
Abstract
Objective
Multimodal non-pharmacological interventions have been argued to have the potential to complement current pharmacological approaches to improving quality of life for people living with dementia. The aim of this review was to identify, synthesise and appraise the evidence for the effectiveness of multimodal non-pharmacological interventions for improving cognitive function specifically.
Method
After a comprehensive search strategy including grey literature, 26 studies were reviewed. The inclusion criteria concerned adults with a primary diagnosis of dementia. Studies used two or more different modes of intervention, and measured a cognitive outcome. Due to differences in the conceptualisations of the term ‘multimodal’, a typology of modes and methods was developed to facilitate classification of candidate studies.
Results
Twenty-one group studies and five case studies were found. Group studies used two or three modes of intervention and multiple methods to implement them. Interventions utilised were cognitive, physical, psychological and psychosocial, nutrition, fasting, gut health, sleep hygiene, stress reduction, detoxification, hormonal health and oxygen therapy. Five individual case studies were found in two separate papers. Each personalised patient treatment utilised in-depth assessments and prescribed up to nine different modes. In 19 (90%) of the 21 group comparisons, participants were reported to have cognitive improvements, stability with their dementia or a delay in their decline. The extent of these improvements in terms of meaningful clinical change was variable.
Conclusion
Multimodal non-pharmacological interventions have the potential to complement singular therapeutic approaches by addressing multiple modifiable risk factors currently understood to contribute towards cognitive decline.
Introduction
The latest estimate of people affected by dementia worldwide is 50 million (Pickett et al., 2018), with a further nine million people developing dementia yearly (WHO, 2017). Current narratives suggest that the progression of dementia is inevitable, supported by the results of pharmacological trials which have been less than encouraging (Cummings, Morstorf, & Zhong, 2014). However, regardless of whether improvements in drug efficacy are possible, people with dementia often have other long-term conditions and so additional medication can cause unpleasant interactions with existing regimes. On the other hand, non-pharmacological interventions can provide complementary therapy, offering useful, versatile approaches to improve outcomes for people with dementia (Olazaran et al., 2010).
Whilst a number of abilities are affected in people with dementia, its primary manifestation is through reduced cognitive ability. Global cognition is a broad term covering various cognitive functions including memory, executive functioning (time management, judgement, planning), attention (ability to direct energy to perform the task at hand, organise tasks into a coherent logical pattern), language and communication. Cognitive interventions (CIs) in people with dementia have been classified by Clare and Woods (2004) into three basic types – cognitive stimulation (CS), training (CT) and rehabilitation (CR). According to Buschert et al. (2011), training for specific cognitive functions is less useful for more impaired participants, but stimulation and activation of everyday functions tend to be more meaningful and successful. Overall, studies show evidence of small but consistent effects of CI in improving cognition (Alves et al., 2013). Moreover, evidence suggests that utilising more than one method of CI can incrementally improve cognition of people with dementia (Barban et al., 2016; Cotelli et al., 2014; Lee, Choi, Oh, Sohn, & Lee, 2016; Panerai, 2016).
Another intervention with potential is routine physical exercise (Olazaran et al., 2010). Exercise increases the size of the hippocampus and improves memory in older adults (Erickson et al., 2011). For example, better cognitive scores, after 6 to 12 months of exercise, were found by Ahlskog, Geda, Graff-Radford, and Petersen (2011) who recommended exercise as a disease-modifying treatment. In particular, there is evidence of a beneficial cognitive effect of high intensity exercise interventions (Livingston et al., 2017). In a meta-analysis of 802 patients in 18 randomised controlled trials (RCTs) the combination of aerobic and non-aerobic exercise interventions (offered at both high and low frequency) positively influenced cognition in patients with dementia (Groot et al., 2016).
Another mode worthy of investigation is nutritional modification, with micronutrients, vitamins and antioxidants showing some evidence of attenuating disease progression (Aliev et al., 2013) and improving cognition through mitochondrial energy production and protein synthesis (Troesch, Weber, & Mohajeri, 2016). Proper nutrition is also related to AD through epigenetic pathways, suggesting a potential role in the prevention of late-onset AD and attenuation of cognitive deficits (Athanasopoulos, Karagiannis, & Tsolaki, 2016).
As well as CIs, physical exercise and nutrition, numerous other modes can reduce the risk for dementia or address the symptoms. Whilst several of these are trialled in the included studies, more are emerging from new evidence that nearly 600 factors can potentiate the development of AD (Kostoff, Zhang, Ma, Porter, & Buchtel, 2017). This understanding that dementia is multifactorial and determined by mechanisms that interact and intervene throughout life (Van der Linden & Juillerat Van der Linden, 2016) has given rise to the emergence of multimodal approaches to prevention.
Dementia prevention trials affirm that risk factors can be reduced when using a multimodal approach, as multiple mechanisms may be necessary for clinically significant effects on global cognition (Ngandu et al., 2015). Indeed, activities containing more than one component seem to be more beneficial in reducing risk (Karp et al., 2006). These may exert a synergistic effect, for instance, whereby physical training guided by CT may facilitate the neuroplastic potential to induce beneficial cognitive effects (Bamidis et al., 2015), controlling cognitive decline and improving quality of life (QoL) (Aliev et al., 2013).
Evidence for multimodal approaches also includes combined training for brain plasticity, neurogenesis in the hippocampus and a neuroprotective effect on the cerebral cortex (García-Mesa et al., 2011). For example, Curlik and Shors (2013) found that a combination of physical training followed by successful mental learning was more beneficial for neuronal recruitment and overall mental health than either activity alone. Furthermore, exercise in combination with dietary factors can affect molecular events related to the management of energy metabolism and the synaptic plasticity of cognition according to Gomez-Pinilla (2011). Köbe et al. (2016) found that omega-3 fatty acid intake combined with aerobic exercise and CS prevented atrophy in AD-related brain regions in mild cognitive impairment (MCI) patients.
Given the emergence of multimodal approaches, some reviews have already been conducted. Rodakowski, Saghafi, Butters, and Skidmore (2015) found small improvements in selected cognitive abilities in early stage dementia from a combination of cognitive and physical exercise. Law, Barnett, Yau, and Gray (2014) found significant cognitive function improvement in four out of five studies combining cognitive and exercise training in older adults with cognitive impairment. However, Rodakowski et al.’s (2015) scoping review looked at adults with a range of cognitive impairment. Law et al. (2014) looked only at exercise and CS in adults with and without cognitive impairment. Therefore, it remains to understand the extant evidence more comprehensively.
Three gaps in the literature have been identified which make this review both timely and relevant. Firstly, whilst there is growing interest in non-pharmacological interventions for treating dementia, little is known about the effect of complex interventions in this population. Secondly, evidence exists for people with subjective cognitive impairment (SCI) and MCI, but evidence is lacking for measured cognitive outcomes in studies specifically for people living with dementia. Thirdly, whilst some reviews, such as the two above have been conducted which look at certain combinations of modalities, a thorough systematic review of all possible modality combinations has not been conducted. Consequently, this review provides a synthesis of the evidence for multimodal non-pharmacological interventions (MNPIs) for improving cognitive function for people living with dementia.
Method
Search strategy and screening
A systematic search of peer-reviewed literature was performed on PubMed, PsycINFO, Medline, Scopus, EMBASE, Cochrane Database of Systematic Reviews, CINAHL and LILACS. Search terms included dementia, Alzheimer’s or cognitive impairment and variations of multimodal, treatment, intervention, activity or programme tailored to each database (Online Appendix 1). Grey literature was also searched for theses, dissertations, policy documents and conference proceedings.
Typology development
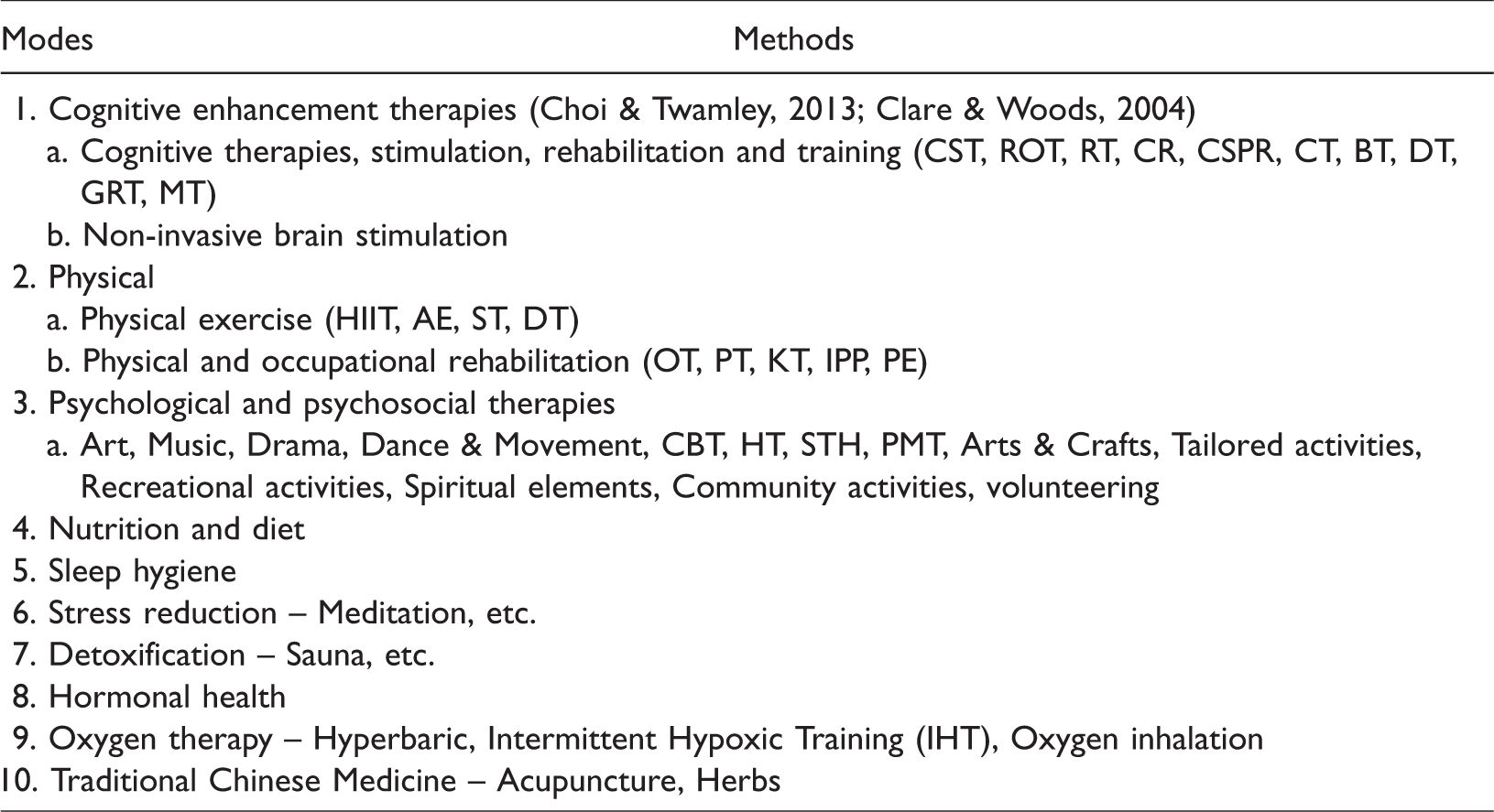
Multiple terms in the evidence have been used to describe ‘multimodal’ interventions. For this review, a classification system was required to determine how many modes a study utilised and hence, whether it was included. Drawing upon the categories of Choi and Twamley (2013) and Clare and Woods (2004), three initial modes were derived:
Cognitive enhancement therapies (CS, CT and CR; non-invasive brain stimulation); Physical interventions (physical exercise, physical and occupational rehabilitation); and Psychological and psychosocial therapies (art, music, dance, cognitive-behavioural therapy (CBT), horticultural therapy (HT), psychotherapy, recreational activities, volunteering, etc.).
Seven further modes emerged from the title and abstract screening (see Table 1).
Typology of modes and methods for dementia interventions – Brief.
Inclusion criteria
All included studies met the following inclusion criteria:
Involved older people with a primary diagnosis of dementia; At least two modes of non-pharmacological intervention; Changes in cognitive function was an outcome measure; Any study design or setting; Studies with mixed participant groups (dementia, MCI, etc.) if subgroup analysis (e.g., individuals with dementia) was available; English language of any date.
Exclusion criteria
Specifically addressed delirium, pain, incontinence or behavioural and psychological symptoms of dementia (BPSD); If only two modes addressed and one of these delivered training, knowledge or support to care staff or family carers; One mode was pharmacological treatment. (If participants were taking stable doses of dementia medication prior to the study it was not excluded.)
(A list of acronyms and abbreviations can be found in Online Appendix 4)
Study selection
Ninety-seven candidate studies were selected at the title/abstract stage by the first author (GC). The other authors (CM and JS) checked 10% of the studies, discussed and resolved any disagreements. Figure 1 shows the searching, screening and selection process. The team consulted on the modes and methods of intervention. Twenty-four papers were initially included (27 group or case studies) finalising the Typology at 10 modes (Table 1). See Online Appendix 2 for detailed descriptions of modes and methods.
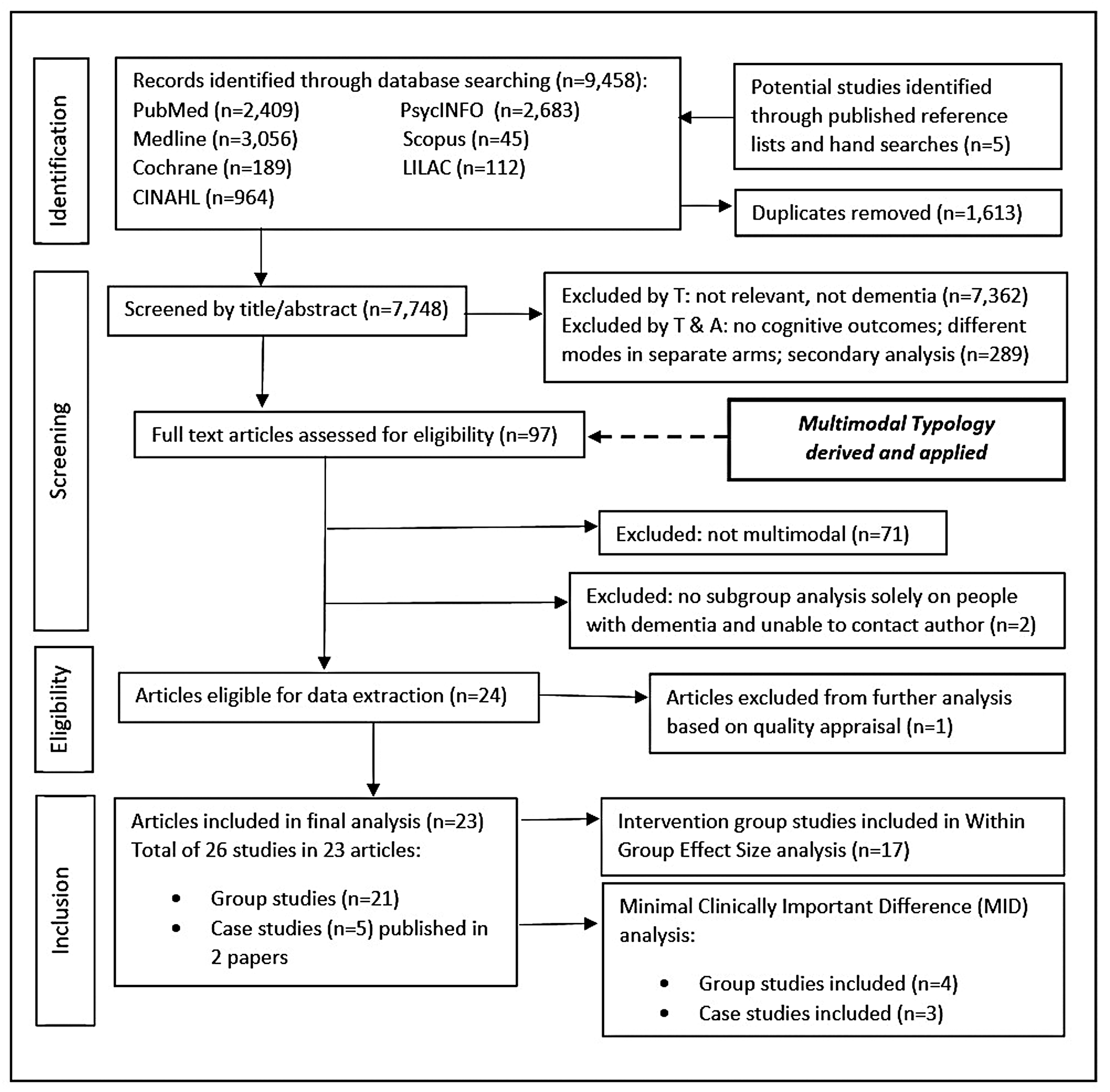
Flowchart of the searching, screening and selection process.
Included studies are shown in Table 2 with their modes of intervention.
Included studies and their modes.
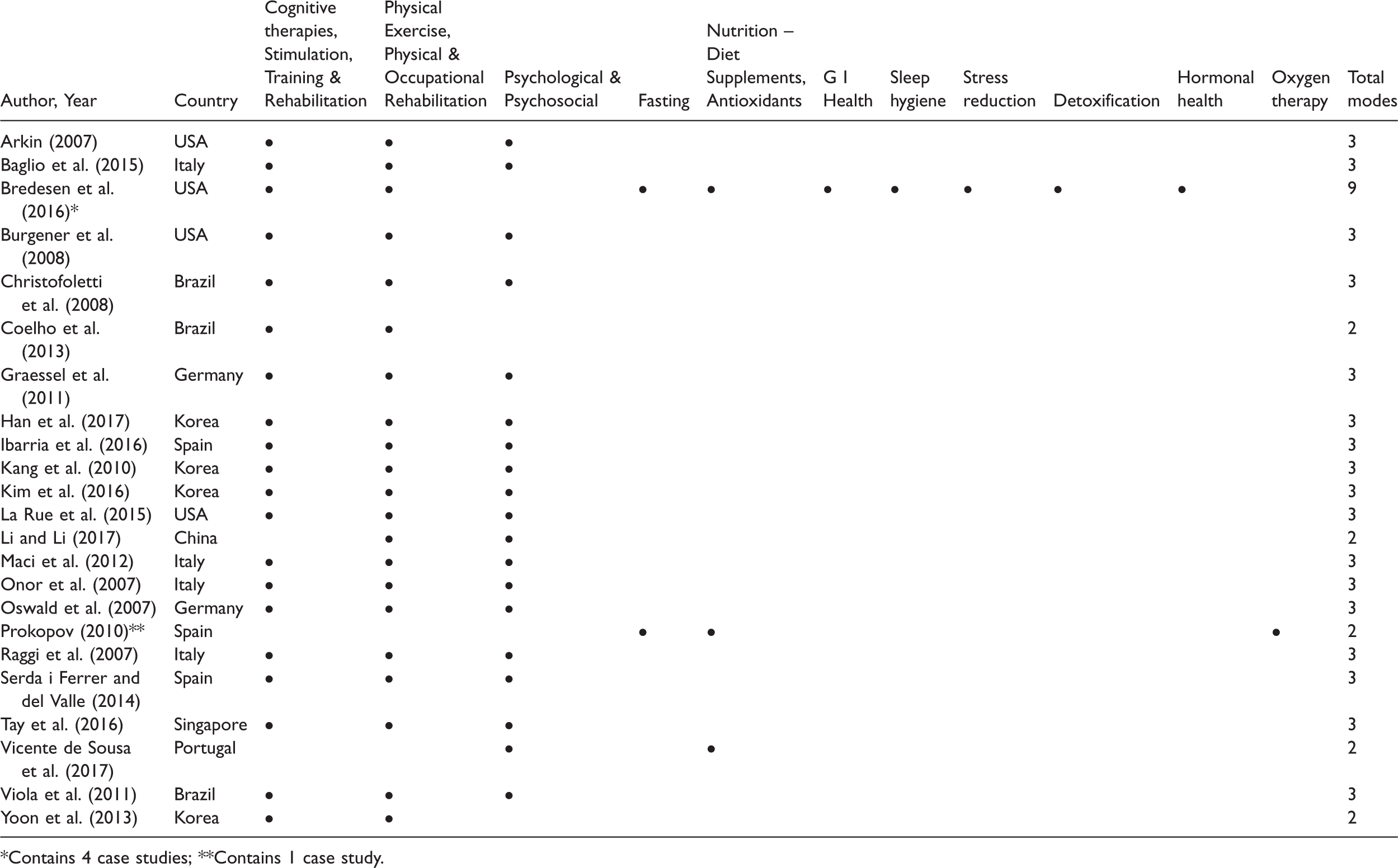
*Contains 4 case studies; **Contains 1 case study.
Searching the grey literature revealed increasing public and practitioner interest in the area of non-pharmacological treatments for dementia, including multimodal approaches. However, no findings from the grey literature met the inclusion criteria.
Quality appraisal
Given that both qualitative and quantitative studies were eligible for inclusion in the review, quality appraisal of the peer-reviewed literature utilised the Mixed Methods Appraisal Tool (
Data synthesis and analysis
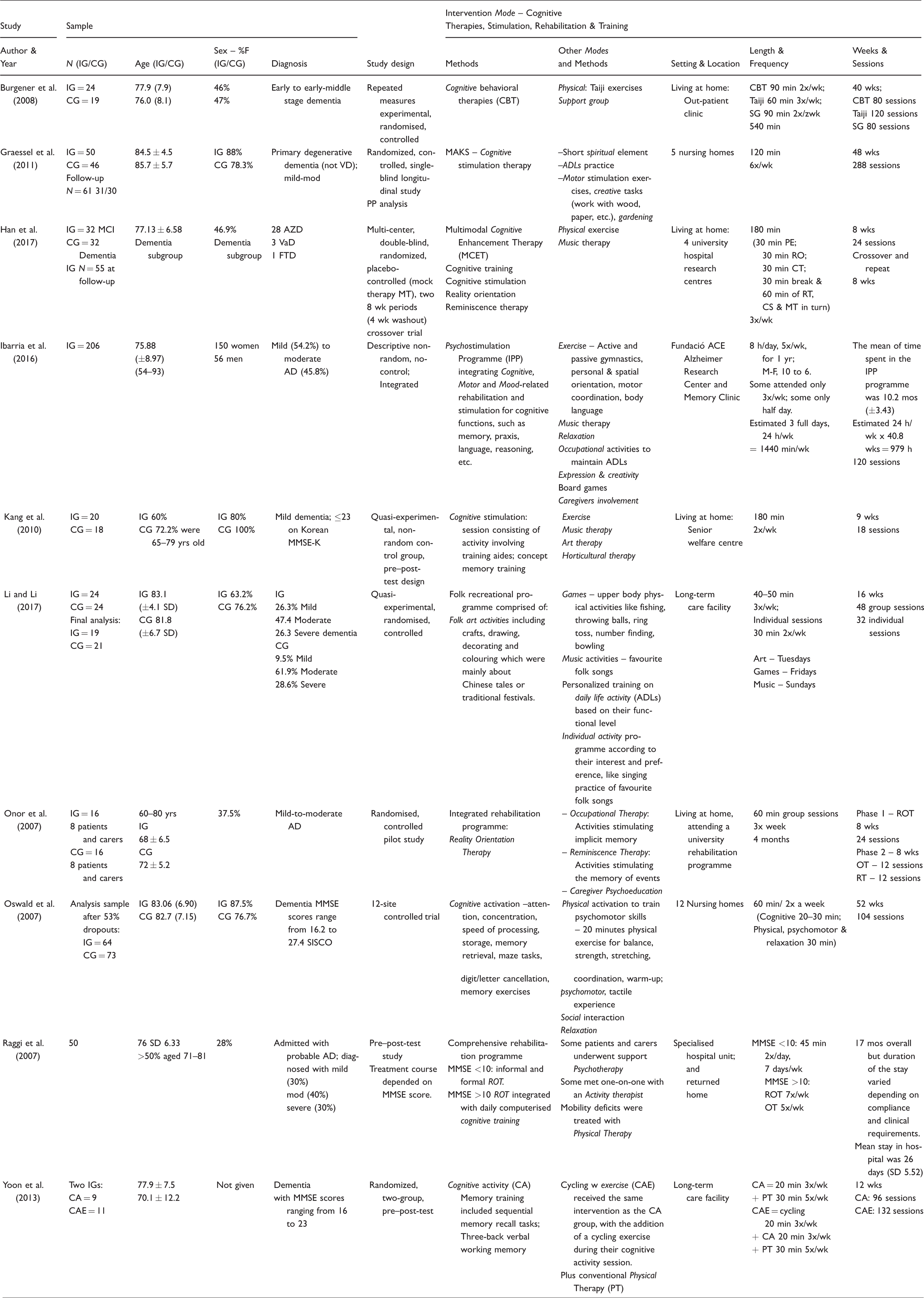
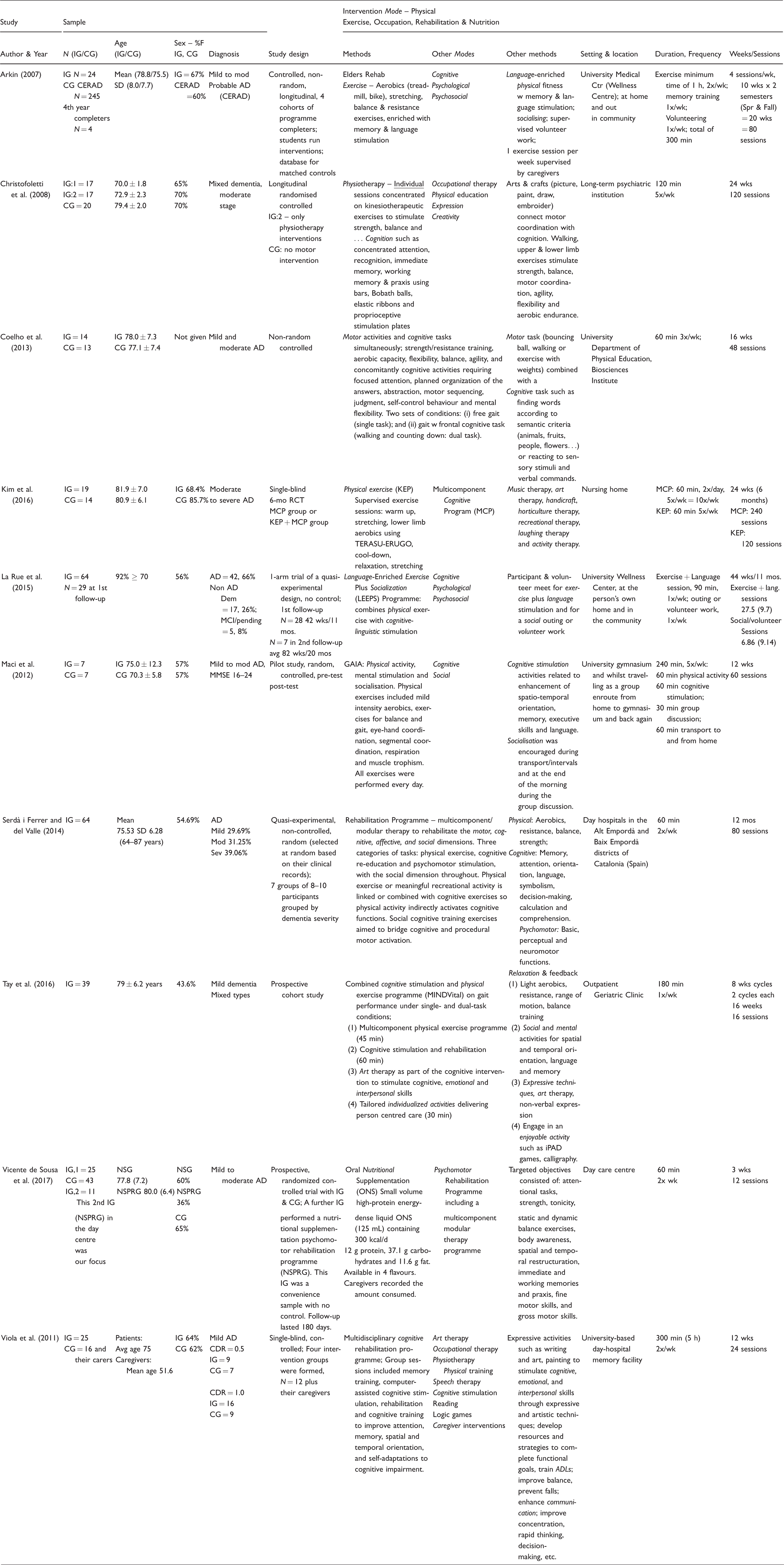
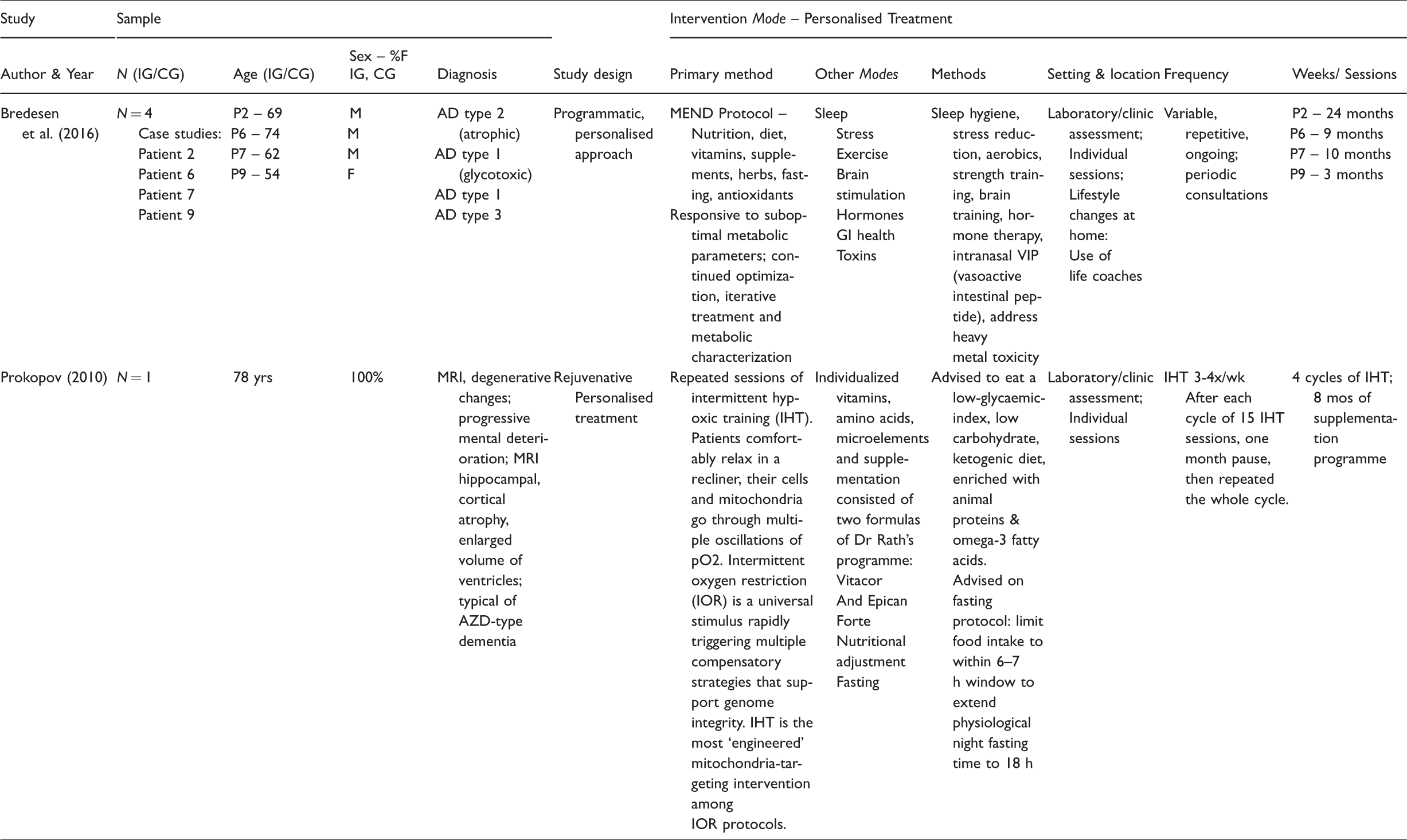
The included studies were found to have one predominant characteristic under which they could be compiled and synthesised. Ten studies in which the intervention mode was predominantly cognitive (therapies, stimulation, rehabilitation or training) are presented in Table 3. Ten further studies in which the intervention was predominantly physical (exercise, occupation, rehabilitation or nutrition) are presented in Table 4. Finally, two case study papers (with a total of 5 individual case studies) in which the intervention mode was personalised treatment in a clinical or research setting are shown in Table 5. Study characteristics included author & year; sample, study design, intervention modes and methods, setting, study length, frequency and time involved.
Study characteristics – Cognitive.
Study characteristics – Physical.
Study characteristics – Personalised treatment – N of 1.
Participants and settings. Studies were from Korea (4), USA (4), Italy (3), Spain (3), Brazil (3), Germany (2), China (1), Portugal (1) and Singapore (1). Participant numbers in the group studies ranged from 14 (Maci et al., 2012) to 206 (Ibarria et al., 2016), with a mean of 58, and an age range of 54–93. Two case studies reported on five patients with dementia, aged 54–78 (Bredesen et al., 2016a; Prokopov, 2010). Participants totalled 1,178, of which 388 in six studies lived in long-term care (nursing home or a psychiatric hospital) and 790 in 16 studies lived at home, attended a day service or were hospitalised for a period of weeks. Two studies (Onor et al., 2007; Viola et al., 2011) also enlisted the caregivers as participants during the intervention.
Pharmacology. Some participant groups were on stable doses of memantine, cholinesterase inhibitors and/or antidepressants prior to, and during, the studies although no study declared participants to be drug-naïve. Individualised treatment programmes that purported to address the root cause of the dementia symptoms (Bredesen et al., 2016; Prokopov, 2010) prescribed pharmaceutical adjuncts such as bio-identical hormones to address specific imbalances.
Study designs. Whilst the methodology was designed to be inclusive of qualitative and mixed methods studies, all studies meeting the inclusion and quality criteria were quantitative in design, but quite heterogeneous. Whilst all carried out pre–post-tests, only 11 (48%) were RCTs (Quality Appraisal 84%). A further five were non-randomised (QA 100%) and seven were quantitative descriptive (QA 100%) (see Quality Appraisal in Online Appendix 3). Han et al. (2017) was the only double-blind or cross-over trial. Three were conducted across multiple centres: Graessel et al. (2011) and Oswald, Gunzelmann, and Ackermann (2007) in German nursing homes, and Serdà i Ferrer and del Valle (2014) in Spanish day hospitals. For characteristics of all studies, see Tables 3 to 5.
Intervention modes and methods. Li and Li (2017) had no cognitive mode, and Prokopov (2010) and Vicente de Sousa et al. (2017) had neither cognitive nor physical mode, but all others had both. Only four lacked a psychological, psychosocial, psychomotor, spiritual, caregiver or support mode. One used oxygen therapy (Prokopov, 2010) and three addressed diet and nutrition and/or fasting (Bredesen, 2016; Prokopov, 2010; Vicente de Sousa et al., 2017). Four studies termed ‘multicomponent’ or ‘dual-task’ combined modes simultaneously and are shown in Table 4 spanning two columns. Methods utilised within the studies illustrated the creative variability of the main modes. Cognitive mode (Table 3) included methods such as therapies, stimulation, rehabilitation and training. Physical mode (Table 4) included methods such as exercise, occupation, rehabilitation and nutrition. Table 5 elucidates multiple methods found in personalised treatment interventions.
Study duration. The length of group intervention ranged from 20 minutes (Yoon et al., 2013) to 8 hours (Ibarria et al., 2016). The shortest timeframe was three weeks (Vicente de Sousa et al., 2017), whereas Arkin (2007) continued a facilitated intervention for up to four years. Personalised N-of-1 treatments were followed-up through clinic visits for 24 months (Bredesen et al., 2016).
Stage and type of dementia. Seven studies included participants with mild dementia, 11 with mild to moderate, three with mild, moderate or severe and one with moderate to severe. Twelve studies included participants with AD whilst 10 included unspecified or mixed types of dementia. A study by La Rue, Felten, and Turkstra (2015) included 8% (N = 5) of participants with MCI. The decision was taken to include this study as >90% of participants fit the inclusion criteria.
Outcome measures. For cognitive assessment, multiple tools were utilised. Predominantly, 21 studies used the MMSE (English, Korean and Chinese versions), nine used the Clinical Dementia Rating (CDR) and fouir used the ADAS-Cog (Cognitive subscale of the Alzheimer’s Disease Assessment Scale) or ADAS-K (Korean version). Fourteen other scales were used once or twice (see Table 6 for details). Of the 21 group studies, 17 (81%) reported pre–post-test scores using the Mini Mental State Examination (MMSE), the Chinese MMSE or the 7MST (7 Minute Screening Test), and could therefore be included in an effect size (ES) analysis (Figure 2). Oswald et al. (2007) uniquely included a staff survey on residents’ cognitive change. In the five case studies only three provided pre–post-test MMSE or similar which hindered comparison of clinical importance (Figure 4). The case studies in Bredesen et al. (2016) reported over 10 instruments including magnetic resonance imaging (MRI) and fluorodeoxyglucose (FDG)-positron emission tomography (PET) scans, metabolic testing, quantitative neuropsychological testing, genetic testing and a battery of cognitive tests. Whilst three of these case studies reported pre–post-test MMSE, one (Patient 9) reported the Montreal Cognitive Assessment (MoCA) instead, which substituted for the MMSE in the ES analysis. Interestingly, all four group studies that showed clinically important differences used MMSE exclusively (Figure 3).
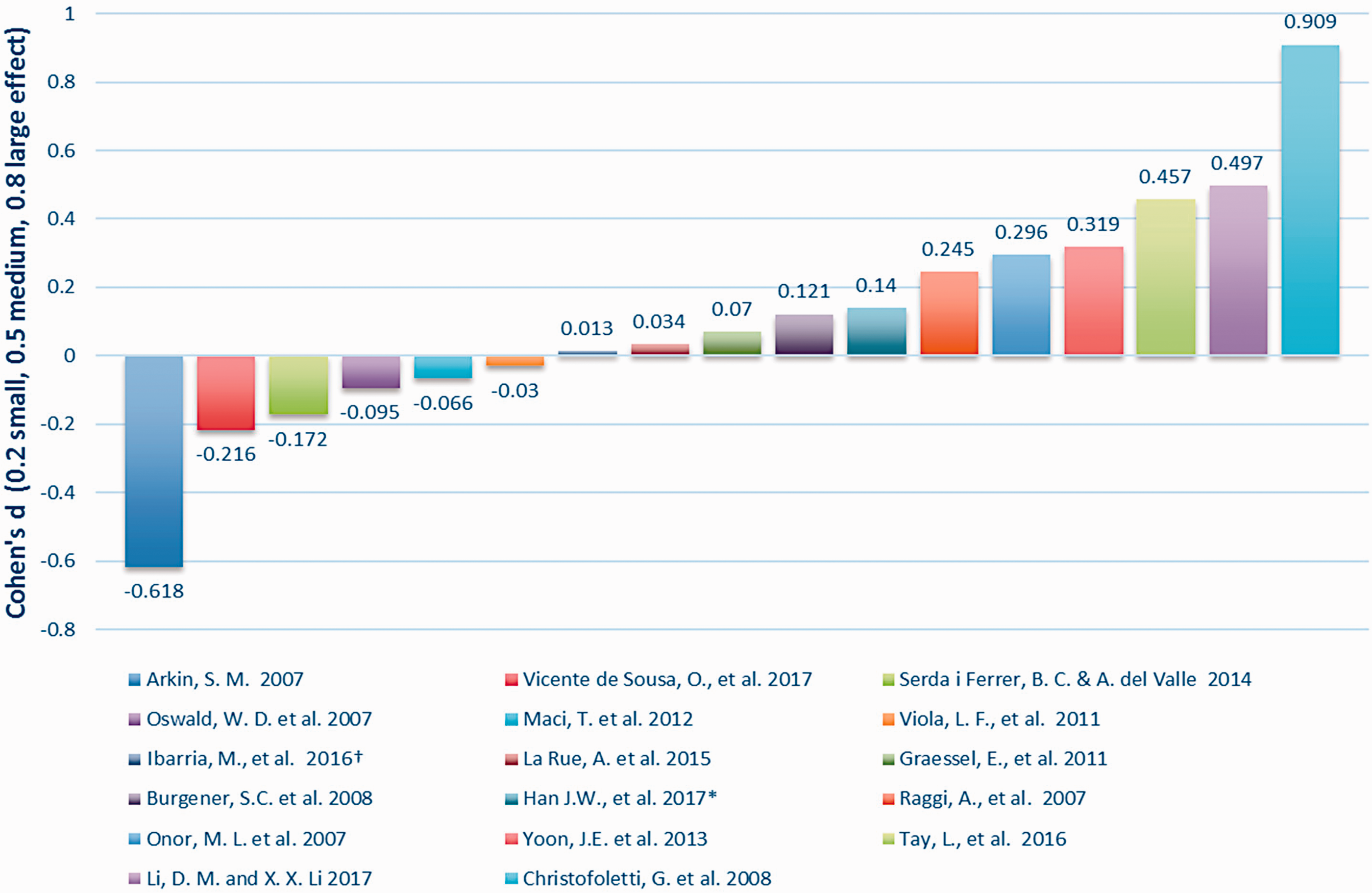
Within group effect size – intervention groups.
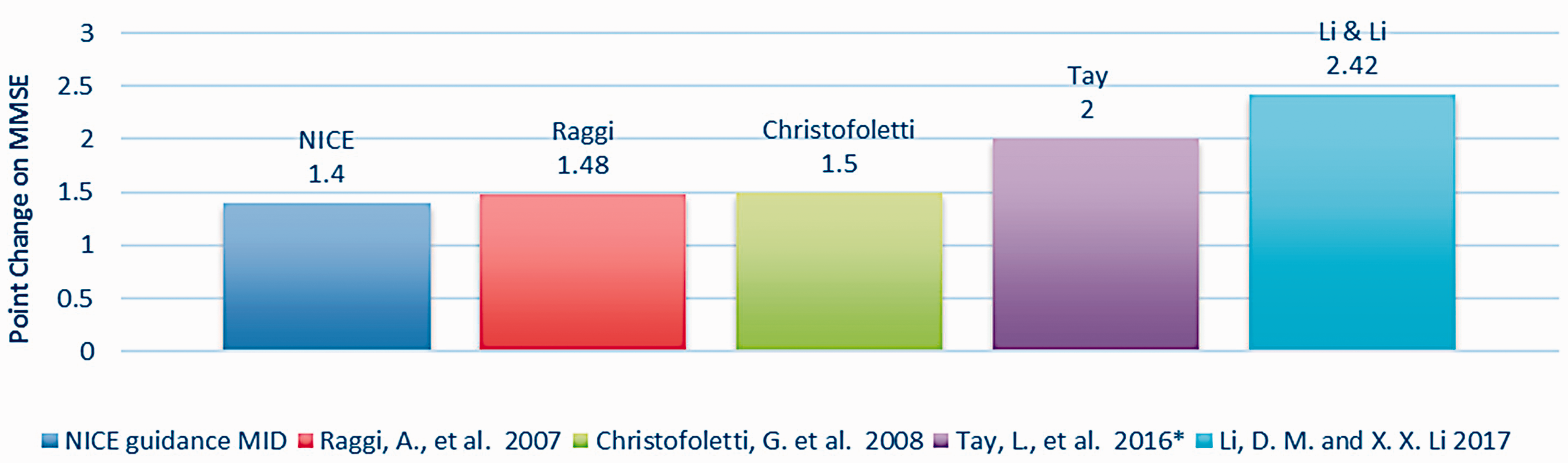
Evaluating group study MMSE change according to NICE guidance on MID.
Cognitive outcomes – Efficacy.
ABCD: The Arizona Battery for Communication Disorders of Dementia; ADAS-Cog: Cognitive subscale of the Alzheimer’s Disease Assessment Scale (scoring range 0 to 70, higher scores indicate greater cognitive impairment); ADAS-K: Korean version of Alzheimer’s Disease Assessment Scale; BCSB: Brief Cognitive Screening Battery; CERAD: Consortium to Establish a Registry for Alzheimer’s Disease; CDR: Clinical Dementia Rating; CDT: Clock Drawing Test; CMMSE: Chinese Mini-Mental State Examination; CVLT: California Verbal Learning Test; DSB: Digit Span Backward; DSF: Digit Span Forward; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; GDS: Global Deterioration Scale; KADLS: Katz Activities Daily Living Scale; MDRS: Mattis Dementia Rating Scale; MFI: phagocytosis index; MMSE: Mini Mental State Examination; MMSE-K: Korean version of the Mini Mental State Examination; MoCA: Montreal Cognitive Assessment; MODA: Milan Overall Dementia Assessment; NAI: Neuropsychological Aging Inventory; NINCDS-ADRDA: National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association; SISCO SIDAM: a global measure of cognitive performance/impairment; SKT: Short Cognitive Test; TMT: Trail-Making Test; WAIS-R: Logical Memory subtest of the Wechsler Memory Scale – Revised; 7MST: 7-Minute Screening Test; SD: standard deviation (given except where ‘SE’ is specified); SE: standard error.
Findings
Eighteen group studies or case studies out of a total of 26 (69%) reported either statistically significant or meaningful within-group improvements in cognition (Baglio et al., 2015; Bredesen et al., 2016; Burgener, Yang, Gilbert, & Marsh-Yant, 2008; Christofoletti et al., 2008; Coelho et al., 2013; Han et al., 2017; Kang et al., 2010; Kim et al., 2016; Li & Li, 2017; Onor et al., 2007; Oswald et al., 2007; Prokopov, 2010; Raggi et al., 2007; Tay, Lim, Chan, Ali, & Chong, 2016; Yoon et al., 2013). Stability of scores or an attenuation of decline was reported in six group studies (Arkin, 2007; Graessel et al., 2011; Ibarria et al., 2016; La Rue et al., 2015; Maci et al., 2012; Viola et al., 2011). Two group studies, Serdà i Ferrer and del Valle (2014) and Vicente de Sousa et al. (2017) reported no cognitive improvement and continual decline. Cognitive outcomes are summarised in Table 6.
(1) What is the evidence for what works and does not work (the predictors of efficacy)?
The ES of each intervention group was evaluated. Cohen’s ES, d, was used to calculate pre–post comparisons (Cohen, 1988). In dementia studies the tendency is for cognition in a control group to decline in the absence of an intervention. Studies that report an ES between groups at the end of the assessment period may therefore show inflation, in part from the declining controls, and consequently give a misleading over-estimate of the effect of the specific treatment or intervention. Therefore, we first chose to examine the within-group ES (Figure 2) to discern which of the interventions worked, in a calculated score uninflated by the tendency to deteriorate in the control group. Using accepted criteria (0.2 – small, ≤0.5 – medium and ≤0.8 – large) (Cohen, 1988), this analysis indicated that of the 17 studies suitable for ES, two studies had a large ES (Christofoletti et al., 2008; Li and Li, 2017), four had a medium ES (Onor et al., 2007; Raggi et al., 2007; Tay et al., 2016; Yoon et al., 2013) and five had a small ES (Burgener et al., 2008; Graessel et al., 2011; Han et al., 2017; Ibarria et al., 2016; La Rue et al., 2015). A further six studies showed a negative ES reflecting the disease course. Interestingly, one study which reported that, based on conventional inferential testing, ‘global cognition did not improve through treatment’ had the largest ES (d = 0.909) (Christofoletti et al., 2008).
The following four group studies were excluded from this analysis for the following reasons. Coelho et al. (2013) used the Frontal Assessment Battery (FAB) which was designed to assess frontal lobe function and to distinguish frontal lobe dementia from AD (Slachevsky et al., 2004). Kim et al. (2016) provided a graph showing positive mean score change. Kang et al. (2010) provided median change scores and Baglio et al. (2015) provided no measures for within-group analysis.
Of equal importance in interpreting change is the minimal clinically important difference (MCID) (Burback, Molnar, St John, & Man-Son-Hing, 1999), defined as the smallest change in an outcome that a clinician would identify as important. The ADAS-Cog is a 70-point scale on which lowered scores indicate improvement. A change of 4 points or more on the ADAS-Cog scale would define a MCID for mild to moderate dementia (Huntley, Gould, Liu, Smith, & Howard, 2015). Again, looking specifically at the intervention group data, two studies reported improvement on the ADAS-Cog (Graessel et al., 2011; Han et al., 2017) but not clinically important.
The MMSE is a 30-point scale on which a higher score indicates improvement and a change of at least 3 points is considered clinically important in North America (Burback et al., 1999; Qaseem et al., 2008). To assess studies with the National Institute for Health and Care Excellence (NICE) guidance in the UK (NICE, 2018) a Minimal Important Difference (MID) of 1.4 is also evaluated. Accordingly, four group studies (Christofoletti et al., 2008; Li & Li, 2017; Raggi et al., 2007; Tay et al., 2016) (Figure 3) reported change in mean MMSE above the NICE threshold of minimal important difference (Figure 3). However, no intervention group outcomes from the group studies reached an MID of 3 points on the MMSE.
These four, plus two more group studies were identified in the Effect Size analysis (Figure 2) as having Good or Medium efficacy. Table 7 shows these Top Six studies and the modes and methods they used.
Top Six most effective group studies.
Two case studies (Bredesen et al., 2016) (P6 and P7) reported change in mean MMSE above the NICE guidance on MID. Both case studies also exceeded a non-UK MID of 3 points. A further case study (Bredesen et al., 2016), Patient 9, reported an MID on the MoCA which is significantly positively correlated (Stewart, O'Riley, Edelstein, & Gould, 2012) and translatable to the MMSE for comparison (Trzepacz, Hochstetler, Wang, Walker, & Saykin, 2015). Patient 9 showed clinically important improvement according to NICE guidance (Figure 4).
Evaluating case study MMSE (or MoCA) change according to NICE and non-UK guidance on MID.
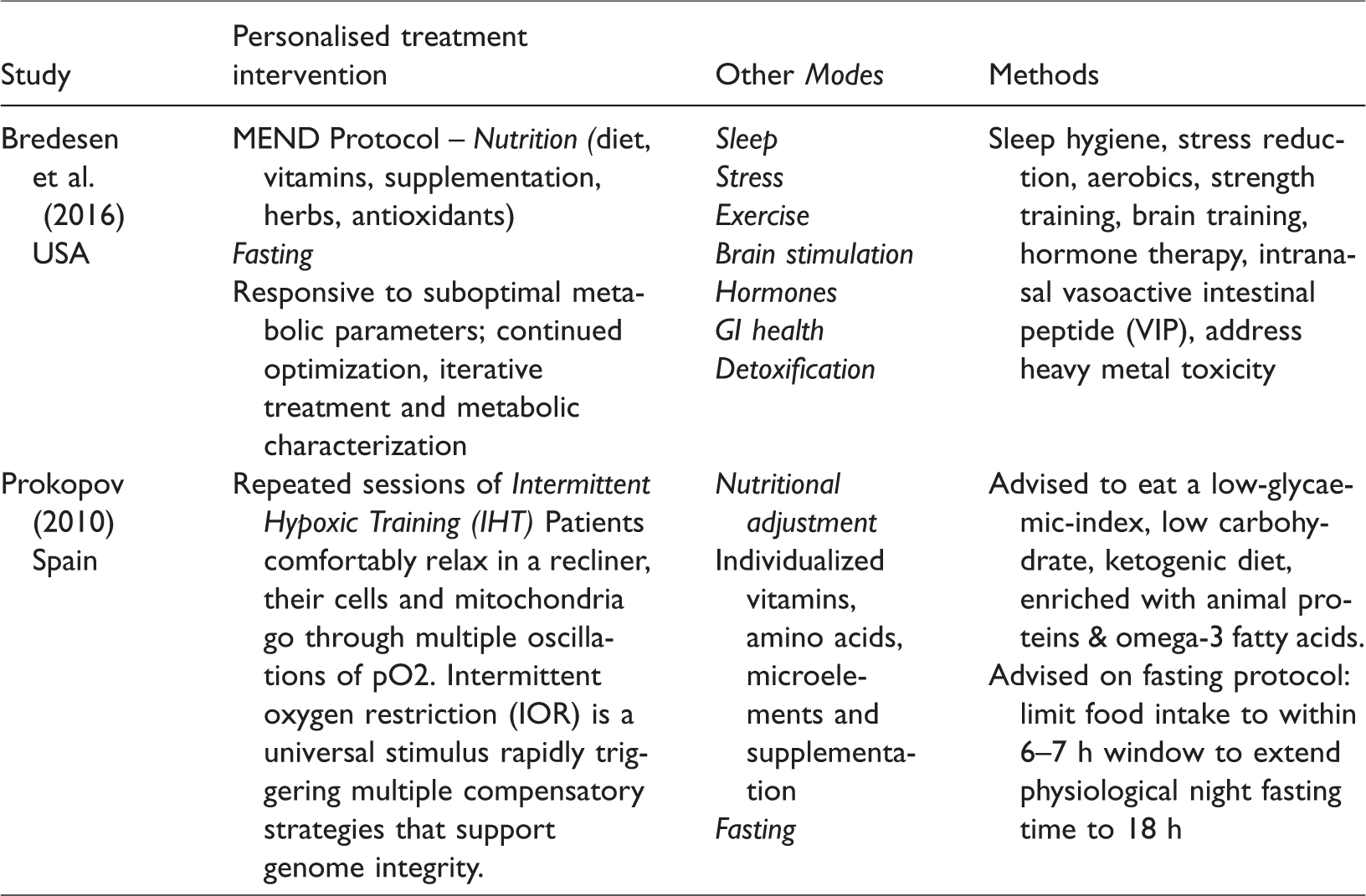
Besides the three case studies that used MMSE or MoCA in Figure 4 below, two more were reported in the included papers (Bredesen et al., 2016; Prokopov, 2010). When providing personalised N-of-1 treatment, the efficacy of the multimodal interventions was determined by the clinician through a range of assessment indicators, including MRI, FDG PET scans, CVLT-IIB and numerous metabolic and neuropsychological tests. These reported clinically important pre–post-test results for these two patients (Table 8).
Case studies – Cognitive assessments showing clinically important differences.
These case studies utilised the following modes and methods (Table 9).
Case studies – Modes and methods.
(2) Does multimodal matter?
Nine of the 11 studies showing positive cognitive ES (Figure 2) used three modes rather than two, indicating that more may be better. However, as well as the number of modes, the number of methods used to carry out the modes is multiple and diverse. For instance, Ibarria et al. (2016) initiated an Integral Psychostimulation Program (IPP) integrating cognitive, motor and mood-related rehabilitation and stimulation for cognitive functions. They also used exercise (active and passive gymnastics, personal & spatial orientation, motor coordination and body language), music therapy, relaxation, occupational activities to maintain ADLs, expression, creativity, board games and caregivers involvement. Also, the focus or general character of the intervention overall (was it largely cognitive or physical?) helped determine the effectiveness of the cognitive mode. For example, five out of six studies which showed a negative ES were predominantly physical with other modes in addition. Conversely, 8 of the 11 studies which showed a positive ES were predominantly cognitive with other modes in addition.
(3) What is the evidence for different groups of people with dementia (early, mid or late stage)?
Analysis of the cognitive impairment levels of participant groups did not indicate that interventions necessarily work any better for the least or the most impaired. In the six papers with the highest ES there was a range of dementia from mild to severe. In fact, the second best ES was achieved by Li and Li (2017) with a participant group that was 82% moderate to severe dementia in a nursing home. Arkin (2007) found that most early stage participants tended to improve or maintain on test scores, but occasionally a person in the moderate stage did also. Graessel et al. (2011) showed that in nursing homes the ESs for the intervention were greater in the subgroup of patients (n = 50) with mild to moderate disease. Raggi et al.’s study (2007) of 30% mild, 40% moderate and 30% severe patients concluded that subjects in all stages of dementia showed some improvement from attending the treatment programme. Kim et al.’s (2016) study of nursing home residents reported improvement in moderate to severe AD taking physical exercise (Kohzuki Exercise Program – KEP) along with a multi-component cognitive programme (MCP), (KEP + MCP).
Predictably, Serdà i Ferrer and de Valle’s (2014) study reported that the magnitude of the effects of the programme diminished progressively in relation to the stage of the disease. Indeed, the most significant and continuous reduction occurred in the dimension of patient cognitive capacity among day hospital patients with mild (29.69%), moderate (31.25%) or severe (39.06%) dementia. Hence, the staging of dementia among the participants seemed to have no direct bearing on the ES of the intervention group, but perhaps had more to do with the level of optimisation of the intervention for participants in different stages of dementia. Given the available study data, the potential for different types of dementia was inconclusive.
(4) What are the strengths and limitations of different study designs used in testing these outcomes?
The most clinically important cognitive differences were achieved in case study designs. Meanwhile, 7 out of 11 group studies with positive ES had a randomised design, whereby the mode was not chosen specifically for the individual but for the cohort generally. However, this did not prove detrimental to the outcomes, as a personalised approach was also evident in the most effective group interventions. For example, Christofoletti et al. (2008), Li and Li (2017), Raggi et al. (2007) and Tay et al. (2016) tailored interventions or individual sessions to the person with dementia, whilst Burgener et al. (2008), Ibarria et al. (2016), La Rue et al. (2015) and Onor et al. (2007) added components of caregiver involvement.
In the design of the sessions (minutes per week, # of sessions), a roughly inverse pattern could be found between time and effectiveness. The time commitment required of participants in the six most effective studies was 24 weeks or less. Some studies requiring a greater time commitment were less effective. For example, Graessel et al. (2011) had the most sessions (288), Oswald et al. (2007) had the most weeks (52) and Ibarria et al. (2016) had the greatest total time commitment of 979 hours (approximated, see Table 3). Because of the nature of a cross-over trial, the length of wash-out period and the relatively short intervention time of eight weeks in Han et al. (2017) they acknowledged that these may have limited the effect of the Multimodal Cognitive Enhancement Therapy (MCET). Since they achieved a small ES for the dementia subgroup, perhaps the overall ES was only hindered by the study duration, and that a longer study might have been more efficacious.
Analysis of the settings found that three of the top four most effective studies were carried out in nursing homes or a long-term care hospital, whereas 83% of the studies with a negative ES were carried out in a day care, day hospital, university facility or research centre with people who attended for sessions but lived at home. One further point about study design, Serdà i Ferrer and de Valle’s (2014) study suggested a mixed method design may be more appropriate for older participants lacking high levels of literacy.
(5) What are the strengths and limitations of outcome measures?
Choice of outcome measures varied across studies (see Table 1) which possibly facilitated statistically significant findings. Also, some screening tests, such as the MMSE have well-reported weaknesses (Stewart et al., 2012; Verma et al., 2015). However, there was a value to using well-recognised instruments as it facilitated at least some quantitative analyses (Figures 2 to 4). The studies were largely heterogeneous and the requirements for individual studies varied depending on the intervention tested. Therefore, conclusions on the relative merits of different measures were not possible and further work is needed specific to multifactorial studies.
(6) What is the evidence for theory on the likely process of change for each mode of intervention?
Of the 10 modes utilised in the studies, other than those modes highlighted in the Introduction (i.e. exercise, especially high-intensity exercise, CS and nutrition), evidence is lacking for primary studies correlating efficacy of these various modes to improved cognition for people with dementia. However, Alzheimer’s disease has been shown to involve multiple pathophysiological factors for which physical, mental activities and exercises normalise and regulate cerebral blood flow (CBF) (Aliev et al., 2013) and promote the production of brain derived neurotrophic factor (BDNF) which correlates with neuroplasticity in the hippocampus (Colcombe et al., 2006; Erickson et al., 2011). Aerobic exercise in particular is associated with increased neurogenesis and angiogenesis, as well as the production of BDNF and other growth factors involved in neuroprotection such as the promotion of cell survival, neurite outgrowth and synaptic plasticity (Cramer et al., 2011) and protecting deoxyribonucleic acid (DNA) from oxidative damage and rejuvenating the mitochondria (Garatachea et al., 2015). Cognitive activity has increased neuronal plasticity and cognitive reserve, a lack of which hastens cognitive decline in dementia (Panerai, 2016). ‘The changes we saw in fMRI support the notion that even the AD brain still has plasticity resources and can react to positive environmental stimuli,’ said Baglio et al. (2015).
Stress relief, meditation and relaxation lowered cortisol, decreased inflammation and increased BDNF. The effect of meditation caused significant changes in CBF (Khalsa, Amen, Hanks, Money, & Newberg, 2009). Neurotoxins such as heavy metals and mould have been associated with cognitive decline and subsequently removed through detoxification with for instance sauna or chelation (Bredesen, 2016; Shoemaker & House, 2006). Hormone balancing optimises thyroid function and regulates sex hormones. Sleep disturbances and disorders may disrupt neuronal pathways, impair working memory, lead to cognitive impairment and are a significant risk factor for dementia (Miller, 2015).
Because DNA methylation, histone modifications, and microRNAs are the principal epigenetic mechanisms involved in AD pathophysiology, some argue that nutrition can prevent the onset of dementia and attenuate cognitive decline, especially if combined with brain exercise and physical training (Athanasopoulos et al., 2016). Dietary factors can complement the action of exercise at the cellular level of energy metabolism and synaptic plasticity (Gomez-Pinilla, 2011). Given the growing evidence base on the process of change for the above interventions, multimodal approaches that target several dysfunctions simultaneously, and that emphasize nutritional, botanical and stimulatory therapies may offer the most benefit (Wollen, 2010).
(7) What are the strengths and limitations of different evaluation tools used to assess the effectiveness of MNPIs on improving cognitive functioning?
In Kim et al. (2016), nursing home participants with moderate-severe AD did not improve significantly after six months in the KEP + MCP group compared to the MCP group on the MMSE and CDT. However, the ADAS-Cog score showed significant improvement at the same time point, which may relate to its greater sensitivity to detect change. The MMSE is widely criticised for this relative lack of ability. Indeed, Ibarria et al. (2016) also reported cognition as stable on the MMSE but slightly declined on the ADAS-Cog. Two studies used the FAB (possible score 18, higher indicates improvement). With so much heterogeneity among the studies the strengths and limitations of different tools are unclear.
(8) What is the effectiveness of different modes of delivery on the effectiveness of MNPIs for improving cognitive functioning for people with a diagnosis of dementia?
Different modes may take more time to register an effect than others. For example, Vicente de Sousa et al. (2017) investigated a nutritional supplementation psychomotor rehabilitation programme (NSPRG) lasting 21 days. But cognitive benefit might require a longer intervention, as evidenced by the improved test scores found in 91% (N = ?) of analysed studies in this review, all of which exceeded 21 days. Some of the most effective group studies included individualised aspects to their interventions.
Christofoletti et al. (2008) (d = 0.909) provided tailored physiotherapeutic sessions concentrating on specific kinesiotherapeutic exercises that stimulated strength, balance and cognition. This study observed an attenuation of cognitive decline, in particular verbal fluency and executive function. Li and Li (2017) (d = 0.497) provided 30-minute individual sessions twice a week according to their likes and preference, such as singing practice of favourite folk songs. Tay et al. (2016) (d = 0.457) gave tailored individualised 30-minute activities. A further personalised approach was found in Raggi et al. (2007) (d = 0.245) which illustrated a comprehensive rehabilitation programme in a specialised hospital unit. Although the study lasted 17 months overall, the mean stay in the hospital was only 26 days, beginning with a thorough investigation including neurological examination and laboratory analyses to inform each person’s integrated, supportive and individualised treatment.
In summary, this review found multimodal intervention research predominantly in Spain, Portugal, USA, Italy and Asia. Group studies commonly utilised 2–3 modes and occurred in long-term care, day care, clinic, hospital, university facilities or in the community. A very small number of case studies were found, utilising up to nine modes. Study duration varied from three weeks to four years and sessions lasted from 20 minutes to 8 hours. Time commitment required of participants in the six most effective studies was 24 weeks or less. People with all stages of dementia participated and studies occasionally involved caregivers.
Discussion and implications
The results of this review have important implications for dementia treatments, as 92% (24/26) of included studies demonstrated statistical improvement, stability or attenuation of decline. Studies that personalised the multimodal approach by identifying individual needs of participants or patients and tailoring interventions accordingly, resulted in the greatest ESs. These findings should encourage extensive research of complex multimodal interventions for dementia, including cognitive, physical or psychological therapies alongside novel ones such as brain stimulation (Raggi, Tasca, & Ferri, 2017), oxygen therapy, detoxification, stress reduction, sleep hygiene, hormonal health, fasting and nutrition. Some considerations have emerged:
Length of study. A multimodal or ‘complex’ intervention contains interacting components requiring specific design guidance (Craig et al., 2013). One difficulty in designing multimodal interventions is accounting for the varying timeframes within which different effects may impact individuals. Because the shortest study (Vicente) had one of the smallest ESs and four of the longest studies showed maintenance of cognition, we investigated whether study length was an indicator of ES. We found that the length of intervention was not an indicator of effectiveness as evidenced by the results of Raggi, Han, Tay, Li and Li and Kang, all of which lasted four months of less. As Vicente was predominantly a nutritional intervention, which also assessed the effect on cognition, it is not surprising that a short study length would have proved unproductive cognitively. Similarly, in the case of Onor et al. (2007), there was a ‘lack of improvement of cognitive function … probably due to the short duration of the rehabilitation program’ (p. 268).
Effect size versus benefit. Reviewing multimodal studies by looking at a measurable gain in only one mode such as cognition, can lead to erroneous assumptions about the success of the research and indeed the benefits of the intervention for the participants with dementia. An example of this is Arkin’s study (2007), which scored lowest on ES of the intervention groups. In spite of this, maintenance of function, or improvement on several discourse measures, was achieved by the programme’s 11 first-year participants. This study was also successful in reducing the annual rate of decline between 3rd and 4th year to just 1 point, which was significantly less than the CERAD comparator group. Therefore, a small amount of decline can be a benefit when compared to rapid decline in the untreated population.
Holistic approach. Since dementia is multifactorial in terms of the numerous risk factors involved, then a holistic approach to treatment would perhaps stand the best chance of addressing a range of symptoms. This is the premise for multimodal interventions, at least as they are currently designed, which cannot be unpacked to determine which element helped to delay or reverse cognitive decline. Positive emotions, enjoyment, creativity, belief, even spirituality can contribute to cognition as much as exercise and diet for example. Onor et al. (2007) reported that socialization itself can lead to improvements, and ‘programs that take a more holistic approach to the individual are more effective than those focusing on cognitive rehabilitation alone’ (p. 270). Maci et al. (2012) echoed this with their integrated approach of CS, physical activity and socialisation to slow down affective decline and reduce carer burden.
Assessment tools. Judging from the multiple tools that have been reported one might jump to the conclusion that many tests are administered in hopes of finding positive outcomes to report. However, multimodal studies require numerous tests – a complete battery for each mode. This enables more insight into the various ways the intervention might be helping to improve cognition. But testing can also contribute to participant burden and might even encourage drop-outs. There is thus a pressing need in multimodal research to analyse the strengths and limitations of different evaluation tools.
Recently, Webster et al. (2017) found that cognitive measures such as the MMSE can be distressing and demoralising for people with dementia and their carers who preferred that cognition should be taken in context of previous ability. It was felt that ‘a larger package of specific measures would give a holistic view of an individual and include more detail’ (p. 13) and that timed measures which estimate cognitive processing speed should be considered, along with the recommended validated measures of MMSE and ADAS-Cog. In keeping with this, studies reported a range of testing including CSF biomarkers, blood work, metabolic analysis as well as in-depth narrative assessment. One paper (Oswald et al., 2007) included data from another informant, a questionnaire for nursing staff on the changes in cognitive and functional ability of residents.
For future studies the use of a range of testing relevant to the population sample is recommended, as well as a standardised, free and widely available instrument for pre–post-test assessment. For instance, the CDR global score has been recommended as a staging or impression of change outcome measure in future studies (Webster et al., 2017). The Short Cognitive Test (SKT) has also been known to be ‘more sensitive to subtle changes’ than the MMSE as it is a ‘more comprehensive cognitive assessment battery and takes account processing speed and response accuracy’ (Viola et al., 2011).
Study design – Pharmacology and the Naturalistic. Although this review searched for, selected and focused on non-pharmacological approaches, the advent of disease-modifying drug treatments is near for preclinical and prodromal stages as disease models improve their ability to predict the likely course of dementia (Ritchie et al., 2017). Drug-naïve patients with a diagnosis of dementia are practically non-existent as this review discovered. Therefore, the opportunity arises for collaborative interventions that combine and integrate pharmacology with non-pharmacological treatments as shown in Ibarria et al. (2016). So-called ‘naturalistic’ studies, which follow a group of patients in an outpatient clinic over many months are relevant and informative to clinical practice. Bragin et al. (2012) showed arrest in cognitive decline for 60 months for patients with depression, dementia, physical disability and medical illnesses. Patients were treated with a multimodal intervention specific to their needs, including anti-depressants, cholinesterase inhibitors, N-methyl-D-aspartate (NMDA) receptor antagonists, vitamins and supplements as well as physical and cognitive exercises. This example strengthens the evidence base, informs clinical practice and is relevant to people living with dementia who (1) would routinely be prescribed a dementia drug, and (2) often have comorbidities. Such a patient consequently may benefit from a combined, integrative treatment model, as Bragin et al. (2012) aptly demonstrated.
Terminology. Because innumerable descriptive terms for utilising more than one mode pervaded the intervention literature, an added benefit of this review was to develop the typology described herein. The Typology of Modes and Methods for Dementia Interventions (Online Appendix 2) organises them into a comprehensive and logical structure. This typology enables a systematic evaluation of where a study sits relevant to the extant literature. It also facilitates multidisciplinary comparison of studies as different fields have their own ways of describing modes of interventions. This typology can help to classify research involving multimodal, multicomponent, dual-task, integrative, combined or complex interventions.
Involving people with dementia. There are opportunities in research design and implementation to include participants in a meaningful way. Perhaps one of the reasons why N-of-1 interventions worked so well is the involvement of the patient, particularly by helping to formulate and then agree the treatment approach with the practitioner or researcher. This goes beyond mere consent to participate and freedom to withdraw. This is about collaborative engagement – co-ownership throughout the process. Another paper by Tay et al. (2016) went into more depth about their goal-oriented approach (Chew, Chong, Fong, & Tay, 2015). Cognition goals as well as goals to improve engagement and socialization; reduce caregiver stress; and improve physical function, behaviour and mood were set and 61.8% of participants met them.
Diversity of needs. Groups are complicated by the diversity of needs within them. Serdà i Ferrer and del Valle (2014) found, on the one hand, that advanced age, diverse symptoms, the stage of the disease and the impracticalities of working with a group led to significant and continuous reduction in patient cognitive status. On the other hand, they noted that the improvement in QoL was ‘decisive and groundbreaking’, suggesting that ‘psychological factors may have helped mediate the relationship between exercise and QoL’ (p. 197).
Personalised approach. It is a commonly held belief across the lay population and mainstream media that no disease-modifying treatments for dementia exist (Webster et al., 2017). We have now shown that optimised and targeted interventions can help to address the underlying causes of cognitive decline. The role of neurotoxins, nutritional deficiencies, inflammation and the gut microbiome in neurodegenerative disease (Bland, 2016) can lead to a personalised care plan and enhanced precision of treatment decisions (Galvin, 2017). Moreover, a person’s dementia has a unique etiology which must be understood individually to develop personalized treatment (Pomorska & Ockene, 2017). Likewise, effort must also be taken to add some component of support for individuals in research studies. Should personalised treatments for individuals become more widespread, the learning and application can benefit research as well as patients and residents in long term care (Bodai et al., 2018).
Limitations
The wide diversity of nomenclature in multimodal studies means our search strategy may not be as comprehensive or successful as intended. Interventions not described in-depth may have led to erroneous categorisation. Decisions about which assessment measures to include in order to maintain consistency but also to include as many studies as possible may have weakened our conclusions. Lack of response from some authors meant we had to omit some studies from the computational analyses.
Conclusion
Overall, there is some evidence that MNPIs can improve cognitive function in adults with a primary diagnosis of dementia by addressing multiple modifiable risk factors currently understood to contribute towards cognitive decline. In cases where cognitive outcomes were improved, the following seven research components tended to be in place:
At least three modes were utilised and the methods for implementing the modes were multiple and diverse; The general character or focus of the intervention was on cognitive therapies, stimulation, training or rehabilitation, augmented with other modes such as physical, psychosocial, nutritional, etc.; A personalised one-to-one interaction specific to each individual was included which involved engagement, investigation and assessment helping to focus or fine-tune their intervention; Social, logistical or practical support involved caregivers or students, or a general widening of social networks; The degree of a person’s cognitive impairment was not seen as an impediment to intervention but rather was optimised for those with moderate to severe impairment to maximise potential benefits; Study design and outcome measures allowed for the generation of measurable improvement and the timely and meaningful data capture of the results; Interventions leveraged recent advances in our understanding of the underlying causes of dementia and ways to disrupt these neurodegenerative mechanisms through nutrition, fasting, oxygen therapies, stress reduction, sleep hygiene and so on.
The aim of this review was to determine the effectiveness of MNPIs for improving cognition in people with a dementia diagnosis. As research increases in this area, healthcare practitioners will be more able to treat people with cognitive impairment in ways that help to reduce the symptoms and slow the decline by addressing the underlying causes of dementia. Health and social care providers need to be better informed about lifestyle medicine as an adjunct to existing pharmacotherapies in order to improve choices for their patients and service users. It is socially and economically imperative that practice does not fall behind emerging evidence. Current relevant findings on effective treatments may empower and encourage people with dementia and their carers towards personal health through self-care, whilst directing and stimulating research that continually improves clinical understanding and therefore patient outcomes.
Supplemental Material
Supplementary material1 - Supplemental material for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia
Supplemental material, Supplementary material1 for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia by Garuth Chalfont, Christine Milligan and Jane Simpson in Dementia
Supplemental Material
Supplementary material2 - Supplemental material for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia
Supplemental material, Supplementary material2 for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia by Garuth Chalfont, Christine Milligan and Jane Simpson in Dementia
Supplemental Material
Supplementary material3 - Supplemental material for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia
Supplemental material, Supplementary material3 for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia by Garuth Chalfont, Christine Milligan and Jane Simpson in Dementia
Supplemental Material
Supplementary material4 - Supplemental material for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia
Supplemental material, Supplementary material4 for A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia by Garuth Chalfont, Christine Milligan and Jane Simpson in Dementia
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the AIM Foundation.
Supplemental Material
Appendices are available online.
![]() , Geography MA, Architecture PhD) roots his research in therapeutic nature environments. He promotes a holistic approach to dementia treatment in the UK, integrating ‘root cause’ investigations with mainstream NHS practice. RAD:ISH (Research Addressing Dementia: Interventions Supporting Health) will involve neighbourhood food-growing, multimodal activities, social support and education to inspire awareness for emerging evidence; stimulate healing with lifestyle medicine; and nurture human capacity for self-care and healthy ageing.
, Geography MA, Architecture PhD) roots his research in therapeutic nature environments. He promotes a holistic approach to dementia treatment in the UK, integrating ‘root cause’ investigations with mainstream NHS practice. RAD:ISH (Research Addressing Dementia: Interventions Supporting Health) will involve neighbourhood food-growing, multimodal activities, social support and education to inspire awareness for emerging evidence; stimulate healing with lifestyle medicine; and nurture human capacity for self-care and healthy ageing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.