
Abstract
This article reports on findings of a scoping review aimed to map the published literature concerning the impact of Covid-19 on the care and quality of life of people living with dementia and their carers. Twenty-nine articles were included in the review. Three overarching themes were identified: (1) Impact on people with dementia – unmet and increased care needs; (2) Impact on carers – increased stress and burden and (3) Impact according to demographics. Overall, findings show that Covid-19 has led to a reduction in support from health and social services and to a move towards technology-based support. Furthermore, Covid-19 has had a negative impact on the care and quality of life of people living with dementia and their carers, and that this impact was influenced by the severity of dementia.
Introduction
Dementia has become one of the greatest healthcare challenges of the 21st century, linked to high demand for medical, social and institutional care (Ibarria et al., 2016; World Health Organization 2017; Lindeza et al., 2020). Family carers play a major role in supporting people with dementia, not only in their daily activities and personal care, but also in preserving the individual’s sense of self and mental wellbeing (Dening et al., 2012; Farina et al., 2017; Lindeza et al., 2020). The challenges of caring are significant, and a large body of scholarly evidence demonstrates the detrimental impact on the physical and mental health of dementia carers (Connell et al., 2001; Schoenmakers et al., 2010; Gilhooly et al., 2016; Lindeza et al., 2020). Supporting the estimated 50 million people affected by dementia worldwide has therefore become a key national and international health policy priority (World Health Organization, 2012; Alzheimer’s Disease International (ADI), 2016). Due to the unprecedented situation and concerns regarding the impact of Covid-19 on people with dementia and their carers, there has been a high volume of rapidly published research. In this review, we explore evidence concerning the impact of Covid-19 on the care and quality of life (QoL) of people with dementia and their carers. QoL is highly debated but widely recognised as a multi-dimensional construct comprising both subjective and objective aspects (Bowling, 1995). In relation to dementia and for the purposes of this review, we draw on the conceptual model developed by Lawton (1997). This model considers QoL across four domains: 1. Behavioural competence (ability to function in adaptive and socially appropriate ways, e.g. social relationships with family and friends, and social engagement); 2. Objective environment (aspects external to the individual, e.g. physical safety, presence of amenities, housing/place of residence and healthcare); 3. Psychological wellbeing (e.g. happiness, agitation, depression, affect state, emotional expression and spirituality) and self-esteem (self-esteem, life satisfaction and morale) and 4. Subjective satisfaction with the overall QoL.
The need to focus on people living with dementia and their carers has been heightened as a result of the Covid-19 pandemic. During most of 2020 (and a significant proportion of 2021), quarantine rules, designed to protect those most at risk, have led to restricted freedoms, limited contact with others and potentially increased isolation of people living with dementia and their carers. Furthermore, government responses to Covid-19 have prioritized income support and the withdrawal of health and social services, support groups, social activities and respite care initiatives, limiting the level of formal and informal support available (Daly, 2020; Giebel et al., 2020a). Relatedly, international evidence is beginning to emerge that demonstrates that people with dementia are disproportionately impacted by Covid-19 with the condition exacerbating the risk of mortality (Alzheimer’s Disease International (ADI), 2020; Numbers & Brodaty, 2021). For example, evidence from the National Health Service (NHS) in the UK shows that people with dementia were at a higher risk of Covid-19 hospital deaths (Williamson et al., 2020). Similarly, estimates show that people with dementia accounted for nearly one third of all Covid-19 related deaths in Scotland and a quarter of such deaths in England and Wales (Suárez-González, et al., 2020) The particular vulnerabilities to Covid-19 that people with dementia face, coupled with a specific type of policy response, raise important questions concerning the impact of the disease on the QoL of people with dementia. It is particularly important to understand whether the impact of Covid-19 can be traced along lines such as gender, type of dementia and severity, and living arrangements all of which have been shown to have an impact on QoL outcomes of people with dementia and their carers (Schumann et al., 2019).
The aim of this scoping review was to map research on the impact of Covid-19 on people with dementia and their carers. Specifically, we consider: ⁃ How Covid-19 and linked changes in provision of services have influenced the care and QoL of people with dementia and their family carers? ⁃ How the impact of Covid-19 differs according to diagnosis and illness severity, type of care facility (i.e. primary care, acute care, residential care, the community, etc.), gender and other relevant demographic characteristics?
Methods
A scoping review methodology was chosen, as this is an emerging and rapidly evolving area of research. Scoping reviews aim to provide a ‘map’ of the available evidence on a topic area (Aromataris & Munn, 2020). They do not focus on assessment of included studies but, instead, they are concerned with systematically charting a broad area of research with the aim of summarizing overarching findings and identifying gaps in the existing research literature (Arksey & O’Malley, 2005). The methodology for this review draws on the scoping review guidelines developed by the Joanna Briggs Institute (Peters et al., 2015). The objectives, inclusion criteria and methods for this scoping review were specified in advance and documented in a protocol developed by the team.
Eligibility criteria
Articles were included if: (1) the primary focus was people with dementia and their family carers; (2) the settings for the research reflected the community or care settings (hospitals, nursing/residential care homes and assisted living facilities); (3) they reported on primary research data on outcomes related to care provision and/or QoL; (4) they were reviews of primary research with a replicable methodology and (5) they were published in English. All types of study designs were considered.
Articles were excluded if: (1) they did not have a clear focus on people with dementia or their carers. For example, studies where dementia was one of many variables and where it was not possible to disaggregate the reported results (e.g. research looking at all residents in a care home setting); (2) they did not report primary research data (e.g. commentary or opinion piece) and (3) they were not published in English.
Search strategy
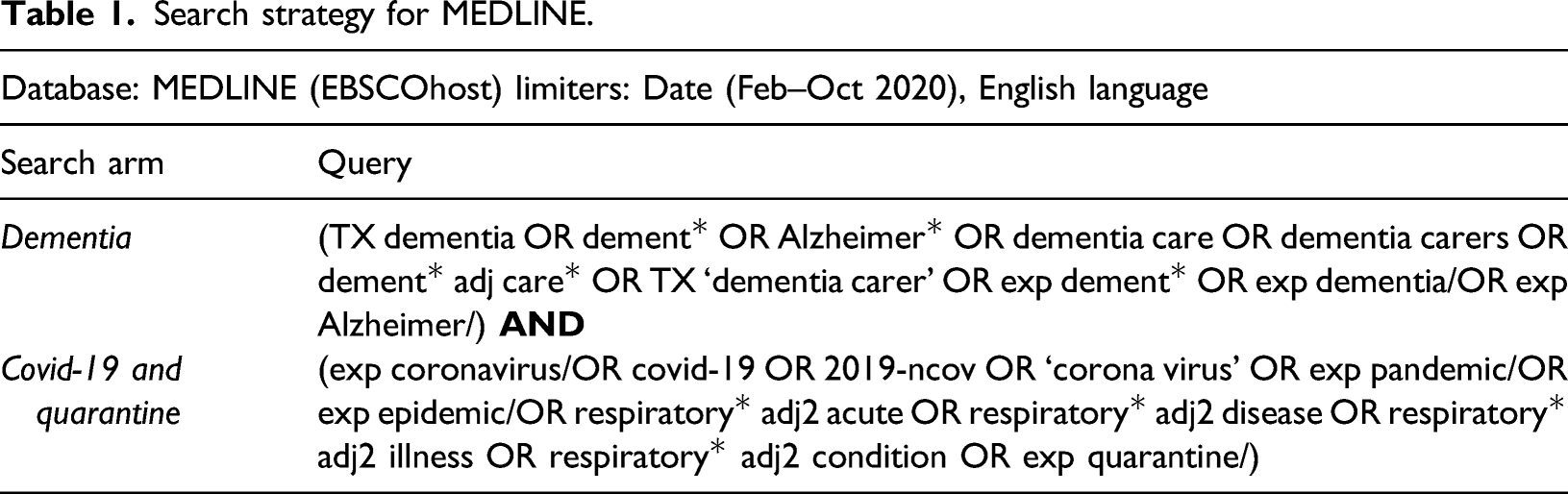
To identify potentially relevant documents, the following databases were searched from February to October 2020: MEDLINE, CINAHL, PsycINFO as well as Google Scholar. Sources of grey literature were searched, for example, clinical trial databases or special registers. (For a complete list of grey literature sources see Supplementary file 1). Reference lists of publications were hand searched for additional articles.
Search strategy for MEDLINE.
The lead author (PMA) and MCA carried out the searches and the review process, which involved two levels of screening: a title and abstract review followed by a full-text review. The research team then met to discuss and review full-text papers that were unclear. See Figure 1 for the PRISMA flow diagram (Centre for Reviews and Dissemination, 2009) that describes the review process. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for the scoping review process.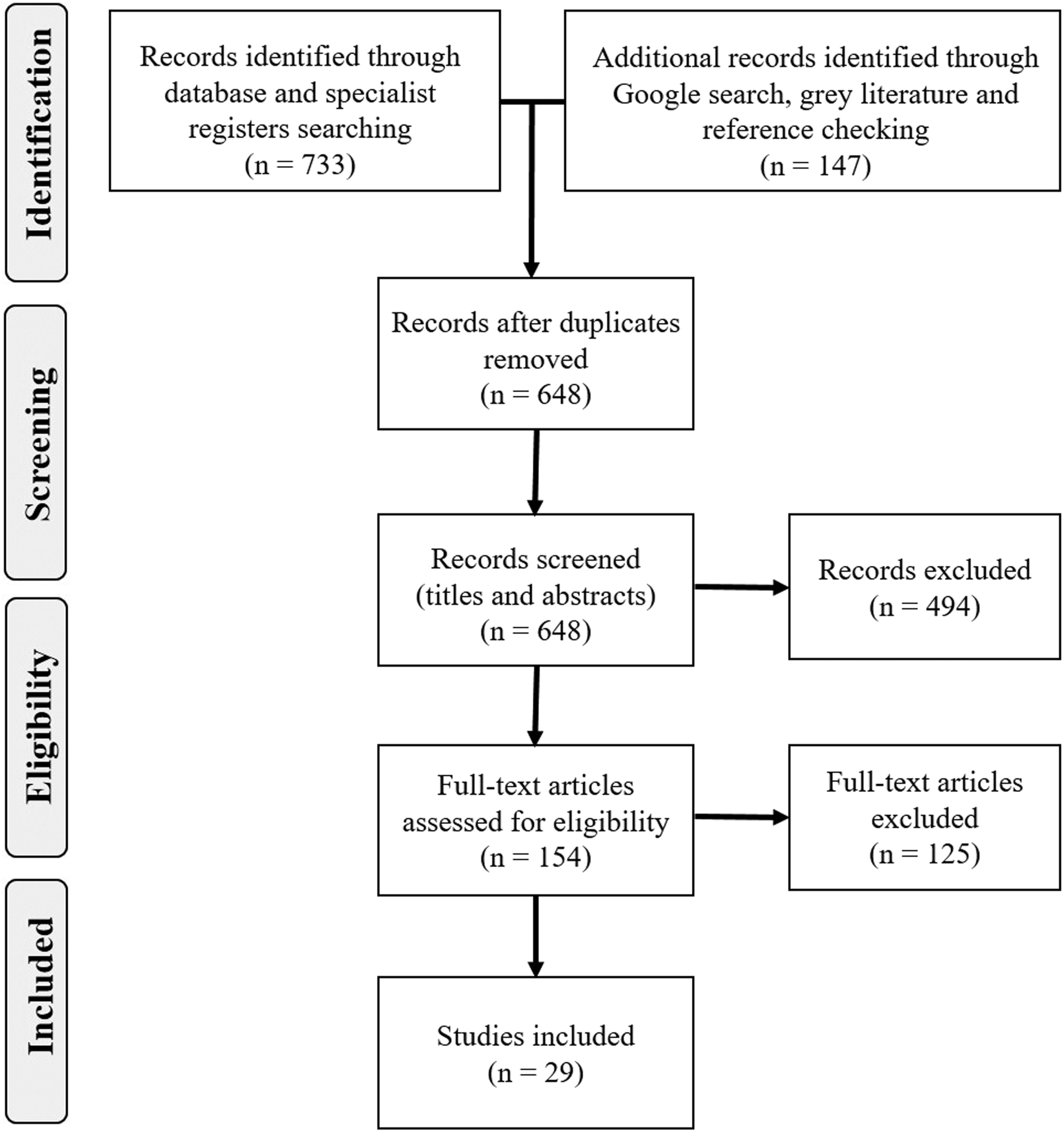
Data charting process
A bespoke template for data extraction was prepared in consultation with all team members. As recommended by the Centre for Reviews and Dissemination (2009), data extraction forms were piloted on a sample that included 10 studies in order to guarantee that the relevant information was captured, and resources were not wasted in extracting irrelevant data. Two reviewers (PMA and MCA) independently extracted the data, discussed the results and iteratively updated the data extraction form. Information was extracted on author, title, country, publication type, aims/purpose of the study, setting/context, sample characteristics (e.g. age, gender, ethnic group, socio-economic status and health), methodology, characteristics of interventions/initiative/support service (if applicable) and key findings. A further check on data extraction from a random 10% sample of the included studies was undertaken by the remaining three team members (GW, MH and NK). No disagreements were identified.
Synthesis of results
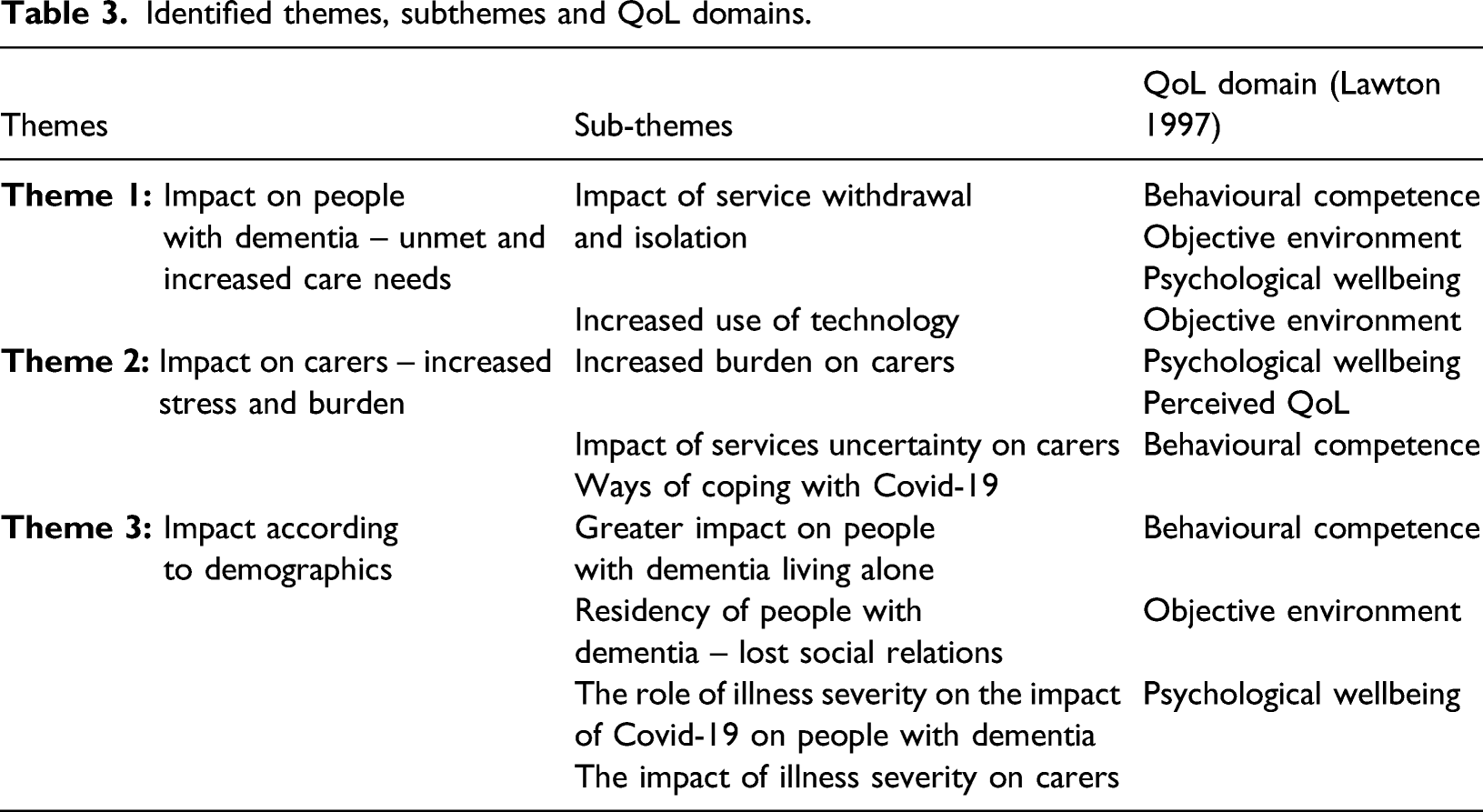
We used Arksey and O’Malley’s (2005) scoping review framework to map key concepts across different studies and to summarize in the form of themes, the main overarching findings, identifying gaps and priorities in the existing literature. Extracted data were categorized according to the review questions and outcomes of interest identified prior to the research but also according to other issues that emerged through the research. Similar categories were combined and organized to highlight key themes. The research team organized regular meetings to review extracted data. An iterative process was followed in order to collectively evaluate, refine and collate all data into categories to develop the final themes. Conflicts regarding the themes, although minimal, were resolved by comparing and discussing different interpretations during regular team meetings. The final themes and sub-themes were mapped onto Lawton’s (1997) four QoL domains: behavioural competence, psychological wellbeing, environmental quality and perceived QoL.
Results
Selection of sources of evidence
A total of 880 studies were identified during the search process. Following the removal of duplicates, this number was reduced to 648. After screening titles and abstracts against the eligibility criteria, 494 were excluded, with 154 full text articles retrieved and assessed for eligibility. Twenty-three studies were excluded because they did not have a clear focus on dementia. One hundred studies were excluded for not reporting on primary research data (e.g. commentaries and opinion pieces). Finally, two studies were excluded because they were not in English. Following this, 29 studies were included (Figure 1).
Characteristics of sources of evidence
Characteristics of all included studies and relevant data extracted (PWD: People with dementia; VD: Vascular dementia; BPSD: Behavioural and psychological symptoms of dementia; AD: Alzheimer’s disease; YOD: Young onset dementia; MDT: Multidisciplinary team).

The studies were conducted in several countries with a majority based in Europe (n=16). Most empirical studies were set within the community (n=18) with participants being people with dementia and/or carers living at home. One study presented data in a hospital setting and another in a care home setting. The remaining studies (n=9) were literature and systematic reviews. Most studies collected demographic data relevant to this review on age (n=17), gender (n=17) and living arrangements of participants (n=12). A small number recorded data on ‘educational attainment’ (n=8), and very few on ethnicity (n=4) or hours of care (n=4). The majority of included studies carried out telephone interviews (n=10) or online surveys (n=7).
Synthesis of results
Identified themes, subthemes and QoL domains.
Theme 1: Impact on people with dementia - unmet and increased care needs
Impact of service withdrawal and isolation
A substantial number of the included studies (n = 11) focussed on the detrimental impact arising from the absence of regular services and isolation for people with dementia. The Covid-19 outbreak and the enforced prolonged conditions of social isolation affect behavioural and psychological symptoms and QoL of people with dementia. Studies reported on negative impacts on cognitive symptoms such as memory (Canevelli et al., 2020; Carpinelli & Lavarone 2020), orientation abilities (Canevelli et al., 2020) and difficulty concentrating (Alzheimer’s Society, 2020) as well as functional decline in terms of reduced level of independence in personal care and housekeeping (Suárez-González, 2020). Nine studies reported a negative impact on apathy, anxiety, agitation/aggression, as well as on depression of people with dementia (Alzheimer’s Society, 2020; Carpinelli & Lavarone, 2020; Canevelli et al., 2020; Cohen et al., 2020a; El Haj et al., 2020; Lara et al., 2020; Manca et al., 2020; Simonetti et al., 2020; Suárez-González, 2020). Two studies also described how the stress from the Covid-19 pandemic and lockdown triggered fear and contagion phobia and other PTSD-like symptoms (Cagnin & Di Lorenzo, 2020; Savla et al., 2020) for which patients with dementia are inherently more vulnerable due to the neuropathology of dementia.
The pandemic has led to a reduction in staff numbers and specialist support for people with dementia (e.g. specialist dementia wards) (including therapists) due to redeployment, sickness and shielding (Royal College of Psychiatry, 2020). This, as hospital leads that took part in the study carried out by the Royal College of Psychiatry (2020) report, has negatively impacted the quality of care for people with dementia, including the discharge process which was often considered to have been rushed, poorly planned or unsafe, hence causing an increase in length of stay of people with dementia.
Increased use of technology
Five studies provide findings on the use and acceptance of novel technologies (e.g. video conferencing, telehealth and TV) as a means to address the needs of people with dementia during periods of confinement (Di Lorito et al., 2020; Suárez-González, 2020; Goodman-Casanova et al., 2020; Lai et al., 2020; Royal College of Psychiatry, 2020). For example, Goodman-Casanova et al. (2020) aimed to explore the effects of a television-based assistive integrated technology (TV-AssistDem) on cognitive stimulation and health status of people with dementia. Although they found no significant differences in QoL outcomes, respondents using TV-AssistDem performed more exercises than those in the control group.
There is limited evidence in relation to the application of novel technologies within clinical settings (e.g. clinical assessment, referrals or reviews) undertaken via phone/video call. Geddes et al. (2020) carried out a review of telemedicine studies in Alzheimer’s disease and cognitive impairment. The authors report that there was no difference in the efficacy comparing in-person diagnosis with diagnosis made via video conference and that this online approach had been shown to be acceptable for carers and people with dementia. They conclude that, in the context of the pandemic and similar future crisis, telemedicine has the potential benefits of enabling access to specialists among patients with reduced mobility and/or geographical constraints and improved patient convenience and comfort.
This review shows that evidence on the use of remote technological adaptations to professional care are still scarce and that these adaptations are underpinned by the need for rapid service transition and, consequently, require further development and evaluation. Remote support and digital technologies need to be ‘fit for purpose’ and supplemented (not replaced) by face-to-face social activities and support services that meet the needs of people with dementia and their carers (Giebel et al., 2020b; TIDE 2020; Vaitheswaran et al., 2020). Importantly, three studies report that not everybody has access or knows how to use ‘technology’ and that age-related perceptual, language and cognitive barriers of people living with dementia must be considered (Geddes et al., 2020; Giebel et al., 2020b; Savla et al., 2020). Patient privacy and confidentiality, risks to quality and continuity of care, and the potentially negative impact of remote care on patient–clinician relationships should all be considered ahead of implementing technology mediated services (Geddes et al., 2020).
Theme 2: Impact on carers – increased stress and burden
Evidence suggests that
during the Covid-19 pandemic carers have experienced higher levels of stress and exhaustion. They have found themselves more isolated and being exposed to critical levels of stress because of having to manage, with little external support, complex circumstances (Alzheimer’s Society, 2020; Cagnin et al., 2020; Canevelli et al. 2020; Cohen et al., 2020a; Savla et al., 2020; TIDE, 2020; Vaitheswaran et al., 2020). Seven studies reported that family members felt that the burden of care and depression-related symptoms had severely increased because of the pandemic (Altieri & Santangelo, 2021; Canevelli et al., 2020; Cohen et al. 2020a; Cohen et al. 2020b; Giebel et al. 2020b; Savla et al., 2020; TIDE, 2020). For example, Cohen et al. (2020a) found that 12% of family members felt ‘the burden’ was severe before the pandemic, noting an increase to 42% during the pandemic. Studies such as the one carried out by the Alzheimer’s Society (2020) report that the pandemic has had a strong negative emotional impact on mental health outcomes for carers (44%) and that emotional outcomes strained their relationship to their relative (42%). Altogether, carers reported struggling to care for themselves and for their relative (22%).
Increased burden on carers
A number of reasons are presented as factors driving the impact on QoL. Firstly, carers have expressed concern about deterioration in the symptoms of the person they care for due to lack of social interaction and cognitive stimulation. This deterioration has, in turn, led to increased complexity of care required by the care receiver and therefore, an increase in care burden (TIDE, 2020). Secondly, carers have found themselves dealing with the difficulties of balancing risk (e.g. whether to go out for a walk; how to get food and medication if you have been told by your GP not to leave your home) (Cagnin et al., 2020; Goodman-Casanova et al., 2020). Thirdly, the lack of services and support for the people with dementia and for themselves has been one of the main sources of concern to carers. Restrictions such as lockdowns have had negative consequences on the possibility of carers being psychologically and emotionally supported by others, leading to social isolation and disconnection from support networks (Altieri & Santangelo 2021). TIDE (2020) report how carers ‘had never felt less visible’ and felt there had been a loss of identity as the media started referring to all health and social care workers as ‘carers’.
Impact of services uncertainty on carers
The uncertainty on what services will look like after the pandemic and on the timing for their re-opening has also been a source of increased worry and distress as has the lack of clarity on the extent and duration of public health restrictions (Giebel et al., 2020b; Giebel et al., 2020c; TIDE, 2020). Many carers found themselves repeatedly trying to explain the distancing and confinement rules to people with dementia, who often struggled to understand (Savla et al., 2020).
Ways of coping with Covid-19
Despite their many challenges, some carers found ways to cope with isolation and other restrictions (Goodman-Casanova et al., 2020; Savla et al., 2020). Carers reported ‘passive’ strategies such as computer games or phone conversations with others and ‘active’ strategies such as going for walks on their own or gardening. All were used to create space for themselves.
Altieri & Santangelo (2021) found that resilience played a role in determining how carers reacted to this crisis. In this study, they compared the impact on levels of depression and anxiety before and after lockdown according to carer’s resilience and found a large effect size. Carers with high resilience reported lower levels of depression and anxiety before the lockdown when compared with carers with low resilience. This study also found that lower levels of resilience and a higher functional dependence of people with dementia predicted higher levels of carer burden during the lockdown. The impact of the pandemic is reported to have been ameliorated by communities demonstrating resourcefulness in striving to continue to support the needs of carers and people with dementia (e.g. delivery of meals and prescriptions, phone calls) (Savla et al., 2020). This support contributed favourably to carers’ ability to continue providing care.
Theme 3: Impact according to demographics
Greater impact on people with dementia living alone
Several studies identified living alone as a significant contributing factor that increases the risk of negative QoL outcomes related to the Covid-19 restrictions (Alzheimer’s Society, 2020; Goodman-Casanova et al., 2020). For example, Goodman-Casanova et al. (2020) report that participants living alone reported being sad and bored, and experienced greater anxiety and more sleeping problems than those sharing a household. A study carried out by the Alzheimer’s Society (2020) found that during the first period of lockdown people with dementia living alone were more likely to report an increase in symptoms such as memory loss and difficulty in reading or writing during lockdown compared to people with dementia living with others. According to their study, people with dementia living alone were least confident going outside during the easing of lockdown rules and were more likely to describe their experience of the pandemic negatively. In fact, 56% of people with dementia living alone stated feeling lonely, compared to 23% for people with dementia living with others.
Residency of people with dementia – lost social relations
There is limited evidence from care home settings, with Suárez-González (2020) suggesting that the ban on care home visits from spouses and partners is causing a significant deterioration in the health of residents with dementia. A study by the Royal College of Psychiatry (2020) reports on the impact of visiting restrictions on QoL outcomes such as increased feelings of isolation and loneliness as well as reduction in the levels of stimulation.
The role of illness severity on the impact of Covid-19 on people with dementia
The severity of the dementia influences the impact of the pandemic on people with dementia. Vaitheswaran et al. (2020) report on how the confinement has exacerbated neuropsychiatric symptoms on patients with low cognitive function, whereas no such symptoms were induced in patients with more preserved cognition. They further report that AD patients with low cognitive function may be more prone to experience confusion and disorientation, exacerbated by reduced social contact and/or reduced physical activity.
Cohen et al. (2020a) report that when comparing the frequency of behavioural symptoms within each dementia group category, anxiety, depression and insomnia were more prevalent in subjects with mild dementia compared to subjects with severe dementia. Cohen et al. (2020a) further explain that one possible explanation for these findings is that comparatively, mild dementia subjects might have suffered a more radical modification in their lifestyle habits during quarantine (e.g. significant reduction in social interactions and physical activity).
The impact of illness severity on carers
Five studies found that psychological outcomes were dependent on the severity of the dementia (Carpinelli-Mazzi et al., 2020; Cohen et al., 2020a; Cohen et al., 2020b; Giebel et al., 2020a; Giebel et al., 2020b). For example, Carpinelli-Mazzi et al. (2020) conclude that higher increase in stress levels in relatives of people with severe dementia are linked to the fear of losing the support from paid carers. This was the case for 42% of participants, who lost the assistance of professional nurses and domestic aids. On the other hand, the stress levels of relatives of people with mild dementia were found to be mainly linked to concern for the risk of Covid-19 transmission and of passing on the disease (Cohen et al., 2020a; Giebel et al., 2020b). Similarly, other studies reported on how carers were put in the position of having to make difficult choices such as discontinuing external caring/support services (and also avoid hospitals or health clinics) because of fear of infection, even in cases of severe dementia, when services are most needed (Cagnin et al., 2020; Giebel et al., 2020a). During the 2020 initial lockdown, these difficult choices were shown to have a direct negative impact on stress-related symptoms in carers of people with severe dementia. A study carried out in Argentina by Cohen et al. (2020b) found that 60% of carers stopped visiting relatives in care homes irrespective of the severity of their illness because of fear of infection. In contrast, only 28.6% of their sample suspended home paid care. They concluded that, overall, the level of burden on the family carer after 4 weeks of quarantine was higher for those with relatives with advanced dementia.
Discussion
This scoping review has explored the impact of Covid-19 on the care and QoL of people with dementia and their family carers. Most of the studies investigated the impact of the enforced isolation and withdrawal of health and social care services during the pandemic and cut across the four domains of Lawton’s (1997) conceptual model of QoL.
People with dementia lost invaluable support offered by health services and community organizations, and family carers lost vital respite support resulting in feelings of abandonment and despair (Dening & Lloyd-Williams, 2020; Giebel et al., 2020a; Wang et al., 2020). Hence psychological wellbeing and ability to function was compromised for people with dementia, with worsening symptoms, behavioural disturbances and adverse psychological consequences. Similarly, for carers, Covid-19 restrictions and accompanying lack of support led to even higher levels of stress and exhaustion, both at a critical point before the pandemic.
Our review echoes what others have reported, that the full impact of Covid-19 is only now emerging. By the time the pandemic is under control, millions of patients living with health problems, including dementia, will have been affected. Millions will have missed vital opportunities to receive initial assessments and diagnosis and necessary treatment (British Medical Association, 2020). In fact, since February 2020, there has been a steady decline in dementia diagnosis rates in England, dropping from 67.6% in February 2020 to 63.2% in July (National Health Service (NHS), 2020). Misdiagnosis of dementia has always been a matter of concern; however, the risk at hand is not having any diagnosis at all. Similarly, the impact of Covid-19 among those who rely on social care, and those working to care for them, is becoming clear. Ironically, by putting a spotlight on the social care sector, Covid-19 has played a vital role in exposing the urgent need for its reform. Although a world pandemic was always likely to cause major disruption, the drastic shut down of routine care is a consequence of over a decade of underinvestment and cuts to services (including public health and social care) and long-lasting structural issues (The Health Foundation, 2020). Without changes to the funding of long-term care and enhanced support for carers, care quality will continue to deteriorate (British Medical Association, 2020; The Health Foundation, 2020; Manthorpe & Iliffe, 2021). Recovery should include the reform of support systems for carers, informed by lessons learnt during the pandemic to mitigate against future crisis situations (Altieri & Santangelo 2021); Boutoleau-Bretonnière et al., 2020; Canevelli et al., 2020; Cohen et al., 2020a; Cohen et al., 2020b; El Haj et al., 2020; Giebel et al., 2020a; Giebel et al., 2020b; Giebel et al., 2020c; Simonetti et al., 2020; Suárez-González, 2020)
Adapting services – a move towards remote service delivery
There is a clear evidence gap on how health and social care services were adapted during the pandemic to meet the needs of people with dementia and their carers. Our findings indicate that further exploration of the effectiveness of internet and technology-based supportive interventions is warranted. Their low cost and potential to reach larger numbers of people compared to face-to-face services make them an attractive alternative. A recent review of RCTs (Leng et al., 2020) found that internet-based supportive interventions are generally effective at ameliorating depressive symptoms, perceived stress, anxiety and self-efficacy in family carers of people with dementia and have potential benefits on care recipients. Technology-mediated services may then be a useful complement to existing services. Similar to studies in the field of cancer (Heynsbergh et al., 2018), our review supports the need for future research to explore the feasibility, usability and acceptability of adapting traditional services to a technology mediated service. This need is particularly severe in the case of studies focussing on people with dementia since most evidence to date has focussed on exploring the feasibility and impact of technology-based interventions on family carers (Killin et al., 2018). Hence, future research should incorporate an understanding of the barriers to access and the personal experiences of people with dementia and their family carers with technology use, considering cognitive decline, age (Hunsaker & Hargittai, 2018) and levels of income and education (Silver, 2014; Gell et al., 2015; Dorsey et al., 2017;). Research should also ensure that online services match the clinical, social, psychological and practical requirements of people with dementia and their carers. Finally, the development of implementation guides that address the level of skill and training required of those delivering these online services would be beneficial.
Review limitations
The search for this review focused on research databases and grey literature sources judged to be the most appropriate for the aim of this review. Some, however, relevant articles and reports may have been missed. There has been a rapid turnaround of research publications as a result of the pandemic, but at the time of this review the amount of published evidence was still relatively limited. It is likely the restrictions placed on society in terms of contact with others, and the pressure of rapid changes to online modes of teaching and undertaking research may have led to delays in the development and publication of Covid-19 related studies. Similarly, the impact of the restrictions may have led to people with dementia and their carers being initially unwilling to take part in studies. As society has begun to adapt to the situation and researchers have adapted to different ways of working, further research not captured in this review is likely to become available. Also, only studies written or translated into English were included in this review because of limited financial resources to translate; relevant studies written in other languages may have been left out.
There was also an overall lack of representation of studies carried out in lower income countries and of diversity in the study populations. Participants were more likely to be white and female, there was no explicit LGBTQ representation, and scarce attention was paid to those with lower socio-economic backgrounds. People living in rural and remote areas where service provision is often limited were not clearly represented. In most of the studies, the data were collected online or via telephone from people already receiving services. Consequently, the impacts reported in this article are likely to be under-estimated.
Conclusion
Evidence from the review suggests overwhelmingly that people with dementia and their carers experience poorer QoL as a result of the Covid-19 pandemic and its associated policy responses. This review has specifically focused on outcomes relating to service withdrawal and its impact on quality of care. The need for clearly articulated policy that seeks to acknowledge and address the vulnerability of people with dementia and their carers to the virus must be extended beyond protectionism and removal of risk and move towards acknowledging and supporting outcomes relating to QoL as well as protection from harm. Our review found that the policies of restricted movement had detrimental impact upon the QoL of people with dementia and their family carers and could be understood as unintended consequences which require further investigation. Crucially, the voices of people with dementia and their carers will be critical in rebuilding and learning from the pandemic, if there is to be a shared effort to develop systems of support for recovery.
Supplemental Material
sj-pdf-1-dem-10.1177_14713012211053971 – Supplemental Material for Exploring the impact of Covid-19 on the care and quality of life of people with dementia and their carers: A scoping review
Supplemental Material, sj-pdf-1-dem-10.1177_14713012211053971 for Exploring the impact of Covid-19 on the care and quality of life of people with dementia and their carers: A scoping review by Patricia Masterson-Algar, Maria Cheshire Allen, Norah Keating, and Gill Windle in Dementia
Supplemental Material
sj-pdf-2-dem-10.1177_14713012211053971 – Supplemental Material for Exploring the impact of Covid-19 on the care and quality of life of people with dementia and their carers: A scoping review
Supplemental Material, sj-pdf-2-dem-10.1177_14713012211053971 for Exploring the impact of Covid-19 on the care and quality of life of people with dementia and their carers: A scoping review by Patricia Masterson-Algar, Maria Cheshire Allen, Norah Keating, and Gill Windle in Dementia
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval is not required for this scoping review study because the methodology of the study only consists of data from articles in public domains.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
![]() to help dementia carers develop skills and take care of themselves.
to help dementia carers develop skills and take care of themselves.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.