
Abstract
Family caregiving is considered a social transition as changes in the health of the care recipient create a process of transition for the caregiver when they are more vulnerable to threats to their own health. Family and friend caregivers take on many responsibilities and experience high levels of burden when caring for community-dwelling older adults living with dementia and multiple chronic conditions. However, little is known about the changes they experience in their caring roles or how they cope with these changes. This qualitative descriptive study was part of a larger mixed methods randomized controlled trial evaluating a web-based caregiver support toolkit. Multiple semi-structured phone interviews were conducted with caregivers of older adults with dementia and multiple chronic conditions. Content analysis was used to generate thematic descriptions. Six themes were generated and grouped into two categories. Significant changes experienced by caregivers are described by the following themes: ‘everything falls on you – all of the responsibilities,’ ‘too many feelings’ and ‘no time for me.’ The themes describing how caregivers coped with these changes include: seeking support, self-caring, and adapting their caregiving approach. Study results indicate that caregivers of older adults with dementia and multiple chronic conditions experienced many changes in their caregiving journey resulting in increasing complexity as they tended to the care recipients’ declining health and well-being. These caregivers used several creative strategies to cope with these changes. Health care providers should consider both the caregiver and care recipient as clients in the circle of care, and facilitate their linkage with health and community support services to help address the increasing complexity of care needs.
Introduction and background
Over 47 million individuals worldwide are living with dementia and this number is expected to increase to 75 million by 2030 (World Health Organization (WHO), 2017). Dementia has a profound physical, mental, and social effect on persons with dementia and their caregivers (WHO, 2017). Additionally, older adults with dementia have a high prevalence of multiple chronic conditions (MCC); (Koroukian, Schiltz, Warner, Stange, & Smyth, 2017). Living with MCC (commonly defined as two or more chronic conditions) is associated with increased risk of mortality, disability, and poor quality of life, compared to having a single condition (Fried et al., 2014; Ploeg et al., 2018; Prince et al., 2015; Salive, 2013). Older adults with dementia and MCC are heavily reliant on family caregivers for support and care (Giovannetti et al., 2010; WHO, 2017). Family caregiving is considered a social transition, whereby changes in the health of the person with dementia create a process of transition for the caregiver during which time they are more vulnerable to risks, such as caregiver distress (Meleis, Sawyer, Im, Hilfinger Messias, & Schumacher, 2000; Peacock et al., 2017). Transitions are ‘both a result of and result in change in lives, health, relationships and environments.’ (Meleis et al., 2000, p. 13). How caregivers cope with transitions in their caregiving journey or manage the challenges of MCC in the context of dementia is not well understood (Bunn et al., 2014).
Some qualitative research has explored the experiences of caregivers supporting older adults with MCC. An interpretive description study reported family caregivers found managing the care of older adults with MCC ‘overwhelming, draining and complicated’ (Ploeg et al., 2017, p. 7). These caregivers provided emotional support, cognitive stimulation, social outings, and personal care (Ploeg et al., 2017). Another interpretive description study reported that spousal caregivers were particularly challenged if they could not leave the care recipient alone or met unwelcoming social attitudes towards the care recipient (Peacock et al., 2017). These caregivers used strategies such as taking time for themselves and staying socially connected as means to cope with caregiving demands (Peacock et al., 2017). A longitudinal study of caregivers of older adults with MCC described caregiving as a trajectory requiring learning and accepting help in later phases (Williams et al., 2016). Gill et al. (2014) explored caregivers’ frustrations with the health care system and found caregivers struggled to make health care decisions on behalf of the older adult with MCC.
To our knowledge, only three qualitative research studies have been conducted regarding the experiences of caregivers of persons with dementia and only one other chronic condition. Bunn et al. (2017) discovered that caregivers not only had to advocate for access to health care but they also had to coordinate the delivery of that care. Feil, Lukman, Simon, Walston, and Vickrey (2011) revealed the main challenges for caregivers in managing diabetes in persons with dementia were taking over medication administration and snack and meal provision especially when the care recipient would not acknowledge having diabetes. Sanders and Powers’ (2009) reported that older husband caregivers took on a ‘protector’ role of their wives’ personhood, providing personal care, planning activities and socialization, and performing more household duties.
Despite the growing number of older adults with dementia and MCC and the potential negative health and social outcomes for these older adults and their caregivers, little is known about the transition experiences of these family caregivers. An understanding of these unique experiences and coping is essential to plan and deliver health and social care for this population of older adults and caregivers. The purpose of this paper is to describe the significant changes in the caregiving journey experienced by family caregivers of persons with dementia and MCC living in the community and how they cope with these changes. This paper reports on the qualitative findings of the following research questions: (1) What are the significant changes experienced by caregivers of persons with dementia and MCC? and (2) How do caregivers cope with these significant changes?
Methods
Study design
This study was part of a multi-site pragmatic mixed methods randomized controlled trial (Duggleby et al., 2017). The purpose of the larger study was to evaluate the impact of using a web-based caregiver support toolkit (known as My Tools 4 Care) on the quality of life, hope, and self-efficacy of caregivers of persons with dementia and MCC compared to an educational control group (Duggleby et al., 2018; Ploeg et al., 2018).
A qualitative descriptive method was used as its grounding in naturalistic inquiry facilitated the description of caregivers’ experiences as close as possible to what was shared (Sandelowski, 2000, 2010). Qualitative description was a complementary method to the larger, mixed methods study due to its ability to capture participants’ experiences related to caregiving (Neergaard, Olesen, Andersen, & Sondergaard, 2009). Qualitative description produces a ‘comprehensive summary of an event in the everyday terms of those events’ (Sandelowski, 2000, p. 336).
Sample
The inclusion criteria for caregivers for the larger study were: (a) family member or friend who was providing physical, emotional and/or financial care to an older adult (≥65 years of age) living at home with dementia and two or more other chronic conditions; (b) English speaking; (c) ≥18 years of age; and (d) access to a computer with an active email address. Participants were primarily recruited through local Alzheimer Societies. Maximum variation sampling was used to obtain a purposeful sample of male and female caregivers with different relationships to the care recipient (i.e., spouse, child). Of the 199 caregivers who participated in the larger trial, 72 caregivers from both the intervention (n = 36) and control groups (n = 36) agreed to be interviewed for the qualitative strand of the mixed methods study.
Data collection
Data collectors were health care providers with experience in qualitative interviewing. An interview guide was used based on a literature review and expert input from the research team. Semi-structured phone interviews were conducted from June 2015 to April 2017 at one month (intervention group only to discuss initial experiences with the web-based toolkit) and again at three months and six months (both groups) after enrolment in the larger study. Interview questions posed were: ‘Describe any significant changes you experienced as a caregiver in the past 3 months’; and ‘In the past 3 months did you do something to help you deal with the significant changes you experience as a caregiver?’ These interviews, lasting between 20 and 40 minutes, were digitally recorded and transcribed by a professional transcriptionist, bound by a confidentiality agreement. A research assistant checked the accuracy of the transcripts.
Data analysis
Data analysis occurred concurrently with data collection. A four-member subgroup of the research team undertook the qualitative content analysis, a strategy consistent with qualitative description (Sandelowski, 2000, 2010). The researchers used conventional content analysis whereby they independently read each transcript, took note of impressions and thoughts, and labelled parts with codes, often using in vivo codes (i.e., codes derived directly from the data) rather than preconceived categories (Hsieh & Shannon, 2005; Saldaña, 2016). The members then discussed, reviewed, and revised the emerging codes in a dynamic and iterative process. To answer the research questions, particular attention was paid to how caregivers described what had changed and how they coped with these changes. The researchers continued to group and re-group codes, culminating in the development of themes (Hsieh & Shannon, 2005). Poetic reconstruction, arranging the in vivo codes from a number of participants together in a ‘found poem’, was another means used to develop and convey the themes (Saldaña, 2016, p. 109). Found poems are an effective analytical tool in qualitative description to synthesize data and describe the essence of an experience (Saldaña, 2016). The research team collectively decided to complete data collection when it was determined that the themes were supported by the on-going interviews, evidence that saturation had occurred (Neergaard et al., 2009).
Trustworthiness of the data
Multiple strategies to enhance rigor were used, including: purposeful sampling of a large and diverse group of caregivers; repeated interviews to earn participants’ trust and to elicit details of the caregiving experience over a period of time; data collectors’ participation in data analysis to provide insights into the context of the interviews; frequent team meetings; maintenance of a coding journal as an audit trail of analytical decisions; and commitment to production of themes as close to the data as possible (Neergaard et al., 2009; Tong, Sainsbury, & Craig, 2007).
Ethics
The study was conducted in accordance with the Tri-Council Policy Statement, Ethical Conduct for Research Involving Humans (Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, & Social Sciences and Humanities Research Council of Canada, 2010). Institutional ethics approval was obtained from the Hamilton Integrated Research Ethics Board (#15–309) and the University of Alberta Health Research Ethics Board (#Pro00048721). Informed consent was obtained by data collectors by telephone and a copy of the consent form was emailed to participants.
Findings
Characteristics of the sample
Seventy-two caregivers participated in a total of 135 qualitative interviews (35 at one month, 65 at 3 months, and 35 at 6 months). Reasons for not completing interviews included: care recipient death or move to long-term care. Most caregivers were female (80.6%), a partner (52.8%) or child (43.0%) of the person with dementia and MCC, and living with the care recipient (80.6%). The caregivers were aged 64.3 years on average (range: 22–91) with a mean of 1.5 chronic conditions (range: 0–8). Care recipients were an average of 80.5 years and had a mean of 10 chronic conditions (range 3–20 in addition to dementia). The most commonly reported chronic conditions of the care recipients were: incontinence, hypertension, and arthritis. Refer to Table 1 for a summary of the characteristics of the caregivers and care recipients.
Demographic characteristics of caregivers and care recipients.
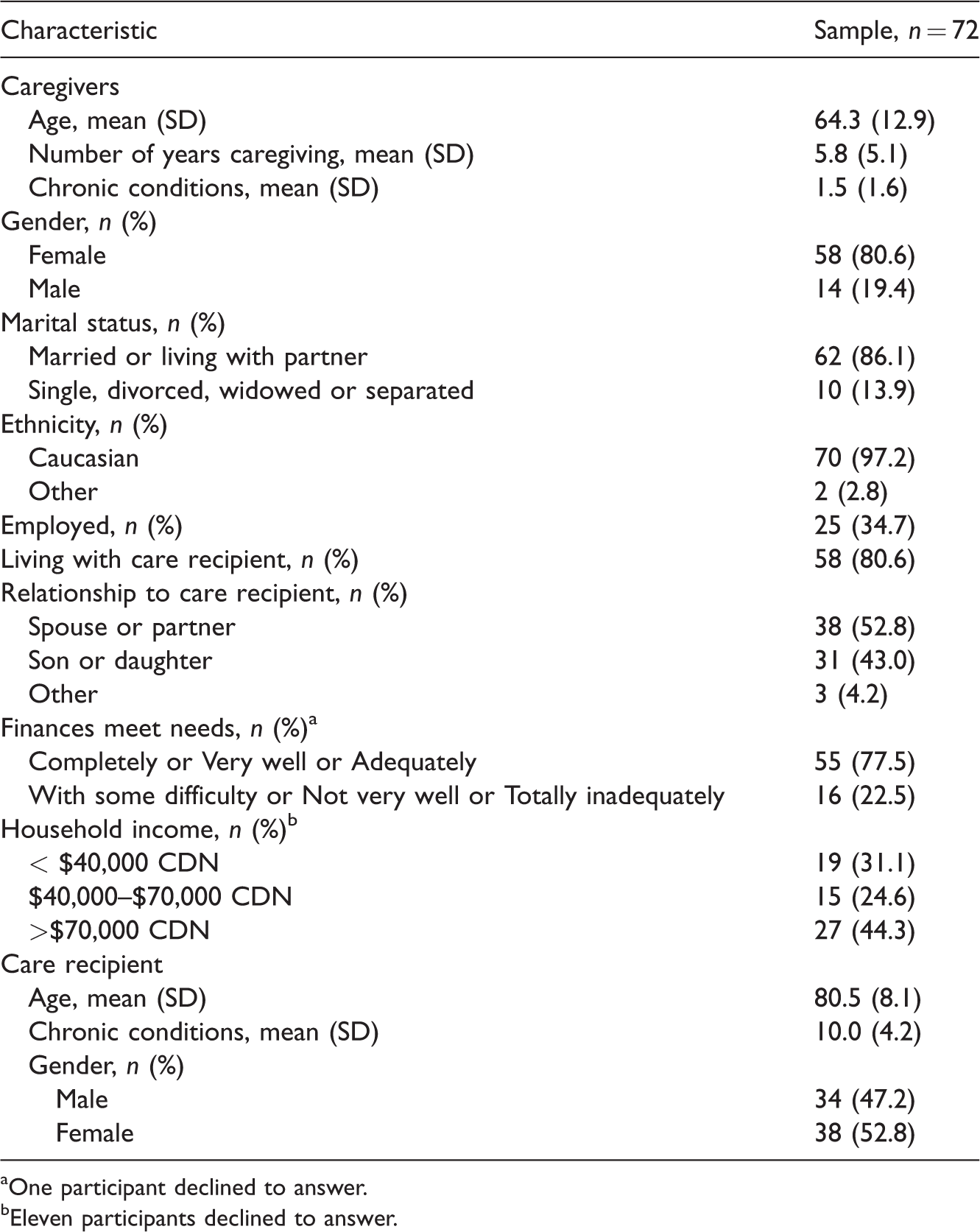
One participant declined to answer.
Eleven participants declined to answer.
Overview of the findings
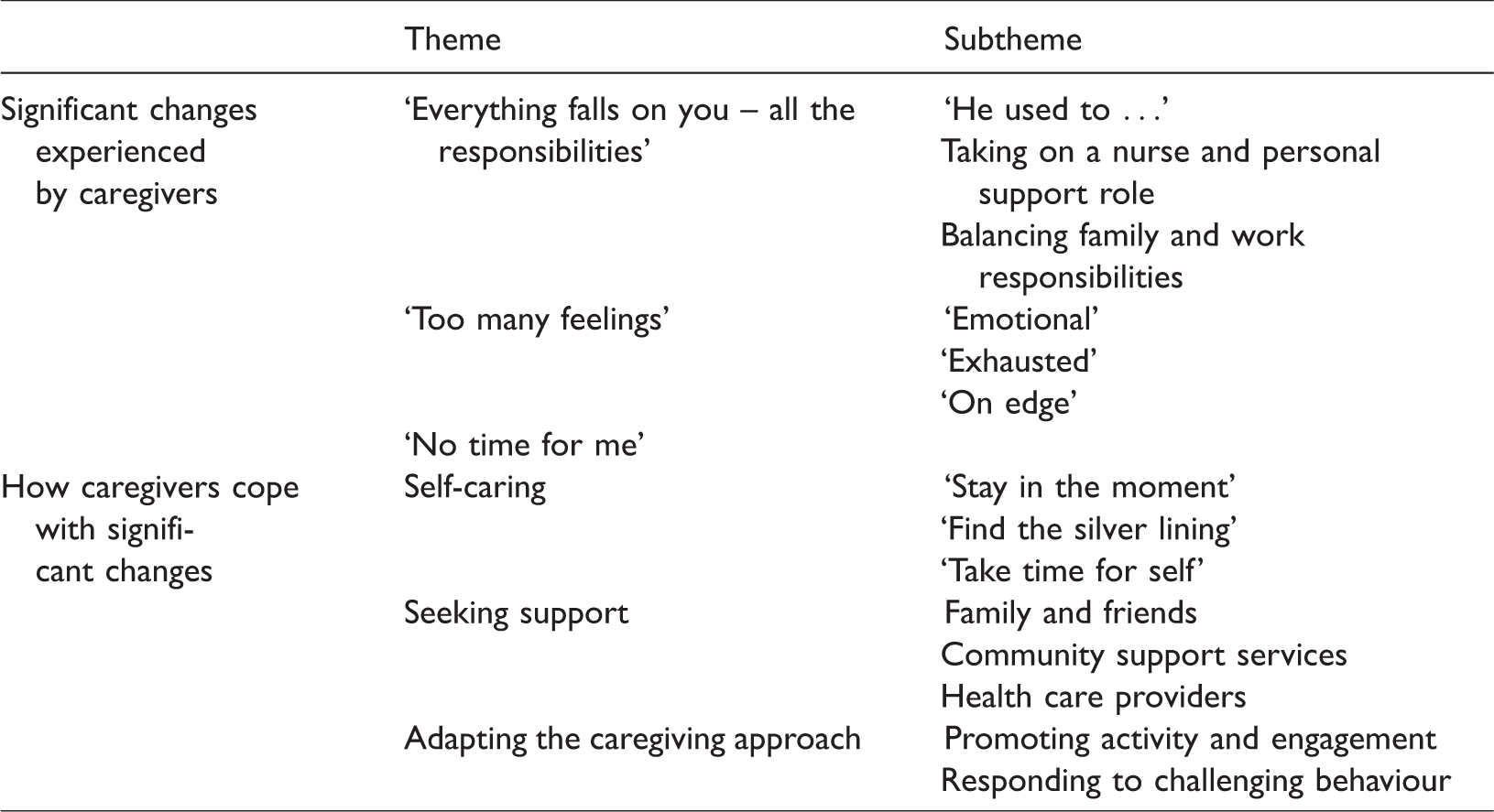
Six themes and related subthemes were generated through data analysis (refer to Table 2). The significant changes experienced by caregivers were described as: ‘everything falls on you – all of the responsibilities,’ ‘too many feelings’ and ‘no time for me.’ Caregivers coped with these significant changes by: seeking support, self-caring, and adapting the caregiving approach.
Overview of findings: Study themes and subthemes.
Significant changes experienced by caregivers
Participants described increasing responsibilities as dementia and MCC progressed for the persons in their care. These added responsibilities created feelings of exhaustion, frustration and being ‘on edge.’ Consequently, the demands of caregiving meant that caregivers had much less time to attend to their own needs.
Theme 1: ‘Everything falls on you – all the responsibilities.’ Caregiver participants repeatedly used the adjective ‘more’ to relate how much more difficult and challenging providing care to persons with dementia and MCC became as they progressed in their caregiving journey from both task performance and emotional perspectives as elucidated in this found poem:
More … of everything
More lifting More bending More helping More tending More dressing More washing. More planning More repeating More instructing. More stressed More anxious More tension More exhausted More emotional More lonely. More worried More concerned More unsure. More patient.
Taking on a nurse amd personal support role. Caregivers also expressed having to learn and assume responsibility for a number of nursing and personal support tasks that the persons with dementia and MCC needed. While the loss of self-care abilities was a consequence of dementia, the new caregiving roles were compounded by the presence of other chronic conditions, such as managing urinary and faecal incontinence, performing catheter care, post hip-fracture care, assessing for pain, and administering medications. This participant described the impact of dementia on her husband’s ability to self-manage his type 1 diabetes: I asked him tonight to just calculate the total carbs [to determine dose of insulin], he didn’t have a clue. So you can never do that by yourself when you have Alzheimer’s. Dealing with one [condition] is bad enough, but when you’ve got the double whammy, it’s twice as bad, if not more than that. (315)
Balancing family and work responsibilities. For some caregivers, increasing responsibilities were in addition to already busy work and family lives, as shared by one daughter: ‘I really can’t stop being a wife and mom to take care of dad’ (322). Caregivers who also had paid employment, experienced financial strain from missing work for caregiving duties and guilt from leaving the person with dementia and MCC alone during the work day. Caregivers often juggled competing demands of other family members: ‘My husband’s been ill, and he hasn’t been working all summer, and so that means I have to work more, but Mom still has needs’ (307). Some participants were sorrowful at not being able to spend as much time with their children or grandchildren due to the intensifying demands of caregiving.
Theme 2: ‘Too many feelings.’ Caregiving for a person with dementia and MCC comes with significant emotional and mental costs, including feeling ‘emotional,’ ‘exhausted’ and ‘on edge’ as revealed in this found poem:
Too Many Feelings
Too many feelings, there is no happy middle. Frustrated and numb, Depressed and frightened, Angry and guilty. I’m losing my patience. I’m trying not to cry. I try to keep my cool. I can’t do it anymore. I’m going to miss him.
‘Emotional.’ For the majority of participants, the care recipient was loved and the changing dynamic of their relationship was hard to bear: ‘My mom was always someone I can turn to and of course she isn’t in that role anymore’ (402). A husband disclosed his feelings related to initiating the long-term care placement process and wishing that he could do more for his wife: ‘I can’t control my emotion any more … I hate myself so much’ (026). Caregivers described feeling many emotions towards the person with dementia and MCC, such as frustration, impatience, annoyance, mourning, and fear. They described feeling ‘harder to cope’ (004), ‘extremely emotional’ (023), ‘tired out mentally’ (310) and ‘helpless’ (335).
‘Exhausted.’ Participants also experienced physical exhaustion, in part from the constant vigilance required to maintain the safety of the person with dementia and MCC. A husband described the reason behind his profound fatigue: ‘I can tell you the exact time she goes to the washroom [at night] and goes back in. You don’t sleep’ (311). Caregivers’ keen attention to the needs of the person with dementia and MCC resulted in caregivers becoming exhausted as explored in this found poem:
Exhausted
I’m showing signs of stress, I have pains across my chest. I’m on high alert all day. I sleep with ears wide open. I’m exhausted, I’m slowing down, I’m getting very tired. I’m no spring chicken anymore.
Security Blanket
I’ve become my mom’s security blanket. I caught her wandering one night, She had no idea where she was going. It’s getting scarier to leave her alone. She’ll freely let people in her home, Signing up for things over the phone. That’s a concern. She was getting her meds all mixed up. Sometimes she would double-dose, Sometimes she would under-dose. I’m worried about her falling now. When she’s sleeping, I go to check if she’s breathing.
Theme 3: ‘No time for me’. Caregivers often described providing care to a person with dementia and MCC as a ‘24/7 job’ (314). For many, not being able to leave the care recipient alone translated to no alone time for themselves. Additionally, the coordination of respite was regarded by some caregivers as harder than living without a break. One participant noted of her husband, ‘The preparation for getting him somewhere is exhausting’ (318). The challenges of having less and less time for the caregiver are summarized in this found poem:
No Time for Me
Accusation thrown, You missed your grandchildren growing up. I don’t have my friends calling, They all know I can’t get away. I’ve shut myself off from people ‘Cause I don’t have time for their crap. Things are never going to be The same as they were. It’s all on my shoulders, I have no personal life.
How caregivers cope with significant changes
Despite the significant changes experienced by caregivers in supporting persons with dementia and MCC, participants articulated strategies that they used to positively cope with these changes. Caregivers sought support from family and friends, home and community care, and health care providers. As changes occurred in their caring roles, caregivers applied what they learned from seeking support and adapted their caregiving approach.
Theme 4: Self-caring. In order to retain some optimism and honour the person with dementia and MCC, caregivers described using the following self-care activities: ‘stay in the moment,’ ‘find the silver lining,’ and ‘take time for self.’ As one caregiver summarized, ‘I try to take care of myself as best I can’ (026).
‘Stay in the moment.’ Many participants described intentionally giving themselves an internal pep-talk to stay in the moment by ‘taking one day at a time’ (396) to maintain ‘mind over matter’ (302) regarding the overwhelming feelings of sadness and frustration. One daughter explained that as her mother’s memory became worse, she intentionally shifted her focus: ‘We just take each day and each month as it comes and just kind of go from there’ (304). This required her to consciously set thoughts aside of her mother’s dementia progressing to the point where she may not recognize her daughter: ‘I don’t even want to cross that bridge right now.’
‘Find the silver lining.’ Another strategy that caregivers shared was to ‘find the silver lining’ (336) in their day-to-day life with the person with dementia and MCC in order to lift their spirits and bolster their resilience. One spousal caregiver remarked, ‘I’ve got him and he hasn’t forgotten me yet’ (306). Another spousal caregiver shared, ‘We can still laugh a lot. We talk a lot about the past. I enjoy these conversations with her’ (344). Other participants noted that they had developed skills in the caregiving journey: ‘This has really taught me a lot in communication’ (336); and ‘I’m a stronger person than I ever thought I was’ (388).
‘Take time for self.’ Although caregivers reported having increasingly less time for themselves, making opportunities to take a break was regarded as critical to coping with significant changes. Participants described the importance of not feeling guilty and giving themselves permission to take time away from the person with dementia and MCC. Caregivers shared a range of independent activities that they would undertake, including: travel, activities (e.g., reading, knitting, playing piano, gardening, playing cards), exercise (e.g., tai chi, yoga, walking, hiking, swimming, biking, running, golf), and socializing. A caregiver to her mother shared: ‘If it gets really crappy, I just go for a nice long walk. ‘Cause that’s my therapy. I’m good by the time I get back’ (018). Participants also shared strategies they used to take time for themselves even when they could not leave the care recipient, such as intentionally relaxing by taking a deep breath, having a nap, or praying.
Theme 5: Seeking support. Caregivers of persons with dementia and MCC recognized the need to seek support from family and friends, home and community care, and health care providers to sustain them in their caring role. One spousal caregiver acknowledged: ‘There’s no cure, it’s not going to get better, it’s only going to get worse’ (002). A daughter shared what she had learned in caring for her mom: ‘I think you can’t handle it on your own unless you are super, super strong. But I think you need to have that support system’ (304).
Family and friends. Caregiver participants primarily sought out the support of family and friends to talk or take a break. Caregivers reached out to neighbours, their friends and friends of the person with dementia and MCC, siblings, children and grandchildren, depending on familial relations and geographic proximity. Caregivers described enlisting this support by connecting face-to-face with the support person as well as calling or emailing. One daughter explained: ‘A lot of my friends are going through the same thing. We compare notes constantly’ (304). Conversely, another caregiver acknowledged the gradual loss of some relationships when friends were uncomfortable with her mother’s dementia: ‘It would be really nice if friends would not back away’ (307). Caregivers requested a range of assistance from family and friends to help them cope with changes in their caring roles including: staying with the care recipient when they were out, driving and taking the care recipient out, for example, to have a meal.
Community support services. Participants sought support from their local Alzheimer Society and community support services. Caregivers used many helpful Alzheimer Society programmes, including: support groups for caregivers and persons with dementia, education classes (e.g., preparing for long-term care placement, learning about dementia), and meetings for both the caregiver and person with dementia and MCC inclusive of social, creative arts or exercise components. A daughter explained what she learned from attending education classes: I was amazed because I knew Alzheimer’s made you forget, I didn’t understand what that meant. I didn’t understand that it didn’t just mean forgetting thoughts per se, like you know I can’t remember someone’s name. It meant forgetting what an item is, so how you use it. Then it was like: wow so that’s why she’s doing it! (402)
Health care providers. Some caregivers also accessed government-funded home care services, such as personal support care for the person with dementia and MCC or an occupational therapist home safety assessment. One daughter described the increasing and instrumental role PSWs had played in caring for her mother: We were able to get PSWs in there morning and night, seven days a week. And so that has been the biggest godsend, because that just takes a lot of the worry out of her daily routines, her washing, her getting ready in the morning, taking her meds, taking her nitro patch off. (304)
Theme 6: Adapting the caregiving approach. As the care recipients’ dementia and MCC changed, progressed and worsened, participant caregivers had to creatively adapt and adjust their approach. A wife described the first time her husband refused to get ready to attend his day programme: It’s always changing. You think you’ve got it figured out and you don’t. Because he reacts differently to where you just think you’re getting into a routine, so it just stops you. I just got to say to myself, ‘Okay, how are we going to work on this?’ He changes and then you have to change. (306)
Promoting activity and engagement. Caregivers noted changes in the care recipient’s initiative and interest. ‘She just sits and stares and you need to engage her in anything. Otherwise she has only a few things she would do. Otherwise she does nothing,’ commented one spousal caregiver (397). Caregivers in turn compensated intentionally with a variety of strategies, such as initiating and leading conversations and maintaining social activity. As one wife stated, ‘We have a very active social life and I insist on it because I need it, as well as him’ (306). Caregivers also encouraged exercise as this husband described, ‘She’s not doing much physical exercise, but we now dance for 20 minutes every morning and every afternoon, because she recognizes the old oldies that she used to as a teenager’ (301). Caregivers also discovered new activities when the person with dementia could no longer do hobbies they previously enjoyed, such as word search rather than a crossword puzzle. The rationale for engagement was often to prevent the progression of the disease by keeping the person’s mind active but this caregiver shared another motive: ‘I want her to have a feeling of accomplishment’ (308).
Responding to challenging behaviour. Caregivers frequently had to adapt and change their approach to the person with dementia and MCC when encountering challenging behaviours, such as sleep disturbance, resistance to personal care, or exit-seeking. One caregiver explained: ‘Last night, we went to bed later ‘cause if you go to bed early, he just wakes up in a couple of hours. So, went to bed at midnight, and he slept till 5:45. So, I felt that was a success. I’ve been experimenting with stuff, what works best’ (027). To avoid her husband becoming upset during personal care, this spousal caregiver reported, ‘One rule I’ve made for myself is that when I’m providing care, the hands-on care, like, washing and cleaning and that sort of thing, I take my time. I don’t rush’ (023). Another caregiver was challenged almost daily by her husband feeling that he had to leave to be somewhere else. She shared this story of how she changed her approach to re-direct him: “This is what I’ve been looking for.” And I said, “What?” He said, “Me train ticket.” I said, “It’s your health card.” He said, “No, it’s my train ticket.” “But let me have a look – Oh, yeah, you’re right.” “Have a look at that, read that, tell me what train I’ve got to get on so I’ll know where to get off.” So I had to pretend to look at it, and he went, “Come on, then, get your coat on, else we’re going to be late.” And I said, “Well, this is for tomorrow, not for today.” “Oh. So we haven’t got to go today.” I said, “No, we’ve got to go tomorrow.” And then, so that was one day. (330)
Discussion
The results of this qualitative descriptive study make important and unique contributions to the understanding of the changes experienced by caregivers of persons with dementia and MCC and how they cope with these significant changes. Consistent with transition theory, these caregivers experience multiple, simultaneous and complex patterns of transitions as they tend to the care recipients’ declining health, physical and emotional well-being (Meleis et al., 2000). However, these patterns of transition grow in complexity over time for caregivers supporting persons with a progressive, debilitating brain disease who are also living with other chronic conditions. This notion of escalating, confounding difficulty and the resultant, necessary adaptation for this group of caregivers was a novel finding of this study.
The finding of ‘everything falls on you – all the responsibilities’ was congruent with previous research with caregivers (Feil et al., 2011; Sanders & Power, 2009). What the participants in this study particularly illuminated was how these responsibilities continue to increase over time in both number and complexity. Family caregivers had to perform all the household duties in addition to performing what could be considered professional nursing interventions, for example, implementing mobility restrictions and rehabilitative exercise for a person with dementia post-acute hip fracture.
Caregiver research has previously described the significant personal and emotional impact on caregivers of persons with MCC (Ploeg et al., 2017). The large group of caregivers that participated in this study were particularly articulate, insightful and candid about the profundity and intensification of the mental and emotional toll of ‘having too many feelings.’ This may be due, in part, to the trusting relationships that developed between the data collectors and the participants over repeated phone contact that allowed for these candid revelations. This portrait of their burden is an important warning to heed in considering care delivery to this population, particularly given that caregivers to older adults with dementia and MCC are often older and living with MCC themselves.
These findings also contribute to the body of literature on how caregivers of persons with MCC sustain themselves in caregiving roles; supporting the strategy of taking time for themselves and revealing techniques, such as ‘staying in the moment’ and ‘finding the silver lining’ (Peacock et al., 2017). Although unlike other research where caregivers of persons with MCC ultimately achieve a sense of mastery in their role over time, caregivers in this study described an almost ever-evolving and adapting performance of their role as the needs of the persons with dementia and MCC changed (Meleis et al., 2000; Williams et al., 2016).
An important finding was that caregivers sought support primarily from community support services, such as the Alzheimer Society, firstly and more consistently than health care services. Very few participants described connecting with government-funded home care services, such as a community care coordinator or nurse, as a strategy to cope with challenging transitions. Even when struggling with adjusting insulin doses when the care recipient would refuse meals, for example, caregivers did not routinely describe reaching out to professional health care services. This could be partly explained by the sampling strategy in that most of the participants were recruited through local Alzheimer Societies but does reveal a gap in service provision that potentially could mitigate caregiver burden and distress. Conversely, these findings demonstrate the extremely valuable and important role that community support services play as a coping resource for caregivers of persons with dementia and MCC.
Strengths and limitations
This study has several limitations. The sample of participants was mostly Caucasian and included only a small proportion of those living with inadequate financial means. Additionally, some participants received the study intervention and participants were mainly recruited through the Alzheimer Society caregiver support programmes, which could mean their experiences were uniquely impacted by this support. Conversely, the study has many strengths, including a large sample size; and diversity of caregivers by living situation, working status, age, gender, and relationship to person with dementia and MCC. Also, connecting with participants by phone facilitated broader caregiver engagement as they could take the call at a convenient time, such as after work or when the care recipient was resting.
Implications for practice and research
Comprehensive care of the person with dementia and MCC and caregiver as a unit is required, meaning any service, whether community support or health care, needs to consider both the person with dementia and the caregiver as clients. Unrecognized caregiver burden is a threat to the health and well-being of not only the person with dementia who is relying on their care but the caregiver themselves. Caregiver burden is related to negative health outcomes and increased use of health care services (Williams et al., 2016; WHO, 2017). Consequently, with family caregivers providing the bulk of caregiving tasks for persons with dementia and MCC, any change in their abilities would translate to increased need for professional or institutional care (Williams et al., 2016).
Caregivers in this study shared the significant changes they faced as they cared for persons with dementia and MCC and as a result, a societal obligation presents itself to intervene to assist caregivers to cope with increasing responsibilities, such as the provision of homemaking, home maintenance and personal care services. Furthermore, if society continues to have an expectation of family caregivers to take on professional, health care tasks in the face of their own health issues and behavioural responses of the person in their care, access to health care professional support should be provided. A logical liaison point could be community support services (e.g., adult day programme or caregiver support group) for referral to home care services (Donner et al., 2015).
Caregivers revealed cognitive sustaining strategies that could be beneficial, such as staying in the moment. These positive coping strategies could be taught in caregiver support groups. Also, there is a need for health care and community support service providers to connect caregivers to organizations such as the Alzheimer Society, adult day programmes, and caregiver respite services to provide the much-needed ‘time for me’ for caregivers.
Future research should include understanding the nature of service provision for caregivers of persons with dementia and MCC, map out existing care pathways, and develop and evaluate alternate solutions that care for the comprehensive needs of the caregiver-care recipient unit. Qualitative exploration of the experiences of culturally diverse caregivers would also be important to have a more comprehensive understanding of caregiving experiences. The creation of found poems was an innovative and effective method to convey participants’ experiences and could be a helpful knowledge translation tool to raise awareness of caregiver burden and resilience to the public, decision makers, and health care professionals.
Conclusion
This paper revealed how caregivers of older adults with dementia and MCC face many significant changes in their caregiving journey over time that pose a threat to their physical, emotional and social health. These caregivers experienced unique challenges and used novel strategies to cope with the changes they experienced. Health and community support interventions have the potential to facilitate successful transitions in this long and difficult trajectory. Uptake of such an approach at the community level requires social, economic and political coordination.
Footnotes
Acknowledgements
The authors extend their sincere thanks to all the study participants for their time and commitment to the study and insights shared. We also are thankful for the support of our community partners: Alberta Caregivers Association; Alzheimer Society of Alberta and NWT; Alzheimer Society of Brant, Haldimand Norfolk, Hamilton and Halton; Alzheimer Society of Calgary; Alzheimer Society of Ontario; and Covenant Health Alberta. Thank you also to the data collectors Ann Cotton, Annie Lam, Lori Pollard, Vanessa Ritchie, Kathya Jovel Ruiz, and Tracey Wildeman.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of a programme of research, the Aging, Community and Health Research Unit, School of Nursing, McMaster University, and was supported by the Canadian Institutes of Health Research Signature Initiative in Community-Based Primary Healthcare (Funding reference number: TTF 128261).