all members of the care situation, that is, family carers, care workers (health and social care agencies) and the cared-for person. In this approach, there are four elements of care: ‘caring about’ (recognising need to be met), ‘taking care of’ (accepting responsibility to address need), ‘care-giving’ (the act of caring, care work) and ‘care-receiving’ (perspective of the cared-for person) (Tronto, 1993). Including all individuals in this way acknowledges the relational nature of caring, which if supported appropriately, can result in strong relationships and good quality of life (Mitchell et al., 2020). In this way, relational approaches enable care to be seen as a normative concept central to everyday human life (Barnes, 2012).
Some research has explored experiences of managing continence at home for people living with dementia (Cole & Drennan, 2019) and their family carers (Drennan et al., 2011). However, the impact of incontinence on family relationships remains unexplored and poorly understood (Alzheimer’s Europe, 2014). This present study aimed to investigate the experiences of people living with dementia and their main family carer (family dyad) when managing intimate continence care at home and explore whether this type of care affected their dyad relationship.
Methods
A qualitative approach was adopted for this study, interviewing participants at six-monthly intervals for a year. A phenomenological approach (Giorgi, 1997) was chosen as it allowed for the lived experiences of participants to be described and investigated. This study aimed to recruit a purposive sample of older people (over the age of 65 years) living with dementia with intimate continence care needs and their co-resident main family carer (the family dyad). To obtain diversity in the sample, a range of experiences and participant characteristics was sought. Characteristics of interest were: age, gender, ethnicity, the stage of dementia (using the World Health Organisation (WHO), 2009 criterion), the types of incontinence and difficulties with using the toilet, and the kin relationship type of the family dyad (e.g. spouse, adult–child and sibling). The inclusion of co-resident family dyads was considered an important criterion for the study in the context of family dyad relationships, due to factors such as shared living space and extended periods of exposure to each other.
Inclusion and exclusion criteria.
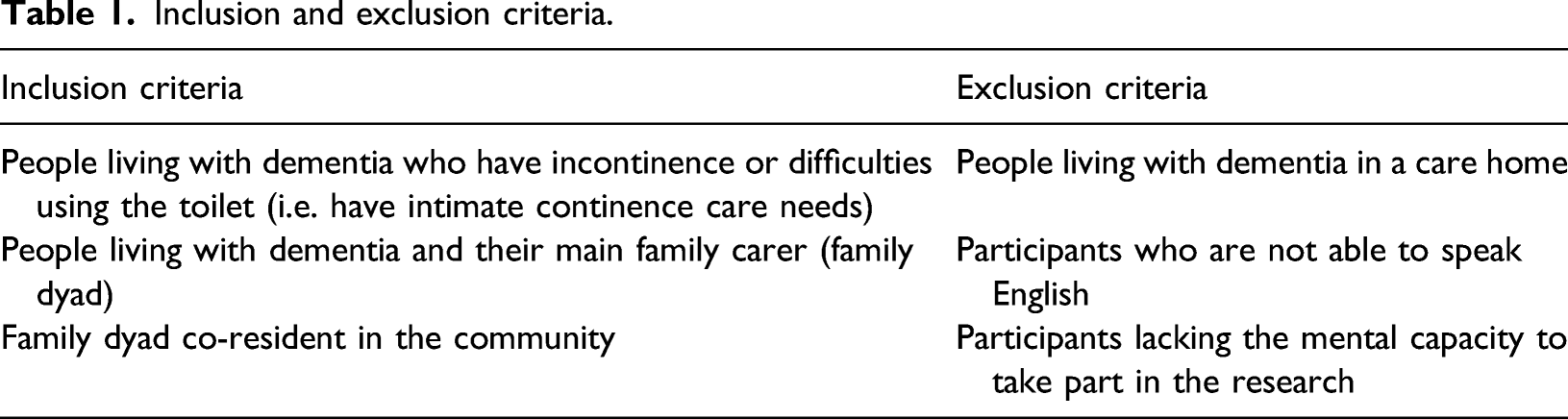
Potential participants were identified via health and social care organisations, and community organisations supporting people living with dementia at home and their family/friend carers, across the Southeast of England. Potential participants received written information about the study either through the post or in person from the researcher (LC). The researcher arranged a time to meet with the family dyad at their home, explaining the research and providing them with study information sheets to keep and consider for at least a 24-h period. Care was taken to involve and support the participation of people living with dementia in the research by providing specially formatted (dementia-friendly) study information sheets and reading the information aloud, if required. The researcher (LC) met with the participants at least once before gaining written consent to establish a rapport and familiarity. These steps were taken to help minimize distress or embarrassment when discussing potentially sensitive issues (Lee, 1993). During this visit, the researcher was able to ascertain whether potential participants had the capacity to take part in the study. Consequently, participants were required to have the ability to understand, retain and ask questions about the study, which enabled them to make an informed decision about whether they wanted to participate (Department of Health (DH) 2005). Written consent was obtained from all participants at the start of the study. However, ensuring consent was an ongoing process and attention was paid to any non-verbal cues (e.g. body language) indicating that an individual might be unhappy or wanting to withdrawal from the study. This was of particular importance for people living with dementia who may experience impaired verbal skills (Samsi & Manthorpe, 2020). If a person with dementia lacked capacity to consent to take part in the study, assent was gained on their behalf by the family carer (DH, 2005). In this situation only the family carer was interviewed and demographics of the person living with dementia were recorded. Ethical approval was gained from North West London Research Committee (REC) 1 (08/H0722/60).
Participants were interviewed on three occasions if possible; firstly at Time One (T1), with Time Two (T2) interviews at 6 months and Time Three (T3) at 12 months. Three timepoints were deemed necessary due to the sensitive nature of the topic under discussion, to establish a rapport with participants and gain a rich dataset. Demographic data were also obtained at T1. Semi-structured face-to-face interviews were conducted with the aid of a topic guide. Conversational interviews were used with people living with dementia as suggested by Murphy (2007), and care was taken not to embarrass or cause the participant distress if they felt unable to answer the research questions.
At T1 the topic guide sought information about the nature of the family dyad relationship prior to the onset of dementia (past relationship), as well as the current relationship. In addition, the researcher enquired about particular aspects of intimate continence care and how the participant might perceive this to be affecting their family dyad relationship. Follow-up topic guides for T2 and T3, concentrated on the current family dyad relationship and any reflections that the participant might have (e.g. of care services received, their health, continence management) over the past 6 months. Each interview was approached with care to ensure that participants felt safe to discuss the subjects relevant to the study’s objectives.
All participants were interviewed in their family home. The researcher indicated that for the purposes of confidentiality it would be preferred if each member of the family dyad was interviewed separately, enabling participants to speak freely. However, dyads were given the choice of being interviewed together or separately, as it was recognised that some people living with dementia might not be comfortable being in another room by themselves.
Participants were asked for their permission to audio-record the interview. Digitalised voice recordings were later transcribed verbatim. Names of participants and their family members, along with place names and any other identifiable details, were removed from the text to maintain anonymity. Each participant was given an identification number.
The analysis followed a descriptive phenomenological method in psychology, as outlined by Giorgi (2009, 1997), which follows 5 steps: (1) assume a phenomenological attitude, (2) read through the transcripts, (3) create ‘meaning units’ or codes, (4) organise units into patterns of meaning or themes and (5) synthesis and explain themes across the sample (Giorgi, 2009, 1997). Emerging themes were formally presented and debated with health and social care research colleagues in a closed seminar format. In a process of ‘peer debriefing’ (Lincoln & Guba, 1985, p. 308), themes were agreed and finalised by LC and VD, with any disagreement resolved by discussion. These methods were used to confirm interpretations of the data by challenging and exploring their meanings, and thereby strengthening the credibility of the findings (Lincoln & Guba, 1985).
Participant characteristics
People living with dementia and carer characteristics.
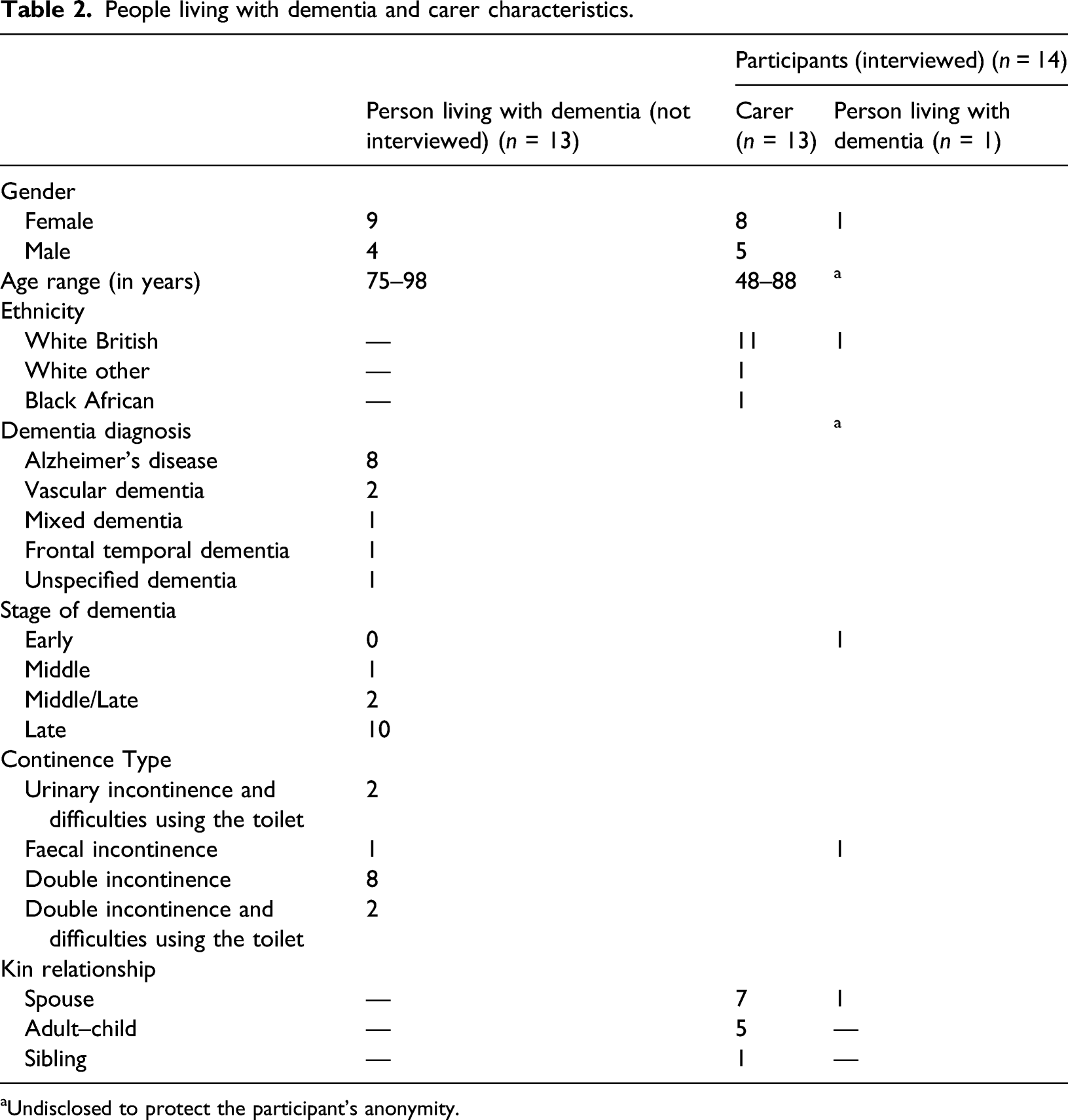
aUndisclosed to protect the participant’s anonymity.
Fourteen individuals (13 carers and 1 person living with dementia) participated in a total 33 interviews. There was attrition of carer participants over time, due to either their relative with dementia dying (n = 3) or moving to a care home (n = 1). Figure 1 contains a summary of participants’ engagement over time. Participants’ participation over time.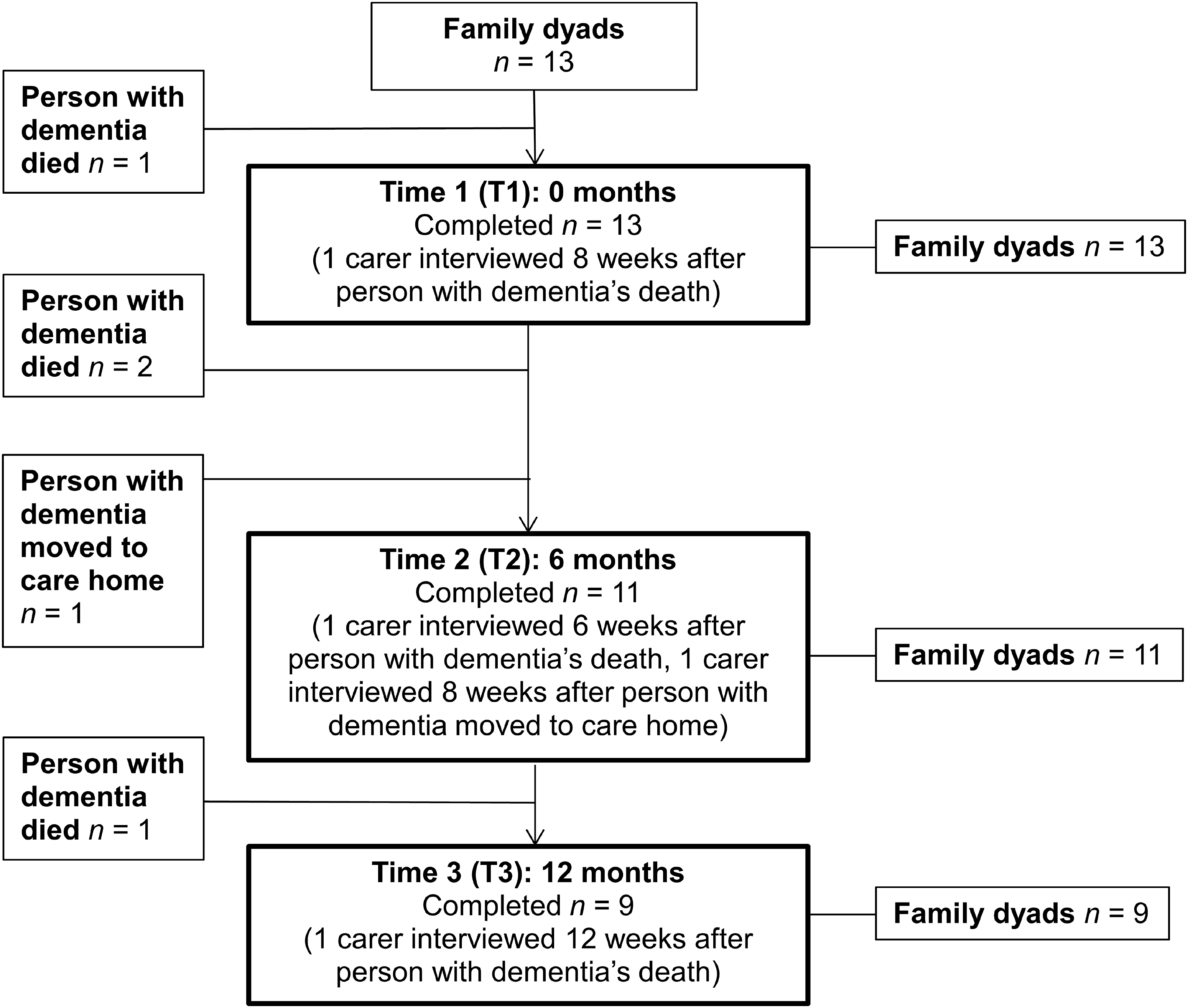
Findings
Findings were grouped in three overarching themes: (1) managing excreta and providing support with intimate continence care, (2) support from health and social care services and (3) impact on the family dyad relationship.
Managing excreta and providing support with intimate continence care
All the carers talked about intimate continence care and managing excreta in negative ways, acknowledging such caring tasks to be unpleasant and something that they did not like to do. Some viewed managing excreta as a necessity and part of their caring role, and others stated their emotional desire to assist their relative to manage continence and intimate continence care. In addition, whilst undertaking intimate caring tasks, many carers experienced uncooperative behaviours which they found difficult to manage or comprehend. These types of experiences and emotional responses are discussed in turn.
Negative emotional responses
Carers reported feeling several negative emotional responses when managing excreta, and were concerned about the appropriateness of providing this type of care to an adult, worrying about what others might think. Carers stated how difficult it was to perform these caring tasks for someone who had been so important in their lives, alluding to the irregularity of the need to provide intimate care to an adult, especially when they were formerly independent. The following exemplar indicates the perceived role transitions that family carers undergo in their relationships when they provide intimate continence care: “But it, it’s, it is difficult (…). I mean when your children are babies that’s one thing, but it’s very hard when it’s somebody you’ve cared for all your life and now you’re having to do things like this for them” (Wife, P04-T1).
The experience of family carers feeling embarrassed whilst performing intimate continence care tasks was also described. The issue of gender and kinship in providing intimate continence care was one of sensitivity for some participants. A brother gave the following reply when asked what it was like for him to help his sister living with dementia to the toilet: “…you, you seem to be posing a question at me as if though, ‘What’s this guy doing? He shouldn’t be doing this’”. (Brother, P12-T1).
This response suggests the carer’s concern about what others may think about the appropriateness of him caring for a relative of the opposite gender, perhaps acknowledging that cross-gender caring in this kin relationship is not the social or cultural norm.
Perceptions of necessity
Most family carers described the ‘necessity’ of intimate continence caring tasks and the ease in which they coped with such matters. They were pragmatic in their approach and goal focused. Some reported that if they did not help their family member get clean then no one else would, and the alternative of leaving them in soiled clothing or pads was just not an option. Another part of this necessity to care was to adopt a task-focused approach. This seemed to act as a coping mechanism for family carers in order to carry out intimate care tasks: “Well just a job as I say, just get on with it. Don’t think too much about it, you know what you’ve got to do with it (excreta), it’s got to get in the yellow bag. So, the sooner you get it in the yellow bag the better it’ll be for you” (Husband, P11-T3).
This spouse carer’s response demonstrates a suspension of any emotional or visceral responses to excreta in order to complete the task of managing the excreta effectively (i.e. the appropriate disposal of the soiled incontinence pad). Another carer reflected on managing excreta: “It’s not anything that bothers me. It’s not anything that bothers her (mother with dementia). It would bother me far more to leave it” (Daughter, P05-T3).
Emotional need to provide intimate continence care
Most carers mentioned in some way that they wanted to provide intimate continence care for their relative for as long as possible. An adult–child carer described wanting to continue to support her mother in this way to avoid exposure of her mother to outside help in intimate care: “Yeh. I know everybody can’t cope with things like that but that’s fine, yeh. I wouldn’t, from my point of view, I mean it might come eventually but, I wouldn’t like other people to do it, you know, I sort of, I like doing it, you know and I like doing the caring (slight laugh) and that, yeh… as long as we can, then, you know, we’ll manage ourselves, yeh” (Daughter, P08-T1).
Some carers explicitly confirmed that their need to care was due to their feelings of closeness towards their relative with dementia and reciprocity in their relationship. A husband carer stated his need to care was based on love: “…well I love the lady! And uh if she wants help she gets help, and it doesn’t matter whether it’s clean or dirty” (Husband, P11-T3).
Difficult and challenging experiences when using the toilet and managing continence
By far, the most problematic situations described by nearly all carers were when their family member was uncooperative or resisting their attempts to assist them to use the toilet or provide intimate continence care. An adult–child described her emotional response to her mother’s non-cooperation in the act of caring: “…what makes me cross is like when she won’t stand up at night to go to bed, or if she won’t let me take her pants down. That’s, they’re the things that irritate me, not the fact that she’s wet or you know” (Daughter, P03-T1).
Carers reported these episodes as very frustrating and stressful, sometimes resulting in angry outbursts, which they later regretted. Feelings of guilt after an outburst of anger were reported by many carers: “I shout. And then I go, and then, and then I walk away, feeling sorry that I done it her (…). And the only advantage that I have is that she doesn’t remember” (Husband, P10-T1).
However, carers often tried to find reasons for these non-cooperative behaviours to understand why their relative behaved in a way that seemed unhelpful and unlike their former selves. Empathising with the person living with dementia was evident in many of the carers’ accounts. A spousal carer described how she tried to hide her feelings from her husband whilst providing intimate continence care: “…it must be very painful for him to have me wipe his bottom. It must be. I would die. I would die if somebody did that to me. So I know that um, I know it’s not easy for him, so I say nothing about anything about it at all” (Wife, P01-T1).
Support from health and social care services in managing continence at home
For all family carers, the involvement of health and social care services and practitioners to support with the management of continence care was a major challenge rather than relief. Whether they had daily or less frequent contact, this engagement seemed to be a source of stress for carers, which had negative consequences on their family dyad relationship.
The impact of insufficient healthcare services
Nearly all family carers reported being unsatisfied with the healthcare that their relative received, stating that the service did not adequately support the management of continence at home. In the following example, an adult–child carer explained how she tried to manage and coordinate primary healthcare services (district nurses, general practitioners, pharmacy), to gain healthcare products to ensure that her mother’s ‘bedsore’ (reportedly incurred through a hospital admission) was adequately protected from her incontinence by fresh, dry, clean dressings. Her exasperation with services is emotionally recounted: “If you wanted to design a system to be difficult, disjointed, uh, frustrating and often didn’t work, this is the one you’d design. It’s an ah, it’s a dog’s dinner quite honestly. It’s dreadful. Absolutely dreadful” (Daughter, P05-T1).
Other carers talked about the lack of support from their local NHS continence service, and their persistent efforts to get the help that their family member required. Problems obtaining continence pads that fitted and contained the excreta were experienced by many and carers believed that their local continence service only offered the cheapest and therefore less effective products.
Many carers explained how the brand of continence pads had been changed by the local continence service and the new products they were supplied with were often considered to be of inferior quality. For one spouse carer, not only had the new pad left a blister on her husband’s hip, but she now used two pads at the same time to contain the incontinence. A son carer considered it imperative that his mother wore pull-up pads (akin to underwear) because she would take off any other designs such as slip-in or insert pads. He was repeatedly informed by the NHS continence service that pull-up pads were not available locally: “And because I was so persistent that I discovered that yes they do do it, you just got to, you got to fight for it. (Son, P06-T1).
He continued by explaining how he feared this ‘battle’ with the authorities to gain support, may have had a detrimental effect on his ability to care for his mother and their relationship: “I had to not only help care for my mum, but I had to, in effect, battle with the authorities to even get that basic need for her (…). I think it’s a bit of a scandal because um, in some way, indirect way, I’m sure it had an impact, a detrimental impact on my mum (…). Uh made, made me more tired and maybe I was a bit, sometimes I could get agitated with my mum because I was uh tired. Um, which is uh, which is a shame” (Son, P06-T1).
From these examples, it is clear that carers believed that the products provided by their local continence service were being rationed on cost grounds.
Gaining and maintaining control of social care
The importance of family carers maintaining the care (including intimate continence care) of their relative and the perceived impact of the threat of losing control of this were evident. Some carers felt that the care they provided was judged and criticised by those outside of the family dyad and feared that their role as the main carer might be taken out of their hands by professionals or other family members. A carer who had successfully defended the care arrangements for her mother with professionals said: “You feel that you shouldn’t have to battle people that are supposed to be helping you (…). So consequently, like in the future if I need help I’m gonna be really wary about asking cos I don’t wanna be taken over, I want an answer to my question” (Daughter, P03-T3).
Most carers perceived home care workers as encroaching on their dyad relationship, as they entered shared living space and interrupted time spent alone together. Some carers reported that they did not find it acceptable to have care workers in their home and in areas of their house that they felt were out of bounds to strangers, ‘ now they have to go into the bedroom’ (Wife, P09-T3).
Carers also discussed possible moves to a care home. Most carers believed that their family members would be better off living at home and considered that care homes would be either a lesser type of care, or even fatal for their relative. However, for some people living with dementia, increasing problems with mobility (or standing) meant that continuing to use the toilet at home seemed no longer an option, as they were unable to physically get to the toilet, and therefore a move to a care home was considered.
Impact on the family dyad relationship
All carers stated that their family dyad relationship had been affected by incontinence. However, the nature of the changes in their relationship due to the incontinence varied.
Intimate continence care does not negatively affect the relationship
None of the participants perceived that intimate continence care by itself had negatively affected their family dyad relationship. For carers, symptoms of dementia were solely blamed for any negative changes in the family dyad relationship, particularly changes in the person living with dementia’s personality, ability to communicate, mood and attitude towards the carer: “…having to care for him hasn’t affected the relationship but the fact is that we can’t communicate, that affects it” (Wife, P04-T1).
Likewise, another spouse carer did not see what providing intimate continence care had to do with their relationship: “…it’s continued our relationship it hasn’t affected it… It, it it’s the same because we just carry on. For better for worse, for richer, for poorer, all that. In sickness and in health. Well you make the promises, don’t you?” (Husband, P11-T1).
Intimate continence care makes the relationship stronger
Four participants (in three dyads) discussed how provision of intimate continence care had resulted in their relationship becoming stronger, as demonstrated in this example: “And the fact that, the fact that I’m able to do all this for (name of person living with dementia), has brought us much closer together. I might have thought that we were close then but a different sort of closeness when you’re not relying upon somebody.” (Wife, P01-T1).
One adult–child carer was able to compare his experience of assisting his mother with intimate continence care before and after the onset of dementia, and reported a loss in their relationship once the dementia was apparent: “before the dementia kicked-in, I would say, she was extremely happy that I had brought her home (from hospital) (…) and maybe, that in a stranger way strengthened our relationship even more, because she knew. Um. So, even though I had to do the personal care for her, she was happy where she was… Um so, and with all the personal care, helping her wash, helping her go to the commode. Um, it wasn’t, you know, life wasn’t easy but I don’t think it really did detrimentally impact on our relationship. In many strange sort of ways it made it possibly stronger. Uh, but once the dementia kicked-in, it just, the, the relationship was no longer there” (Son, P06-T1).
Indirect effects of intimate continence care on the family dyad relationship
Although when asked directly participants did not report intimate continence care as negatively affecting their family dyad relationship, there were several clear indicators that the management of incontinence had affected some aspects of the family dyads’ relationships but possibly not in a way that they overtly recognised.
For spouse dyads, sometimes this meant a change in sleeping arrangements. One husband explained how he had swapped their double bed for two single beds placed side by side. He had opted for separate bedding, tucked in-between the two beds to prevent his wife from rolling onto his side of the bed, and reducing the need for extra washing of sheets should they need to be changed through an occurrence of incontinence: “…the fact that I’m getting a better night’s sleep outweighs the other aspect of any sort of physical contact. As I say, she misses it, and I miss it you know, you just reach across and I’ll hold somebody’s hand feel that they’re there. But there we are, that’s, that’s life” (Husband, P07-T1).
In one of the few occasions when a spouse dyad was interviewed together, the couple explained the reasoning behind them reporting that their relationship had got stronger because of the person living with dementia’s (wife) incontinence. They talked over each other as they explained: Researcher: “And you say strengthened it (the relationship). You both said that actually, separately. I mean, can you explain that a bit more, how you think it might have strengthened it?” Wife: “And if you can love somebody despite, smelling…” Husband: “I mean it could be weakened couldn’t it? We could… I could walk out”. Wife: “…then that’s lovely”. Husband: “But I have no intention of doing that”. Wife: “Mm”. (Pause). Wife: “Can’t say more” (Husband and wife, P11-T1).
This extract demonstrates the differing perspectives of both participants; the wife explained her gratitude, whereas her husband alluded to the imbalance in their relationship.
Discussion
This study examines the experience of intimate continence care for people living with dementia and carers, and the effect this has on the family dyad relationship. Views and experiences were mainly from the perspective of providing intimate continence care (i.e. family carer); however, one person living with dementia was able to give their account of receiving this type of care and the effect this had on her family dyad relationship. Findings from this qualitative study show that participants experienced a variety of emotions and challenges, but some perceived their family dyad relationship to have been strengthened as a result of providing this type of care.
When faced with incontinence and excreta, most carers reported not thinking too much about what they were doing. Some spouse carers demonstrated the use of ‘bracketing’ as described by Twigg (2006); suspending any emotional or visceral responses to excreta in order to complete the task of managing the excreta affectively (e.g. the appropriate disposal of an incontinence pad). Their task was goal focused, ‘to make things right again’ and to ensure the person with dementia was dry and comfortable, taking responsibility to address needs (Tronto, 1993), and uphold their relative’s dignity (Merrick et al., 2016). The negative health and wellbeing consequences of leaving the person living with dementia unclean or uncomfortable clearly outweighed any concerns of the carer’s own personal feelings towards the task ahead. To “get on with it” was a common narrative that has been found elsewhere in the dementia family care literature (Cahill, 2000). However, feelings of disgust may occur, when bodily fluids are present outside the norms of Western society (i.e. uncontrolled and out of place), as described in the works of Douglas (1966), and Ungerson (1983). From this study, there is a suggestion that the ‘thought’ of having to deal with excreta might be worse than ‘doing’ the task, as many carers were surprised at their accomplishments of managing excreta.
Despite this, many carers felt frustrated when the person with dementia did not seem to want or understand their efforts to support with intimate continence care. Some carers thought that the refusal might be due to the person’s feelings of embarrassment, although it was unclear whether these were projections of the carer’s own feelings of shame and stigma of incontinence, or whether these were more perceptions of how the person with dementia might have felt as the care-receiver (Tronto, 1993). This alludes to the presence (or the expectation) of self-stigmatization and feelings of shame that ensue when a person is unable to conduct basic intimate tasks for themselves, which supports the work of Goffman (1963) and Milne (2010).
Participants reported that health and social care services did not always provide effective, individualised dementia services offering person-centred care or equipment, which took the family carer away from spending quality time with the person with dementia to manage the care package, which added to the family carer’s burden. Words such as ‘battle’ and ‘fight’ were often used by carers when explaining their interactions with health and social care services to ensure that needs were met. This perhaps indicates the energy used by the carers in acquiring an acceptable level of support, and the notion that they and service providers were somehow opposed to each other. It is evident that carers considered the result of inadequate services to be a negative physical and emotional impact on their health and their ability to provide care for the person with dementia, and negatively affected their family dyad relationship. These types of negotiations between health care professionals and family carers have been described by Redfern and colleagues (2002) as ‘second-order monitoring’, where family carers advocate on behalf of the person with dementia in order to gain the best care. Empirical findings from this study concur with Redfern et al. (2002), that second-order monitoring is a significant activity of the family carer. From an ethic of care perspective, it would appear, family carers and care providers negotiate their positions in the care arrangement to establish responsibility for the care and ensure the person’s needs are met (Tronto, 1993).
Family carers also reported feeling as though they were losing control of their care situation and felt judged by those outside of the family dyad. The importance of control for family carers of people living with dementia was investigated by Szabo and Strangs (1999) who found that ‘lacking control’ and ‘maintaining control’ were two dimensions which carers moved through and between. Consequently, carers also experienced ‘losing control’ (moving from maintaining to lacking control) and ‘regaining control’ (moving between lack of and maintaining control) (Szabo & Strang, 1999). Similarly, the loss of control and invasion of privacy were also described by Angus and colleagues (2005) in their ethnographic study of 16 adults receiving long-term home support from paid care workers in Canada (Angus et al., 2005). In light of these findings, a relational approach to care (e.g. ethic of care; Tronto, 1993) maybe beneficial for people living with dementia, family carers and practitioners to work together ensuring the care needs of individuals in the family dyad are adequately met and the family dyad relationship is supported (Clarke et al., 2020).
Some participants considered that intimate continence care had strengthened their relationship. Family carers saw caring as ‘an extension of their existing relationship rather than a new role’ (Beard et al., 2012, p. 8). The notion of a ‘continued relationship’, particularly for spouse carers has been found in other research (Beard et al., 2012; Merrick et al., 2016). In the United States (US), Beard and colleagues (2012) interviewed ten spouse couples, where one cared-for the other with Alzheimer’s disease or mild cognitive impairment, and discovered that a co-constructive approach to the dementia care experience was a positive adaptive process for the couple. Similarly, other research has demonstrated that couples bonded over their problems and experiences of dementia together and co-operated in meeting each other’s in a reciprocal manner (Clarke et al., 2020; Merrick et al., 2016). However, there was evidence that intimate continence care may have affected the quality and satisfaction of the relationship in negatives ways. One example was how providing care can change power dynamics in the dyad relationship. This potential for a power imbalance within the family dyad relationship concurs with an ethic of care approach, which acknowledges that receiving care can place the person with dementia in a vulnerable situation and susceptible to overprotective or paternalistic behaviours from the carer (Barnes, 2012; Tronto, 1993). Changes in the family relationship as caring activities increase and become more dominant in the dyad interaction have been reported by Savundranayagam and Montgomery (2010) who found in their quantitative study of older adults that this caused incongruence and discrepancies in how carers viewed themselves as a family member of the person they cared-for.
It was the aim of this study to explore the lived experiences of both individuals in the family dyad; the unit of analysis being the dyad and not either the family carer or the person living with dementia. From a relational perspective, this is important as the views of both individuals in the dyad are required (Merrick, et al., 2016). However, this was not possible as most people living with dementia in the family dyads did not have the cognitive ability to take part in the research, and consequently were unable to give their own account. Although the methods and design of the study tried to address some of the typical obstacles that prevent people living with dementia from taking part in research, mental capacity remains a significant challenge to informed consent and participation in interviews (Samsi & Manthorpe, 2020). In this study, people with dementia who were unable to provide their consent were experiencing dementia in the later stages. Perhaps, this indicates when difficulties with managing continence typically occur, or that gaining the views of people in the earlier stages of dementia (and therefore more likely to have capacity) is difficult due to the multiple stigmas that surround these subjects (e.g. dementia, incontinence and ageing) (Bamford et al., 2014). Therefore, people living with dementia’s perspectives on and lived experiences of receiving intimate continence care, and the effect this had on their family dyad relationship, are largely absent, and the ‘voice’ of people living with dementia was not adequately represented in this study. However, one person with dementia’s contribution is available and valuable as the combined interview with her husband adds to the richness of this study. The intricacies of this dyad’s relationship indicate the nature of imbalanced family care relationships, and the differences in how people living with dementia and their family carers may view these disparities.
A critical review of continence care for people living with dementia living at home has indicated the lack of research and knowledge in this area (Burholt et al., 2020). Although the experiences of incontinence and problems with using the toilet for people living with dementia and their carers living at home have been explored (Cole & Drennan, 2019; Drennan et al., 2011), more research is required about the different aspects of intimate continent care and how policy and practice can use this knowledge to better support people living with dementia and their families living at home (Burholt et al., 2020; Gove et al., 2016). This particularly involves the closer working of continence and dementia services and possible integration of funding streams (Drennan & Cole, 2009), which will remain an ongoing challenge given the disruption to services that the COVID-19 pandemic has brought (Alzheimer’s Europe, 2020).
This study was conducted prior to the COVID-19 pandemic, and is limited in the small numbers of interviews and only one person living with dementia being involved. There is a risk of bias in that participants may have wanted to provide socially acceptable responses and that the study recruited people with particular experiences and confidence. Likewise, organisations and services that helped with recruitment may have identified and introduced specific carers to the study. The views of carers who could not cope with intimate continence care remain under-reported.
Conclusion
This study concentrated on one specific aspect of care for people living with dementia and their family carers living at home, the nature of intimate continence care. Managing excreta infringes on the norms of a family dyad relationship and can be emotionally and physical difficult for family carers and people living with dementia. Although providing intimate continence care at home was perceived to have sometimes made the family dyad relationship stronger, non-integrated and insufficient health and social care services were reported to have put additional strain on the family carers which consequently affected the family dyad relationship. Sustaining caring relationships, such as maintaining the quality of the family dyad relationship, is important as it is an indicator of quality of life for those in the family dyad (Alzheimer’s Society, 2010) and may help to ensure that the person with dementia remains well supported at home for longer.
Footnotes
Acknowledgements
We thank the professionals who aided recruitment and the participants who were interviewed for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents a doctoral research study supported/funded by independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-06061005). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.