
Abstract
This paper examines how the relatives of a person with dementia experience challenges in everyday life. A model of phases is developed on the basis of interviews with 14 relatives from eight families. Data were subjected to a thematic content analysis, which found that the progression of dementia – from the perspective of the family – had three phases. These phases involved small changes in everyday life, adaptations to everyday life, and the loss of everyday life. The analysis further identified the following two archetypes of relatives that develop throughout the progression of dementia: the protective relative and the decisive relative. The study found that the two types of relatives experience different challenges during the three phases. It is important for health professionals to be familiar with these changes, when they evaluate whether the relatives of a person with dementia require help.
Introduction
Dementia constitutes a serious international public health problem, with the number of diagnosed patients expected to double before 2030 (World Health Organization and Alzheimer’s Disease International, 2012). The increased preponderance of dementia affects not only national economies but also the many relatives of persons with dementia, who live with the condition in everyday life (Adelman, Tmanova, Delgado, Dion, & Lachs, 2014; Duggleby, Swindle, Peacock, & Ghosh, 2011; Ivey et al., 2013; World Health Organization and Alzheimer’s Disease International, 2012). Relatives play an important role in how the progression of dementia is addressed because they must accept responsibility for the coherence of family life (Daly, McCarron, Higgins, & McCallion, 2013). The relatives of a person with dementia can experience their roles as a burden because of their increased responsibility for maintaining the everyday life of the family (Duggleby et al., 2011). This burden results in emotional turmoil and uncertainty regarding the future as well as a reduction in health and everyday welfare (Daly et al., 2013; Pinquart & Sorensen, 2007; Schulz & Sherwood, 2008; World Health Organization and Alzheimer’s Disease International, 2012). In this regard, it is necessary to identify the resources available to relatives and how the provision of these resources can be optimized (Grand, Caspar, & Macdonald, 2011; Valimaki, Vehvilainen-Julkunen, Pietila, & Koivisto, 2012). Studies of chronic conditions have examined the issue of relatives’ perspectives and how the inclusion of relatives in healthcare is best attained (Cameron & Gignac, 2008; Grand et al., 2011); these studies have suggested an approach with a greater emphasis on relatives’ resources than on the medical progression of dementia. This approach indicates that the effective interventions should target relatives’ lives and their need for support (Cameron & Gignac, 2008; Schure et al., 2006).
Several studies have examined the experiences of relatives of persons with dementia at various stages of the condition (Daly et al., 2013; Forbes et al., 2012; Phinney, Dahlke, & Purves, 2013). However, no studies have focused on how the resources and needs of relatives change over time. Forbes et al. (2012) developed a model of phases that illustrates the type of information that relatives require throughout the progression of the illness. A similar model could be developed with a focus on the challenges that relatives experience regarding their own resources and needs during the progression of dementia.
Many of the studies examining relatives’ experiences have focused on the individual caregiver (Conde-Sala, Garre-Olmo, Turro-Garriga, Vilalta-Franch, & Lopez-Pousa, 2010; F. Ducharme, Levesque, Lachance, Kergoat, & Coulombe, 2011; F. C. Ducharme et al., 2011). Some, however, have indicated that the relationships between the person with dementia and relatives in the family are also affected (McGovern, 2011; Quinn, Clare, & Woods, 2015). An examination of how relatives experience the progression of dementia over time, therefore, requires a more systemic approach to the family (Haefner, 2014). This approach requires us to consider how a family is able to balance individual’s resources and needs while being a part of a family during difficult times, such as during an illness. An illness such as dementia is bound to cause changes in a family and to challenge the everyday lives of the family. The adoption of a different approach to understanding when and how relatives experience challenges regarding resources and needs could generate knowledge about how to target interventional efforts directed towards families affected by dementia (World Health Organization and Alzheimer’s Disease International, 2012). The aim of this study was to examine how family members experience the challenges of everyday life throughout the progression of dementia, from the first signs of dementia until at least six months after the person with dementia has moved to a care facility.
Methods
Design
A generic qualitative research approach was used to describe and interpret meaningful phenomena in context and, in this case, to investigate family members’ experiences as relatives of a person with dementia over time, from the first sign of dementia until at least six months after admission to a nursing home (Green & Thorogood, 2009; Kvale & Brinkmann, 2014; Ten Have, 2008). To explore this phenomenon, we conducted semi-structured interviews with relatives from the families of persons with dementia (Åstedt-Kurki, Paavilainen, & Lehti, 2001). Qualitative content analysis was used to analyse the data and to conceptualize the findings (Elo & Kyngas, 2008).
Informants
The recruitment of informants was undertaken with the help of the nursing staff in a Danish municipality. A nurse who functioned as an intermediary between the researchers and the families initiated contact with the families on the basis of written information about the study.
The following inclusion criteria were applied: the informants had to be relatives of a person with vascular dementia or Alzheimer’s dementia, because it was not possible to contact persons with other types of dementia in this municipality; the person with dementia must have moved to a care facility at least six months earlier; the informant must have cared for or given support to the person with dementia on a daily basis before the move to the care facility or have had regular contact with the person with dementia; and there had to be one to three close relatives in the family. In this study, a relative was considered a member of a family. A family was defined as two or more individuals who depend on one another for emotional, physical, and economic support (Kaakinen, Coehlo, Steele, Tabacco, & Hanson, 2015).
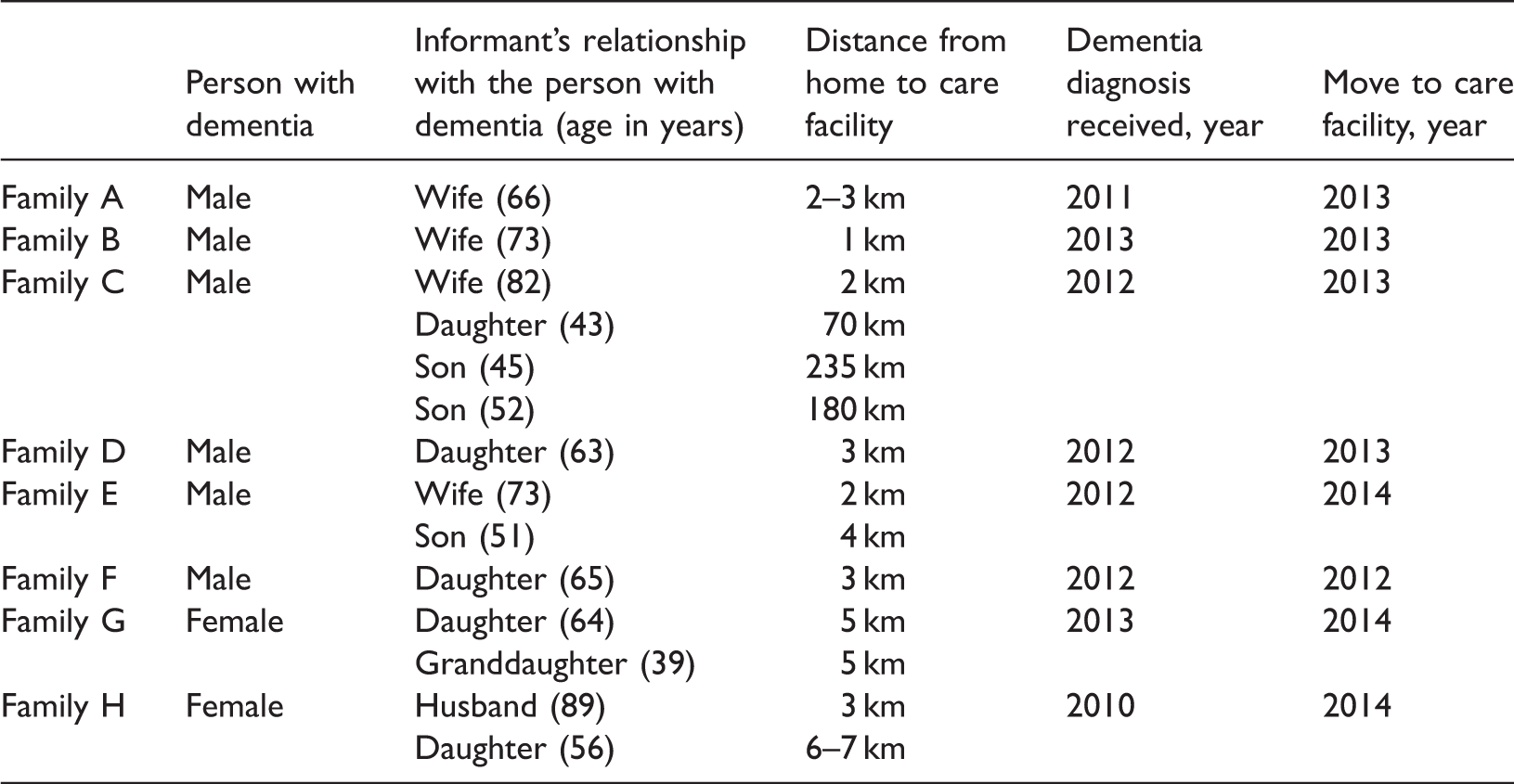
Description of families.
Data collection
Over the course of two months (15 June 2014–15 August 2014), 14 individual interviews were conducted. To facilitate the interviews, we informed the informants that they could be interviewed in their homes. The interviews were completed by the first three authors. To promote a common approach across the interviewers, we conducted a pilot interview with all of the interviewers present. Furthermore, all of the interviewers listened to all of the interviews during the interview process to ensure consistency across the interviews.
The interview guide was semi-structured and thematized according to the following research question: ‘What is the experience of a relative of a person with dementia over time?’ Furthermore, the guide was inspired by the existing literature, which contributed to a pre-understanding regarding the subject in question (Daly et al., 2013; Duggleby et al., 2011; Forbes et al., 2012; Kvale & Brinkmann, 2014; Stephan et al., 2013).
The questions in the interview guide were formulated as open introductory questions with the option to pose additional questions. Examples of questions concerning the personal experiences of the participants and the relationship between the participant and the person with dementia were as follows: ‘Tell me about a situation or experience that you recollect as being particularly difficult’ and ‘Please describe how you help each other’ (see Appendix 1). All of the interviews lasted 45–75 minutes and were tape recorded and fully transcribed verbatim.
Data analysis
This study employed qualitative content analysis, inspired by Elo and Kyngäs (2008). The inductive approach is recommended when knowledge about a phenomenon is insufficient or fragmented. The inductive content analysis process involves three stages of open coding, creating categories and abstracting. A thorough reading of all of the data was undertaken to obtain an overview before open coding was applied to capture and describe the valuable aspects of the content. Codes referring to the same content were grouped into categories. Coding, grouping into categories and abstracting were performed as an iterative process, making it possible to explore content in the data by going back and forth in the analysis process.
Firstly, the analysis process identified a pattern of three core phases in the progression of dementia. We observed that, within these three phases, the relatives in the families had different perceptions of the course of the illness, as captured by three main categories: phase one: small changes in everyday life; phase two: adaptations to everyday life; and phase three: loss of everyday life. With this pre-understanding in mind, a repeated data analysis process was completed.
The transcribed data were re-read to thoroughly investigate the conflicting variations in the relatives’ perceptions. Coding, grouping into categories and abstracting focused on the content of the relatives’ perceptions of and attitudes towards the three phases. The content analysis (Elo & Kyngas, 2008) led to an outline that shed new light on the relatives’ experiences of the progression of dementia. In this stage of the analysis process, two archetypes of relatives in a family of a person with dementia emerged as generic categories: the protective role and the decisive role.
Example of the abstraction in the inductive analysis process of identifying phase one.
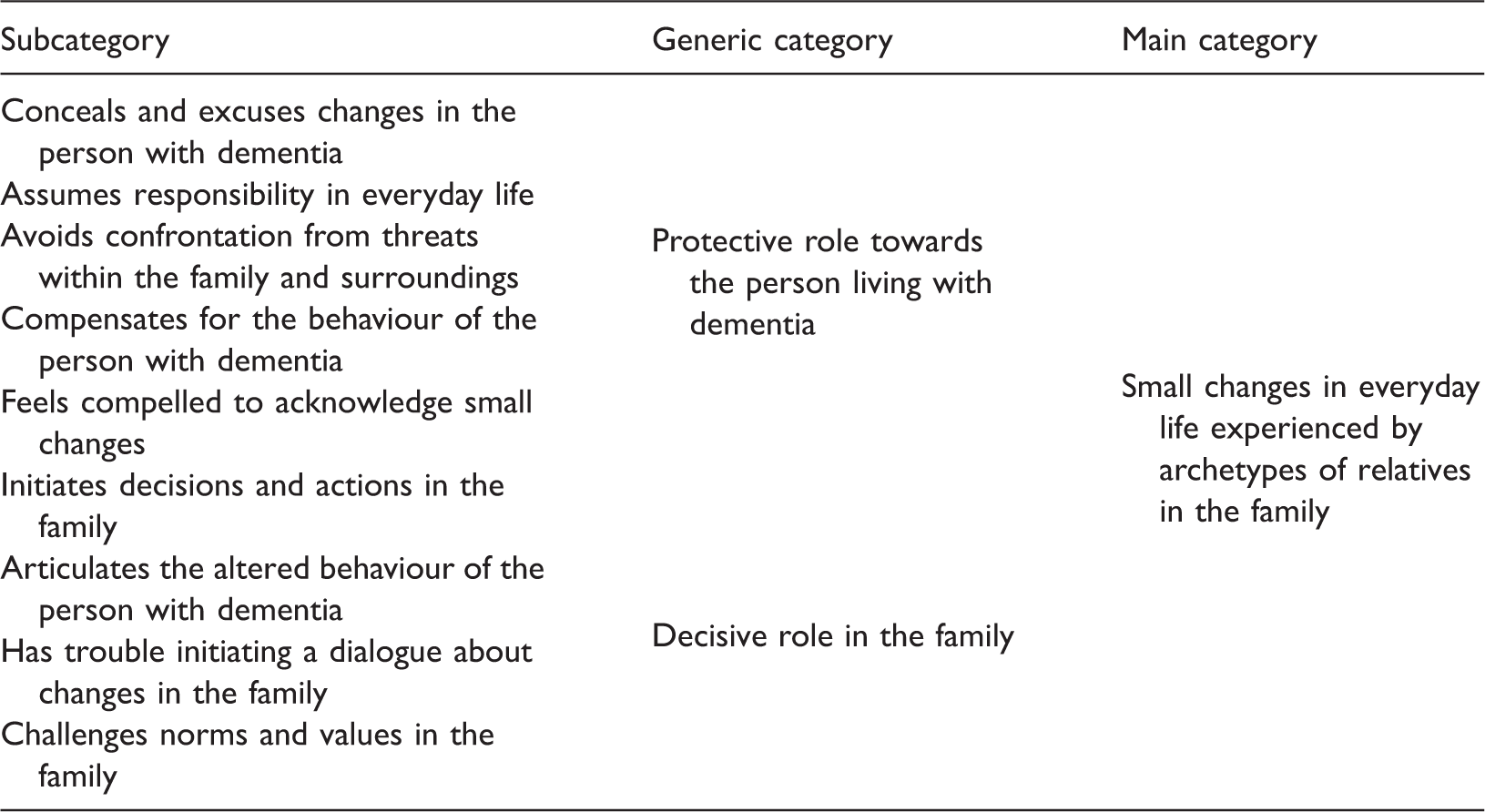
By compiling the analysis process, we were able to interpret the data in greater depth and to describe and develop subcategories within each of the phases experienced by the two archetypes; see Figure 1 for an overview of the phases and the subcategories.
Overview of the phases and the subcategories.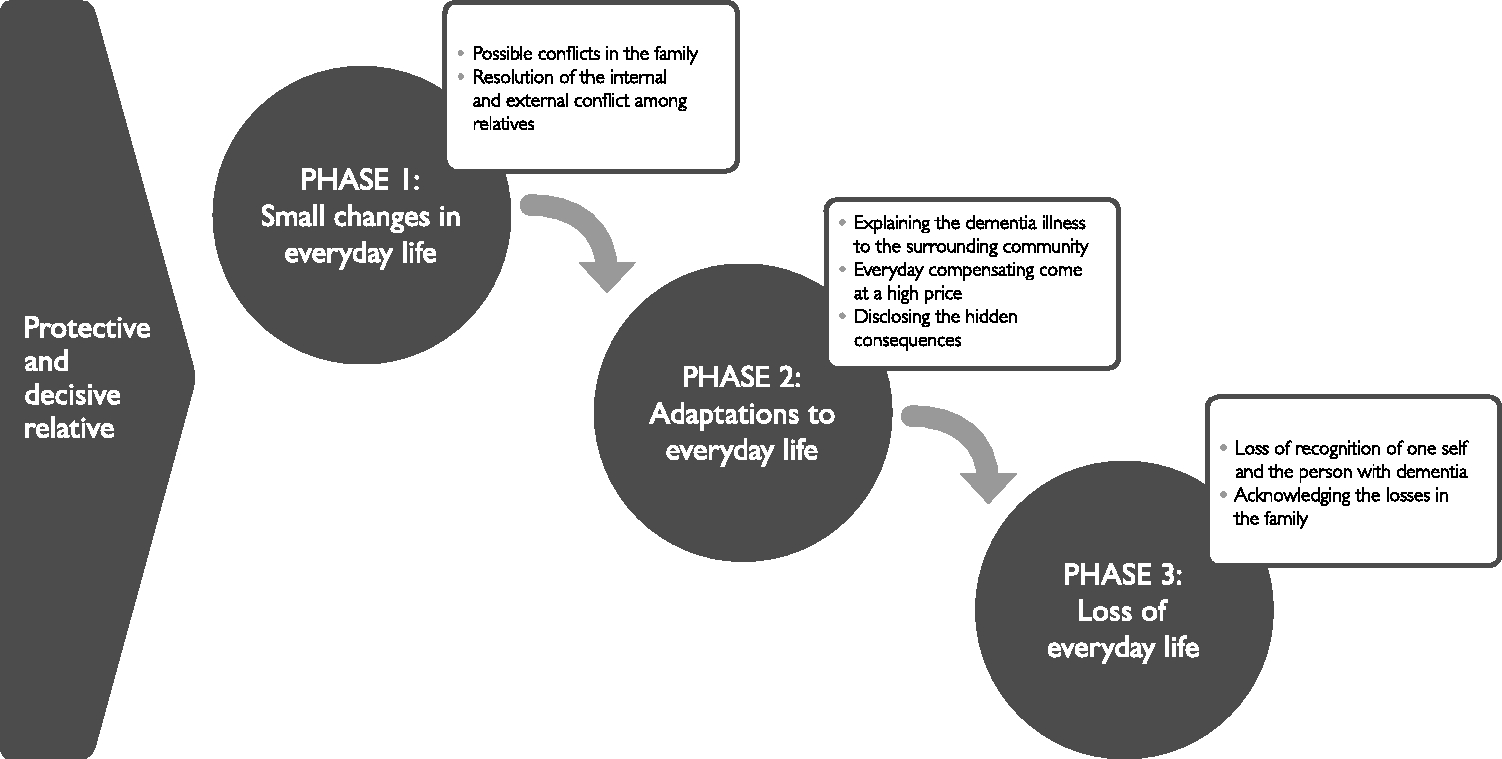
The first three authors contributed to and participated in all of the stages of the analysis process. The first three authors validated the transcribed data by listening to the tapes and reading the transcriptions and selected quotes that described the phases. Discrepancies in interpretations of the analysis process and results were discussed repeatedly with the fourth author to reach a consensus regarding the categories and findings (Patton, 2002).
Ethical considerations
The study was performed in accordance with the Helsinki Declaration (World Medical Association, 2013) and was registered with the Danish Data Protection Agency (§2014-54-0681). All of the participating informants were anonymized, and they provided written consent prior to participating. Every interview concluded with a debriefing. The informants were encouraged to contact the researcher if necessary. None of the informants did so.
Results
To enhance readers’ understanding of the findings, we first present the two archetypes of relatives. Then, we present the nuances of the three phases through the subcategories related to the archetypes.
Two archetypes of relatives
The data indicated a pattern of the following two archetypes of relatives in the families: the protective relative and the decisive relative. In all of the participating families, these roles appeared unintentionally and arose naturally from the family’s history and current circumstances. There was a tendency for the two archetypes of relatives to form early in the progression of the illness. However, the type of responsibility accepted by the relative seemed to be consistent throughout the phases of the illness.
The role of the protective relative
A characteristic of the protective relative is that he or she assumes practical responsibility in daily circumstances. The relative notices changes but does not want to admit them to him-/herself or confront the person with dementia or the people in his or her surroundings with the consequences of the situation. One daughter described this phenomenon as follows: This is why it took so long before we found out … that he had a condition. You repress it; you don’t want to see it. (Family D, Daughter)
The role of the decisive relative
The data showed that the decisive relative is a family member who previously had and currently has regular, positive, and close interaction with the person with dementia. A son provided the following statement: We have always helped each other out … I also talked him into … you must sell the house too … So I have been deeply involved all along. This is also because my little brother lived far away at that time. (Family E, Son)
A relative does not necessarily assume the role of the decisive relative consciously or freely. The data showed that the decisive relative often does not live with the person with dementia, perhaps because the relative who lives with the person with dementia on a daily basis is too close to the problem to identify the development and extent of changes. An important part of the role of decision maker is articulating the problems that occur as a consequence of dementia. There appeared to be a recurring pattern for the relatives to assume this role in the family. These relatives found that it WAS difficult to start a dialogue about the changes that they identified. One grandchild expressed this difficulty as follows: It actually ended up being me who held the first meeting with a health worker because my mother felt it was inappropriate to intervene in my grandmother’s life in that manner. (Family G, Granddaughter)
Description of and nuances in the phases of dementia progression
The inductive content analysis indicated that there were three phases. The phases are presented separately and as a simple linear process; however, the process of the three phases can continuously begin again. By identifying the three phases, we found that they were experienced differently. Furthermore, the analysis found additional subcategories in each of the phases with regard to the role that the informant played in the family; see Figure 1.
Phase one: Small changes in everyday life
The first phase is characterized by small changes in the behaviour of the person with dementia that are subsequently noticed by the family. One son discussed the gradual changes that he noticed in his father: I noticed that he didn’t remember things very well, and he found it difficult to recognize those who came to visit … But I wondered whether it was only because he was becoming old. (Family E, son)
Possible conflicts in the family
At this stage, the decisive relative experienced an internal conflict. Conflict arose when the relative experienced changes in everyday life that led to a concern about dementia. The relative was alone with these thoughts, generating a sense of ambivalence because none of the other relatives wished to ask whether something was wrong. However, the decisive relative was aware that something had to be done. One daughter described her experience of this internal conflict as being in opposition to the rest of the family in recognizing that something had changed: I constantly felt like I had to … retain my relationship with my old father, but I also had to explain to the family that there was something wrong. (Family F, Daughter) At first, I didn’t have my doctor’s support because he didn’t think anything was wrong … I thought that was horrible … that it was only me feeling this way … Everyone thought that I was only trying to put him in a nursing home. (Family D, Daughter)
Unlike the decisive relative, the protective relative experiences this phase as a threat to existing family life. He/she seems to experience the risk of exposure as potentially leading to an external conflict, in which the protective relative struggles with outside expectations of how a family should manage. A wife explained how she struggled with family members and caregivers’ intentions concerning the family’s need for help: I was offered help several times … but I don’t like having strangers in my home … not when I’m able to take care of him myself … I didn’t want anyone to know [about the husband’s advanced illness]. (Family E, wife) But then we could see that my dad was sneaking around afterwards to make sure that she had remembered to turn off the stove correctly. And this was just something he did, that is, taking care of everything and constantly looking after her. (Family H, Daughter)
Resolution of the internal and external conflicts among relatives
The resolution of all relatives accepting the changes in everyday life becomes conceivable when these changes can no longer be hidden from the surroundings and must be articulated. This phase seems to occur when the person with dementia becomes a danger to either him-/herself or another person, and the protective relative must agree with the decisive relative’s concerns. This transformation results in the family entering into a dialogue about the condition of the person with dementia. One daughter explained how her father became a danger to himself and others: The moment it occurred to us that … he was not safe, when we knew that we must say, ’Dear father, something has happened’, was when he didn’t handle his weapon properly. (Family C, Daughter) Then, he took a piece of meat from his plate and tried to put it into a bottle of red wine. I think this was the first time it occurred to my sister that … something is really wrong. (Family F, Daughter)
Both protective and decisive relatives must feel as though their feelings are legitimized with regard to potential internal or external conflicts for the family to relate to dementia and permit adaptation to the condition. Resolution, therefore, often occurs in connection with members of the family, broader society, and/or health professionals confirming that it is necessary to act on small changes. At this stage, the interactions between the person with dementia and the various family members (and the various roles that they assume) determine how early the relatives react to the condition.
Phase two: Adaptations in everyday life
The next phase is characterized by resolution and the family’s identification of dementia. The relatives experience life adaptations to the changes caused by the illness. Apparently, there is a change in the relationships with the person with dementia because the relatives must increasingly care for this person. For instance, one wife noted the following: I asked him several times, ‘Can you remember our new address?’ – ‘Yes, yes’ [the spouse with dementia responded]. And then I thought it would be OK if he got lost … he knows where he lives. (Family A, wife) We took turns bringing him … and sitting with him. (Family C, son)
Explaining the behaviour of the person with dementia to the surrounding community
The study showed that adaptations to everyday life include a need to explain the behaviour of the person with dementia because it does not correspond with the person’s behaviour prior to the diagnosis. For the protective relative, this process involves excusing the altered behaviour. This approach is motivated by the desire to avoid having the surrounding community view the person with dementia and his or her family differently. One wife discussed how aggressive behaviour must be explained to the surrounding world: It was incredibly painful that he wanted to strike out. He had always been so good in all the years that we were married. (Family C, Wife)
Protective relatives might not be able to articulate their need to share emotional and stressful experiences with others. In contrast, decisive relatives are good at seeking out and demanding opportunities for sharing. At this stage, it is characteristic of the decisive relative to seek articulations and explanations of dementia to find support and to understand why the person with dementia acts differently. One son explained this characteristic as follows: It is an enormous advantage to disseminate knowledge about having to consider things, and it would be good for the family that … somebody be present … and it may … lead to … it being possible to prolong the time that the person with dementia lives at home. (Family C, Son)
Everyday compensations come at a high price
As part of the new everyday life with dementia, there is a natural change in the distribution of everyday tasks. Chores previously performed by the person with dementia are transferred to relatives. Although all relatives participate in these chores, the protective relative naturally assumes greater responsibility because of the wish to be self-reliant, which is found in many families. As a result, this period can be experienced as exhausting because the protective relative is left alone with the person with dementia because he or she desires to cope with everyday life without interference. One wife explained this phenomenon as follows: Because in the beginning, I thought … [that] I was used to … taking care of yourself for as long as possible … and, therefore, I didn’t involve anybody in it. (Family A, Wife) We could also sense that my father increasingly took care of laundry. Small things like that, where he says: “Well, I have gotten good at it”. (Family H, Daughter)
Disclosing the hidden consequences
In many instances, the decisive relative notices how difficult it is for the protective relative to manage daily life and thus articulates the issue. The remaining family may feel a sense of guilt that the relative has managed to support the person with dementia on a daily basis. One daughter who assumed the role of the decisive relative described this effect: I feel intensely that … his wife … has done all the work and that she has not explained fully how it was … Because we talked about it for a long, long, long time before she admitted that she would have to do something. (Family C, Daughter) But then my husband required more and more help … he couldn’t help himself anymore. One time, when I had to help him after he had fallen, I could feel how it hurt my shoulder. Then, I said to myself: ‘No, now I have to get some help’. (Family A, Wife)
The dilemmas in adapting to the new life are that the family becomes accustomed to living with the condition and that the protective relative hides how difficult daily life has become. It appears as though the family is managing well as long as the protective relative compensates for the person with dementia on a daily basis, and the consequences of this compensation are only psychological and social. These consequences remain hidden from the family. A new situation occurs when the decisive relative discovers that the protective relative can no longer cope physically in daily life and thus can no longer compensate for the person with dementia. This new situation may lead both the protective and decisive relatives to realize that the family will inevitably experience a new everyday life, leading to the third phase of losses described next.
Phase three: Loss of everyday life
The final phase is characterized by the relatives experiencing a loss of their shared daily lives in the family. The dementia diagnosis has been known for a long time, and due to the progression of the condition, the changes in the behaviour of the person with dementia have become more comprehensive and invasive. The relatives in particular experience a reduction in regular activities and the increasing unpredictability of behaviour as substantial losses. The family experiences considerable changes in everyday life, and there is a need for help in sustaining a relationship with the person with dementia, which involves the decision to relocate the person to a care facility. This decision generates an understanding that the family has been permanently transformed. One daughter explained her experience of losing her mother: If one could say that a parent has been lost, physically … that is one thing, but this is not the case … We have lost her in a different way, but she is still there physically. (Family H, daughter)
Loss of recognition of oneself and the person with dementia
The two archetypes of relatives express a general sense of loss when losing the person with dementia to the illness. During this phase, this sense of loss is expressed in various fashions. The personality of the person with dementia is altered such that it becomes difficult to recognize the person. One son explained how his father was no longer the same: The thing about this bloody condition is that it changes your personality completely, right? In many ways, you become an empty husk. (Family E, Son) I think … it is probably difficult for them now that he is having difficulties … Who will they visit? (Family B, Wife)
Acknowledging the losses in the family
Another aspect is the loss of confidence in the person with dementia because the person becomes unpredictable and a danger to him-/herself or others. The protective relative, in particular, experiences difficulties in this area. It is no longer possible to trust the person with dementia. One wife noted this difficulty: And, finally, when he was home, then he began to want to leave home. I remember once when I took garden waste to the landfill – when I came back, the neighbour told me that he had left. (Family C, Wife) I simply decided that I could not manage to come up here. (Family C, Daughter)
There is one final type of loss that the families experience: the loss of collective memories. Both types of relatives must accept that the person with dementia can no longer participate in the family’s everyday life. The family will never be the same again. It is difficult for the protective relative, who has aimed to retain the relationships and illusions of the original family, to accept this loss. One spouse related the following: I can’t really bring her because it is … far too difficult. And she knows that she can’t come because I tell her every time I do something. (Family H, Husband) Of course, you have to visit … I don’t want to see my dad … I don’t enjoy it. But, I need to visit … to ensure that everybody is okay. I know it sounds harsh. (Family C, daughter)
In another family, a daughter with the protective role explained her attempts to include the person with dementia in the new everyday life after institutionalization: She [my mother] is always at the grandchildren’s birthdays. I always bring her … She has to … Oh yes. Otherwise, it would be wrong. (Family G, daughter)
Discussion
The purpose of this study was to examine how family members experience the challenges of everyday life throughout the progression of dementia.
The study identified three overall phases in the progression of dementia from the perspectives of the relatives. This division was confirmed by the literature in the field (Daly et al., 2013; Forbes et al., 2012); the innovation in our results is that they include experiences regarding the full progression of the condition, from the first sign of dementia to at least six months after admission to a care facility, and they emphasize family relationships. Other studies have emphasized the relationship between the person with dementia and an individual relative (Quinn et al., 2015; Sanders & Power, 2009). The distinguishing feature of these studies was that the phases, from the perspective of the relatives, differed according to which role the relative played in the family throughout the progression of the illness. In addition, these findings suggested that the relatives’ resources and needs during the three phases could not be understood solely from a linear perspective; rather, the subcategories associated with one phase could resurface later in another phase. An example of this complexity is seen in the case of the identified internal and external conflicts among the two types of relatives in phase one and again in phase three. This example illustrates the possibility that the subcategories within the model of phases are independent of the medical progression of dementia. One potential reason for this finding is that relatives are constantly, not only around the time of the diagnosis of dementia, confronted with new changes and challenges in everyday life because of the behavioural changes of the person with dementia caused by the illness. The model of phases developed in this study might therefore more appropriately follow a dynamic approach; hence, the process of the three phases could be represented as continuously re-starting from the beginning of phase one, as illustrated in Figure 2 by adding a possible dynamic process represented by the dotted line. In health work, it is common for a person to have to revisit previous steps in a process of change to attain a higher level of understanding and greater capacity to act (Holzkamp, 1983; Prochaska & Velicer, 1997). The suggested dynamic approach must be further explored regarding possible movement within and between the phases. Further research is necessary to verify whether the dynamic representation is viable.
A dynamic representation of the phases.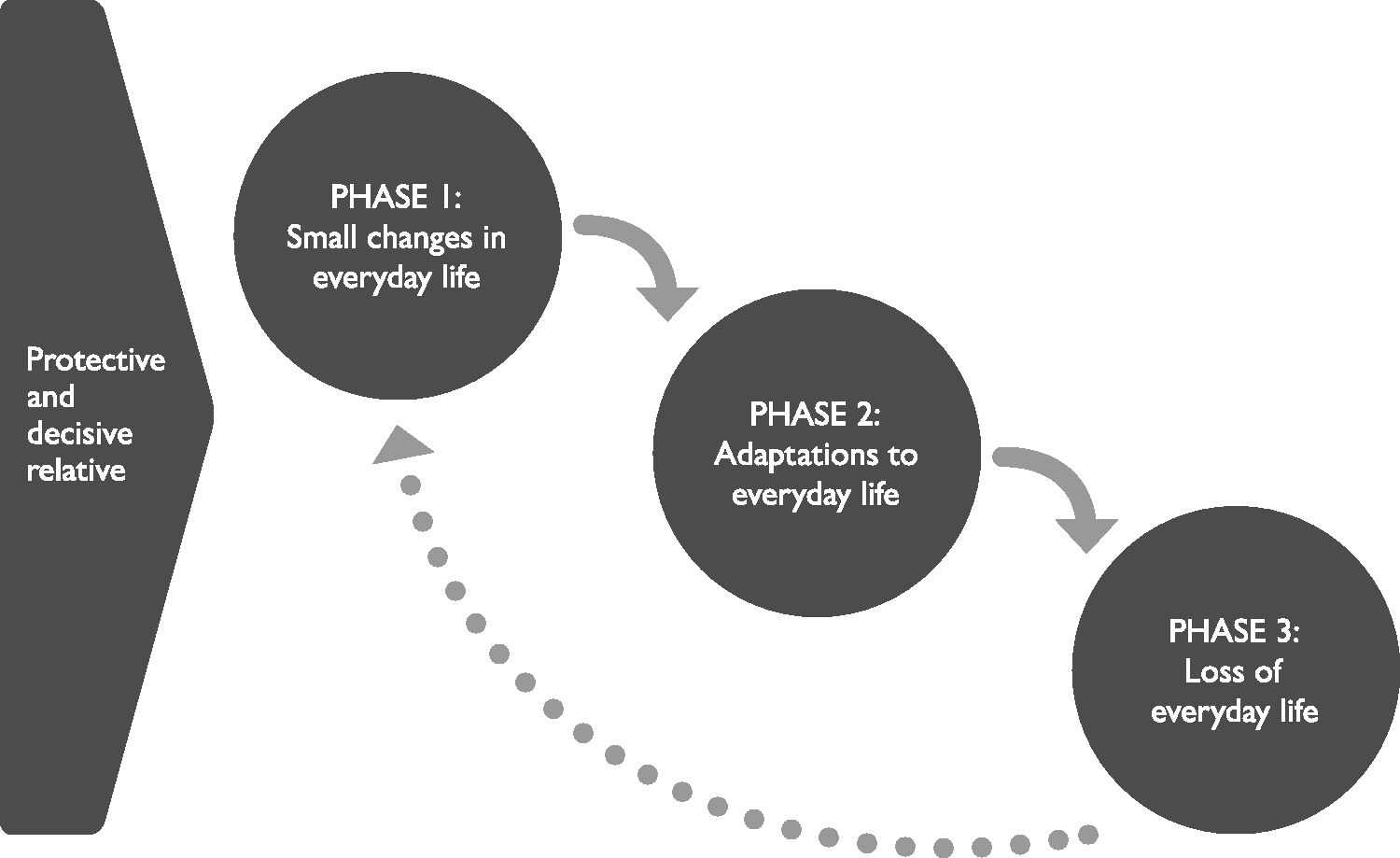
Theories of change in connection with illness have often adopted a more linear approach to the progression of the condition as having a beginning and an end (Gibbons, Ross, & Bevans, 2014; Kralik, Visentin, & Van Loon, 2006). However, in cases involving chronic illness, progression is likely not linear because the families of persons with dementia constantly identify new challenges that they must adapt to and overcome (Kralik et al., 2006). From the perspective of the relatives of persons with dementia, the phases involve a dynamic process in which changes occur, the family responds to the challenge, and then a new change occurs and the process repeats.
A key finding of this study is that there are two archetypes in the family. Archetypes refer to stereotypical references that exist deep in the human collective consciousness. Archetypes thus constitute a universal way to understand the relatives’ experiences of their roles (Smythe & Baydala, 2012). All families recognize a pattern; therefore, the discussion can extend beyond defining a close relative merely as a caregiver. In this study, the roles of the relatives appeared to be stable throughout the progression of the illness. When a systemic approach is used, it is possible that the reactions of the person with dementia affect the family dynamics. This particular aspect has not been previously explored. A family systemic approach revealed that there are different tasks that must be managed in the family (Haefner, 2014). Often, the spouse who lives with the person with dementia on a daily basis assumes the protective role. Therefore, a different relative must accept the role of the decisive relative.
The role of the decisive or protective relative is natural to some relatives, whereas other relatives experience being forced into a role. From the perspective of family systems theory, this process is called ‘triangling’. There is tension between various family members as they attempt to manage a difficult situation, such as a dementia diagnosis (Goodell & Hanson, 1999; Haefner, 2014). In such a triad, when one member of the family changes his or her behaviour because of dementia, another family member will step in and take over his or her role – including the role of protective relative. To retain the balance in the family, the decisive member must adapt his or her behaviour (Goodell & Hanson, 1999). This necessary adaptation may be experienced as positive and enriching, but some of the informants expressed that this perception was not always the case. Kralik et al. (2006) explained that the individual’s identity is threatened and that the transition process, which is the basis for a new and positive identity, requires time. However, decisive relatives do not necessarily have such time during the progression of the condition. Another study also identified different roles throughout the progression of the illness (Caron & Bowers, 2003). In contrast with the findings of our study, this previous study suggested that the relative’s role changes concurrently with the increasing need for caregiving. The relative’s role with regard to the person with dementia shifts focus from maintaining life, as it previously was to maintaining the emotional and physical comfort of the person with dementia (Caron & Bowers, 2003). The two roles in our study were not necessarily played by only two relatives in the family. We have examined only the phenomenon of two archetypal roles from the perspective of eight families. It is possible that several relatives in a family adopt the protective or decisive role. Although this study only examined eight families and in some families only one family member agreed to participate, both archetypes within the families were mentioned in all interviews. Furthermore, the distribution of archetypes is unknown when there is only one relative in the family. The presence of the archetypes and the nature of how they are distributed within the family warrant further exploration.
In the initial phase, it may be important for the decisive relative to experience internal conflict about being alone with regard to his or her suspicions that the small changes in everyday life displayed by the person with dementia indicate symptoms of a serious medical condition. Thus, the decisive relative may have a greater need for support from the surrounding community at this stage of the condition. Members of the community can support the decisive relative by articulating concerns so that the relative does not feel alone in bringing the family out of balance (Schulz & Sherwood, 2008). F. Ducharme et al. (2013) studied family conflicts and found that female caregivers experience more conflicts in the family than male caregivers do. Furthermore, the spouse of the person with dementia has fewer family conflicts than the children (F. Ducharme et al., 2011; F. Ducharme et al., 2013). These findings were similar to the results of our study. Differences in what is perceived to be difficult to manage as a relative may be related to gender (Greenwood & Smith, 2015). However, in our study, there was no correlation between gender and experiencing conflict. This finding was in agreement with another study suggesting that the experiences of relatives of a person with dementia are influenced by the quality of the relationship before the diagnosis (Caron & Bowers, 2003). It is possible that the distribution of the archetypes is also dependent on this relationship, but we did not analyse this possibility in the present study. Our study suggests that how and when family imbalance is experienced as a conflict depends on the role that the relative plays. In family systems theory, the effect of a change in the family varies in intensity and quality among family members. A discrepant view among family members can have an important influence on the individuals’ self-identity because the family provides the initial experience of self-awareness and helps members to become acquainted with who they are (Kaakinen et al., 2015). As a consequence of the protective and decisive relatives’ different experiences of conflict, it becomes necessary for the relative with the outside view to balance his or her own needs with the needs of the family and the person with dementia. Quinn et al. (2015) has termed this process ‘balancing needs’. The current study found this balancing act during the initial phase, i.e. when the decisive relatives performed the necessary tasks. In the second phase, these relatives must increasingly consider the family’s and their own needs. This change has the unfortunate consequence that the decisive relative withdraws from the remaining stages, as indicated by the informants. In family systems theory, this withdrawal can be viewed as an ‘emotional cutoff ’ (Goodell & Hanson, 1999), suggesting that the decisive relative experiences the internal conflict as a substantial challenge and is forced to distance him-/herself from the other family members, in this case, the person with dementia. The decisive relative becomes geographically or emotionally distant (Haefner, 2014). In the present study, the same pattern was identified in several families. The decisive relative withdrew physically or emotionally from the person with dementia and from the family to some degree.
The second phase identified in this study is characterized by the family – with its new knowledge of dementia – attempting to maintain everyday life as much as possible. The responsibility for this task often falls on the protective relative, who naturally has the greatest contact with the person with dementia in everyday life. The protective relative compensates for the changed behaviour of the person with dementia, which is a substantial burden. This finding has been described in general terms in studies concerning relatives’ experiences of the progression of dementia (Campbell, 2008; F. Ducharme et al., 2011; Stephan et al., 2013). Our study adds to this literature by showing that the protective relative does not recognize the burden, until it becomes physically too difficult for him or her to maintain the perception that the person with dementia is living an unchanged life. A literature review of relatives’ experiences showed relatives’ strong need to preserve everyday life by maintaining an active role in the family for the person with dementia (Bunn et al., 2012). The present study also found this experience in that the protective relative naturally sought to hold onto a previous relationship with the person with dementia. Here, the protective relative was especially motivated by the desire to be self-reliant and to not require help from the remainder of the family or professionals. Thus, it can be difficult for the protective relative to accept the need for help before physical limitations force him or her to surrender.
It appears as though the relatives are motivated to retain the relationship and the sense of everyday life for different reasons, including to be self-reliant, through a sense of decency towards the person with dementia, or to attempt to retain one’s own identity. This variability in motivations was also recognized by Quinn et al. (2015). In these authors’ study, the relatives did not see any other option than to care for the person with dementia (Quinn et al., 2015). In addition, Hodgins et al. (2011) found that the extent to which relatives are motivated by duty depends on the quality of the relationship before the dementia diagnosis. This phenomenon was also found in the current study, in which the spouses, in particular, adopted the role of protectors. Spouses had very different perceptions of what was experienced as a burden and as difficult in the relationship. Several spouses explained how difficult it was to ask for help and that it was easier when the family was able to talk about problems. For health professionals, this finding has special relevance. It might be necessary for the professionals in contact with the family to seek knowledge about what constitutes a physical, psychological or social burden in the family on a daily basis (Hjortbak & Rehabiliteringsforum Danmark, 2011; Marselisborgcentret & Rehabiliteringsforum Danmark, 2004; Quinn et al., 2015).
The third phase is characterized by the various experiences of loss for all of the involved relatives. The differences between the challenges that the two types of relatives face are not as clearly distinguished as those in the previous phases because the first two phases are more challenging than the last phase. This phenomenon can also be found in other theories that consider phases (Meleis, Sawyer, Im, Messias, & Schumacher, 2000). An interesting feature of the last phase is that the relatives struggle to accept the transitory nature of daily life in the family. It is important for both the protective and the decisive relatives that the situation be resolved and that the need for action to be taken becomes apparent to everyone. It is possible to move forward in the last phase only after this point has been reached. By meeting the relatives’ needs, health professionals can help them through the transitory process such that the family can collectively resolve the challenges caused by dementia (Kralik et al., 2006).
During the final phase, all relatives seek information about the everyday wellbeing of the person with dementia. The reasons why the two archetypes of relatives seek such information differ. The protective relative is driven by care for the person with dementia, whereas the decisive relative is driven by guilt about whether the changes have been managed satisfactorily. From a family systems approach, families subjected to an extended period of stress tend to repeat unhelpful behaviours and to scapegoat individual family members to retain a sense of balance (Haefner, 2014). This response can be directed towards the decisive relatives in this study. In the third phase, the decisive relatives feel a sense of guilt and identify themselves as the scapegoat, feeling that they have forced the person with dementia into a care facility. Due to feelings of uncertainty about whether the right decision has been made, the decisive relative may avoid contact with the person with dementia.
A considerable limitation of this study was the small sample size of 14 informants, making generalization difficult. Additionally, the retrospective design of the study led to the risk of recall bias. In the interview situations, the informants were urged to elaborate on their earlier experiences. A longitudinal study during the progression of the illness with more informants could contribute to the findings of this study.
Another limitation of the current study concerned the recruitment of the informants in the eight families. We decided to have nurses at the care facilities initially contact the informants. Therefore, the basis for consecutive selection was influenced by which families the nurses considered viable to contact. We had no knowledge about which families were not selected. It is likely that the families that communicated best with health professionals were selected over other families. This selection bias may be a problem because the most capable families might be those who were able to maintain good relationships (Staniszewska & West, 2004). Thus, the informants might have been better at reflecting on the conflicting emotions that occur in the progression of the illness than members of other families. In fact, the ability to communicate and set expectations as a recipient of services from health professionals determines how the progression of the illness is experienced (Duclos et al., 2005).
An additional limitation with regard to contact with the informants was that the relatives in some of the families did not permit interviews with additional family members. This reticence indicated that the informant sought to protect other relatives. Thus, we were not able to obtain a more nuanced understanding of the participating families. As a result, we were not able to cast light on the existence of archetypes in some of the families, and we instead interpreted the various roles and functions held by other family members. The interesting feature of this limitation is that it supported the primary finding of the study, namely, that there are two archetypes: the decisive relative and the protective relative. In the cases in which initial contact was made through a protective relative, it was more difficult to gain access to other family members.
Furthermore, an overall limitation of this study was the use of content analysis. During the qualitative analysis process, the developed concepts are only abstractions devised by the researchers (Botes, 2002; Morse, Mitcham, Hupcey, & Tason, 1996). Hence, this study was not based on a theoretical framework. Thus, although the findings presented here contribute to the development of knowledge concerning the growing burden of caregivers of persons with dementia, further research is needed.
Conclusion
Adopting a family-oriented approach, this study identified three phases in the progression of dementia. The primary findings were that the phases are experienced according to the role that the relative holds in the family in relation to the person with dementia. Despite the small sample size, this study identified the following two archetypes: the protective relative and the decisive relative. Furthermore, the two archetypes may experience the three phases in a nonlinear manner. In other words, the relatives continuously experience challenges throughout the progression of dementia and must adapt to these changes and losses in everyday life. A greater understanding of each of the archetypes’ experiences during the identified phases is necessary when providing care to a family of a person with dementia.
The arbitrary findings of the inductive analysis supported the existence of two archetypes throughout the three phases. However, the provisional nature of the findings indicated the need for further exploration of how the archetypes’ roles are developed and distributed within the family.
One recommendation for practice is for health professionals to attend to the experienced phases and roles within the family. Such attention could help health professionals to facilitate the inclusion of relatives’ resources throughout the progression of dementia. There is a need for future research into the efforts that are necessary to support families. Such studies could profitably adopt an interdisciplinary approach because of the complexity of the illness.
Footnotes
Acknowledgements
We would like to thank the local government in Fredericia, including our contacts and the management. We would also like to thank the families who participated in the interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was developed on the basis of an interdisciplinary research project supported by the Health Sciences Research Centre at University College Lillebaelt in Denmark and the Department of Nursing, the Department of Physiotherapy and the Department of Occupational Therapy at University College Lillebaelt.