
Abstract
Self-management support for people with dementia is important to help them and their family caregivers to cope with challenges in daily live. Insight into the effects of self-management support interventions on people with dementia is however lacking, despite existing relevant systematic reviews. We therefore conducted a meta-review of relevant systematic reviews, following the PRISMA statement. Systematic literature searches were conducted in PubMed, CINAHL, the Cochrane Library, Embase and PsycINFO. The searches were done in December 2015, and all relevant references until then were taken into consideration. No conclusions about the effects of self-management support interventions on people with dementia could be drawn. Recommendations for future research and practice include that self-management support interventions and effect measurements should be wider in scope than psychological well-being.
Introduction
Living with dementia presents a huge challenge both to the person with dementia themselves and to their family caregivers. Dementia leads to severe cognitive problems, changes in mood and behavior, and changes in the relationship with the partner and members of their social network (e.g., Milano, Saturnino, & Capasso, 2013; Spalletta et al., 2010). The care is often a considerable burden on persons directly involved, not just physically but also emotionally and because it affects their social lives (e.g., Peña-Longobardo and Oliva-Moreno, 2015; Torrisi et al., 2017).
Self-management is therefore important both for the person with dementia and for their family caregivers in dealing with dementia and the consequences for their daily lives. Following the definition of Barlow, Wright, Sheasby, Turner, and Hainsworth (2002), we define self-management as “the individual’s ability to manage symptoms, treatment, physical and psychological consequences and life style changes inherent in living with a chronic condition.”
However, self-management is far from being a matter of course for people with dementia. They may need support with their self-management, for example, from health care professionals or in the form of eHealth, in the sense of dementia-related information and/or support with the aid of computers or related technologies. Yet up till now there has not been an overview of the effectiveness of the available interventions for self-management support in people with dementia, despite of existing relevant systematic reviews. We have therefore conducted a meta-review of these existing systematic reviews. However, it became clear during the analysis for the meta-review that it is too soon to draw conclusions on the effects of self-management interventions on people with dementia. Nevertheless, the meta-review gives some interesting insights into the kind of interventions being used and provides recommendations for future research and practice. This brief research paper presents the results of the meta-review.
Methods
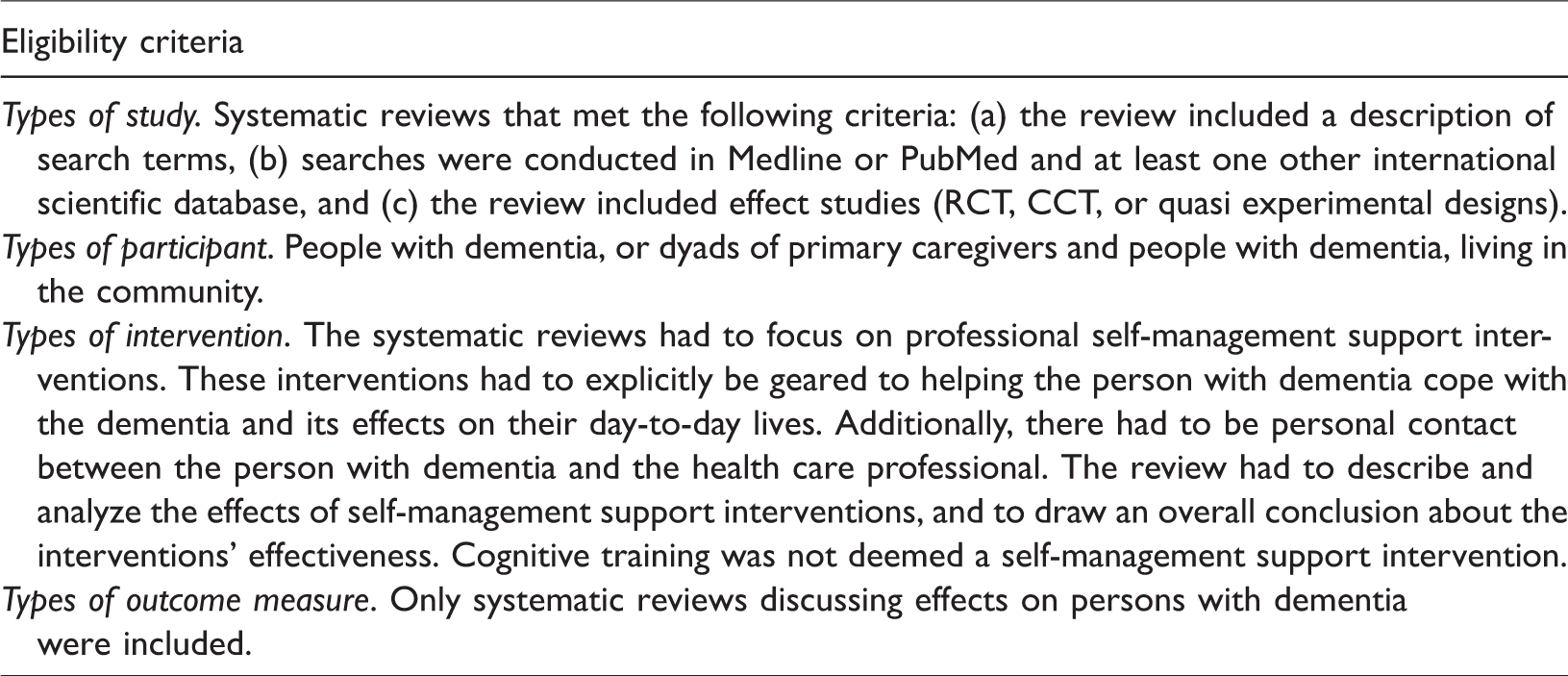
We conducted a meta-review, in the sense of a systematic literature study of existing relevant systematic reviews. We followed the PRISMA Statement for systematic reviews (Moher, Liberati, Tetzlaff, & Altman, 2009) wherever possible, as incorporated in a protocol drawn up in advance. The reviews had to deal with self-management support in dementia, in which the effects were measured at the individual patient level. Table 1 summarizes the specific inclusion criteria.
Inclusion criteria for the meta-review.
Search strategy and sources
Systematic literature searches were conducted in PubMed, CINAHL, the Cochrane Library, Embase and PsycINFO in December 2015. First, a sensitive search strategy was developed for PubMed/Medline. This was then adapted for use in the other databases. All publications up to December 2015 were taken into consideration, regardless of the publication language.
Study selection
A two-step procedure was used to identify references for inclusion. First, the titles and abstracts of the references that resulted from the database searches were checked to see whether they satisfied the inclusion criteria. One reviewer (JGH) screened all the references. The second reviewer (ALF) then independently screened a 10% random selection. The first reviewer proceeded individually if the level of agreement (Kappa) was ≥0.60. If enough information could not be obtained from the title and abstract, those references were taken to the next step of the selection process. In this second step, the full texts of the references selected in the first step (including the references with insufficient information in the title and abstract) were independently screened by the two reviewers. A third reviewer (RV) was consulted if the first and second reviewer did not agree.
Methodological assessment
After the second selection step (see before), the methodological quality of the reviews was determined with the Quality Assessment Checklist for Reviews developed by Oxman and Guyatt (1991). Reviews with a score of 2 or less were considered to be of “low quality” and were subsequently excluded.
Results
The flow chart in Figure 1 shows the number of studies assessed, excluded, and included at each stage of the selection process.
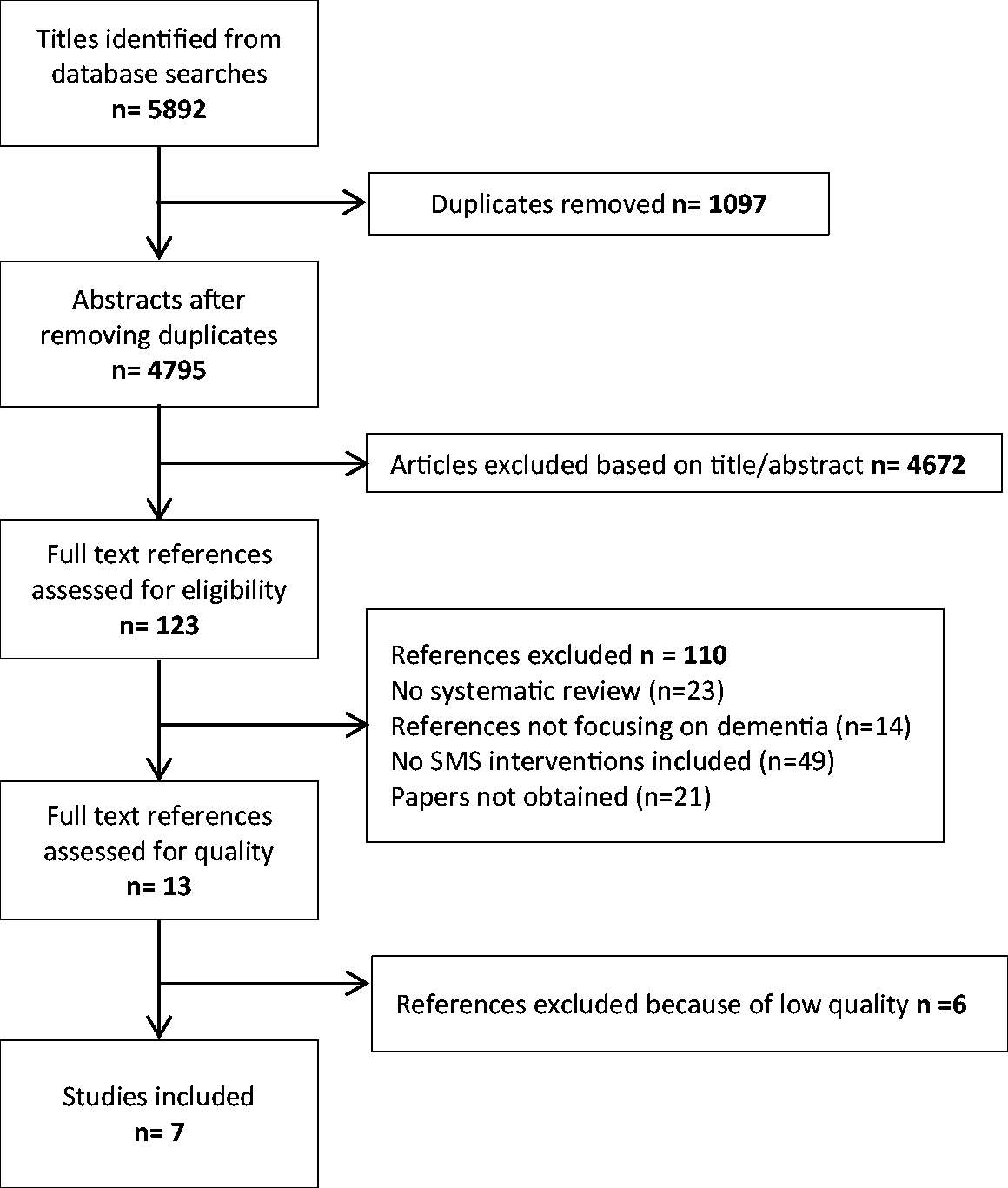
Flow chart of the study selection.
In the end, seven reviews were found that satisfied all the inclusion criteria (Cooper et al., 2012; Corbett et al., 2012; Orgeta, Qazi, Spector, & Orrell, 2015; Reilly et al., 2015; Spijker et al., 2008; Van’t Leven et al., 2013; Zabalequi et al., 2014). One review was identified to have “major flaws,” based on a quality score of 3.0 (Corbett et al., 2012). Three reviews received a quality score of 4.0 (Zabalequi et al., 2014), 5.0 (Cooper et al., 2012), or 6.0 (Van’t Leven et al., 2013) reflecting “minor flaws.” Three reviews received a quality score of 7.0 indicating that they met all quality requirements of the Quality Assessment Checklist for Reviews (Orgeta et al., 2015; Reilly et al., 2015; Spijker et al., 2008). Tables 2 and 3 show the key features of these seven reviews.
General and methodological characteristics of the reviews that were included.
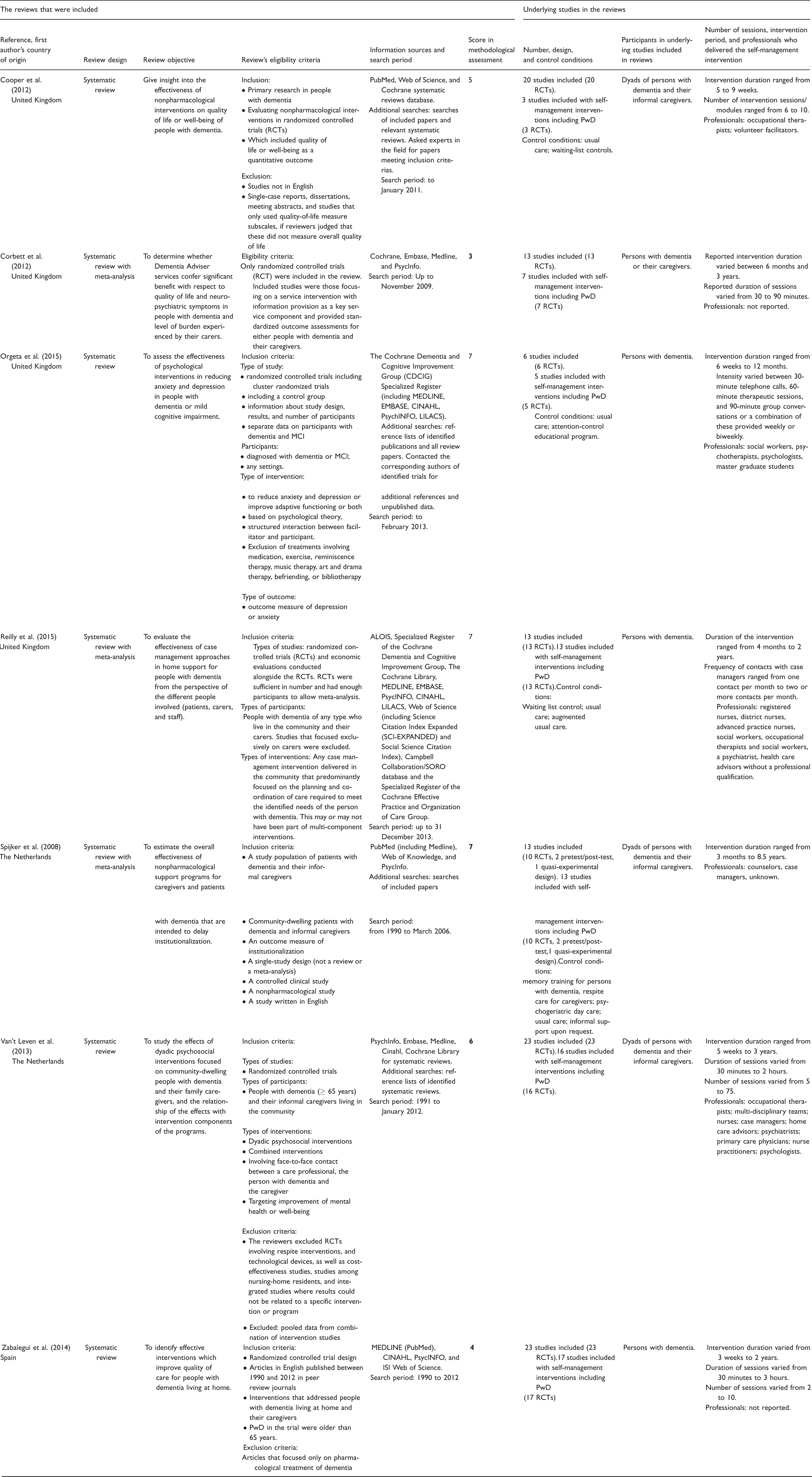
PwD: person(s) with dementia; RCTs: randomized controlled trials; MCI: mild cognitive impairment.
Outcome and effects of the reviews that were included.
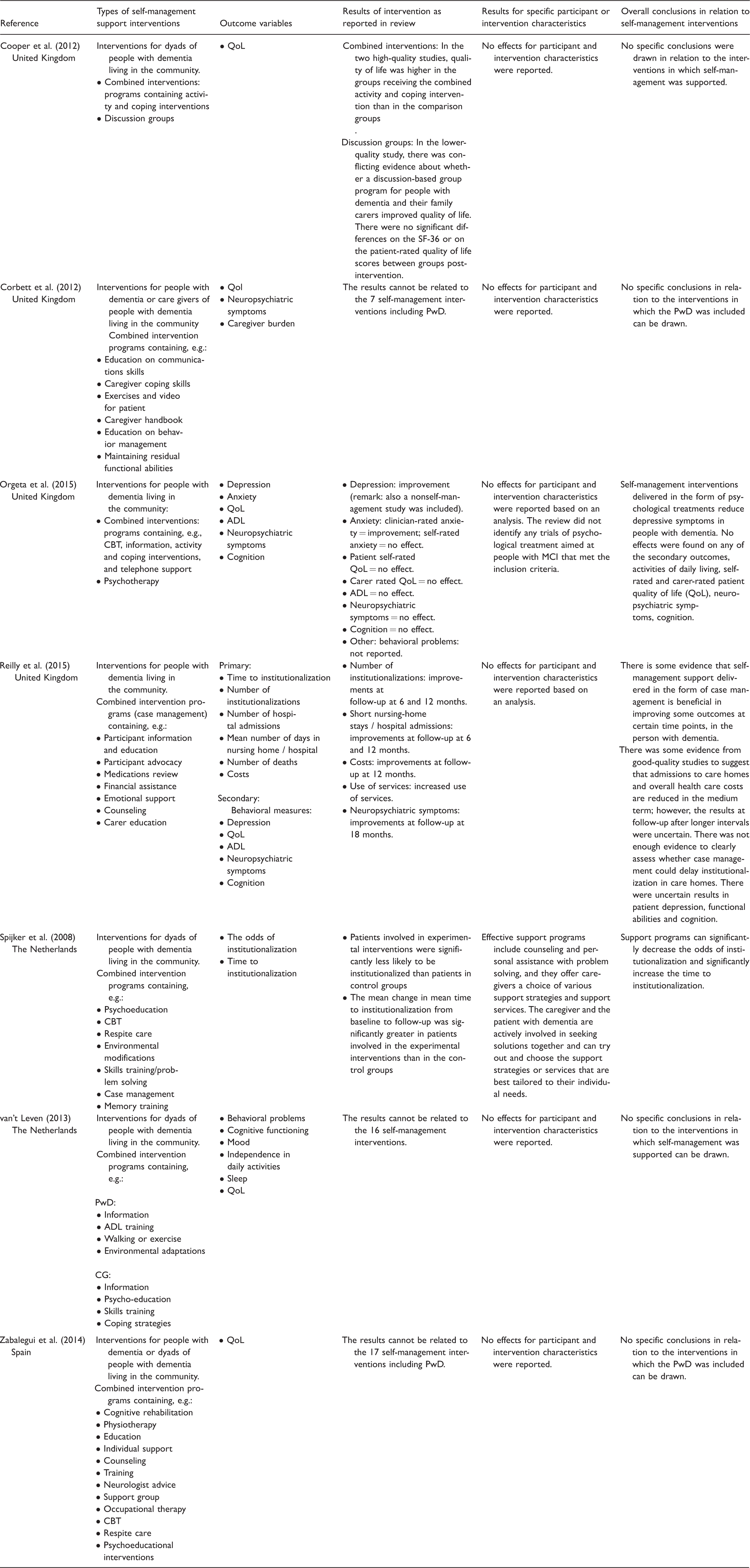
PwD: person(s) with dementia; RCTs: randomized controlled trials; MCI: mild cognitive impairment; QoL: quality of life; ADL: activities of daily living.
Description of the interventions
The term “self-management support” is rarely mentioned explicitly in the seven reviews that were included. However, if the above-mentioned definition based on Barlow et al. (2002) is applied, the selected reviews do indeed consider interventions in which self-management was a central component. Table 3 shows the elements that comprised the self-management support interventions we identified. Self-management support was often aimed at dealing with problems affecting the psychological well-being of the person with dementia. The table also shows that self-management is often combined with cognitive behavioral therapy (CBT) or coping interventions.
Professionals and a focus on managing psychological problems
The interventions were primarily performed by psychologists, occupational therapists, and psychiatrists. Nursing staff were only explicitly mentioned as professionals providing self-management interventions in two of the seven reviews (Reilly et al., 2015; van’t Leven et al., 2013). The interventions focused primarily on managing psychological problems, for example, depression or anxiety. In addition, improvement of quality of life in general and/or postponing admission to a nursing home was often an important aim of the interventions.
Effects
The seven systematic reviews that were included show effects for a number of outcome variables in the person with dementia, for example, depression (Orgeta et al., 2015) and the time to admission to a nursing home (Reilly et al., 2015). However, it was not possible to draw conclusions from this about the effects of self-management support on people with dementia. There are two key reasons for this.
In the first place, self-management support interventions often include other components as well. A clear example of such a combined intervention can be seen in the study by Burgener, Yang, Gilbert, and Marsh-Yant (2008), included in the systematic review by Orgeta et al. (2015). Burgener et al. studied the effects of a support group in which people with dementia learned how to resolve problems in their day-to-day lives, which can be considered as a self-management intervention. However, this was combined with tai chi exercises and CBT (Burgener et al., 2008). The combination of interventions meant that the individual effects of the self-management components could not be distinguished properly.
The second reason was that four of the seven systematic reviews included studies of self-management support interventions, but did not analyze them separately from studies of other kinds of interventions. The review by Cooper et al. (2012) is one such example. It included a study by Logsdon et al. (2010). Logsdon et al. researched the effects of a self-management support intervention in which discussion groups of people with dementia and their family caregivers talked together about how to deal with how dementia impacts social and family relationships and about making plans for the future. In this review, the effects of this self-management support intervention were analyzed together with those of cognitive stimulation therapies that did not include any self-management support components (Chapman, Weiner, Rackley, Hynan, & Zientz, 2004; Davis, Massman, & Doody, 2001; Spector et al., 2003).
Discussion
Despite the fact that the reviews we examined showed positive effects, it is not possible at this point to draw conclusions about the effectiveness of self-management support interventions on people with dementia. A main reason for this is that the self-management support interventions that were studied were often combined with other kinds of interventions such as CBT.
By excluding reviews with low methodological quality (score of 2 or less), we reduced the risk of biased conclusions. Seven of the eight reviews included received a quality score of 4 or more indicating either minor or no flaws, which is also important for providing unbiased, valid results.
However, a limitation was that the reviews did not label the interventions as “self-management support interventions.” Guided by the explicit inclusion criterion that “interventions had to explicitly be geared to helping the person with dementia cope with the dementia and its effects on their day-to-day lives and there had to be personal contact between the person with dementia and the healthcare professional,” we decided whether interventions concerned self-management support. This decision implied subjective judgments.
This meta-review also teaches us that existing self-management support interventions (even if they are not always explicitly denoted as such) focus almost exclusively on the psychological well-being of the person with dementia. Self-management support interventions should however be wider in scope. In addition to psychological well-being, the “relationship with relatives,” “maintaining an active lifestyle,” “techniques to cope with memory change,” and “information” are also important objectives for self-management support interventions (Martin, Turner, Wallace, & Bradbury, 2013). Future interventions should include one or more of these objectives as well in order to provide the best possible support for self-management by people with dementia and those around them.
Accordingly, different outcome measures linked to the above-mentioned objectives should be used in future research on the effectiveness of self-management support interventions for people with dementia. Examples are outcome measures that indicate “the quality of the relationship with family caregivers,” “the number of social contacts,” or “knowledge about dementia.”
Hence, future research is needed on the effects of self-management support interventions on patients. At the moment, more information is available regarding the effects on relatives. A previous meta-review (Huis in het Veld, Verkaik, Mistiaen, van Meijel, & Francke, 2015) described effects of self-management support on informal caregivers of people with dementia, for example, an increase of well-being, stress relieve and more quality of life. However, in current health care in which patients themselves are also expected to execute self-management, it is important to further investigate which kinds of self-management support interventions are effective in particularly people with dementia and which are not.
The meta-review also revealed that self-management support is often provided by psychologists, occupational therapists, and other therapists. It is striking that nurses were only mentioned in two of the seven reviews, since self-management support fits with a core competency of nurses, namely acting as an information and education resource for clients seeking to improve life styles, and who have to cope with changes in health and disability and death (ICN, 2008). Nurses are often in closer contact with the person with dementia than psychologists and occupational therapists, for example, and they accordingly see self-management support as part of their job (Verkaik, van Antwerpen-Hoogenraad, de Veer, Francke, & Huis in het Veld, 2016). Nursing professionals can incorporate self-management support in the regular care that they deliver to people with dementia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study forms part of the research program “NurseSMS—Nurses Self-management Support for people facing progressive incurable diseases” (2014–2019), which is funded by ZonMw; The Netherlands Organization for Health Research and Development, Program “Tussen Weten en Doen.”