
Abstract
Background
Although minority ethnic families have a lower uptake of dementia care services, little research has explored how minority ethnic carers cope with and manage dementia care in their everyday lives. The aim of this study was to investigate organization of family dementia care in Turkish, Pakistani, and Arabic speaking minority ethnic families from the perspective of family carers, primary care dementia coordinators, and multicultural link workers in Denmark.
Methods
Semi-structured qualitative individual and group interviews with minority ethnic family carers, primary care dementia coordinators, and multicultural link workers. Hermeneutic phenomenology was used as theoretical framework and results were analyzed using thematic analysis.
Results
A total of 21 individual and four group interviews were conducted, including a total of 30 participants. A key finding was that the care responsibility was usually shared between several family members, who took turns to provide 24-hour care for the person with dementia. Rotational 24-hour care, either by having the person with dementia live with different family members or by having different family members take turns to move in with the person with dementia, emerged as a common alternative to formal care. Another important finding was that despite decreasing the burden of care of individual family carers, rotational care could be confusing and stressful to the person with dementia and could have a negative impact on the quality of life of all involved.
Conclusion
The way minority ethnic families organize dementia care have implications for understanding and communicating about support needs. Higher reliance on shared family care should not be taken to indicate that minority ethnic communities are not in need of support from formal services.
Introduction
In Denmark, approximately two-thirds of people with dementia are supported in the community, and family carers are the primary source of dementia care (Danish Dementia Research Center, 2018). This is especially true among minority ethnic populations, who are less likely to access public dementia care services (Nielsen et al., 2019; Stevnsborg et al., 2016). Turkish, Pakistani, and Arabic speaking populations represent some of the largest minority ethnic populations in Denmark, and knowledge about dementia care in these communities remain limited.
Most research on dementia care in minority ethnic groups has been conducted in the United States and has mainly focused on Asian, Hispanic, and African American populations (Cooper et al., 2010; Daker-White et al., 2002; Dilworth-Anderson & Gibson, 2002; Janevic & Connell, 2001). In Europe, this line of research is generally a more recent phenomenon and has primarily adopted a service perspective focusing on issues of access and suitability of health and social services, including the attitudes, experiences, and needs of family carers of people with dementia in minority ethnic communities (Baghirathan et al., 2018; Berdai Chaouni & De Donder, 2018; Denktas et al., 2009; Hossain et al., 2018; Johl et al., 2016; Kenning et al., 2017; Mukadam et al., 2011; Nielsen & Waldemar, 2016; Næss & Moen, 2015; Parveen et al., 2017; Sagbakken, Spilker, & Ingebretsen, 2018). Significant variation between minority ethnic communities has been described regarding the motivation to adopt the carer role, the willingness to care, the experience of being a carer, and the use of external support (Parveen et al., 2011). However, generally the literature point at lower service use and higher reliance on family care in Turkish, Pakistani, and Arabic speaking minority ethnic groups compared to European majority ethnic groups.
Despite the growing literature on barriers in access to care and the evidence for a lower uptake of dementia care services, there is very little research exploring how minority ethnic carers cope with and manage dementia care in their everyday lives. Rather than involving formal care services, some studies indicate that minority ethnic families may be more likely to adopt family care patterns in which several family members share the responsibility between them (Boughtwood et al., 2011; Lawrence et al., 2008; Sagbakken, Spilker, & Ingebretsen, 2018). However, little attention has been paid to the organization of these care practices, why they emerge, or the consequences they have for family carers and the person with dementia.
The aim of this study was to investigate organization of family dementia care in Turkish, Pakistani, and Arabic speaking minority ethnic families from the perspective of family carers, primary care dementia coordinators, and multicultural link workers in Denmark.
Setting
In Denmark, free access to medical and social care is available for all legal residents, including in-home services (personal care, homemaking, home nurse, etc.), elderly daycare, and nursing homes. However, there are no public or private dementia services catering to specific minority ethnic groups. As in other western European countries, Turkish, Pakistani, and Arabic speaking migrants form some of the largest minority ethnic groups in Denmark. Out of a total population of 5.8 million people, approximately 9% is of non-Western origin, including about 64,000 people of Turkish, 26,000 of Pakistani, and 150,000 of Arabic speaking origin (www.statistikbanken.dk). Older Turkish and Pakistani immigrant men generally came to Denmark as working migrants in the 1960s and 1970s due to a demand for manual labor and later settled permanently with their wife’s and children through family reunification programs. Older Arabic speaking immigrants came both as working migrants in the same period or as refugees in the 1980s, mainly from countries in the Middle East and North Africa. Despite having lived in Denmark for many years, Danish language proficiency is generally limited among older Turkish, Pakistani, and Arabic speaking immigrants and many have little or no education, especially women. The majority in all immigrant populations are Muslim.
Methods
Design
Semi-structured interviews were conducted by two experienced researchers (TRN, a certified psychologist and PhD; DSN, a registered nurse and PhD) using hermeneutic phenomenology as theoretical framework (Kvale, 1983). Informed by current literature as well as the researchers’ clinical and research experience with minority ethnic groups, an interview guide was developed to provide a frame of reference and guide the process. Topics in the interview guide included the experience and understanding of dementia care, how family carers organized and coped with dementia care, the family carers’ attitude toward dementia care and the person they cared for, the family carers’ attitude toward formal dementia care solutions, how and why family carers sought formal dementia care, and implications of providing dementia care within the family. All interviews were conducted between February and September 2018 at a location chosen by the participant(s) and lasted between 28 and 73 minutes. Interviews with family carers were conducted as individual interviews or group interviews comprising two or three family members, depending on their preferences. All other interviews were conducted as individual interviews.
Participants
Primary care dementia coordinators and multicultural link workers were purposively recruited from urban areas with large minority ethnic populations in Odense and Copenhagen and then by snowballing from those contacts. Primary care dementia coordinators are employed in all Danish municipalities where they organize post-diagnostic dementia care and often act as dementia case managers. They typically have a professional background as occupational therapist, nurse, or nurse assistant with specialist training in dementia. Multicultural link workers are employed in several municipalities with large minority ethnic populations where they provide health education and promotion, information and support groups, and, to a lesser extent, casework and counseling to link minority ethnic communities to Danish health and social services. They come from a range of professional and ethnic backgrounds and have no specific training in dementia. Minority ethnic family carers were recruited from the professional contacts of primary care dementia coordinators.
Inclusion criteria for family carers were: having personal experience with caring for a family member with dementia; and being of Turkish, Pakistani, or Arabic speaking origin. The inclusion criterion for primary care dementia coordinators was: professional experience with minority ethnic older people with dementia. Inclusion criteria for multicultural link workers were: professional or personal experience with minority ethnic older people with dementia; and Turkish, Pakistani, or Arabic speaking background. Turkish, Pakistani, and Arabic speaking was defined as being anyone who identified themselves as having Turkish, Pakistani, or Arabic identity or heritage by links to Turkey, Pakistan, or any Arabic speaking country. Experience was defined as any form of current or previous engagement in supporting or caring for minority ethnic older people. Dementia could be of any subtype.
Demographic information was collected for all participants. Although speaking Danish was not an inclusion criterion, all family carers and multicultural link workers were able to participate in Danish. Recruitment continued until saturation was reached and no new themes emerged from the data.
Data analysis
All interviews were recorded with a digital audio recorder and transcribed verbatim. Transcripts were analyzed using thematic analysis (Braun & Clarke, 2006). This analysis consisted of a comprehensive process of data coding and theme identification following six key stages: (1) familiarization with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report. The thematic analysis was a recursive rather than linear process, in which the authors moved back and forth between the six stages to generate and develop initial codes and identify themes. First, the transcripts were read several times. Then, responses to interview questions along with other themes that emerged at this level were coded and compared across participant categories and ethnic groups. Finally, themes were reviewed and refined in an iterative process and a final coding scheme was agreed by consensus.
Initial coding was undertaken by TRN and researcher triangulation employed via code and interpretation cross-checking by other members of the research group (DSN and GW). The trustworthiness and credibility of the data analysis was further supported by triangulation of sources (i.e. family carers of different genders, educational backgrounds, and relation to the person with dementia; primary care dementia coordinators; and multicultural link workers) and methods (individual and group interviews). Data were stored and organized using NVivo software (QSR International Pty Ltd, v.12, 2018), which also allowed us to develop an audit trail to increase transparency and further substantiate trustworthiness of the analysis.
Ethics
All participants provided written informed consent after reading a participation information sheet and having the opportunity to ask additional questions, following the principles of the European Framework for Research Ethics (European Commission, 2013). The study was approved by the Danish Data Protection Agency (jnl no.: 2012–58-0004) and conducted in accordance with the Helsinki Declaration. Approval by an official ethics committee was not required by Danish law.
Results
Participants and demographics
A total of 21 individual and four group interviews were conducted, including a total of 30 participants. Of these, 26 (87%) were female. Family carers had provided care for a family member with Alzheimer’s disease for 3–15 years; two were spouses, nine children (or children-in-law), and one a grandchild. All people with dementia were first-generation immigrants to Denmark. Among family carers, two had primary education, three short-cycle tertiary education, four Bachelor or equivalent education, and two Master or equivalent education. Primary care dementia coordinators had supported 2–10 minority ethnic older people with dementia within the last year, while multicultural link workers had experience with 1–20 through their professional and personal networks. Demographic characteristics are presented in Table 1.
Participants.
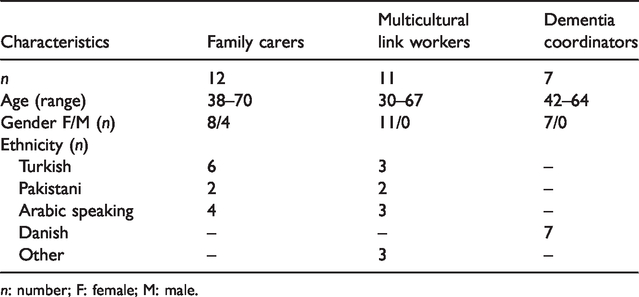
n: number; F: female; M: male.
Themes
The results of the analysis revealed three main themes: (1) organization of family dementia care—rotational care practices; (2) motivation for family dementia care—good children take care of their parents in old age; and (3) consequences of family dementia care—social isolation and dislocation from the community. No patterns in the emergence of themes were found with regard to participant characteristics, and no themes or codes were exclusive to any particular participant category or ethnic group.
Organization of family dementia care—Rotational care practices
The interviews revealed a strong norm for keeping dementia care within the family in the minority ethnic communities. Although different family care models were identified, most participants described models building on cooperation between members of the immediate family sharing the responsibility. When a principal family carer could be identified (often a spouse), interviews generally revealed significant involvement from other family members. However, the most frequently described care model entailed rotating care between different family members by having the person with dementia live with several adult children or by having different family members move in with the person with dementia on a rolling basis: Well, they are kind of alternating in the way that they are staying four weeks in one home and then four weeks in another home, and then the daughter takes over, right. In a way they are nomads […] Some move around and some [children] actually move in with … or take turns to stay with mom or dad, right. (40–49yo Danish female primary care dementia coordinator) I’ve got Mondays, or the weekends if she is alone or … but Mondays are mine. (50–59yo Arabic speaking female multicultural link worker) Although she alternated between all of us, she mainly lived with my older brother and his wife. But she visited us … stayed for a shorter period … well, sometimes she stayed overnight for 14 days or something like that […] and she has also lived with my sister for a while (in Turkey). For almost six months. (40–49yo Turkish female family carer) We have also moved in with her, where the grandchildren have also contributed. For instance, my son moved in … because we did not live far from each other … and stayed overnight with my mom for a year and a half. (40–49yo Pakistani female family carer) Well, there isn’t … there isn’t much help at all. The only thing is that it’s us who have handled it all wrong. (40–49yo Arabic speaking female family carer) There are two things at stake here. One thing is that it’s kind of … kind of more … well, fair that it’s not just one who takes care of them, right. But also … well, towards the community, that the others will not lose face. (50–59yo Turkish female multicultural link worker) It’s kind of a taboo. It’s like … we keep managing on our own and we don’t want outsiders to interfere with our lives. (30–39yo Arabic speaking male family carer)
Motivation for family dementia care—Good children take care of their parents in old age
A common theme across all interviews was that dementia care was very much considered to be a family obligation in minority ethnic communities, especially for the younger generations. On one hand, this obligation was imposed by cultural norms and values, and on the other hand by individual feelings of responsibility based on the relationship with the person with dementia and a belief that the family provides the best care. Often, these aspects overlapped or contradicted in the discourses about the motivation for providing dementia care within the family.
All minority ethnic participants considered notions of reciprocity, or paying back, to be a fundamental cultural value in their community: It is a cultural view that we must take care of our parents. They have given us so much. We must pay them back. (60–70yo Arabic speaking female multicultural link worker) In Islam, it’s a duty of your children to take care of you. (30–39yo Pakistani female multicultural link worker) As a child I am … or rather us children in general, or us sisters … we are better able to take care of our parents because it’s our … this, this responsibility you can’t give to someone else. Not even to someone from our own culture. Even if you are very helpful and so on, you will never be able to treat someone else’s parents as well as you treat your own. (30–39yo Pakistani female multicultural link worker) Well, for me it’s been a huge burden. Because I am forced … I feel forced to do it […] I feel it’s a duty. That I just must do it, because … it’s an expectation. It’s my own expectation and it’s the expectation of my siblings. So, I am part of it. Well, if I don’t contribute they would be burdened. (50–59yo Arabic speaking female multicultural link worker and family carer) It’s kind of a matter of cause that they have been there for you when you were little and now they need you. And if you don’t live up to that as a child, people will point their fingers at you. Well, then you would be labeled as being a bad child. (50–59yo Arabic-speaking female multicultural link worker and family carer)
Consequences of family dementia care—Social isolation and dislocation from the community
The way families organized dementia care helped to preserve a façade of family coping toward the minority ethnic community, while supporting individual family members in maintaining their own family, social, and working lives. However, several participants expressed that rotating care by moving the person with dementia from one child to another could put strain on familial relationships if family members did not agree on their role, or on how to provide care: I haven’t talked to my brother for a while because I don’t think he should yell at my mother. And, and his children shouldn’t say; you know what, we don’t want grandma to be living here. And my sister, she also doesn’t want to visit him because, listen, he did the same when my sister was there. (50–59yo Turkish female family carer) Well, among other things you have to put yourself and your own needs aside. You have to reorganize everything. (30–39yo Pakistani female multicultural link worker) As children we have had to provide a lot for … and that has also affected our, uh, careers and so on, you may say. We have had to put our educations on hold, especially my sister and I. (40–49yo Pakistani female family carer) Well, because it’s a really tough job to live with some with dementia. And these individuals stay at home until they are much more progressed in their dementia (compared to ethnic Danes). If they go to a nursing home at all, it will not be until they are in the very final stage of their dementia. To live with a person who is that severely ill is incredibly hard … and especially if you have to go to work or have young children, or something else. So, I simply think it’s a survival strategy … to say okay, we can manage for one month. Then we rest, and you get the ball. (40–49yo Danish female primary care dementia coordinator) Essentially, I think these individuals often end up having worse lives than I could see them having. Well, they simply don’t get the required care that they need. They are often … you often get the impression that they are becoming somewhat isolated, right. (50–59yo Danish female primary care dementia coordinator) Well, there are some reactions to being moved around. Behavioral disturbances. (50–59yo Danish female primary care dementia coordinator) But it’s a prison. My home has become a prison, because I can’t do anything. (40–49yo Turkish female family carer)
Discussion
This study is the first to consider in more detail the organization of family dementia care in Turkish, Pakistani, and Arabic speaking minority ethnic families in Denmark. As in previous studies in minority ethnic communities in Europe (Baghirathan et al., 2018; Berdai Chaouni & De Donder, 2018; Hossain et al., 2018; Næss & Moen, 2015; Parveen et al., 2017; Sagbakken, Spilker, & Ingebretsen, 2018; Sagbakken, Spilker, & Nielsen, 2018; van Wezel et al., 2016), we found a preference for keeping dementia care within the family with limited support from formal care services but more details about how this was managed by the families.
A key finding of the study was that in most families, several family members shared the care responsibility. Although different care models were identified, rotational 24-hour care—either by having the person with dementia live with different family members or by having different family members take turns to move in with the person with dementia—emerged as a common alternative to formal care. As in other research in Turkish, Pakistani, and Arabic speaking communities (Berdai Chaouni & De Donder, 2018; Hossain et al., 2018; van Wezel et al., 2016), it was evident that children of the person with dementia were central in these care arrangements. However, previous research has not focused on organization of shared family care, despite this care model has been considered when discussing dementia care in Turkish, Pakistani, and Arabic speaking minority ethnic communities (Boughtwood et al., 2011; Lawrence et al., 2008; Sagbakken, Spilker, & Ingebretsen, 2018). The current study illustrates that in some families, 24-hour rotational care of an older family member with moderate or severe dementia was organized between the children according to a more or less fixed schedule, while more ad hoc rotational care practices were also described that could even involve children living in another country. Several factors were found to influence on decisions made about dementia care. On one hand, rotational care practices emerged due to notions of religious duty and shared reciprocity (Nielsen et al., 2018), and on the other hand to alleviate or distribute the burden of care between adult child carers who often had to manage dementia care while juggling multiple other responsibilities related to paid work and childcare. Also, in line with reports from previous research (Baghirathan et al., 2018; Berdai Chaouni & De Donder, 2018; Hossain et al., 2018; van Wezel et al., 2016), many family carers considered formal dementia care culturally inappropriate and/or inadequate due to lacking cultural, language, and religious sensitivity and thus disengaged from mainstream services. As noted in other studies (Baghirathan et al., 2018; Shanley et al., 2012), families would often prefer options that provided them with the flexibility necessary to provide family care for the person with dementia at home (e.g. economic compensation of lost income for the family care provider) or having a home care provider who spoke their language. However, in Denmark, such options are generally not available. The rejection of formal care services further contributed to rotational care practices as these accommodated cultural expectations about children’s obligation to provide care for their parents in a generation brought up in a society and historical time in which women are expected to be part of the labor force. Although similar care models have been described in Spain and Malta (Innes et al., 2011; Rivera et al., 2009), such care arrangements are extremely rare in Denmark, where formal care is generally more accepted and available.
It is important to notice that the attitudes, beliefs, and behaviors of family carers were not uniform but varied within minority ethnic groups. In line with previous research (Boughtwood et al., 2011; Hossain et al., 2018; Rivera et al., 2009), primary care dementia coordinators and multicultural link workers found both socioeconomic status, education, and acculturation to influence decisions about care. Often, families struggled in trying to reconcile multiple values and commitments, such as financial considerations with family and cultural expectations. Adult children with more education were generally perceived to be more informed about and likely to use formal services, especially if the children had an education within health or social care. Another factor that was perceived to influence the attitude toward caregiving was religious beliefs. All family carers in the present study were Muslim, and as described in previous research (Johl et al., 2016), it was clear that holding strong religious values motivated and shaped family carers’ desire to provide care for a family member with dementia. Especially in the case of adult child carers, providing care was seen as the cultural norm and an opportunity to reciprocate parental love and support. Also, all people with dementia and most of the family carers in the present study were first-generation migrants to Denmark, and previous research has revealed that different migration experience, including the age at which the person migrated and the reason for migrating, influence their caring experience (Berdai Chaouni & De Donder, 2018; Johl et al., 2016).
Another important point made by the primary care dementia coordinators was that despite decreasing the burden of care of individual family carers, rotational care could be confusing and stressful to the person with dementia and would often have a negative impact on the quality of life of all involved. Although family carers in the present and previous research often highlight positive aspects of providing care for an older family member, such as feelings of satisfaction, because they are fulfilling their religious and cultural obligations, and the respect and appreciation they get within the family and from the community (Hossain et al., 2018; Parveen et al., 2011; van Wezel et al., 2016), it is also evident that the stress of family care could have a negative impact on family relationships as couples were often unable to spend time together and siblings got into conflicts (Boughtwood et al., 2011; Hossain et al., 2018). Importantly, with progressing dementia and increasing care demands, family carers and the person with dementia would often become increasingly socially isolated as it was difficult to remain involved in activities outside the home (Innes et al., 2011). As described in previous research, often family carers did not find members of the extended family or the minority ethnic community to be supportive (Boughtwood et al., 2011; Hossain et al., 2018; Parveen et al., 2017). These isolating mechanisms were most likely linked to a strong stigma associated with dementia in the minority ethnic communities, which has been found to interfere with the willingness of people with dementia and their families to participate in the community (Berdai Chaouni & De Donder, 2018; Hossain et al., 2018; Johl et al., 2016). In combination with the rejection of formal care services, this contributed to dementia care being dislocated from the community. This is a very important finding considering that caring for a person with dementia exerts huge psychological, physical, and emotional demands and impacts on all family members, including children (Hossain et al., 2018; Lawrence et al., 2008).
Our findings have implications for understanding support needs and for service planning. Currently, people may not access support and care services as they do not fit cultural norms and values about family care or support the adopted care model. Support programs for minority ethnic carers should also target the adult children and include strategies to manage competing values in decision-making and dealing with family disagreement in the context of dementia. As suggested by other researchers (Boughtwood et al., 2011), it is important that service providers are sensitive to different family structures and understand that, both between and within ethnic groups, people may hold different cultural values that will impact on decisions made about dementia care. Services might be considered more acceptable if they could communicate their commitment to respecting individual preferences for care, and to supporting, rather than substituting, family members in their caregiving role (Baghirathan et al., 2018; Lawrence et al., 2008).
Limitations
Limitations of the study include the fact that although we were able to get in-depth information from people with experience with dementia care in three minority ethnic communities in Denmark, this may not be representative of other minority ethnic communities or even all people in those communities, particularly as most participants were females from two larger cities who all spoke Danish. Especially the Arabic speaking minority ethnic group is a large and heterogeneous group, but even in more homogeneous groups, there will be differences among individuals. It is important to notice that although the participants made several general observations, the attitudes, beliefs, and behaviors of family carers were also perceived to vary within the minority ethnic groups. Apart from their cultural background, family carers were perceived to be influenced by factors such as education, acculturation, family background, economic circumstances, religious beliefs, and migration experience.
Conclusion
This qualitative study provides novel knowledge about the organization of dementia care in Turkish, Pakistani, and Arabic speaking families from the perspective and experiences of family carers, primary care dementia coordinators, and multicultural link workers. Rotational 24-hour care practices in which the person with dementia lived with different family members or different family members took turns to move in with the person with dementia were identified as a common care model. This care practice emerged both due to notions of religious duty and shared reciprocity, and to alleviate or distribute the burden of care between adult child carers. A general lack of culturally and linguistically appropriate formal care solutions meant that involvement of formal care would often not be considered until all other options had been tried, especially in the case of nursing homes that would be strongly rejected by most family carers. Although rotational care practices with little or no support from formal care services were described to decrease the burden of care of individual family carers, progressing dementia and increasing care demands would often have a negative impact on the quality of life of all involved.
The study findings highlight that the attitude toward dementia care and the way care is organized by minority ethnic families have implications for understanding and communicating about support needs. Importantly, as noted by others (Sagbakken, Spilker, & Ingebretsen, 2018), lack of service use and higher reliance on shared family care should not be taken to indicate that minority ethnic communities are not in need of support from formal services. However, formal care services may not always be a culturally acceptable solution to the families. Dementia care policy needs to take this into account and consider innovative and pro-active strategies for supporting minority ethnic families in providing the best possible dementia care through appropriate training, support, and liaison. At the same time, more research is needed to explore the specific needs of people from minority ethnic groups with dementia and their family carers, and to develop culturally appropriate interventions to support the families.
Footnotes
Acknowledgements
The authors are grateful to all participants for their valuable contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by THE VELUX FOUNDATIONS (grant number 00017257), which had no role in the formulation of research questions, choice of study design, data collection, data analysis, or decision to publish. The Danish Dementia Research Centre is supported by the Danish Ministry of Health.