
Abstract
Extra care housing facilities in the UK are intended to offer a community-based alternative to care home placement. However, little is known about staff’s views of the appropriateness of extra care housing for people with dementia. This paper describes a mixed-methods study which explored this issue using statistical modelling of frontline staff’s recommendations of the best care setting for care home entrants; thematic analysis of transcripts from a simulated Resource Allocation Management Panel meeting; and content analysis of care coordinators’ reasons for not considering extra care housing in actual care home applications. Frontline practitioners saw extra care housing as a valuable alternative for a significant minority of care home entrants. However, extra care housing was not recommended if people needed care at night. Social care managers expressed general support for the idea of extra care housing, but appeared overwhelmingly focused on maintaining people at home and unsure where in the care pathway extra care housing sat. More evidence is needed on whether extra care housing can be an alternative to care homes and how services should be arranged to meet the needs of people living in extra care housing.
Introduction
The promotion of personal choice, autonomy and control are central aims of health and social care policy in many countries (Winblad et al., 2016). As a result, the long-term care continuum for older people with mental health problems (including those with dementia), which has traditionally ranged from care at home to admission to a care home or long-stay hospital ward is changing. The overriding aim is to enable older people to live at home as long as possible. Furthermore, where some form of residential care is required, the desire is to make this as homelike as possible (Moise, Schwarzinger, & Um, 2004). To this end, a range of new facilities have been developed which provide ‘housing with care’ for older people, including a number of specialist facilities for older people with dementia (Evans et al., 2012; Verbeek, Van Rossum, Zwakhalen, Kempen & Hamers, 2009). Some of these initiatives are designed to serve as alternatives to long-term care home placement, such as the small-scale living complexes found in the Netherlands (Verbeek et al., 2009) and the Green Houses seen in the US (Kane, Lum, Cutler, Degenholtz, & Yu, 2007); others are positioned at an intermediate point between living at home and institutional care, such as Sweden’s group living schemes (Annerstedt, 1994).
In the United Kingdom, a number of extra care housing (ECH) facilities have been developed with the intent of providing a community-based alternative to care home placement (Department of Health, 2010). Although there is no standard definition of ECH (also known as very sheltered housing), such schemes typically offer older people their own flat as well as care and support in a purpose-built complex designed with the needs of highly dependent people in mind (Department of Health, 2010; Netten, Darton, Bäumker, & Callaghan, 2011). Personal care (often provided by an on-site care team) is generally available 24 hours a day and communal facilities typically include a laundry, restaurant/dining room and lounge (Laing & Buisson, 2010).
To date, several studies have explored the characteristics of ECH residents and how they differ from those of older people living at home or in a care home (Bäumker, Netten, & Darton, 2010; Darton et al., 2012; Netten et al., 2011). In summary, this work suggests that ECH residents need more assistance with personal care and domestic tasks than older people living at home (Netten et al., 2011), but less assistance with activities of daily living (ADLs) than care home residents (Darton et al., 2012). Nevertheless, over half of ECH residents are unable to go outdoors or manage steps or stairs, a similar proportion require assistance with washing and bathing, and over a third need help with dressing (Netten et al., 2011).
Other research has focused on the ability of ECH to promote independence and security and reduce isolation (Bäumker et al., 2010; Callaghan & Towers, 2014; Shaw, West, Hagger, & Holland, 2016). For example, one English study found that older people who had moved into ECH identified a significant decrease in their unmet needs and a significant increase in their quality of life compared with their situation at home (Bäumker et al., 2010). Another reported that 80% of ECH residents described their social well-being as either ‘good’ or ‘as good as it can be’; 90% had made new friends; 85% were positive about their social life; and 75% were occupied in activities of their choice (Callaghan, Netten, & Darton, 2009). Although such studies have included people with cognitive impairment, they have usually formed only a minority of the sample, and it has often been suggested that older people with dementia are less likely to participate (and hence be socially isolated) than other residents in ECH (Callaghan et al., 2009; Croucher, Hicks, & Jackson, 2006; Dutton, 2009). Nevertheless, there is mounting evidence to show that the quality of life of people with dementia in ECH is generally good, particularly where staff have specialist dementia expertise, enabling them to develop meaningful relationships and provide specialised activities (Dutton, 2009).
In contrast, there has been little focus on how recommendations of ECH entry are made by frontline staff and managers. Indeed, although many studies have examined the factors that predict care home admission for people with dementia (Gaugler, Yu, Krichbaum, & Wyman, 2009; Luppa, Luck, Brähler, König, & Riedel-Heller, 2008), evidence is lacking about the factors that predict transition to ECH, or health and social care professionals’ perspectives on the best use of such facilities (i.e. who is most appropriately supported in ECH). This is despite the fact that such information would seem to be of great value to service planners seeking to optimise resource use and to frontline practitioners, facilitating the provision of advice and transition planning. Against this background, this paper presents new, previously unpublished analysis of the views of a range of frontline practitioners and managers on when ECH is the most appropriate option for older people with mental health problems, in particular dementia and examines the barriers to its wider use with this client group.
Methods
This paper uses three strands of data (see Table 1) to explore the potential use of ECH for current care home entrants in Site X, a ‘prospering smaller town’ whose older residents had a sociodemographic profile resembling England as a whole, albeit the proportion from ethnic minorities was less than half the English average. At the time, the study was the number of people in long-stay residential care was close to the England average (15.1 per 1000 people aged 65+ compared with 14.1 nationally), but there were fewer care home beds. The local authority was interested in exploring the use of ECH as an alternative to care home placement and had recently upgraded several sheltered housing complexes into ECH for older people; none of these were specifically dedicated to the care of people with dementia. The data were collected as part of a Balance of Care (BoC) study, which sought to identify the most appropriate mix of community and institutional services to provide for older people with mental health problems in North-West England (Challis et al., 2014; Tucker, Brand, Wilberforce, Abenstern, & Challis, 2015). Balance of care is a long-standing strategic planning framework, identifying people whose needs can be met in more than one setting (e.g. in hospital or at home) and exploring the potential costs and consequences of changing the mix of services provided in a simulation exercise grounded in the knowledge of frontline practitioners (Challis & Hughes, 2002; Clarkson, Hughes, & Challis, 2005; Tucker et al., 2015; Tucker, Hughes, Burns, & Challis, 2008).
Summary of research activities.
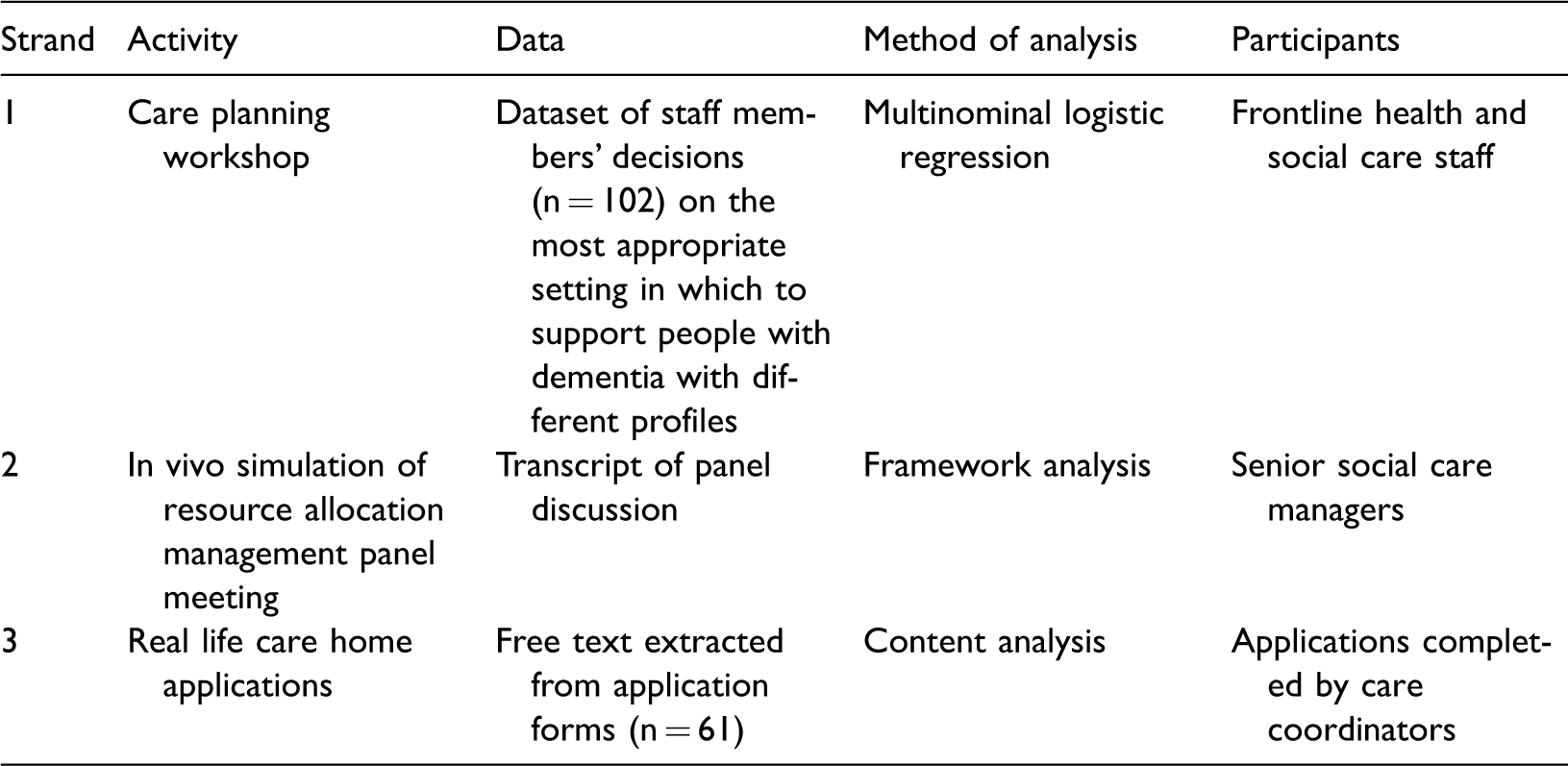
Strand 1. Care planning workshop. The identification of care home entrants for whom ECH could be more appropriate: Frontline practitioners’ recommendations
Anonymised information on 169 older (65+) care home entrants with mental health problems was collected by their care co-ordinators. Data collection was undertaken in 2010/2011 and encompassed details of individuals’ sociodemographic, functional and clinical characteristics, including a number of standardised measures (Folstein, Folstein, & McHugh, 1975; Kroenke, Spitzer, & Williams, 2003; Mahoney & Barthel, 1965; Morris et al., 1994; Yesavage et al., 1983). Further information was collected on individuals’ recent service receipt and reason for admission. Short-term admissions for planned respite or intermediate care and people moving from one care home to another were excluded.
The sample was divided into subgroups of people with similar needs for care on the basis of three variables deemed important in determining the locus of care (Tucker et al., 2008). These were the individuals’ need for help with ADLs, their level of cognitive impairment and the presence of behaviours that carers often find hard to manage (Table 2). As each of these variables had three levels, we could generate 27 unique combinations of these variables, representing subgroups or ‘case types’ of patients (3 × 3 × 3).
Criteria used in the classification of case types.
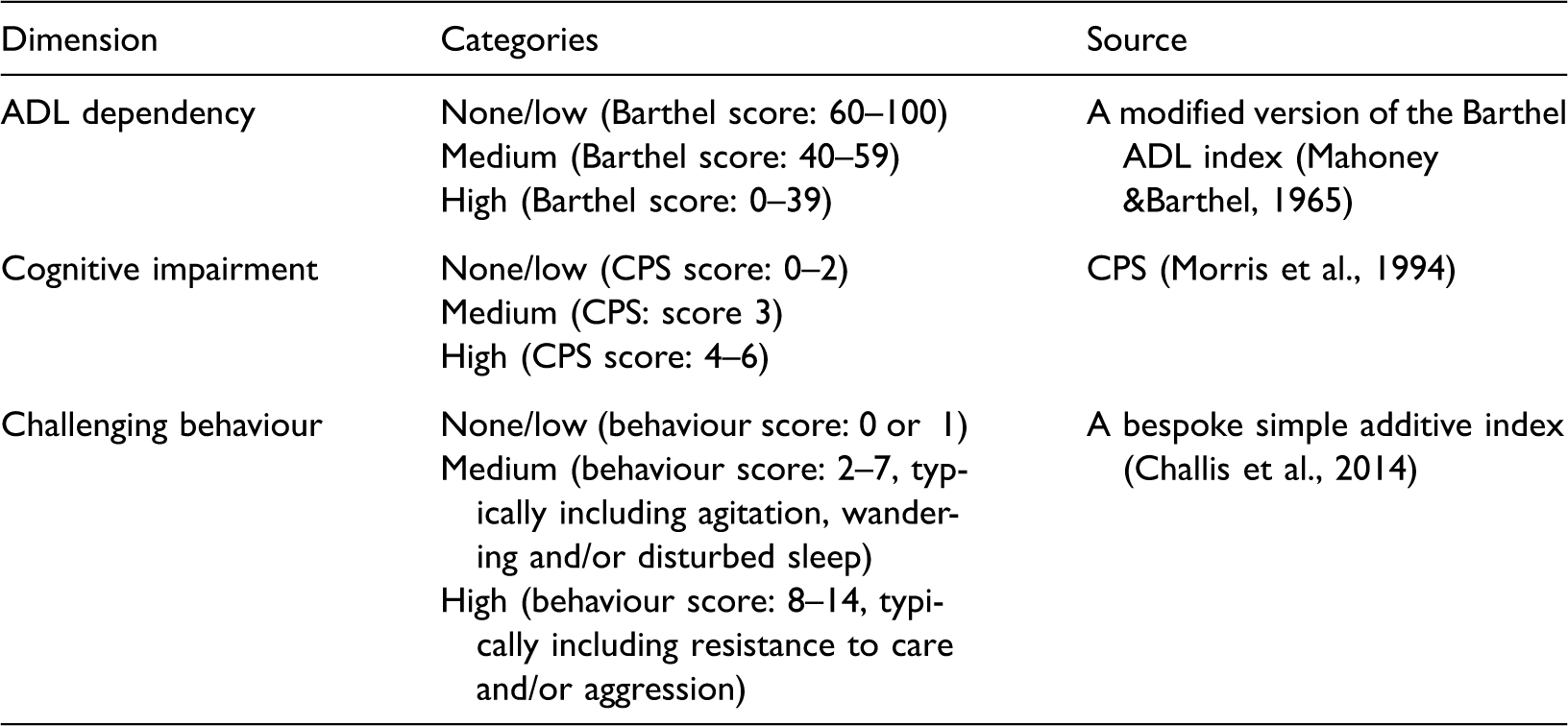
ADL: activity of daily living; CPS: cognitive performance scale.
A series of vignettes (n = 14) were formulated to exemplify the most commonly populated case types. These were based on real individuals in the dataset and took the form of short case summaries depicting the person’s situation immediately before care home entry – the point at which alternative care options could realistically have been considered. Each vignette systematically incorporated information about the three key variables listed above, as well as their risk of falling, physical health status, living situation, service receipt, location on assessment (hospital or home) and care preferences. An example of a vignette is given in Box 1.
An example of a vignette, Mrs E living with dementia.
Mrs E is an 80-year-old lady who usually lives with her husband. She is currently an inpatient at the district general hospital where she has been treated for a urinary tract infection and delirium.
A range of frontline practitioners (NHS and Social Care staff) were invited to a care planning workshop in October 2011 at which the most appropriate ways of meeting the needs of the people depicted in the vignettes were explored. Workshop participants (n = 17) were divided into small multidisciplinary groups, each of which was allocated six vignettes. Using a modified nominal group approach (Bowling, 1997), participants were asked to read the vignettes carefully and to decide, first individually and then in their small groups, where they believed each depicted person would be most appropriately cared for – their own home, ECH (for older people generally or dementia specific) or a care home (for older people generally or dementia specific, with or without nursing). Still in their small groups, participants then chose case types for whom they felt care at home or in ECH was a realistic proposition, and specified the care services and professional support needed to achieve this. For the purposes of this exercise, participants were asked to put aside any short-term constraints in current services (including the then lack of ECH specifically dedicated for people with dementia) and to think creatively, whilst remembering that all provision inevitably has funding implications. A list of services available in other parts of the country was provided to facilitate this activity, and a comprehensive costing approach was subsequently used to estimate the weekly costs of the proposed community care packages.
Descriptive statistics were used to characterise the recommendations for each case type (vignette), and modelling was employed to illuminate the decision-making process. The decisions of individual practitioners and small groups formed the analysis dataset, and a multinomial logistic regression was undertaken to explore the factors associated with the choices made.
Strand 2. Simulated resource allocation management panel. The identification of care home entrants for whom ECH could be more appropriate: social care managers’ views
Details of the case types for whom practitioner groups recommended community care (including ECH) were presented at a specially convened meeting of the Site X Resource Allocation Management (RAM) Panel in November 2011. This was composed of three senior social care managers who acted as gatekeepers for access to long-term care home placement. The Panel was asked to consider each case and to decide whether or not the proposed alternative support arrangements were: (i) appropriate; (ii) sufficient to enable the depicted individuals to remain in the community; and (iii) fundable.
This exercise took the form of an in-vivo simulation of a normal RAM Panel meeting and utilised local proformas containing information on:
The individuals’ needs (as depicted in the vignettes); Their actual care home placement (with or without nursing, for older people generally or dementia specific) including the cost to social services; and The alternative community care packages proposed by practitioners, including the estimated cost to social services.
With the participants’ consent, the RAM Panel discussion was audio-recorded, and the transcript was professionally transcribed. A framework approach was used to manage and interpret the data (Ritchie & Spencer, 1994; Spencer, Ritchie, O’Connor, Morrell, & Ormston, 2014). This matrix-based system was developed to support thematic analysis and involves a series of stages to familiarise, sort, index and summarise data, allowing movement between levels of abstraction, whilst staying close to the original material. Data are summarised by both case and subtheme facilitating cross and within case analysis. Three authors (HV, ST, MA) undertook this task individually, with later discussion to challenge and refine themes and build understanding and consensus, a method that was both iterative and comprehensive.
Strand 3. Real life care home applications: Reasons for not considering ECH
Free text information on the reasons why ECH was not considered suitable for actual care home entrants, the vast majority of whom had significant cognitive impairment or dementia, was extracted from real life (anonymised) care home application proformas (n = 61) completed by care co-ordinators and presented to the RAM Panel over a three-month period in 2010. Coding used conventional content analysis (Graneheim & Lundman, 2004). This derives themes/categories directly from the data at hand (avoiding the use of preconceived categories), making it an appropriate approach for exploratory analyses (Hsieh & Shannon, 2005). Interpretation was limited to manifest content, i.e. which is visible and obvious (Graneheim & Lundman, 2004). Two researchers (HV and ST) independently analysed the data to identify basic codes, which were subsequently grouped into broader categories and refined and compared in discussion with a third team member (MW).
Ethics
Ethical approval for the study as a whole was granted by the then Cambridgeshire 3 Research Ethics Committee (reference number 10/H0306/51) and research governance procedures in each participating organisation were fulfilled.
Results
Strand 1. Care planning workshop. Identification of care home entrants for whom ECH could be more appropriate: Frontline staff’s recommendations
Of the 169 care home entrants, just over half were ≥85 and 68% were female. Although the vast majority had previously lived at home (8% lived in ECH), most were admitted to a care home directly from hospital (49% from a general ward and 9% from a psychiatric ward). Approximately two-thirds had at least medium ADL dependency; more than four-fifths had medium or high levels of cognitive impairment; and a still higher proportion presented with medium or high levels of challenging behaviour. Full details of the study sample are available elsewhere (Challis et al., 2014).
Of the 27 case types used to characterise the care home entrants, 23 were populated. As would be expected, some combinations of characteristics were more prevalent than others, and in combination the 14 vignettes represented 77% of the sample (see Table 2). Nine of the vignettes depicted people with a formal diagnosis of dementia, whilst three others depicted people with some degree of cognitive impairment (including memory loss, disorientation to time and word-finding difficulties). The remaining two had no significant cognitive impairment, but had marked anxiety or depression.
As noted, 17 (frontline and managerial) staff participated in the care-planning workshop, and each of the 14 vignettes was considered by at least six individuals (maximum 11). Mental health nurses were the most frequently represented discipline, but other participants included social work and housing staff. Altogether, individual participants made a total of 102 recommendations, of which 37 were for ECH – 23 for ECH for older people generally and 14 for dementia-specific ECH (see Table 3). Indeed, at least one individual recommended ECH for 12 of the 14 case types.
Views of practitioners’ on the most appropriate settings in which to support the 14 case types depicted in the vignettes.
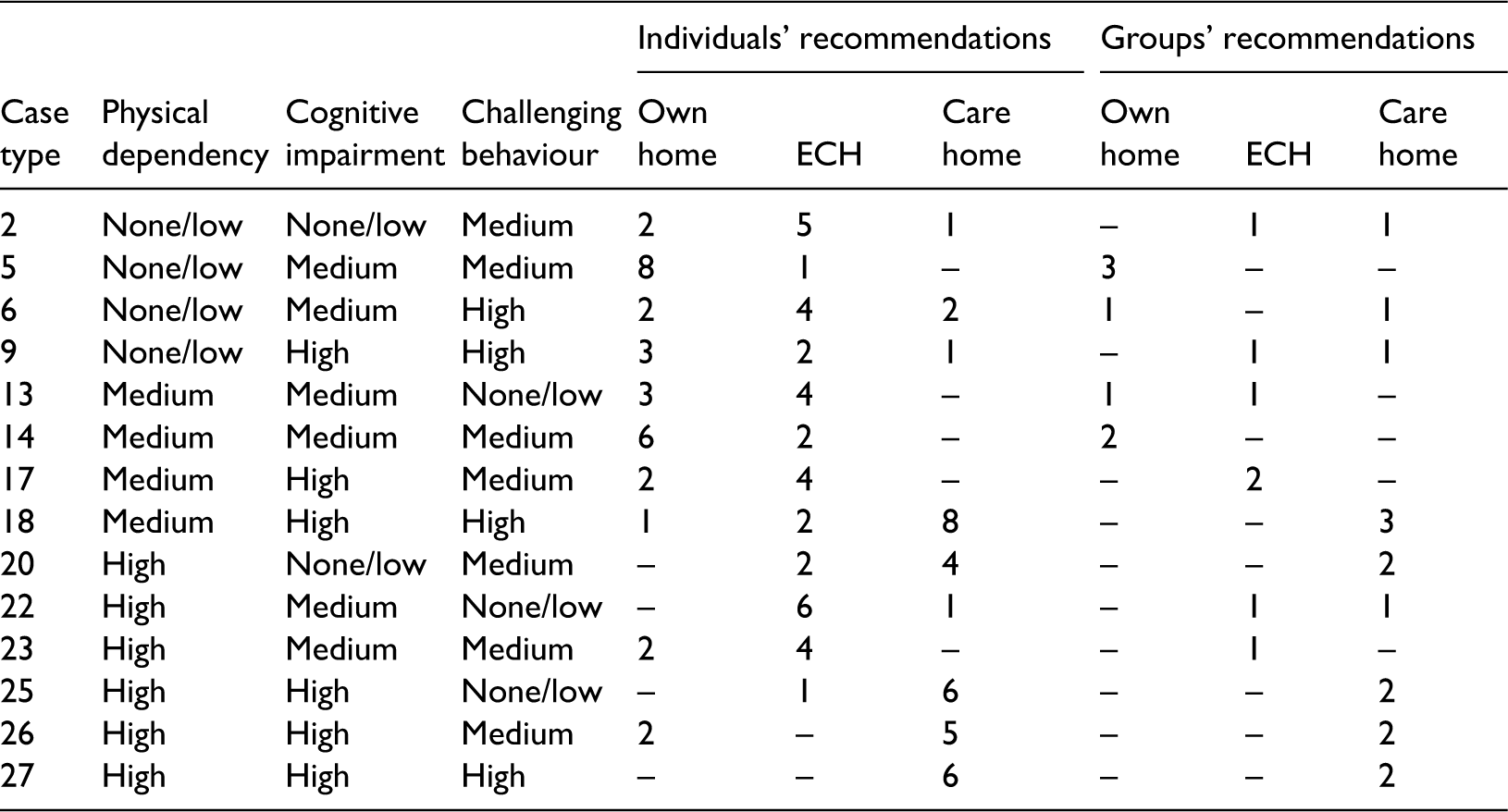
ECH: extra care housing.
Fourteen alternative care plans were formulated by the multidisciplinary groups, of which seven identified ECH as the most appropriate care setting (see Table 3). These pertained to six case types, of which three represented people with a formal diagnosis of dementia and two represented people with evident cognitive impairment.
Characteristics influencing decision making of practitioners.
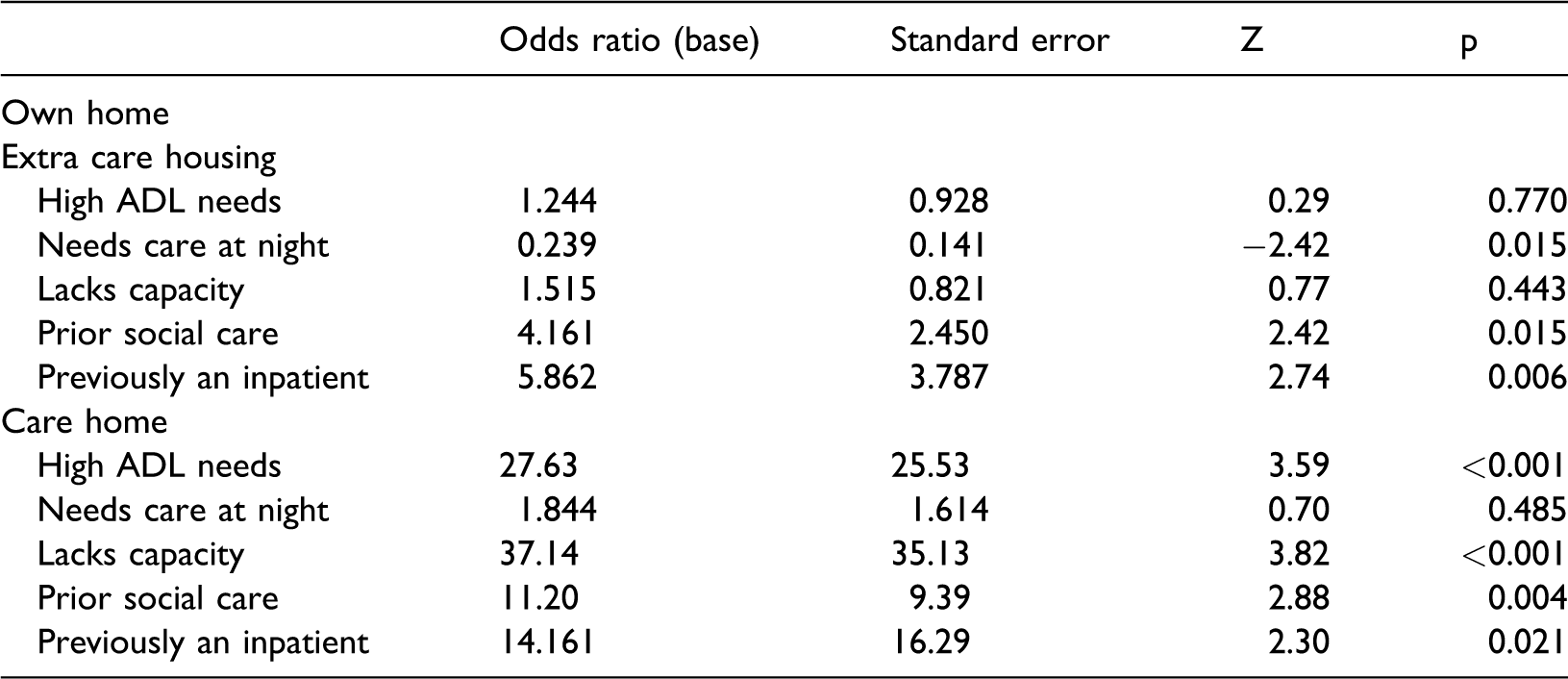
ADL: activity of daily living.
Note: N=116, LR χ2(10) 88.82, p < 0.001, Pseudo R2 = 0.3503.
Strand 2. Simulated resource allocation management panel. The identification of care home entrants for whom ECH could be more appropriate: view of social care managers
When presented with the details of the five care home case types with dementia/evident cognitive impairment for which the staff groups recommended ECH, the RAM Panel supported ECH for just one (case type 22). Furthermore, the home of the depicted individual in this case was described as physically unsuitable to meet their needs, meaning a change of residence was (at least in the short-term) inevitable. In each other case, the Panel favoured care at home.
Five main themes relating to the rejection of ECH as the most appropriate care setting were identified from the RAM Panel discussion: (1) the desire to support people at home wherever possible; (2) the wish to support individuals’ preferences; (3) the need to avoid potentially disruptive moves; (4) uncertainty about at what stage in the care pathway ECH was most appropriate for people with dementia and (5) the lack of sufficient information to justify such a move.
Perhaps, the most pervasive of these was the Panel’s strong desire to support people with dementia at home wherever possible for as long as possible (taking into account the risks the person would face in doing so). ‘Our key brief and our key principle is that we will always try and support somebody in their own home’.
When considering whether a proposed move to ECH was appropriate for a particular person, for example, the Panel often started by asking whether or not the individual had any needs that could not be met at home, or whether all home care options had been ‘exhausted’: ‘I suppose from my perspective just before we got to this level [ECH] I suppose we’re looking to see what additional support can we provide within the home…’ (Case type 9). ‘What would extra care housing give her that we couldn’t provide by enhancing her care package?’ (Case type 17).
Second, whilst staying in one’s own home appeared to be seen as a ‘good’ in itself, the desire to support the person’s wishes was often cited in support of their decision: ‘You know, if somebody was really keen on returning home and wanting to stay there and that was their wishes, then we’d look to support those’ (Case type 22).
However, analysis suggested that where individuals (or more often their family) felt they couldn’t remain at home and/or expressed fears about their ability to cope, the Panel’s initial response was still to see if they could address/overcome these issues by providing more support at home. Talking about the situation of Mrs E in Box 1, for example, for whom they were inclined to provide support at home, they noted that: It doesn’t say anywhere in here that the husband or the family are saying that actually with additional support they feel they would, … be able to support her at home. So I mean, realistically, that’s a piece of work that really does have to be undertaken before you go anywhere because they’re saying they’re at their limit. (Case type 9)
Indeed, identifying the optimal time to move to ECH was identified as a fourth theme of itself, and seemed to pose the Panel something of a quandry, as whilst they considered that older people with dementia would be more likely to adapt to ECH if they moved at a relatively early stage in their illness (the long-term perspective), they also wished to prevent any unnecessary moves (the short-term perspective) and were concerned that people may subsequently need to move into a care home (the long-term perspective): Looking at placements for extra care at an earlier point is sometimes more useful for people because it gives an opportunity to orientate, but then you’re left with the dilemma of will it ultimately still lead to a place in a residential home in which case you’ve had several moves. And I suppose on that basis you do try to support people as long as possible as well at home… so you’ve got sometimes a bit of a dilemma. (general discussion) Clearly this lady is at the moment in hospital. She’s got a urinary tract infection sort of overlaying on her diagnosis anyway of vascular dementia… This lady will need some time, and in terms of … her behaviour, you know, perhaps situational… (Case type 9)
Strand 3. Reasons for not considering ECH in actual care home applications
The reasons care coordinators (frontline practitioners) gave for not considering ECH for actual care home entrants fell into five main categories: the extent of care the person needed; the level of individuals’ needs; the perceived inability of ECH to maintain people’s safety; the desire to respect the individual’s (or family’s) wishes; and the previous, unsuccessful trial of ECH.
The first and most common of these (noted in 42 applications) concerned the extent of the care the person needed, which was perceived to exceed that available in ECH. This was expressed in several different ways. For instance, many care co-ordinators highlighted the frequency of care service users required, including the need for ‘care throughout the 24 hour period’ or ‘24 hour supervision’, whilst eight applications stated that the person needed somebody with them at all times to prevent them becoming distressed. Other applications rather emphasised the degree of care the person required (e.g. needs two carers and hoisting) or the fact that care inputs could not be regularly scheduled (e.g. ECH would not be a viable option… due to the unpredictability of his toileting needs), whilst the need for care at night or nursing care were also seen as prohibitive.
Coming at this in a different way, in 27 cases care coordinators emphasised the level of individuals’ needs (the second category), arguing that these were too severe/complex to be met in ECH. In some cases, no further detail was given. However, many applications made reference to specific psychological or behavioural concerns, predominantly people’s level of cognitive impairment, anxiety and depression. In one instance, for example, ECH was deemed unsuitable because of the person’s ‘agitated state and verbal aggression’, whilst in another instance, it was stated that the individual’s ‘level of disorientation’ made ECH inappropriate. By contrast, only two applications referred to the extent of people’s physical needs.
Related to the above, a third category concerned the perceived inability of ECH to maintain people’s safety. This was mentioned in 15 applications, with ECH seen as particularly inappropriate for people at risk of falls. However, the same argument was sometimes made for people reported to wander.
The fourth set of reasons related to the older person’s or family’s wishes, which were mentioned in connection with 17 applications. Some of these were linked to the person’s aforementioned level of needs. However, a more common scenario was that the person had been temporarily placed in a care home in response to a crisis, and had since settled, such that they/their family or staff were reluctant to consider another move. Frequently, however, no explanation was given other than that the person or their relatives did not want to consider ECH.
Finally, in a handful of cases, ECH was said to have been tried and unsuccessful (n = 3), or unavailable (n = 3), there no suitable schemes within the area the person wanted to live in or no vacant flats at the right time.
Discussion
This study provides new insight into views of frontline practitioners (including care coordinators) and social care managers on the appropriate use of ECH for older people with mental health problems and identifies potential barriers to its greater employment. As indicated in the first strand of the results from the care planning workshop, frontline staff viewed ECH as a valuable alternative to care home placement for a significant minority of current care home entrants, particularly people with a formal diagnosis of dementia or evident cognitive problems who lived alone. However, ECH was not recommended for people who needed care at night. Indeed, the third strand of the results, the analysis of real care home applications, showed that the need for more care (and in particular more frequent – often 24 hour – care) than was perceived to be available was given as a reason for not considering ECH in more than two-thirds of actual care home applications. In contrast, the second strand of the findings, the analysis of the RAM Panel meeting, revealed that social care managers appeared overwhelmingly focused on maintaining people at home, and saw few if any advantages to ECH for the presented case types, despite expressing general support for this form of housing.
Looking across the different datasets, this study indicates a lack of clarity as to the place of ECH in the care spectrum, which may prevent its wider development for people with dementia. On the one hand, when asked to state why ECH was not appropriate for actual care home entrants in the third strand of the study, frontline staff suggested it did not provide sufficient care, arguing that individuals’ needs were too high to be met in such facilities. This would appear to indicate that they saw its place in the care spectrum as close to care at home. On the other hand, when asked to identify the most appropriate care option for certain current care home entrants in the first strand of the study, social care managers typically argued that the individuals’ needs did not warrant ECH. This might seem to suggest that they would perceive it as closer to care home entry. As indicated in the introduction, however, studies suggest that ECH can enable older people to lead fulfilling lives in an environment that is widely perceived to be less restrictive than many care homes (Callaghan & Towers, 2014; Demos, 2014). Further, the limited evidence available from similar, homelike residential models in other countries suggests that residents’ satisfaction with care is high in such environments (Ausserhofer et al., 2016; Verbeek et al., 2009). Together, this might encourage social care staff to view ECH as a discrete alternative to both of these environments.
Another important finding from this study highlights a lack of consensus about the point on the care pathway at which ECH is most appropriate for people with dementia, with different staff placing different weights on different arguments. These include the belief that people with dementia are more able to adapt to a change of residence early in the care pathway; the likelihood that a change of residence will create major stress and a potential deterioration in functioning and the assumption that a move to ECH will not be for life. The latter, in particular, appeared to be an important obstacle to the greater use of ECH in this study. However, internationally, other small-scale, homelike care models have developed to support very highly dependent people, sometimes in close relation with other assisted living facilities (Verbeek et al., 2009; Wimo & Morthenson Ekelöf, 2005), and it might be argued that given to the flexible care available, residents should be able to stay in ECH as their needs progress. More research is needed to investigate whether these expectations can be met over time. Further, whilst frontline practitioners tended to consider ECH inappropriate for older people who needed frequent care or supervision or posed potential risks, particularly in relation to falls, whether care homes can minimise these risks to a greater extent than ECH and are better placed to provide 24-hour care is a moot point. There is certainly some evidence that care homes find it difficult to meet the needs of people with complex, unpredictable presentations, and that sufficient time and prerequisite skills among care home staff may be lacking (Robbins, Gordon, Dyas, Logan, & Gladman, 2013). Moreover, whereas care homes in some other countries employ their own specialised medical staff, facilitating the care of people with greater needs (Conroy et al., 2009), in the UK, medical responsibility for both ECH and most care home residents is held by general practitioners (GPs).
Finally, interestingly, this study found no evidence that costs were a key factor in driving staff’s decision making, with there being minimal reference to costs in any of the three strands. Previous evidence has suggested that ECH can be a cost-effective alternative to care home admission (Bäumker et al., 2010) and it may be that the participating staff were aware of this. Alternatively, it may be that other reasons, such as the desire to support people at home were perceived as more important. Indeed, as noted above, particularly for the RAM Panel, this desire appeared to override any other concern, including on occasion older people’s and families’ preferences.
Limitations and strengths
A major strength of the current study is its use of both quantitative and qualitative methods. The materials used in the care planning workshop drew on a rich dataset of current care home residents’ characteristics at the precise time of care home admission. It facilitated the construction of representative case types whose care needs were explored using a modified nominal group approach, whilst the in vivo RAM panel exercise and the analysis of real life care home applications supplied rich data on the factors underlying both managers’ and frontline practitioners’ decision making. Nevertheless, four key limitations must be acknowledged. First, the research was conducted in just one area of the UK, which may limit generalisability of results. For example, the limited extent to which social care managers’ regarded ECH as a valuable alternative to care home admission could be a local effect. Second, although there were several ECH facilities in the study site, none of these were dedicated for people with dementia. Whilst the focus of the study was on the services needed by people with dementia, as opposed to the services available, it is possible that the participants in the first two strands of the study (the care planning workshop and simulated RAM Panel) may have over- or under-estimated what such facilities can offer. Third, the study focused solely on staff views and did not directly involve older people with mental health problems or their carers themselves, albeit information on their preferences was included in the vignettes. Fourth, the issue of ownership (i.e. whether people’s previous housing was privately owned or rented) was not considered in the decision about different ECH options.
Conclusion
This study provides new understanding of perspectives of frontline practitioner’ and social care managers on the appropriate use of ECH for people with dementia. Whilst social care managers’ appeared overwhelmingly focused on maintaining people at home, frontline practitioners viewed ECH as a valuable alternative to care home placement. More empirical evidence is needed on whether, for whom and in what circumstances ECH provides a preferable alternative for people with dementia, including the views of users’ themselves. In the meantime, local care planners and commissioners could investigate whether the concerns and reservations about the use of ECH identified above are mirrored in their locality and consider the potential utility of alternative supported housing models from other countries.
Footnotes
Acknowledgements
We thank all frontline practitioners, social care managers, participants of the Resource Allocation Panel and care coordinators who have participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0606-1109).