
Abstract
Aim
To describe older persons who had commenced a memory assessment, experiences of living with memory impairment and related symptoms.
Background
Persons with subjective memory impairment are two times more likely to develop dementia over the years than their peers. Older persons seldom seek help from primary health care clinics solely for subjective memory impairment. Of those who seek help, it can take up to 35 months from the person experiencing initial symptoms to referral to a memory clinic. Further research is needed regarding how older persons live with memory impairment with related symptoms before they receive a memory diagnosis.
Method
A qualitative study with 23 participants who had commenced a memory assessment in primary care. Semi-structured interviews were held. During the interviews, the Neuropsychiatric Inventory was completed and discussed with the participants. Interview data were analysed using Interpretive Description.
Results
The results are presented under four themes: Conflicting views about the situation, Unveiling the presence of neuropsychiatric symptoms, Compensating with external and internal strategies to recall and Worrying about self and future. Persons with memory impairment were encouraged by family members or others to seek a memory assessment. Few persons were self-referred as memory impairment was often seen as a part of aging. Polarised viewpoints existed within the families regarding the impact of memory impairment on daily life. The presence of neuropsychiatric symptoms appeared unexplored in the participants seeking a memory assessment. In this study, the majority of participants experienced neuropsychiatric symptoms at the time of contact for a memory assessment.
Conclusions
Memory problems experienced were often viewed by the person as being part of an aging process. The presence of neuropsychiatric symptoms was not acknowledged as being connected to memory impairment. Contextualising ‘memory impairment’ as a part of a ‘cognitive process’ may help the person in identifying the presence of neuropsychiatric symptoms.
Background
Dementia is a global public health priority with an estimated 47 million persons living with the syndrome, the number is said to triple by the year 2050. Globally, dementia is ‘under-detected, under-diagnosed, under-disclosed, under-treated and under-managed in primary care (Prince et al., 2016, p. 7).
Alzheimer’s disease [AD] and other dementias are regarded as a major health problem for persons 65 years and older (Hebert et al., 2013). Wilson et al. (2012) refer to the presence of cognitive impairment in older persons which can exist up to 7.5 years prior to the onset of dementia. During the course of AD changes in the person’s self-awareness of memory function occurs (Vannini et al., 2017). According to Roberts and Knopman (2013), an estimated 15% to 20% of persons over 65 years live with mild cognitive impairment and approximately one third progress to develop dementia. Mitchell et al. (2014) state that persons with subjective memory impairment are two times more likely to develop dementia over the years than their peers. In Sweden, many older persons reside independently in their own homes (Wimo et al., 2017) this includes persons with dementia, with up to 50% who live alone (Cermakova et al., 2017).
The majority of persons during the dementia trajectory experience neuropsychiatric symptoms [NPS] (Lyketosa et al., 2011). Symptoms referred to are, for example, delusions, aggression, anxiety and apathy (Cummings et al., 1994). In longitudinal studies following persons over the dementia disease trajectory, NPS were present at baseline increasing (Vik-Mo et al., 2018) significantly and were consistent during the course of the disease (Brodaty et al., 2015). Hill et al. (2018) identified that persons with mild cognitive impairment commonly experience affective symptoms like depression and anxiety.
A timely diagnosis can facilitate advance care planning (National Institute for Health and Care Excellence, 2018), this includes access to support, services, prescribing potential medications and providing information (Porok et al., 2013). Furthermore, a timely diagnosis can help avoid financial exploitation (Manthorpe et al., 2012) and reduce caregiver fatigue (Park et al., 2015) and is regarded as cost effective for society (Prince et al., 2011). The Swedish National Guidelines for Care of Persons with Dementia recommend that persons with suspected memory impairment should be offered a memory assessment within primary health care (National Board of Health and Welfare, 2017). Primary health care is often the first line of contact for persons or families of persons with concerns regarding memory impairment or cognitive decline (Bunn et al., 2012; Galvin & Sadowsky, 2012).
Older persons seldom seek help solely for subjective memory impairment, limited research is available regarding how older persons view their memory difficulties and how they seek assistance (Begum et al., 2012). Persons can view their situation as a possible threat to their autonomy, sense of security and that it affects their meaningful role in society; however, this depends on the person concerned (Steeman et al., 2006). Campbell et al. (2016) studied older persons who sought assistance for memory impairment and described a transition process involving; onset, identifying symptoms, seeking assistance and diagnosis. Daily life for the persons concerned was overshadowed by a sense of uncertainty. It can take an average of 35 months from the person experiencing initial symptoms to referral from primary health care to a memory assessment clinic (Koskas et al., 2018). Lafortune et al. (2015) highlighted a fragmented primary health care service which can create barriers for the older adult to access services. Perry-Young et al. (2018) identified in their study that ‘discounting, misattributing and deferring’ of memory impairment were some of the reasons for persons in delaying seeking contact with health care for memory issues.
Further knowledge is required surrounding older persons experience of living with memory impairment and their needs in a community setting prior to receiving a dementia diagnosis (Parsons et al., 2013). This study was undertaken with a view to expand the knowledge by capturing the experiences of older persons with memory impairment who had commenced a memory assessment.
Aim
To describe older persons who had commenced a memory assessment, experiences of living with memory impairment and related symptoms.
Method
This is a qualitative interview study which aims to gain insights and understandings of a phenomenon from the persons’ who are being interviewed point of view (Kvale & Brinkmann, 2015). In this study, the person’s experiences of living with memory impairment is in focus. An interpretative description [ID] approach as described by Thorne (2016) was used to analyse the interview data in this study. ID is a means of designing a study encompassing the knowledge and conceptual base of the health care discipline of the researcher.
The purpose of ID is threefold: to answer a real-world question, identifying empirical knowledge of the field and awareness of the contextual and conceptual ‘realm’ of the audience. It is a means of engaging with identifiable questions from the applied disciplines of health care departing from ‘self-evident’ knowledge to a more interpretative level of knowledge. It builds on both clinical and evidence-based knowledge and creates an opportunity to identify new insights. These new insights can help shape new practices and inquiries (Thorne, 2016).
This study presents initial interview data of a repeat interview qualitative research study. Interviews were carried out with 23 study participants at their basic memory assessment prior to memory diagnosis. Interviews were held during October 2017 to December 2018.
Sample
A purposeful sampling strategy was used to recruit participants who through their experiences could greatly enhance the study with their contributions (Polit & Beck, 2017). Inclusion criterion for this study were persons over 65 years residing in a community setting, with a Mini Mental State Examination [MMSE] (Folstein et al., 1975) scores over 15 points and who had commenced a memory assessment in primary health care. A total of 31 persons were invited by health care personal at a primary health care clinic to join the study. Eight persons later declined participation in the study mainly due to time restraints. When interviewing began, 23 persons were interested in participation and included in the study (Table 1). Upon receiving confirmation from the primary health care clinic that the participants wished to join the study, contact was taken by the first author (MT) per telephone.
Study participants demographics, MMSE scores and NPS self-reported.
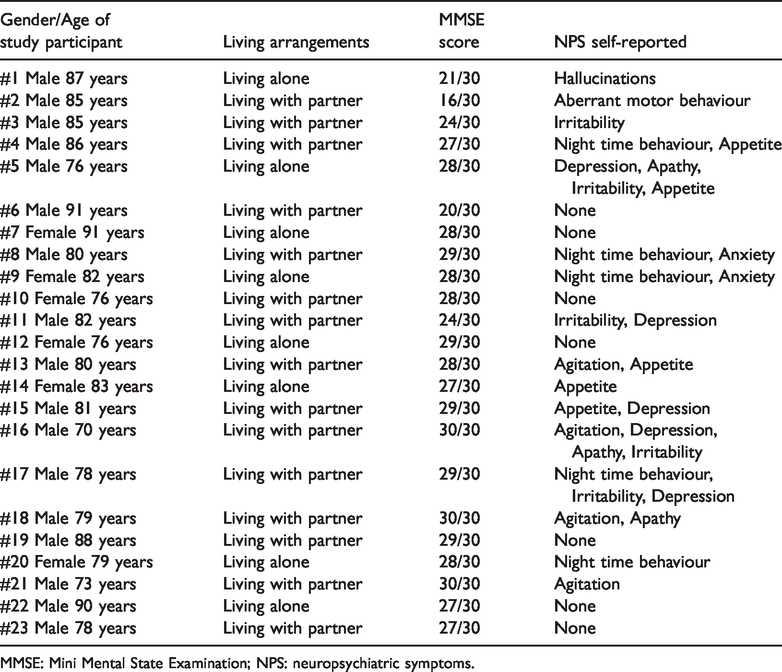
MMSE: Mini Mental State Examination; NPS: neuropsychiatric symptoms.
Data collection
Each participant was contacted by the first author to arrange a convenient time and place for the interview. Interviews were held as per participant’s request; in their home, in the first author’s place of work and in two cases, where the participants were self-employed, in their place of employment.
An interview guide with semi-structured questions was used in this study. Semi-structured questions provide a means for the researcher to cover the topic of interest and allow participants to talk freely about the topic under discussion (Polit & Beck, 2017). Questions included were; what it is like to live with memory impairment, and how does memory impairment affect your life. A question regarding if the participant experienced other symptoms which they thought could be related to memory impairment was posed. The Neuropsychiatric Inventory [NPI] (Cummings et al., 1994) was then presented and completed with the participant. The NPI presents a list of 12 NPS. The 12 symptoms listed in the NPI are hallucinations, delusions, depression, apathy, anxiety, irritability, agitation/aggression, euphoria, disinhibition, aberrant motor behaviour, night time behaviour and appetite. Each NPS in the NPI was discussed with the participants, and upon recognition of the presence of an NPS, it was important to establish that the symptom/s were newly debuted. The Neuropsychiatric Inventory Nursing Home [NPI-NH] version (Cummings et al., 1994) was the NPI instrument of choice in this study. To the authors’ knowledge, the only available NPI instrument, at the time of the study, translated and validated in Swedish. Terms pertaining to a nursing home context in the NPI-NH were excluded in the interview. The NPI-NH facilitates the possibility to report frequency, severity and distress related to the NPS for the person concerned. Questions regarding frequency, severity and distress were posed in the interview when it was deemed relevant for the study participant.
Thorne (2016) states how ‘counting’ and observing prevalence is a common way to interpret the world and although the use of numbers is not the mainstay of qualitative research, it can however enhance the transformation of data to results. ID as an approach facilitates the use of various methods of data collection as long as they are aligned with the research focus and the ‘disciplinary knowledge objectives’ (Thorne, 2016). In this study, the inclusion of the NPI helped the study participants to identify the possible presence of NPS (Table 1).
The duration of each interview ranged from 30 to 75 minutes. Upon receiving permission from the participants, 19 of the interviews were audio-recorded, on a code lock audio device, by the first author. Notes were taken during all interviews, and the interviews were transcribed by the first author, directly after each interview.
Data analysis
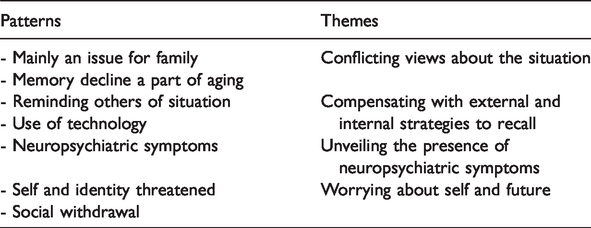
Using an ID approach, the data analysis process was initiated and led by the first author who read through the transcribed interviews several times, and relationships between texts were identified forming patterns. Thorne (2016) describes the importance of testing relationships among data to assist the emerging analysis. The first author then clustered the patterns which developed and formed common themes (Table 2). Academic discussions, regarding initial patterns and themes, were held with the research team. Thorne (2016) warns about the risk of over-estimating patterns and the importance of the researcher to hold a critical approach to frequency of topics in the text. In attempts to avoid ‘premature closure’ (Thorne, 2016, p. 194), initial patterns and themes were reassessed and discussed by the research team several times prior to agreement on final patterns and themes.
Examples of patterns from the data analysis presented as themes.
Ethical considerations
This study was approved by the Regional Ethical Review Board. All participants received written and verbal information about the study during the recruitment process. Participants were informed that their participation was voluntary and were reminded that they could at any point of time opt to withdraw from the study without consequences. Informed consent was gained from the participants in accordance with the Declaration of Helsinki (World Medical Association Declaration of Helsinki, 2013) which includes that the rights and interests of the study participants must take precedence over the goal of the research.
Results
The results are presented under four themes: Conflicting views about the situation, Unveiling the presence of NPS, Compensating with external and internal strategies to recall and Worrying about self and future.
Conflicting views about the situation
Study participants described their own perspective of living with memory impairment and that of others (family, peers and physicians). Participants highlighted how polarised standpoints existed in their families regarding the presence and impact of memory impairment. For participants, concerns about memory impairment had faded in significance in comparison to other aspects of life and general well-being. Family members were portrayed as having contrasting views focusing on the impact memory impairment had on relationships and daily life.
Study participants viewed their memory impairment as part of an aging process which was toned down as having little to no impact on their life. Memory impairment was rationalised as the result of wear and tear on the body due to biological aging. I have started to understand that I need to get used to living like this, prepare myself for forgetting things, in a way I think when you have turned 81 and have worked your entire bloody life, it’s ok to be forgetful. My partner is constantly nagging me that I have forgotten things, I know I forget things … it’s my partner that is mostly affected, she says don’t tell me you have forgotten it … no you cannot have forgotten it, and of course I have [embarrassing laugh] Over the last six months my wife has been telling me that I have forgotten this and have forgotten that, but I can’t remember everything she does, I mean we are two different people what I deem important, I can recall. I met some old work-mates … we talked away and then I forgot what we were discussing, so they said to me … you should get your memory checked out … I mean it can be so bad that you have actually developed memory loss. First of all, it wasn’t me who wanted this [memory assessment], they contacted me. Out of the blue I got a letter from them [primary health care], I thought it was ok and accepted the offer … I was told that my [memory test] results were very good. They didn’t think that I needed to go any further … This surprised me somewhat as I would say it was a harmless memory assessment … can you fold this piece of paper in the centre and so … [laugh].
Unveiling the presence of neuropsychiatric symptoms
Exploring if study participants had developed other symptoms parallel to developing memory impairment was not an easy task. Participants had great difficulties in spontaneously identifying potential associated symptoms. Memory impairment was the ‘mother symptom’ with consequences such as forgetfulness and disorientation viewed as sub-symptoms. Of those participants who had developed physical symptoms, such as headaches and back pain, these symptoms were tangible and easier to identify and discuss.
When discussing the possible presence of NPS associated with memory impairment, study participants appeared both perplexed and curious. Perplexed, surrounding the possibility that memory impairment could be associated with other symptoms, which were latent and could now be revealed and were not part of the aging process. At the same time, a sense of curiosity and eagerness existed to hear about potential symptoms which were unexplored and undetected. When the list of NPS from the NPI was presented, recognition and confirmation of certain symptoms, which had not been discussed earlier, was shared by the majority of the participants despite variations in MMSE scores. I don’t think that I have any other symptoms … [read NPI list] I think I have become more aggressive, if that has something to do with memory problems I don’t know … I take very little initiative [these days] … it is often my wife who is the driving force, I would prefer to stay at home.
Mentioning certain symptoms listed in the NPI (Cummings et al., 1994) such as hallucinations, disinhibition, euphoria and delusions appeared amusing for some participants who responded with outbursts of laughter and humorous comments. For them, the initial thoughts of developing such symptoms were absurd and beyond belief as they represented a loss of self-control and ability to regulate. I don’t experience delusions [laugh] however I have problems with others who have. e.g. like politicians … I don’t have depression instead I have a straight line which I would like to think that one day would curve upwards to a bit of euphoria … I only experience euphoria when I go to the theatre.
Compensating with external and internal strategies to recall
Managing daily life alongside expectations from self and others in the face of memory impairment required strategies. Strategies were created and adapted by participants to maximise performance and compensate for memory impairment. Internal and external strategies were described. Internal strategies involved using themselves as a tool and external strategies involved the use of physical memory tools.
Documentation was a common external strategy used. To document upcoming events, appointments, etc. in an accessible diary or a calendar had become an essential part of life and helped maintain a sense of structure and normality. Technology was another external strategy commonly used, mobile phones were mentioned as valuable sources of help to keep track of time and recall words or events. I try to systemise my life, but it doesn’t always work [laugh] … I carry a diary in which I have all sorts of things documented [shows and opens the diary] I can’t say that I need to apologise for myself, I have accepted what has happened. I have my son, he is my external memory … If it continues like this, then I am ok with it. … emmm my wife has a plant by the window, to remember the name of the plant, I need to go on a detour with words and think, if I am able to [‘orkar’] water the plant, I get ‘orkar’, then I can retrieve the name orchid [‘orkidéér’]. A direct connection to the word doesn’t exist for me It’s like this, I have to remind people around me that I forget!
Worrying about self and future
Memory impairment entailed losses and feelings of vulnerability in the face of an uncertain future. The term ‘memory impairment’ was a synonym for cognitive impairment. It was not an isolated cognitive symptom, it came hand in hand with impairments of thought processing and intellectual functions. Thoughts and worries regarding a progressive cognitive decline impacted on how participants viewed themselves and what the future held.
Deficits in a cognitive domain such as memory was observed by peers and threatened their sense of self and identity impacting on personal and social relationships. This resulted in participants feeling less relied upon and trusted by family and peers. This was a cause of concern and worry, as trust and reliability were attributes which had been valued and were symbolic of them as a person. [my wife] now regards me as unreliable when she asks me to do things. My former workmates have received information that I have received a ‘blow’ and that I’m the same person I was before, I think that I was good fun back then, I’m not so today … my girlfriend thinks that I can hold a good conversation. Getting involved in politics again is not on the agenda due to my memory problems … I am still president of our resident’s association. I don’t want this to get any worse so that I end up disappearing into the mist … that’s why I need to suss out in advance what’s going on up there in the brain department!
Discussion
The main findings in this study highlight how participants with memory impairment viewed their situation as a part of an aging process. This is confirmed by Beard and Neary (2013) who described how older persons did not always view memory problems as a pathological development. Participants in this study explained how their memory impairment was problematised by family members placing strains on family life. Most of the participants were encouraged by others to seek a memory assessment, and few participants were self-referred to their primary health care. This is in keeping with a study carried out by Perry-Young et al. (2018) who identified that ‘discounting, misattributing and deferring’ of memory impairment were some of the reasons for persons in delaying seeking contact with health care for memory issues (p. 11). Fears of stigma and social isolation (Phillipson et al., 2015) are other reasons why persons refrain from contacting health care for subjective memory impairment. Furthermore, lack of insight and initiative taking can be viewed as early symptoms in dementia. These symptoms are included in the cognitive domains; social cognition and executive function, which can be affected in both mild and major neurocognitive disorder according to the Diagnostic and Statistical Manual of Mental Disorders fifth edition [DSM-5] (American Psychiatric Association, 2013). Self-awareness of cognitive impairment varies in the early stages of AD according to Hill et al. (2016). Clare (2003) in a seminal study identified how persons with AD processed self-awareness of perceived difficulties related to their disease. Processes were divided up into two domains: self-maintaining and self-adjusting. In this study, participants described how they compensated for memory impairment, normalising and minimalising impact on their lives prior to memory diagnosis which according to Clare (2003) are themes seen in self-maintaining.
Further findings in this study highlight that participants seeking a memory assessment were unaware of the presence of NPS. Prior to the introduction of NPI, participants had difficulties in identifying possible co-related symptoms to memory impairment. The majority of participants identified, with the help of the NPI (Cummings et al., 1994), that they experienced one or more NPS. NPS identified were new symptoms which had gradually developed over time and were not overtly associated with memory impairment. It was often the first time the participants had identified and spoken about these symptoms. To the authors’ knowledge, the NPI is not used in primary care or in specialist memory clinics for persons seeking memory assessments. Borsje et al. (2019) describe how community residing persons with dementia are living with high levels of NPS. According to Karttunen et al. (2011), approximately 80% of persons, in the very early stages of AD, reported the presence of NPS. Borsje et al. (2019) highlight the need for primary care to investigate the presence and follow-up NPS in persons with dementia. Hill et al. (2018) described the impact memory impairment had on persons with mild cognitive impairment, it varied from frustration to social withdrawal depending on the meaning placed on the experienced deficits. One participant in this study reluctantly reported the presence of hallucinations which was not openly discussed before, and other participants reported NPS such as agitation/aggression and irritability which appeared directly related to frustration surrounding memory impairment. Loss of appetite was reported by some participants. The Swedish Dementia Registry annual report (SveDem, 2017) identified that one third of persons with dementia are undernourished with a body mass index of under 22. Examples of other NPS reported in this study were depression and anxiety. Hill et al. (2016) describe how subjective memory impairment is associated with depressive and anxiety symptoms.
Keady and Jones (2010) described, in their case study, the significance of using a person-centred approach in understanding why a person with dementia exhibited NPS in a nursing care facility. This study shows how older persons prior to a cognitive diagnosis were living with NPS in a community setting. The use of the NPI helped highlight the presence of NPS which otherwise could go undetected during the memory assessment. Using a person-centred approach in primary care and completion of the NPI can assist in the identification of NPS and provision of follow-up care and support.
In this study, the term memory impairment was not contextualised, for the participant, as one of several cognitive processes influencing behaviour and emotions. Such explanation may have helped the participant identify previously undetected cognitive symptoms and NPS. In an international multi-centre study, Rabin et al. (2015) identified that memory was the most common cognitive domain investigated in older persons experiencing subjective cognitive decline. Reisberg and Gauthier (2008) discuss how subjective cognitive impairment is commonly known as subjective memory complaint. However, they recommend the use of the term cognitive decline as opposed to the term memory impairment due to the complexity of the field and by saying cognitive decline it is not limited to memory alone.
According to Morgan et al. (2014) family members encouraged contact with a memory clinic to gain validation about symptoms experienced and to receive a diagnosis for future planning. In the event the person received a dementia diagnosis, it facilitated an understanding of their situation; furthermore, a diagnosis helped the person with memory impairment to accept their situation (Morgan et al., 2014). One participant explained how he received an invite to commence a memory assessment, the participant speculated that it was part of a routine health check and accepted the offer. To systematically offer memory assessments to persons over a certain age may influence the number of referrals and help identify persons at risk of developing dementia or cognitive impairment.
Receiving an early dementia diagnosis can assist the person in planning future care with focus on interventions and support (National Institute for Health and Care Excellence, 2018; Porok et al., 2013). However, treating physicians are sometimes reluctant in setting a dementia diagnosis due to concerns of the potential stigmatisation (Gove et al., 2016) and in the absence of available interventions and social support (Smith et al., 2017). This may further delay the process of diagnosing dementia for the persons concerned. It is a process for the person themselves to recognise if symptoms experienced warrant a medical investigation or not. According to Steeman et al. (2006) in the pre-diagnostic phase, persons can fluctuate between both awareness and denial which can exist simultaneously. Not all of the participants in this study were eligible to continue a memory assessment after the initial visit to their primary health care. The participants concerned scored full marks on the basic cognitive screening, and during the initial assessment, the treating physician evaluated that there was no need to proceed with a memory assessment. These two participants were high-functioning individuals and were surprised how standardised and basic the testing was. Both study participants reported the presence of NPS when completing the NPI. According to National Institute for Health and Clinical Excellence (2018), the risk of developing dementia can exist in persons with normal scores in cognitive testing. Not confirming the person’s worries about subjective cognitive concerns leaves the situation unresolved and the person is left in an ambiguous position (Birt et al., 2019). Cognitive testing offered in primary health care includes the completion of the MMSE (Folstein et al., 1975), which according to Breton et al. (2019), has lower sensitivity than other cognitive screening instruments.
Limitations in this study were that participants were recruited from one primary health care clinic in a city in Sweden. No data were gathered about the participants’ level of education; despite this, many of the participants appeared to have university-level education.
Conclusion
Memory problems experienced were often viewed by the person as being part of an aging process. The presence of NPS was not acknowledged as being connected to memory impairment. Contextualising ‘memory impairment’ as a part of a ‘cognitive process’ may help the person in identifying the presence of NPS.
Implications for practice
Older persons may view their memory impairment as part of an aging process and therefore not see the need to seek a memory assessment. Primary care should be aware that screening for NPS as part of a memory assessment can help identify the presence of symptoms which otherwise can remain undetected and unmanaged for the person concerned.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding received are for both studies. The two studies were funded by the Sophiahemmet Foundation and author Dorota Religa was supported by grants provided by Region Stockholm (ALF project) and Swedish Research Council (Drn 2012–2291).