
Abstract
Policy and practice guidelines recommend person-centred care to support people to live well with dementia in long-term care. Therefore, staff working in long-term care settings need to be trained in dementia awareness and person-centred care. However, the access to, content of and reach of training across long-term care settings can be varied. Data on current and ongoing access to person-centred care training can form an important component of data gathered on usual care in research studies, in particular clinical trials within long-term care. However, no suitable assessment tools are available to measure dementia awareness and person-centred care training availability, content and reach. This paper describes the development of a training audit tool to meet this need for a usual care measure of dementia awareness and person-centred care training. The ‘Assessment of Dementia Awareness and Person-centred care Training’ tool was based on a review of published person-centred care literature and consultation with dementia and aged care experts. The Assessment of Dementia Awareness and Person-centred care Training tool was piloted in 13 long-term care facilities the UK and Australia, before being used to assess the content of dementia and person-centred care awareness training in 50 UK settings in a randomized controlled trial as part of usual care recording. Following pilot testing, modifications to the Assessment of Dementia Awareness and Person-centred care Training tool’s wording were made to enhance item clarity. When implemented in the randomized controlled trial, pre-baseline training assessment data showed that the Assessment of Dementia Awareness and Person-centred care Training tool was able to differentiate between the training in different long-term care settings and identify settings where further dementia awareness training was required. The Assessment of Dementia Awareness and Person-centred care Training tool was then used as a method of recording data on dementia awareness and person-centred care training as part of ongoing usual care data collection. The Assessment of Dementia Awareness and Person-centred care Training tool is suitable for use by researchers to establish the availability, content and reach of dementia and person-centred care awareness training to staff within research studies.
Introduction
Person-centred care (PCC) is internationally recognised as a best-practice model of care for people with dementia (Bolster & Manias, 2010; Kontos & Naglie, 2007; McCormack & McCance, 2006), and is recommended in international policy and practice guidelines National Institute for Health and Care Excellence/Social Care Institute for Excellence (NICE/SCIE, 2011). Nevertheless, poor quality dementia care in long-term care (LTC) settings remains a serious concern (All-Party Parliamentary Group on Dementia, 2008; Alzheimer’s Australia, 2013; Department of Health, 2010; Orfaly Cadigan, Grabowski, Givens, & Mitchell, 2012; Pot & Petrea, 2013; Zimmerman, Sloane, Heck, Maslow, & Schulz, 2005). Practice and policy guidelines highlight the need for improved dementia training in LTC staff; particularly PCC (All-Party Parliamentary Group on Dementia, 2009; Fossey et al., 2014; Prince, Prina, & Guerchet, 2013). These calls for action have led to increased PCC training for LTCs and the development of PCC training packages by training providers, dementia support groups and government agencies.
A recent review of PCC training packages (Fossey et al., 2014) identified that 80% were of variable quality and 98% were not evidence based, highlighting the need for LTC providers to evaluate the quality and content of training being delivered. It is vital that LTC providers are able to access evidence-based PCC packages to meet the training needs of their staff and to monitor PCC understanding, implementation and reach among their staff, in a climate of high staff turnover (Chu, Wodchis, & McGilton, 2014; ekosgen, 2013; Trinkoff et al., 2013). Aditionally, the drive to deliver better PCC has led to increased research on the application of psychosocial interventions within LTC settings and standardised methods for assessing usual care components that may also impact on outcomes, such as staff exposure to PCC training, are required.
The ADAPT was developed in response to this need within the DCM™ EPIC (Surr et al., 2016) randomized controlled trial (RCT), to allow researchers to monitor the type, content and reach of dementia and PCC awareness training within a usual care (UC) delivery in order to:
Assess baseline levels of dementia awareness and PCC training across study sites to ensure all met a minimum baseline standard of training. Assess baseline characteristics of the LTC settings in the RCT to inform analyses of intervention effectiveness. Track dementia awareness and PCC training over time in the LTC settings in order to assess UC across all study sites.
The ADAPT was informed by a comprehensive literature search and review of existing dementia training audit tools that evaluated the content and use of dementia awareness and PCC training. Only one other tool was identified from the literature. A PCC training audit tool was developed for the PerCEN RCT (Chenoweth et al., 2011, 2014, 2015) to evaluate in detail the dose and duration of PCC training as the trial intervention, thus measuring intervention fidelity. Evaluation of the tool indicated it is suitable for use in studies where detailed information on PCC training and adoption as an intervention is required across sites. As this was not the purpose of collecting data on dementia and PCC awareness training in the DCM™ EPIC RCT, where instead the information was required for the monitoring of UC, the PerCEN tool was not suitable. Since no other PCC training audit tools were identified in the literature, the ADAPT tool was subsequently developed for use in the DCM™ EPIC RCT. This paper reports on the development, testing and use of the ADAPT tool.
It aimed to answer the following questions:
What data items and information should an audit tool collect to assess the availability, content and reach of dementia and PCC awareness training as part of UC monitoring? Is the wording or language of data items clear and understandable to staff working in LTC settings? Is the data required to complete the tool readily available in LTC settings? Can the tool differentiate between settings with regard to the availability, content and reach of dementia and PCC awareness training?
Method
Development of the ADAPT tool
A review of existing published research, theory, audits and curricula covering dementia awareness and person-centred dementia care was conducted, and the key principles, concepts or content were extracted to inform the initial draft of the ADAPT tool. The tool was then reviewed by dementia experts from academia, LTC, other forms of clinical practice, and individuals with a diagnosis of dementia or a relative with dementia: the DCM™ EPIC Trial Management Group. Feedback from these individuals resulted in revisions to the ADAPT tool’s constructs, wording and item structure. Consensus from group members was achieved in developing the final version for piloting ahead of use in the RCT.
The ADAPT tool is structured in three sections: dementia awareness training; person-centred dementia awareness training and higher level dementia qualifications, with sub-sections focusing on completion rates amongst staff members. The first section asks whether the care home provides dementia awareness training, and if so, whether training covers three key areas; knowing the signs of dementia, knowing the different types of dementia and understanding how to communicate with people with dementia. The second section asks whether person-centred dementia awareness training is available, and if so, whether it covers seven key areas: what is PCC; the importance of seeing the person as an individual; understanding what living with dementia might be like; the importance of knowing the person; the importance of supporting daily life choices; understanding all behaviour is meaningful not challenging; understanding how care practices can impact on well-being and the impact of communication and actions on others. For the first two sections, several training packages can be evaluated at once. The final section asks whether anyone within the care home has a higher-level dementia qualification (e.g. BSc in Dementia Studies or equivalent), to assess the potential for leadership of person-centred dementia care in the setting.
Pilot testing of the ADAPT tool
The ADAPT tool underwent pilot testing to ensure that it was suitable for use in LTCs with regards to whether the information required to complete the tool was available within the care home records, or through discussions with key staff; whether the items could be understood by individuals who had not been involved in its development; whether it could effectively differentiate between care homes whose dementia training included different person-centred content; and whether training reach among staff could be assessed. Seven care homes in Wales and six care homes in Australia volunteered to participate in piloting of the ADAPT tool. These care homes were members of two large care providers not involved in the RCT with whom the team members were acquainted and who had expressed an interest in practice development work. As these care homes were recruited from large organizations, staff in all care homes in each group should have received the same training, however decisions around training delivery were designated to the care home manager.
Care home managers were asked to identify a suitable person, usually the person responsible for staff training, to complete the ADAPT tool in their care home and return this to the research team. These staff were asked to consult their care home’s training records, and if possible the appropriate training manuals, to ensure that the review was completed accurately. The review was completed for all 13 homes within one month and returned to the University.
Individuals who completed the assessment were asked to provide feedback on the ease of locating information, whether the language within the ADAPT tool was appropriate and whether they had any feedback on making it more user friendly. Managers were also asked to provide information on whether training was standardized across the care home, whether any categories of staff were not included in the ADAPT tool review, and how easily they were able to calculate the percentage of staff who had completed relevant dementia awareness and PCC training. Modifications to the ADAPT tool were made following this feedback, including changes in language and increased space for the person completing the audit to make notes about evidence to support their decision.
Use of the ADAPT tool in a randomised controlled trial
To ensure all LTC facilities taking part in the DCM™ EPIC RCT had achieved a minimum training standard prior to baseline data collection, an appraisal of their current dementia and PCC awareness training content and reach was conducted using the final version of the ADAPT tool. This was completed approximately eight weeks prior to randomisation to the RCT. LTCs not meeting the stipulated minimum standard were provided with person-centred dementia awareness training prior to data collection commencing. The minimum standard for sections 1 and 2 (dementia awareness training and person-centred dementia awareness training) was that all key subject areas were covered in the training. There was a further minimum standard criterion that at least 20% of all direct care staff had received the training package(s).
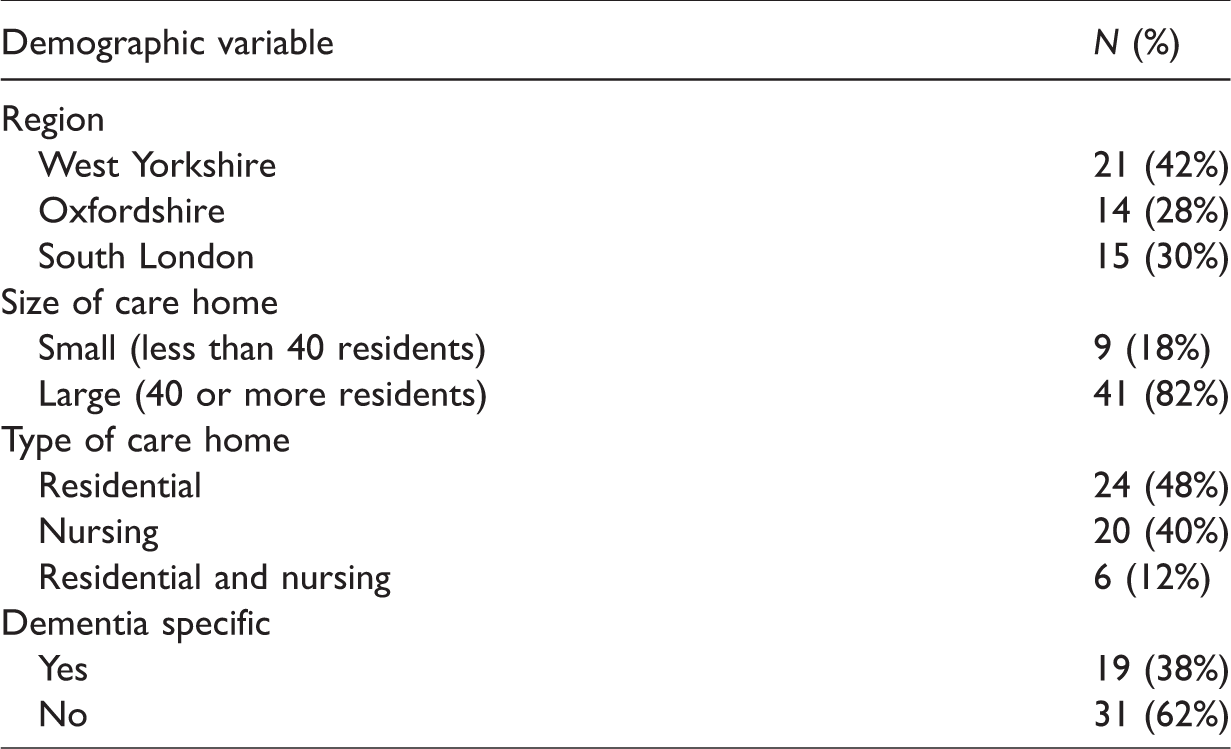
The ADAPT tool was used in all 50 UK LTCs (see Table 1 for an overview of care home demographics) taking part in the DCM™ EPIC RCT. The LTCs were located in three areas of England; West Yorkshire, Oxfordshire and South London. To be eligible for participation, care homes were required to provide care for older adults, have at least 24 people living in the home and recruit at least 10 people with dementia to the study.
Care home demographics.
The ADAPT tool was administered three times in all 50 care homes; pre-baseline to establish whether care homes required additional dementia awareness training before commencing baseline data collection and at 6 and 16 months post care home randomisation (follow-up). At each time point, completion of the tool took approximately 15–30 minutes. Only the ADAPT tool data collected at baseline are reported here.
Results
Use of the ADAPT tool
A researcher from the trial team administered the ADAPT tool with the assistance of a senior staff member from each LTC. Assisting senior staff included the care home manager (n = 45, 90%), the training manager (n = 2, 4%), administrator (n = 1, 2%), company chief operating officer (n = 1, 2%) and head of care (n = 1, 2%). The ADAPT tool data indicated that dementia awareness training was available in 48 of the 50 care homes (96%), and that person-centred training was available in 45 of the 50 care homes (90%).
The minimum standard for section 1 was met by 44 of the care homes (88%). Two care homes did not know whether these areas were covered in the training, two did not cover ‘knowing the different types of dementia’ and two did not cover ‘understanding how to communicate with people with dementia’ (see Figure 1). All six care homes who reported ‘no’ or ‘unknown’ for one or more of section 1 criteria were judged by an independent assessor to need additional dementia awareness training prior to baseline data collection, along with the two care homes that did not have dementia awareness training available.
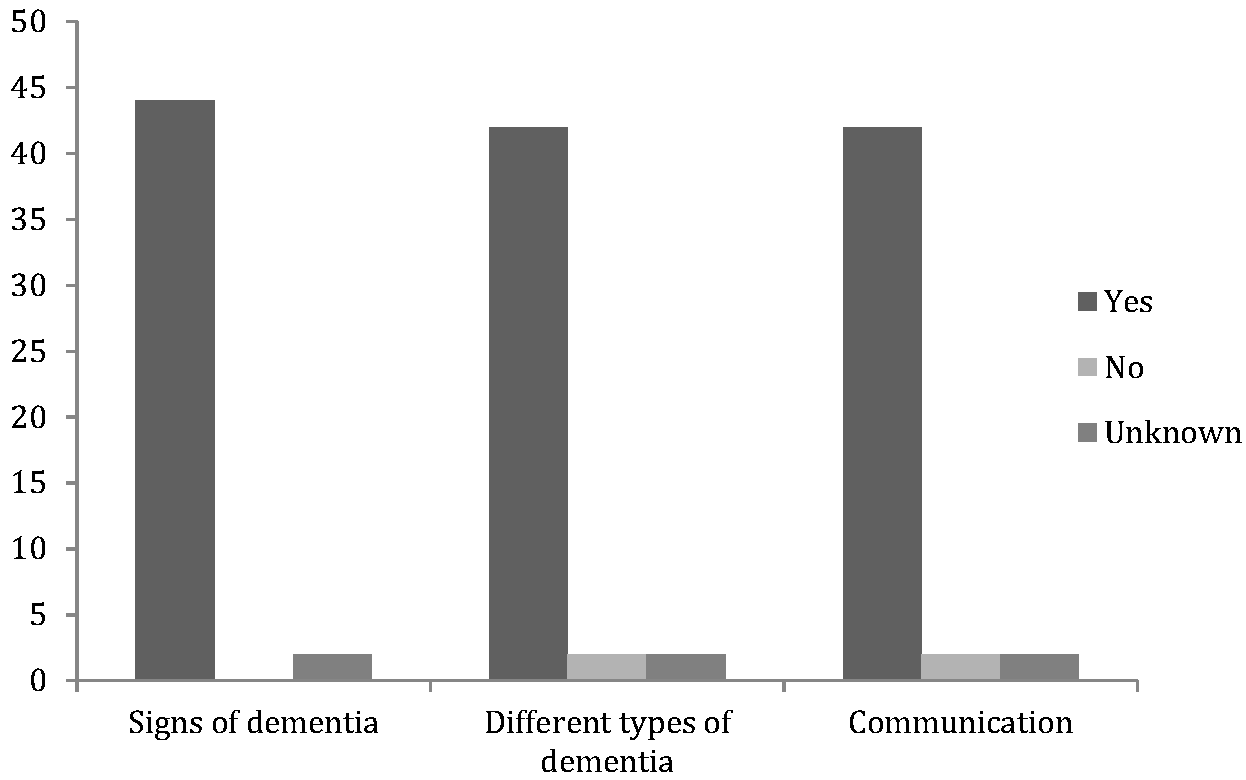
Areas covered within dementia awareness training.
Additionally, four care homes required dementia awareness training as less than 20% of direct care staff members had completed training previously. This particularly occurred in care homes which were part of large aged care provider chains, where the same topics were covered within training programs in all homes, but differed on completion rates by staff.
The minimum standard for section 2 of the ADAPT tool was met by 37 of the care homes (74%), with eight care homes reporting one or more areas as unknown or not covered (see Figure 2). Five care homes stated that they did not have person-centred dementia awareness training. Understanding what it may be like to live with dementia and how care practices impact on well-being were the two areas most frequently not covered in previous training, or were identified as unknown. All eight care homes who reported ‘no’ or ‘unknown’ for one or more of these criteria, in addition to five care homes who reported not having this training available, were determined by an independent assessor to need additional dementia awareness training.
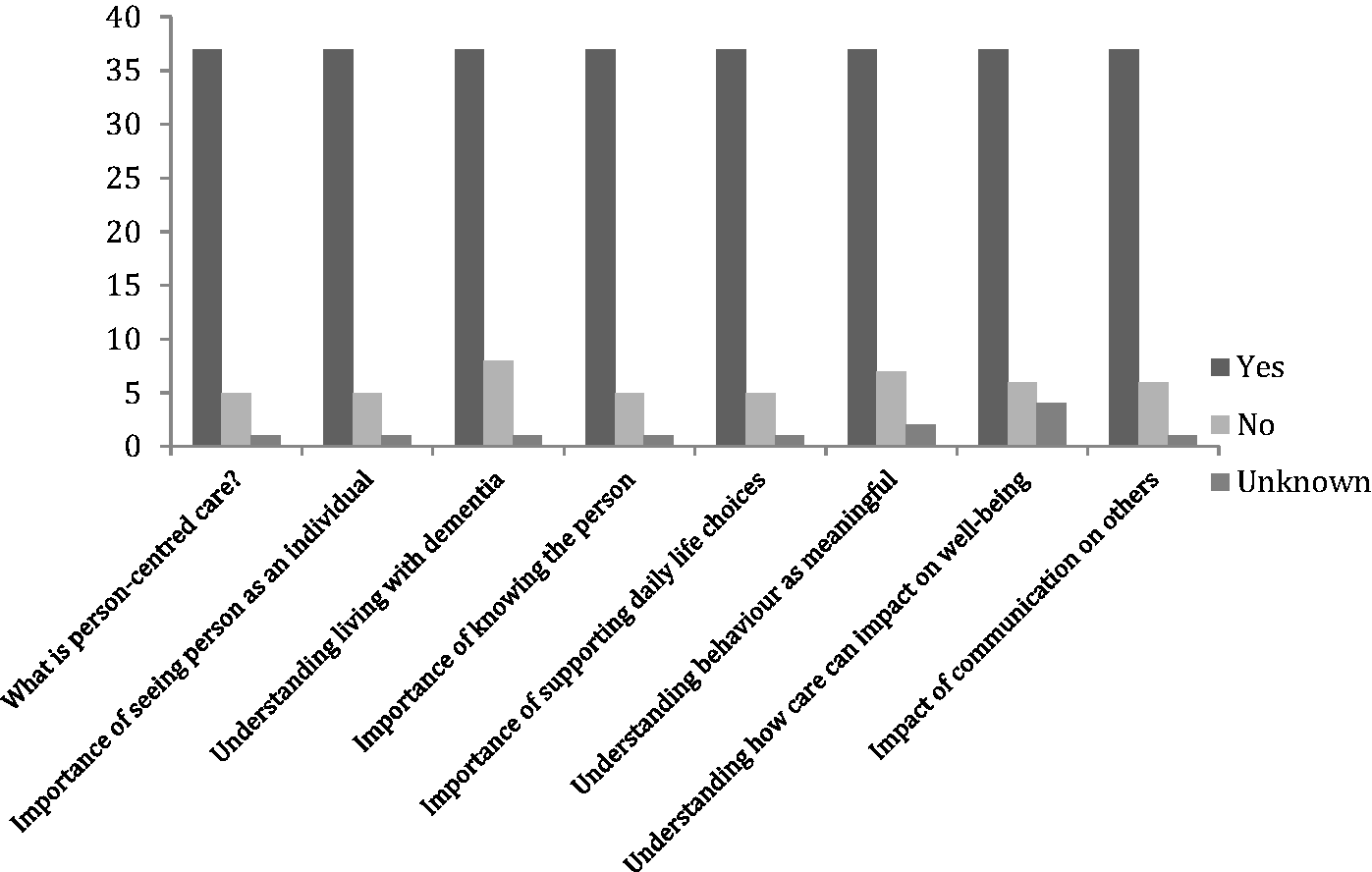
Areas covered within person-centred dementia awareness training.
LTCs who required dementia awareness training based on the section 2 criteria were also more likely to have less than 20% of care staff members who had completed training previously (four care homes in total). These four LTCs were the same as those which met this requirement for section 1.
In addition to the LTCs identified as requiring dementia awareness training as they did not meet the section 1 or section 2 criteria, there was one LTC that met all of these criteria, and had completion rates of 25% across care staff, thus meeting the ‘completion’ criteria. However, this LTC also received dementia awareness training because a senior member of staff and the researcher considered that this would be beneficial since many staff had not received training within the past year. This reflects the ability to use the tool pragmatically where relevant. Since none of the care homes that met all of the criteria had training completion rates above 50%, the ADAPT tool was able to effectively distinguish whether care homes met the minimum required standards.
Section 3 of the ADAPT tool asked whether any staff member had a higher-level dementia specific qualification. Of the 50 LTCs, 26 reported that one or more staff members held a higher-level relevant qualification. This question was supplemented by a free text box, in which the person completing the tool stated the title of the qualification and where it was awarded, providing qualitative evidence of the dementia leadership training staff in the LTC had undertaken.
Discussion
The current paper presented the development, piloting, and use of the ADAPT tool, developed to evaluate dementia awareness and PCC training. When used as a pre-baseline measure of training, it enabled researchers to identify whether staff in LTCs had received appropriate training. There was usually sufficient information available within care home records to enable effective completion of the tool, with only three LTCs reporting ‘not known’ for training content items. The ADAPT tool identified that the majority of participating LTCs provided sufficient dementia and PCC dementia awareness training to their care staff, according to levels determined within the (name removed for peer review) RCT. A total of 13 care homes (26%) received additional training before entering the RCT.
While the ADAPT tool permitted identification of homes that did not provide PCC training at all, there was a degree of regularity across reported data with care homes tending to cover all or none of the content areas, rather than demonstrating variability. This may be due to these content areas being widely accepted as core components of PCC in the UK and therefore, all being covered as standard in PCC training, where it is provided. It may also be due to the sample of care homes that participated in the RCT, with those with a poor/inadequate quality rating as given by the Care Quality Commission, who regulate care home services in England, deemed ineligible. Thus our sample may have been more likely to provide comprehensive PCC training due to their higher quality. Additionally, the ADAPT tool does not provide data on the methods or depth of coverage of core content and so is unable to differentiate between the quality of PCC training provided between the care home sites.
The ADAPT tool was able to differentiate between care homes, even from the same large aged care provider, where the same topics were covered within training, but completion rates differed. This indicated the importance of not only obtaining information about what is covered within training, but also who has completed this training.
Completion of the ADAPT tool was reliant on a senior member of staff having access to training records for all current members of staff. Challenges in completing the tool were faced when training records were difficult to obtain or had not been recently updated. Administration of the tool highlighted the importance of maintaining up to date training records. In England care homes must be able to demonstrate appropriate staff training to the regulation and inspection agency (the Care Quality Commission) and a similar requirement may exist internationally where LTC services are regulated. Therefore, this should support availability of data for the completion of the ADAPT in international research studies. The piloting of the ADAPT tool in Australia suggested this information was readily available in most LTCs there. However, this study did not pilot the ADAPT outside of the UK and Australia and so the availability of such information in other LTC settings internationally remains unclear.
The development and use of the ADAPT tool in an RCT suggests it will be a useful measure of the availability, content and reach of dementia and PCC awareness training for LTC researchers. The tool provides a relatively quick evaluation of training within a care setting, which may represent a single training package or several packages.
Despite being developed earlier, the ADAPT maps well onto emerging training standards and frameworks. For example, the audit tool maps well to the English ‘Dementia Awareness’ level within the Dementia Core Skills Education and Training Framework (Skills for Health, Health Education England and Skills for Care, 2015), and to the dementia awareness and PCC outcomes within the ‘Informed Practice’ level of the Scottish Promoting Excellence Framework (Scottish Government, 2010) The ADAPT has not been developed to replace or measure compliance with a specific training framework or standards. Indeed, given that there are a variety of training frameworks or standards internationally and in countries such as the USA training requirements are set at a state level and are thus extremely varied (Burke & Orlowski, 2015), an audit tool designed to cover all or relate to just a single framework or standard would limit its international applicability. Therefore, the ADAPT is designed to be an internationally relevant tool for use by researchers in auditing dementia and PCC awareness training. Benefits of the ADAPT tool for researchers in addition to its international relevance are, that it is relatively quick to complete, it can collect data on a number of different training programmes, it provides information on the numbers of staff with dementia specific qualifications and provides data on the proportion of staff that have completed dementia and PCC awareness training, thus giving valuable information about levels and reach of training as well as availability and content.
This study has demonstrated the ADAPT tool is suitable for use in research where a minimum standard of dementia awareness training is required, prior to implementation of PCC interventions. It supports setting of a minimum standard and identification of LTCs that fall below this. The ADAPT data can also be used to monitor dementia awareness training provision and reach as part of UC monitoring over time in RCTs and other research studies. The data gathered may be useful for example when adjusting for covariates. In studies aiming to establish the effectiveness of a staff skills development intervention, understanding the baseline levels of access to dementia and PCC awareness training and higher level dementia qualifications among the workforce is imperative to understanding any potential differences between settings before intervention implementation.
There are two limitations in the development of the ADAPT tool. Firstly, LTCs who participated in the research trial were randomly selected, but represented only a sample of those screened and approached to take part in the DCM™ EPIC trial. Therefore, those who agreed to participate in the trial may not provide a representative sample of LTCs, as those with ongoing issues, such as staffing shortages would be much less likely to become involved in the research and LTCs subject to regulatory enforcement were excluded from participation in the RCT. Despite this, the care homes involved in the development of the ADAPT were recruited from three countries (Wales, England and Australia), representing both small and large organisations, as well as dementia specific, residential and nursing care. Furthermore, during the RCT, two care homes were subject to regulatory enforcement notices resulting in admissions bans, demonstrating that the tool can be used within care homes of differing standards. Secondly, alongside a literature review, the criteria used to evaluate dementia awareness training were developed by an expert panel comprised predominantly of UK members and therefore, are based on standards set within the United Kingdom. Although, some of the care homes in the pilot phase were based in Australia, and did not report any discrepancies between the expectations of their regulatory body or education providers and the ADAPT criteria. Versions of the ADAPT based on different international regulatory criteria might be developed. However, use of the current ADAPT tool would allow comparisons between dementia awareness training standards internationally within research studies.
In conclusion, the ADAPT tool provides LTC researchers with an evidence-based audit tool of dementia awareness and PCC training for use in studies including RCTs as a method of assessing UC.
Supplemental Material
Appendix 1 -Supplemental material for The development and use of the assessment of dementia awareness and person-centred care training tool in long-term care
Supplemental material, Appendix 1 for The development and use of the assessment of dementia awareness and person-centred care training tool in long-term care by Alys Wyn Griffiths, Claire A Surr, Byron Creese, Lucy Garrod and Lynn Chenoweth in Dementia
Footnotes
Acknowledgements
We would like to thank the care homes who participated in the piloting of the audit tool. We would like to thank Clive Ballard, Jane Fossey, Murna Downs, Amanda Farrin, Sue Fortescue, Liz Graham, Ivana Holloway, David Meads, Louise Robinson, Najma Siddiqi, Graham Stokes, Daphne Wallace and Rebecca Walwyn for their input into developing this measure.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute for Health Research Health Technology Assessment Programme (NIHR HTA) (project number 11/15/13)
Author notes
An electronic copy of the ADAPT tool is available from the authors on request. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HTA, NIHR, NHS or the Department of Health and Social Care.
Ethical Approvals
Ethical approval for the DCM™ EPIC trial was granted by NRES Committee Yorkshire & The Humber – Bradford REC ref 13/YH/0016. Ethical approval was not required for piloting of the assessment tool as this was deemed not to constitute research.
Supplementary Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.