
Abstract
COVID-19 pandemic and subsequent lockdowns created a global public health crisis generating mental health problems including social isolation, stress, and anxiety especially for persons with dementia and their carers. This article reports on the use of digital technology to maintain social connectivity via a virtual group session that focused on the topic of “what is home.” Participants in this session included 16 day-care center clients representing an immigrant community identified with mild to moderate cognitive impairment. A trained psychodrama therapist conducted the virtual group meeting based on five key techniques: spectrogram, role reversal, doubling, mirroring, and soliloquy. The NVivo software was used for the qualitative analysis of the transcribed video recording to identify key themes based on grounded theory methodology. Zooming from home, clients engaged in significant social interaction. Findings of the NVivo analysis identified the following themes of “what is home”: Emotions and home, Home is family, Home is community, and Reminiscence (with objects and traditions). Findings suggest that digital interactive technologies, like Zoom, enhance social connectivity thus mitigating the negative impact of social isolation for persons with dementia especially during pandemic lockdowns. Our pilot findings based on virtual group meetings from home demonstrate that participants can express significant emotive capacity and enhanced connectivity with one another despite a diagnosis of mild to moderate dementia. While larger studies are needed to confirm these findings, we suggest that this methodology may be used to support persons with dementia not only in times of pandemics but also as an addition to other community and home care services. Changes in reimbursement policies to include these innovative home services may be helpful in building more resilient communities for the more highly vulnerable populations.
Introduction
The COVID-19 pandemic was declared by the World Health Organization on March 11, 2020 (WHO Regional Office for Europe, 2020a). Numerous data in lay press, local governments (Centers for Disease Control and Prevention, 2020; European Centre for the Disease Prevention and Control, 2020; Government Response to Coronavirus, COVID-19, 2020), the WHO organization (WHO Regional Office for Europe, 2020b, 2020c), and academic sources (Brooks, et al., 2020; Holingue et al., 2020; Marroquin et al., 2020) focus on the mental health effects of social isolation policies activated to contain the pandemic. The guideline most strongly and frequently declared is “Stay at Home” thus ensuring safety and physical distancing. The consequences of these guidelines have had dramatic mental health impacts on the general population regardless of previous history of mental disorder. The segment of the population impacted rather severely involve persons living with dementia, their families and paid carers (Wang et al., 2020; Prime, et al., 2020; Russell, et al., 2020; Sheth, et al., 2020). The result of social isolation and anxiety along with the possibility of behavioral changes and confusion place persons with dementia at risk of being hospitalized and further exposed to COVID-19 (Barclay & Rees, 2020; Livingston, et al, 2020). In addition, families caring for a person with dementia may feel cut off, overwhelmed and anxious, particularly if loved ones are living with complex health conditions and are at greater risk especially if they are aging at home and not in a long-term care facility (Cipolleetta, et al., 2021; Cruz, et al., 2018; Hwang, et al., 2021; Lombo, et al., 2021; Ramos, et al., 2020; Tulloch, et al., 2021; Werner, et al., 2021; Zucca, et al., 2021).
Israel’s elderly population has unique characteristics because the country receives a steady stream of immigrants from 119 countries, including many who are Holocaust survivors, representing a wide range of ethnic, economic, health, educational, and cultural differences (The 65+ Population in Israel, 2018; Mainstreaming Aging in Israel, 2020). Unlike other Western countries, many persons living with dementia in Israel reside with their families who are their unpaid informal caregivers (Mashav, 2014). Approximately two-thirds of home care services are provided by live out home care workers (primarily Israeli) and one-third by live-in foreign caregivers, mainly from the Philippines, Nepal, India, Sri Lanka, Ukraine, Moldova, and others (Iecovich, 2012).
National Health Insurance coverage is assured for all citizens and foreign caregivers as well as the availability of private health care plans. In her position paper, Cohen-Mansfield discusses the potential impact of Israel’s health policies along with improvement in care for long-term, care facilities and community-based care during the corona pandemic (Cohen-Mansfield, 2020). With the closures of day centers for older persons, she recommends that organizations: “enable older adults to use technology to maintain contact with relatives and others; organize discussion groups similar to clubs for older adults using technology; and promote and support physical, social and cognitive activities through relationships with family members, caregivers, volunteers and others” (Cohen-Mansfield, 2020, p. 212).
Giebel, et al. (2021) describes how COVID-19 has exacerbated British social policy and the inequities of dementia care in the UK especially for those who wish to live at home. “While remote support does by no means replace the benefits of face-to-face support … accessing social activities online are better than being completely cut off from any kind of social contact” (Giebel et al., 2021, p. 2). Technological innovations have been implemented to mitigate some of the negative impact of social isolation during the corona pandemic. In this paper, we present the use of Zoom technology with persons with dementia (Brown, et al., 2020; see also Cuffaro, et al., 2020) focusing specifically on the meaning of “home” since this is the place where persons with dementia and their carers spend most of their time. Though research samples are small, studies have shown that virtual communities provide opportunities for social interaction and activities, for feelings of being a valuable and contributing member of society, for engendering a sense of identity, for giving and receiving support, and for relieving strain on the caregiver (Birt, et al., 2020; Hoel, et al., 2021; Pinto-Bruno, 2016; Samtani, et al., 2021; Talbot, et al., 2021; Martin Van Jaarsveld, 2020). For the purposes of this article, the group psychodrama Zoom session’s theme of “Home” illuminates different yet similar experiences of how individuals define home. COVID-19 provided the researchers a unique opportunity to connect with clients in their homes and share this experience with their families and other carers.
Methodology
Background
Melabev Community Clubs for Eldercare, a non-profit memory care day center for persons affected by all stages of dementia, provides a safe, supportive, and relationship-centered environment for a variety of therapeutic activities. When the center closed due to COVID-19, the professional staff faced the following dilemma: Would the well-established, close relationships between staff and clients and the connectivity that the clients had developed with one another who attended within the day center environment transfer to a Zoom online community from their homes?
The persons living with dementia described in this article range from 70–100 years of age and are English-speaking immigrants to Israel from a variety of cultures and countries. Prior to the pandemic, they participated in the day care center within the framework of the “Memory Club” with programming specifically designed for mild to moderate dementia as measured by MMSE (20 to 24/30) or MoCA (15 to 22/30) scales and with their physicians’ recommendations. The Memory Club members attend the day care center participating in different kinds of activities such as cognitive exercises, movement, music therapy, bibliotherapy, and gardening. In addition, they also have a weekly 70-minute session of psychodrama led by a psychodrama therapist who has been working with this group for over 5 years using psychodrama techniques described below. With the COVID-19 pandemic lockdown and closure of the center, we initiated new technology like Zoom focusing on music, movement and, with this group, other psychodrama themes including (1) “There’s a Place for Us” using an adjective to describe oneself and another person in the group; (2) Reflections on lockdown and seeing children and grandchildren from a balcony or garden; (3) “You’ve Got a Friend” birthday celebration of a staff member who has been with the group for 7 years. Session included greetings from spouses, carers, and clients along with music; (4) Celebrating holidays and traditions; and (5) 100th birthday celebration of a client with greetings and music. However, this article focuses only on one psychodrama group session via Zoom focusing on the meaning of Home as expressed by day center clients affected by mild to moderate dementia. We chose this topic because Home is the common theme to our clients’ existence: they are all aging at home; they were all confined to home during the pandemic; and, as immigrants, they all had the spiritual motivation to move to Israel, the Jewish homeland.
Meaning of home
“Aging in place” is a popular term in current aging policy (Office of Policy Development and Research Department of Housing and Urban Development, 2013), but simplistically it is usually defined as living in one’s own home, in the community of choice, and with some level of independence, rather than in a long-term residential care facility. Establishing a home is a basic cultural act, as domestic order expresses some of the most basic cultural notions about personhood and social life that one acquires throughout one’s life due to life experiences (Bourdieu, 1973, 1977, 1984, 1990). The home environment represents bodily places of relationships and physical connections with space that are not just lived in, but lived with throughout one’s lifetime (Imrie, 2004; Rubinstein, 1989). Wiles (2011) relates aging in place with a sense of identity through caring relationships and roles found especially in one’s own home. The home environment is not only a source of emotion and meaning, but also plays a critical role in maintaining a sense of self-image and self-identity and how old age is experienced. Rubinstein (1989) describes the importance of an older person’s physical environment as having the potential for lasting longer than their own bodies, a space that is loaded with personal meaning, and thus aiding in the maintenance of self, especially when faced with physical and cognitive decline. One’s physical environment and its objects may come to embody an older person’s key ideas, values, or personal themes, and may function as part of one’s “prosthetic self” (Rubinstein, 1989, s50).
Psychological meanings of home have been associated with security, refuge, privacy, and reflection of one’s ideas, values, and memories (Kontos, 1998; Kontos et al., 2020). Home gives a sense of security and protection, especially to older persons who may feel vulnerable in public spaces (Dyck, et al., 2005). A sociological perspective recognizes home as the center for family life, a place of retreat, freedom and independence, and a place of continuity and permanence (Collier, et al., 2015). Others describe the meaning of home as a constantly changing dynamic process which may contribute to any place feeling like home as long as it is familiar—with familiar activities, familiar people, and familiar objects (Case, 1996). Other research shows that feeling at home is not necessarily about a certain place but about a way of being in the world (Moore, 2000). While anthropological studies acknowledge house and home as a basic physical need for shelter, the literature about home increasingly focuses on the human desire and struggle for belonging (Samanani & Lenhard, 2019). This is especially true for an immigrant population whose experiences of home have traversed continents and cultures. In this article, we focus on illuminating persons with dementia perceptions of “Home” as expressed through psychodrama techniques during a Zoom session.
Psychodrama
Psychodrama, the original form of group psychotherapy, was developed in the early 20th century by a Romanian-American psychiatrist Jacob Levy Moreno (Moreno, 1985; Moreno, 2014). He described psychodrama as “the method that explores the truth of one’s soul through action…” (Moreno, 1959, p. 77). With deep roots in theater, psychology, and sociology and preferably performed in a group format, psychodrama focuses on the uniqueness of the individual as the interchange of various life roles including life’s difficulties and remaining abilities (Cruz et al., 2018). Considered to be individual therapy in a group format, the enactments may represent the various roles that s/he assumes throughout life (Blatner, 1997). The approach, grounded in principles of creativity and spontaneity, combines sociometry, group dynamics, and role theory in order to evoke cognitive, emotional, and behavioral responses where individuals share their insights, inner strengths, and coping methods (Skolnik, 2018). Tian Dayton states, “Psychodrama speaks the words we dared not speak but had shouting within us” (Dayton, 1994, p.9).
Examples of techniques applied during this psychodrama session include spectrogram, role reversal, doubling, mirroring, and soliloquy (Cruz, et al., 2018). Useful as one method of warming up a psychodrama group, the spectrogram is both diagnostic and therapeutic by making abstract issues concrete and empowering the participation and commitment of usually nonverbal members (Kole, 1967). Typical methodology involves five phases: warm up, action, working through, sharing, and closure (Kellerman, 1992). Through the psychodramatic, experiential depiction of memories of real-life situations or unresolved issues, persons affected by dementia might recognize a connection between past and present in order to discover a sense of purpose and dignity in the present (Knittel, 2016; see also Landy, 1996). Life dramas unfold in unpredictable ways yet they do have patterns of recurrence when previous events create scene memories that frequently have their inception during childhood (Tomasulo, 2010).
Project design
The qualitative research design included participant observation, notes, video recording, and transcription of a psychodrama session. Family members and other carers were trained by Melabev team leaders on how to set up and assist with the technology. Grounded theory was used in the qualitative data analysis (Charmaz, 2014, 2016; Corbin & Strauss, 2015). Two staff members familiar with the participants reviewed the transcript from the video recording.
Methodological considerations
Ethics and consent
All participants, family members, and staff were assured confidentiality and anonymous presentation in the findings. Signed consent is on file with the Melabev English-speaking Day Center. The procedures of Process Consent (Dewing, 2008) and assent (Black, et al., 2010) were applied with the clients throughout the session for their continued agreement to participate. Aspects of trustworthiness in studies with a qualitative approach include credibility, dependability, transferability, and authenticity (Elo, et al., 2014). The credibility of our study could have been compromised since verbal and nonverbal expressions are often difficult to interpret, especially through Zoom technology. However, the long-established relationships among all participants assisted in mitigating this challenge. Dependability was ensured in several ways: field notes recorded including reflections; observers collaborated after the session; insider/outsider interpretations considered (Cruz & Higginbottom, 2013). To facilitate transferability of our findings, we describe the characteristics of the clients, provide rich descriptions of their homes as viewed through Zoom, and include participant quotations. Addressing authenticity involved an accurate description of the research process from data collection to writing the manuscript as well as the relevance of the study in a societal perspective, particularly during COVID-19.
Data collection and analysis
Setting the stage
Social memory (or collective memory) is a concept used by historians to explore the connection between social identity and historical memory, particularly of diverse populations who, despite their differences, consider themselves a member of a shared group (French, 1995). The cultural built environment of the day center provided the space that created a sense of identity and purpose where the loss of cognitive abilities and verbal communication skills did not interfere with the ability to develop social ties. When clients are afforded the right environment despite their cognitive impairment, they have the opportunity to impact others in their surroundings and engage in reciprocal relationships of giving (Berenbaum, et al., 2020). The newly created online Zoom environment with persons familiar to one another from the day care enabled the clients to feel more comfortable sharing emotions, especially when they can read and call out one another’s names written on each Zoom screen square. Throughout the session, the therapist and staff observed clients for signs of distress or confusion in order to alert carers to intervene.
After viewing a shared-screen music video highlighting the theme of home, the therapist posed the question, “What is home for you?” The therapist made general observations, probed deeper when appropriate, allowed clients to share difficult memories, and provided space for others to react while making connections and bridges to the next person. Spouses and carers were encouraged to participate; clients who were less focused relied upon spouses and carers for support and voice. While families and carers were part of this Zoom session, the analysis of themes is based solely on the participants of the day center. Thirteen of 16 clients responded verbally more than once throughout the session for a total of 38 responses. Four spouses and six paid carers prompted the client or assisted in showing an item from the home; two spouses and one paid carer spoke in response to the therapist’s question on behalf of the person. Through sharing meaningful, physical objects from their homes, participants voiced a sense of belonging, vitality, value, and intimacy. Through interaction by doing, showing, and sharing, they offered their insights, inner strengths, coping methods, and social connectivity while internalizing the experience through their actions, all from the comfort of their own homes.
Setting/participants
Socio-demographics of research participants.
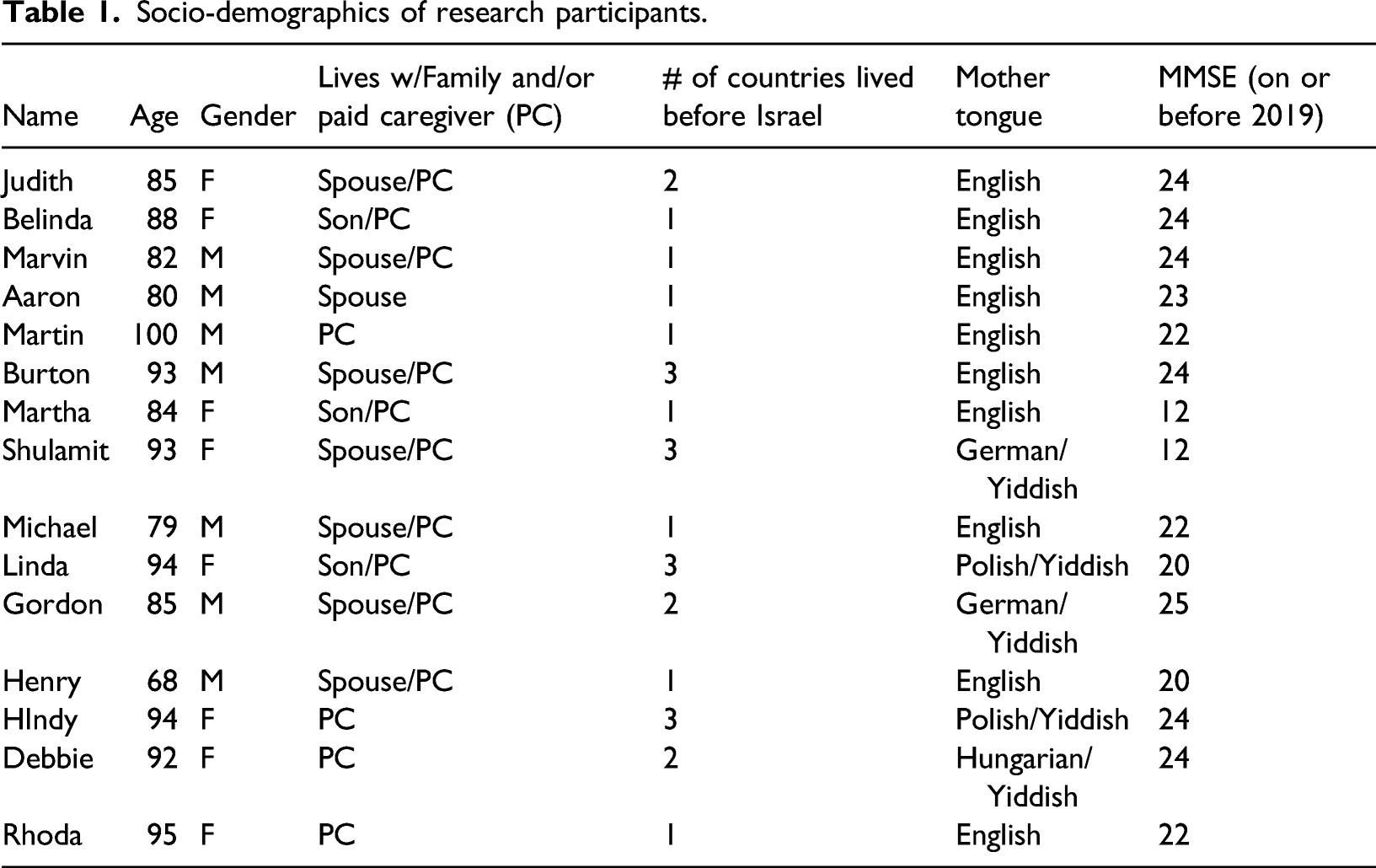
Melabev staff contacted families and paid caregivers by phone and email to provide Zoom instructions. They were advised on the optimal seating position of the client in front of the camera, audio adjustment, operation of the mute function, and blocking the video if necessary. Family members and other carers were invited to participate along with two staff persons, two volunteers, and the psychodrama therapist. Since client safety and well-being are a high priority, a family member or designated carer was available at all times should they experience any agitation or discomfort, including toileting, and to assist in technology related challenges. Experienced staff members were also present to observe the participant’s verbal and nonverbal reactions. Two independent observers reviewed and recorded the main themes that emerged. These themes as well as the actual recorded words of each participant and the major themes that emerged regarding “home” were analyzed through grounded theory (Charmaz, 2014, 2016; Corbin & Strauss, 2015) and are presented in this paper.
Findings
The Zoom environment offered challenges and opportunities. Therapeutic goals involved creating a safe and dynamic environment on the screen that would enable spontaneity, validation, connection, social cohesion, engagement, identity, and belonging to the group. The 70-minute session opened with the therapist greeting everyone individually, asking everyone to do a self-hug, and then connecting with others by extending arms, hands, and fingers. During the Zoom session, the therapist initiated 16 requests that required additional physical action/responses including clapping, waving, and raising hands. Upon examining the video recording and subsequent transcript, all 16 clients responded at least once yielding 119 physical responses to solicited action requests by the therapist.
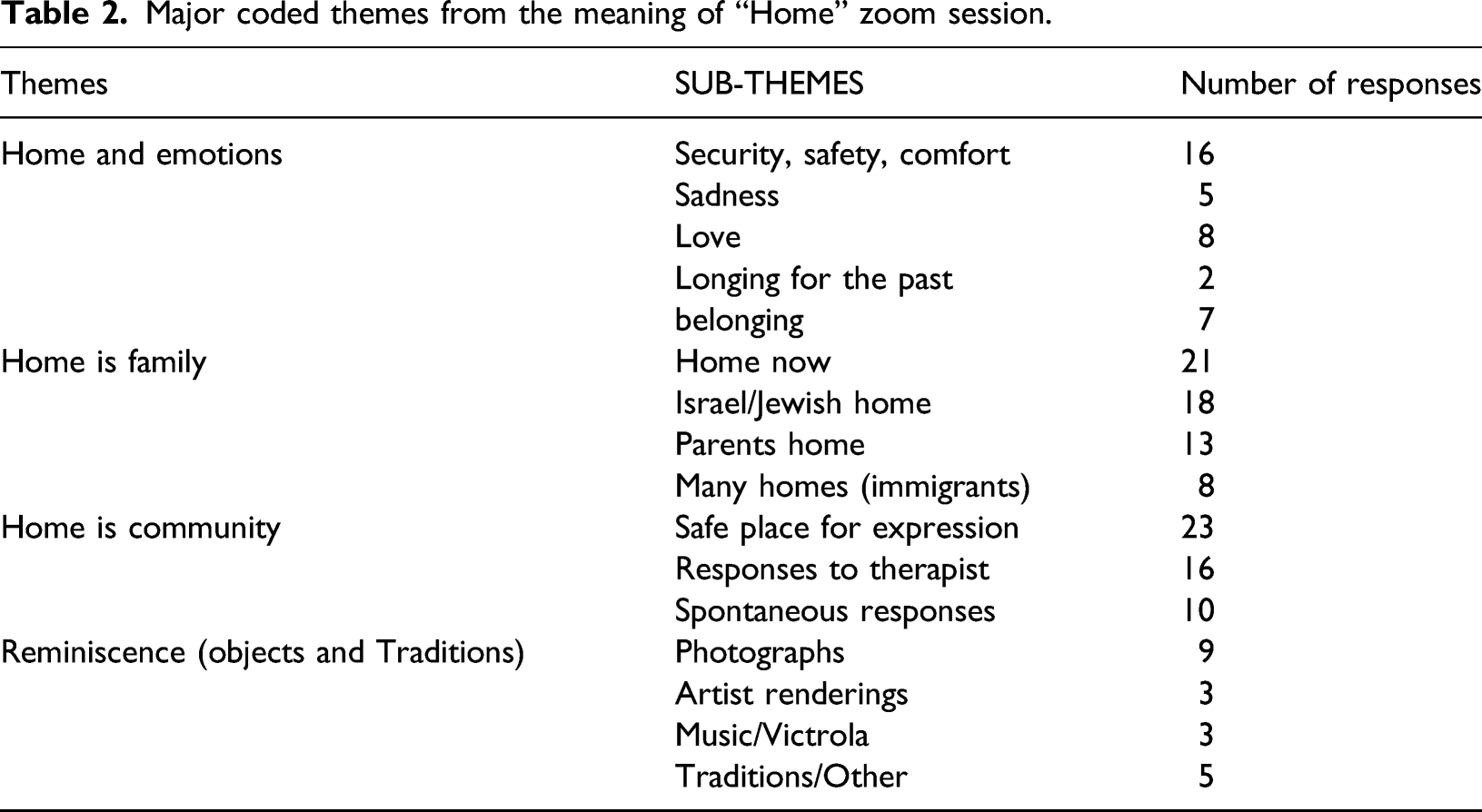
Major coded themes from the meaning of “Home” zoom session.
Quotes from participants.
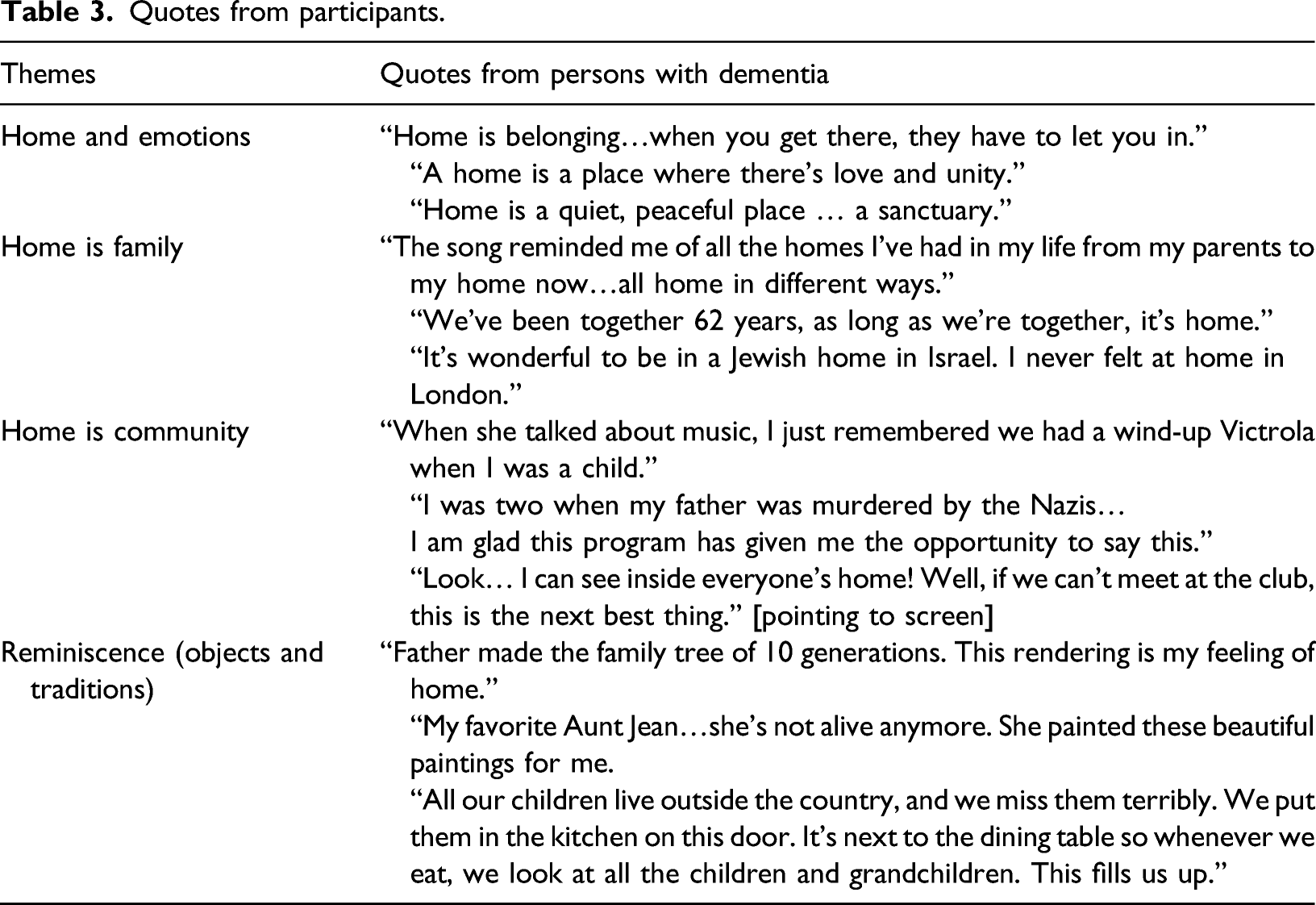
Key themes that emerged from the coded data of the video-recorded virtual sessions, include (1) Home and Emotions (sharing feelings of love, sadness, safety/security, and belonging); (2) Home is Family (sharing memories of childhood, sharing experiences of many homes because of their immigrant experience, the importance of cultural identity of a Jewish home, and reflections on their home now in Israel); (3) Home is Community (expressions of trust and safety within this small group, responsiveness to the therapist, and spontaneous responses among the participants independent of outside stimuli); and (4) Reminiscence with Objects and Traditions (sharing of objects and traditions of importance and value that expressed personal and cultural identity). In order to capture the richness of the content, the video recording was manually transcribed by the author, a practitioner-researcher experienced in qualitative, ethnographic methodology.
Discussion
Our analysis which focuses on a virtual group session demonstrates that persons with mild and moderate dementia are able to socially connect and engage in activities not only in person, but also through interactive communication technology. Culture is key to their maintaining and expressing their embodied self-identity and their remaining emotive capacity—on some level, persons affected by dementia do not forget where they come from (Fuchs, 2020). Research conducted by a group from Montreal focused on the in-action practices of social inclusion within a community day center for persons with mild to moderate dementia (Motta-Ochoa, et al., 2021). Their findings highlight the importance of soliciting feedback from individuals with dementia and the social inclusion demonstrated by these individuals with the staff and one another (Motta-Ochoa, et al., 2021).
Limitations
Despite our promising findings, there are some limitations of our work. This study cannot be generalized due to several conditions: the unique timing due to the COVID-19 pandemic, the small sample size, observations limited to one 70-minute session, and an established community of participants, staff, and therapist with in person experience of previous psychodrama sessions of over 5 years. Our study also includes only those with mild to moderate dementia and are therefore not representative of all persons with dementia. Future studies using larger and more representative samples should be conducted in order to increase confidence in our preliminary findings and to explore the associations between technology usage and well-being.
In addition, the participants in our sample occupied privileged positions to be able to access the internet and digital technology with the assistance of family members and carers. This may not be the case for individuals who live rurally or who are from lower socio-economic backgrounds. This study therefore provides an important foundation for understanding how people with dementia and their caregivers use digital technologies and the challenges they face.
Despite limitations in the body of literature and in this study in particular regarding technology-driven interventions in dementia caregiving, findings suggest benefits for social connectivity for persons with dementia as well as their caregivers. Further research on this topic is needed in order to provide insights into which approaches are the most useful for people with dementia to increase their social participation.
Conclusion
Our analysis demonstrates that the participants affected by dementia were engaged emotionally during the Zoom meetings and able to socially interact through the virtual environment. Therefore, notwithstanding their diagnosis with dementia, emotive capacities appeared to stimulate significant cognitive abilities in working memory. Despite the generally held belief that technology is challenging for this population, our findings demonstrate that with appropriate guidance and minimal training for families and paid carers, persons with dementia will engage with the technology in a variety of ways (Dahlke, et al., 2020; Gilson, et al., 2019; Goodall, et al., 2021; Shu, et al., 2021; Talbot, et al., 2021; Martin Van Jaarsveld, 2020). The combination of psychodrama, culturally sensitive reminiscence therapy, and an established community enhanced their social cohesion, social connectivity, and remaining emotive capacities in the face of dementia.
The new environment of technology made this possible even under coronavirus pandemic restrictions. We, therefore, suggest that those working with persons living with dementia in community settings may benefit from training in the use of interactive communication technologies to enhance the life of those living with dementia and their carers (O’Donnell, 2021). To explore this possibility, specialized staff training programs need to be developed for staff and recognized by the professional societies of social and health related professions as an essential element of their training, qualifications, and continuing certifications. While the technology can be helpful in a crisis situation, it should not be perceived as a preferred means of connection with persons with dementia. Further research on this topic is needed in order to provide insights into which approaches are the most useful for people with dementia to increase their social participation. The importance of making available interactive communication technology for persons with dementia and to see them socially connect and engage through a medium that is not part of their generation has far-reaching implications not only for future research but also for policy considerations to mitigate social isolation and to enhance the lives within this vulnerable population, including the impact of supporting someone with mild and moderate dementia.
In addition, our study suggests that it is important to explore further the use of technology in creating more resilient health delivery systems to deal with pandemics and other emerging crises. For this type of health intervention, reimbursement policies need to be considered along with other health services delivered in the home, not the traditional health care setting (Tziraki, et al., 2020). Persons with mild and moderate dementia should be included in studies and training on the use of modern resources and communication technologies to stay connected with extended family and their community. In addition, the role of carers during the COVID-19 pandemic needs to be explored further. The use of technology allowed the carers to have a first-hand experience of what happens at the day care center. Since the corona pandemic has also affected their own mental status, we need to consider the impact of this population and their responsibilities caring for persons with mild and moderate dementia. If technology-based interventions during lockdowns can also assist them in coping easier, health policy changes need to include the dyad of both persons diagnosed with dementia and their paid carers and/or family members to enhance resilience building for both the individual and for those caring for them.
Footnotes
Acknowledgments
We would like to acknowledge MELABEV staff members Jenny Breuer who assisted during the Zoom session along with Gila Gimpel and volunteer Miriam Stein, and Dvora Marcus, Director of the English-speaking MELABEV Day Center for her continued support. A special thanks to our clients, their families, and their carers who make this all worthwhile.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.