
Abstract
The Cognitive Daisy is an innovative assessment system created to provide healthcare staff with an instant snapshot of the cognitive status of older adults in residential care. The Cognitive Daisy comprises a flower head consisting of 15 colour coded petals depicting information about: visual-spatial perception, comprehension, communication, memory and attention. This study confirmed the practicality of the Cognitive Daisy protocol for assessing cognition in a sample of 33 older adults living in residential care and endorsed the use of the Cognitive Daisy as a tool for recognising the cognitive status of care home residents.
Introduction
Dementia is a heterogeneous condition, the cognitive and behavioural sequelae of which are modified by individual variation in brain structure (Alexander-Bloch, Giedd, & Bullmore, 2013), premorbid cognitive status (Lo & Jagust, 2013), aetiology (McKeith, 1994) and progression (Giebel et al., 2014). Relations between cognitive dysfunction and problematic behaviours in dementia are frequently conceptualised within a needs-driven dementia-compromised behaviour model (Algase et al., 1996). According to this theory, needs-driven dementia-compromised behaviours (e.g. aggressive actions) constitute expressions of unmet needs, triggered by proximal factors (e.g. noisy environments) in people with predisposing background factors (e.g. disinhibition). Indeed, older adults in residential care with cognitive impairments experience increased levels of agitation (Cohen-Mansfield, Marx, & Rosenthal, 1990) and display more negative dementia-related behaviours (Boustani et al., 2005). Although the concept of challenging behaviour in dementia has been questioned (Swaffer, 2015), cognitive impairment also increases the likelihood of falling (Whitney, Close, Jackson, & Lord, 2012) and modifies how individuals with dementia express their needs and interact with others (Morris & McKiernan, 1994). Recognising inter-individual variation in the cognitive abilities of care home residents is therefore fundamental for the delivery of high quality person-centred care yet poses a significant challenge for care workers who face many emotional and physical pressures (Gandoy-Crego, Clemente, Mayán-Santos, & Espinosa, 2009).
In this paper, we introduce the Cognitive Daisy (COG-D) – an innovative method for providing care staff with a succinct visual depiction of an individual’s cognitive status. The COG-D (see Figure 1) comprises a flower head consisting of 15 petals, each of which is colour coded and corresponds to performance on a specific cognitive task (e.g. face recognition, sustained attention, speech production, comprehension, etc.). A copy of each resident’s COG-D is placed in a discrete area of their room, in their care plan portfolio and is displayed in the office of the care home manager. The primary aim of the COG-D is to remind care staff at a glance of the severity of problems within different cognitive domains. These can then be used to adjust interaction with the resident, thereby improving communication, reducing agitation and enhancing person-centred care. Here we evaluate the practicality of the COG-D assessment protocol and examine whether the COG-D helps care staff to become more aware of the cognitive strengths and weaknesses of the residents they care for. To explore these questions, COG-D was introduced to residents and care staff in six residential care homes for older people and its usefulness was evaluated through questionnaires completed by care staff before and after the training and intervention phase.
The Cognitive Daisy and two examples of residents’ daisies. The top example depicts an individual with selective deficits with inhibitory control and verbal fluency. The example below depicts an individual with pervasive cognitive deficits but preserved comprehension.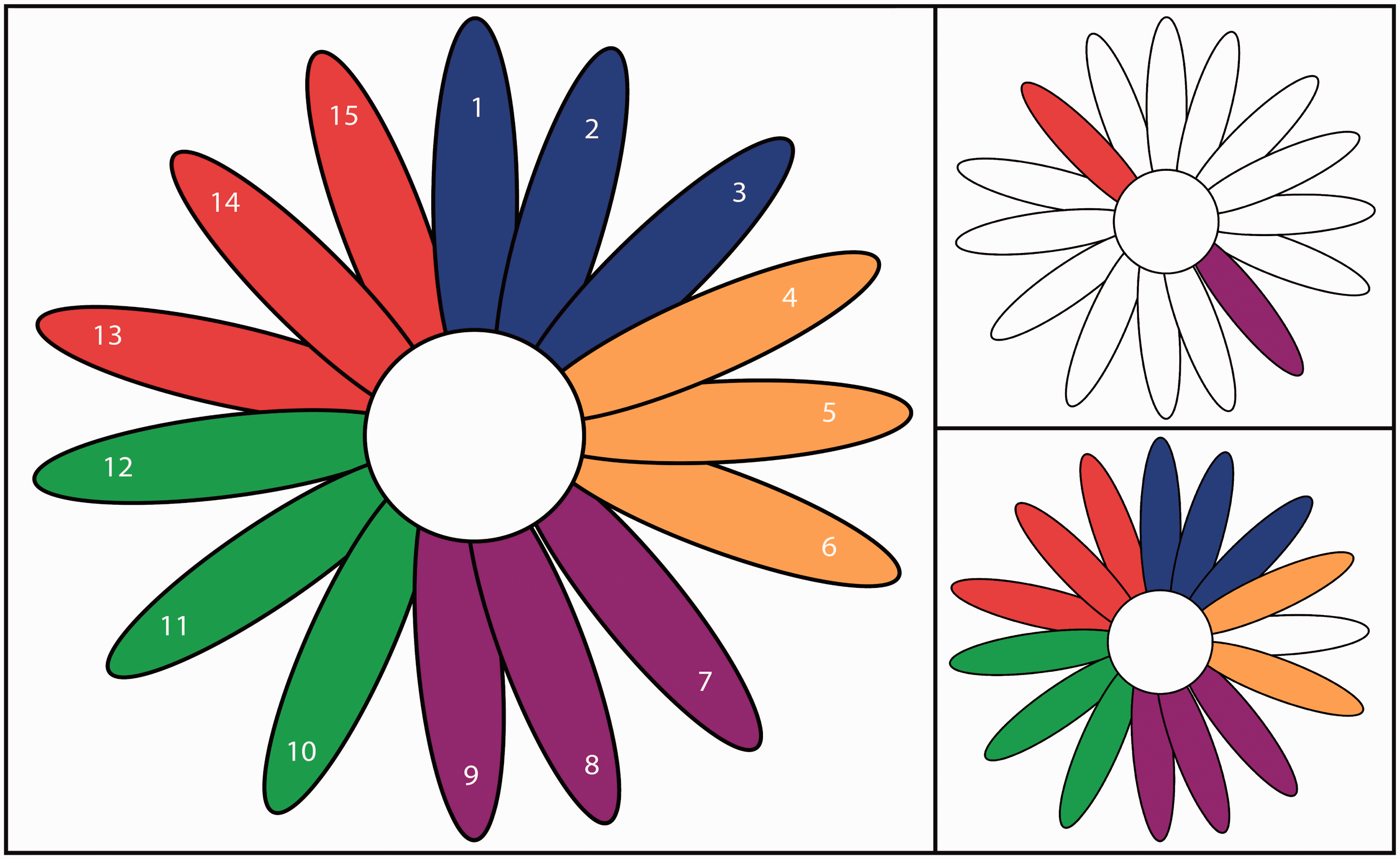
Method
Participants: Twenty-nine senior care staff, all of whom were women, and six men and 27 women (mean age = 87.23 years, range = 74–96 years) from six residential care homes in Lincolnshire, UK participated in this study. In addition, we collected comparison data from 50 older adults (20 men/30 women; mean age = 78.39 years, range = 70–90 years) living in the community. All participants gave informed consent prior to participating in the study. The investigation was approved by the ethics committee of the School of Psychology, University of Lincoln.
Stages of the care home study: The study comprised five stages.
COG-D (neuropsychological) assessment of residents, interpretation of data and construction of individual COG-Ds. Assessment of baseline knowledge of care staff with COG-D (I) questionnaire. The COG-D training session. Application of the COG-D: A two-week period where care staff used the COG-D on a daily basis. Assessment of knowledge of cognitive problems and evaluation of the usefulness of the COG-D for care staff with COG-D (II) questionnaire.
Test characteristics and performance on the COG-D assessment battery as a function of group.
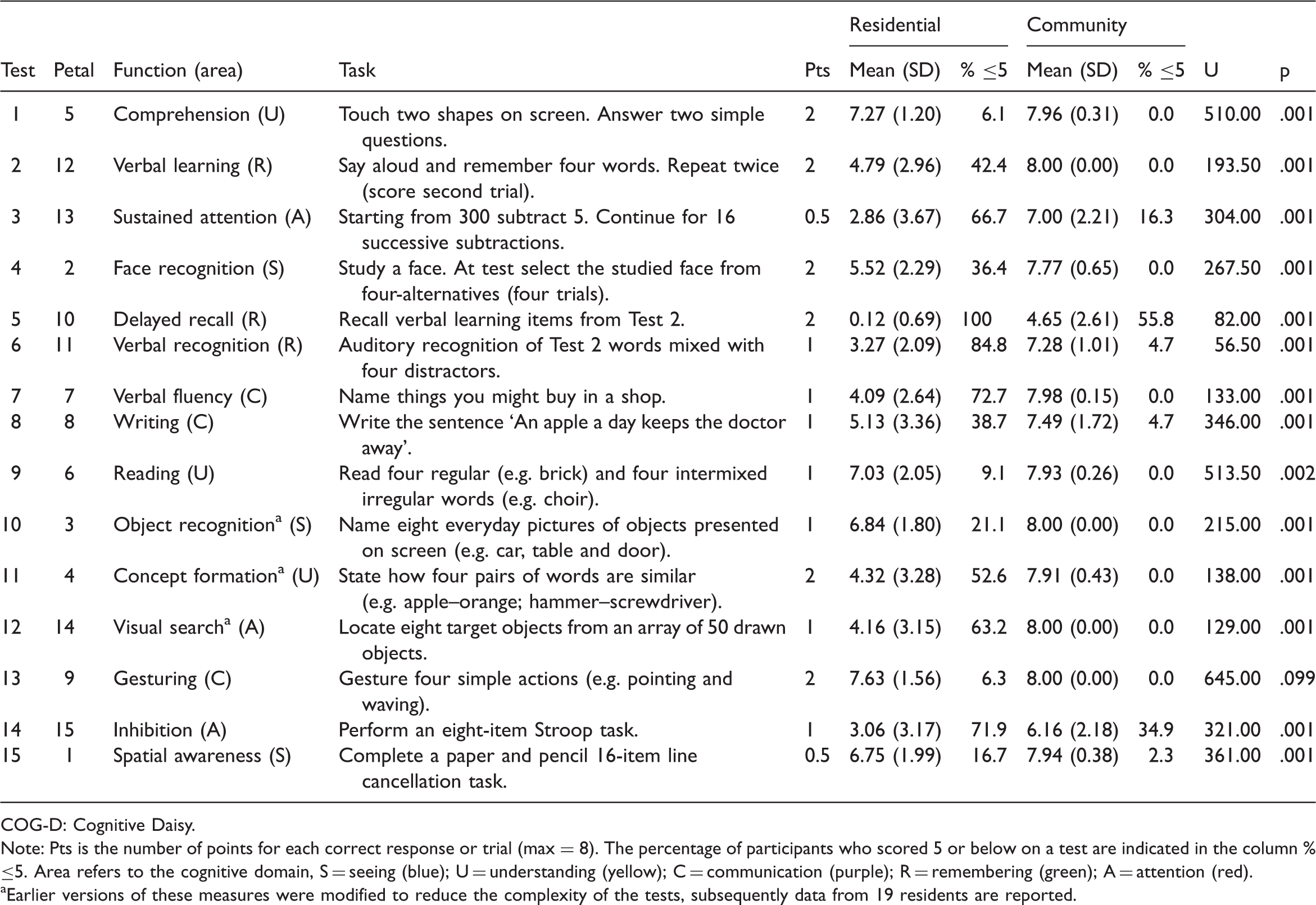
COG-D: Cognitive Daisy.
Note: Pts is the number of points for each correct response or trial (max = 8). The percentage of participants who scored 5 or below on a test are indicated in the column % ≤5. Area refers to the cognitive domain, S = seeing (blue); U = understanding (yellow); C = communication (purple); R = remembering (green); A = attention (red).
Earlier versions of these measures were modified to reduce the complexity of the tests, subsequently data from 19 residents are reported.
Cognitive Daisies: The data from the assessment was used to create a COG-D for each resident. Each COG-D consisted of 15 petals (see Figure 1) representing five cognitive domains which were colour coded as follows: visuospatial perception (blue), comprehension (yellow), communication (purple), verbal memory (green) and attention (red). Each domain of cognition was represented by three petals. The level of impairment within a domain was indicated by the number of coloured petals, cognitive strengths were depicted by white petals. If a test was not performed, the corresponding petal was coloured grey. The position of each petal within a cognitive domain corresponded to a specific function (e.g. blue petals depicted visuospatial perception: position 1 = spatial awareness; position 2 = face recognition; position 3 = object recognition). Each resident’s COG-D (85 mm × 85 mm approx.) was displayed in a discrete but visible place in their room. A more detailed version of the resident’s daisy, which included a description in non-technical terms (e.g. spatial awareness = ‘seeing both sides of the environment’) of each cognitive function associated with each petal, was included in their care-plan folder and in the office of the care home.
COG-D training: Care staff participating in the study attended a 1.5 hour training session led by the authors. The main objective of these sessions was to explain the concept of the COG-D and to ensure an understanding of how the different cognitive domains were represented by different coloured petals. Given the variation of pre-existing knowledge about cognitive dysfunction in dementia, we described the COG-D components to care staff using accessible language, such as
COG-D Questionnaires: Care staff completed pre and post-intervention questionnaires referred to as COG-D (I) and COG-D (II), respectively. Both measures incorporated open-ended questions that required care staff to list cognitive problems associated with dementia and to state how they impact on daily life. In addition, care staff indicated on a 10-point Likert scale: (1) the importance of understanding cognitive problems for delivering person-centred care; (2) how difficult they found it to remember residents’ specific cognitive problems; (3) whether they thought a visual prompt would be useful as a reminder of individual cognitive difficulties. In addition to these four items, COG-D (II) also required care staff to indicate whether they agreed with the statements: (1) it is important for residents to have a cognitive assessment; (2) the delivery of care should take into account the unique cognitive problems of residents; (3) the COG-D will help care staff recognise cognitive strengths and limitations; (4) the COG-D will facilitate the delivery of care in residential homes.
Results
Data from six community participants who scored at or above the cut-off (8) for cognitive dysfunction on the 6CIT and one participant with an uncorrected visual impairment were excluded from further analyses. The remaining participants (19 men/24 women; mean age = 78.40 years, range = 70–90 years) had a mean 6CIT score of 2.93 (range = 0–6).
COG-D Assessment: Following initial observations we modified the measures of object recognition, concept formation and visual search:
Object naming: Residents were presented with line drawings of eight everyday objects on a computer screen and asked to name each one. Most residents were unable to name some of the objects but could name others. We therefore decided to (1) change the format and present each object singly; (2) use colour photographs of objects instead of drawings; (3) replace objects that might be perceived ambiguously and present all objects from a stereotypical viewpoint.
Concept formation: This measure involved pointing to two objects from the object naming test that could be used to perform a specified task. Because of the problems outlined above, we replaced this task with a standard similarities test.
Visual search: Originally this measure involved performing a coloured trails task. None of the residents managed to complete this test and no common errors were observed. We consequently substituted this test with a visual search task which requires residents to find several target stimuli that are dispersed among many distractors.
All the older adults living in the community and all the care home residents bar one completed the modified COG-D assessment battery. The mean scores for both groups on each test are presented in Table 1. Cronbach’s alpha revealed the battery had a high level of internal consistency (15 items; α = .935). Cronbach’s alpha scores for each cognitive domain (three items) were as follows: visuospatial .813, comprehension .638, communication .552, verbal memory .817 and attention .838. Significant Spearman’s correlations were found between 6CIT months backwards and the COG-D Stroop measure of inhibitory control [r = −.407, p = .007] and between 6CIT delayed recall and COG-D delayed recall [r = −.586, p = .001], verbal recognition [r = −.499, p = .001] and Stroop [r = −.427, p = .004]. This indicated concordance between 6CIT indices of working memory and consolidation and those derived from the COG-D test battery.
COG-D Questionnaires: The cognitive problems in dementia that were named in COG-D (I) by care staff were mainly behavioural (e.g. incontinence, aggression) or psychological (anxiety, depression). The percentage of care staff who stated impairments pre- vs. post-intervention which corresponded with the primary cognitive functions as depicted by the COG-D were as follows: visuospatial (26% vs. 63%), comprehension (22% vs. 71%), communication (52% vs. 79%), memory (70% vs. 83%) and attention (11% vs. 58%). Exact McNemar’s tests determined that the COG-D intervention significantly raised awareness in care staff of visuospatial (p = .006), comprehension (p = .001) and attention (p = .001) problems in dementia, but not of communication (p = .109) or memory (p = .289) impairments.
On a scale of 1 to 10 where 10 means that the statement is strongly endorsed, all care staff thought it was extremely important to understand the cognitive problems of residents for delivering person-centred care in both pre (mean = 9.93, SD = 0.26) and post-intervention responses (mean = 9.74, SD = 0.53). There was no significant difference in their pre- and post-intervention responses [t (26) = 1.727, p = .096], indicating that participation in the study had not altered their perception of this principle. On COG-D (I), many care staff indicated that it was quite difficult to remember residents’ specific cognitive problems (mean = 6.86, SD = 1.92) and thought that a visual prompt would be useful (mean = 8.93, SD = 1.77). As can be seen in Figure 2, post-intervention responses clearly showed that the implementation of COG-D had made it significantly easier for them to remember the cognitive problems of residents [t (26) = 8.016, p = .001, η2 = 0.71] and was rated as being extremely useful (mean = 8.89, SD = 1.45). The value of COG-D was unrelated to whether care staff thought a visual prompt of cognitive problems would be useful in the pre-training phase [r = .345, p = .078]. Care staff further stated that it was important for residents to have a cognitive assessment (mean = 9.76, SD = 0.58) and that the delivery of care should take cognitive problems into account (mean = 9.93, SD = 0.26). Notably, they believed that the COG-D would help staff recognise cognitive strengths and weaknesses (mean = 9.82, SD = 0.55) and enhance the delivery of person-centred care (mean = 9.41, SD = 1.18).
The reported level of difficulty for each carer to remember the cognitive problems of individual residents before using the COG-D (grey bars) and with the COG-D (black bars). Two care staff failed to fully complete COG-D (II) (n = 27).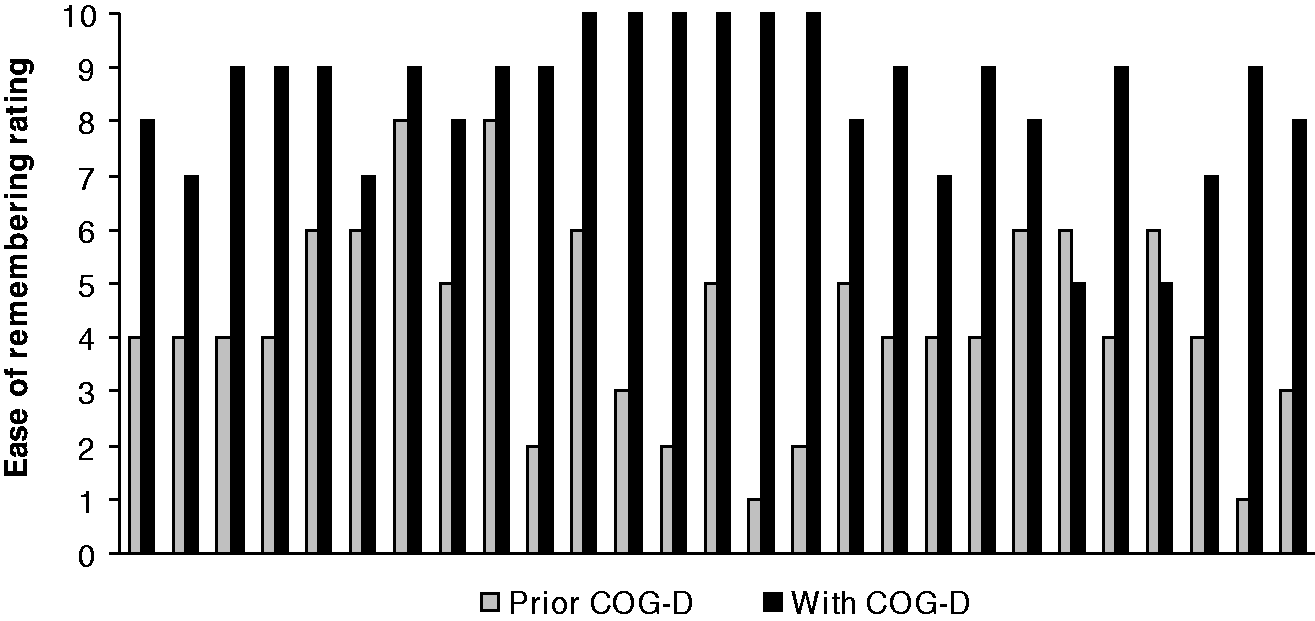
Examples of qualitative responses
The whole aspect of the Daisy is very useful in order to help the staff recognise cognition strengths and limits in order to deliver a good standard of care.
After reading the results of COG-D I was able to better support individuals in areas where I knew there was a deficit but equally important I was able to encourage individuals to be independent with areas where no/little deficit was present.
By using the Daisy I was able to pick up on sensory impairments and amend care notes to inform staff. By having the information as a team we were able to approach B.R in an appropriate manner. Reducing stress and improving communication skills. Also improved communication between health professionals supporting B.R. By using the Daisy it gave me a better awareness of individuals’ abilities and needs – improving person centred care.
The way it has been explained and put into different categories i.e. the cognitive problems each individual can have I feel is extremely useful and interesting to care staff. It is simple and easy to understand.
The daisy would work very well to provide person centred care for all persons that are involved with that resident from care staff to friends and family or even new staff can read the daisy and know the resident situation.
Will help to monitor and review care plans as needs of residents fluctuate. Will help staff to understand and support residents. The project was explained really well and the information is very helpful. All the team would benefit if training was developed so they could grasp the cognitive daisy.
Discussion
Being aware of the cognitive problems of care home residents is a major challenge for care workers yet pivotal to enhancing the delivery of person-centred care, reducing agitation and identifying effective forms of communication. All care staff who participated in this study rated the importance of understanding cognitive problems for the delivery of person-centred care very highly but admitted to finding these difficult to remember. They also endorsed the use of the COG-D as a visual representation of the cognitive status of each resident and believed that by making cognitive strengths and weaknesses apparent the COG-D could improve the quality of person-centred care.
The cognitive profiles of residents in this study were diverse. In fact, 88% of the COG-Ds created were unique within the cohort. Although all residents had profound deficits recalling recent information, on each of the other tests between 28% and 94% of residents were unimpaired. The degree of individual variation in cognitive ability is further highlighted by the distribution of white petals – which indicate no impairment. On each COG-D, the number of white petals ranged from 1 to 12. In this study, only four residents failed to complete a test, which suggests that the overall demand characteristics of the COG-D test battery are appropriate.
Recognising that a resident has a specific cognitive problem can prompt care staff to adopt a number of modifying strategies. For example, if a resident has difficulty with speech production, care staff can modify their own interaction by giving the resident more time to respond and keeping choices simple (Orange & Colton-Hudson, 1998). Alternatively, the residents’ behaviour might be modified by encouraging different means of communication (Hoffman, Platt, & Barry, 1988). For instance, 24 (73%) residents in this study have speech fluency difficulties (test 7), however, 11 of these are competent writers (test 8) and all know how to communicate through gesture (test 13). COG-D not only provides information on specific abilities but can also reveal details on the nature of impairment when the status of complimentary petals is considered. For example, 8 out of 10 residents who demonstrated deficits locating objects in the visual search task (test 12) could recognise individual objects perfectly well (test 10). The difficulty that these residents might experience is therefore not in object recognition per se (e.g. identifying a spoon) but is particular to situations in which many other objects are present (e.g. finding a spoon on a table with an array of crockery and cutlery). Therefore consideration of background factors (via the COG-D) in relation to situational factors can empower care staff with the potential to predict and therefore avert the risk of needs-driven dementia-compromised behaviour (Kolanowski, Litaker, & Buettner, 2005).
In addition to informing the decision making of individual care staff, COG-D can also benefit care home teams and managers involved in the shaping of care plans, organising activities and allocating resources. Incorporating the COG-D into care plans has a number of advantages. First, the COG-D is derived from objective measures of cognitive abilities that are covert and therefore not obvious to care staff. Second, the COG-D is readily interpretable without the need to read lengthy text or understand complex terminology. Third, new staff can readily derive an overview of the residents they will care for. Fourth, viewing COG-Ds constructed at different stages will present health professionals and relatives with a visual system for monitoring progression over time. It will enhance awareness in relatives about the relationship between cognitive decline and behaviour of residents and could serve as a basis to amend care needs appropriately.
The viewing of all COG-Ds from a care home in one place (e.g. on a wall or PC screen) will provide home managers with an overview of common cognitive strengths and weaknesses. This level of detail could be useful for identifying rehabilitative interventions that might be beneficial to numbers of residents and delivered on a group basis (e.g. speech therapy). Similarly, the identification of common strengths among residents will facilitate the formation of groups of residents that could benefit from participating in the same recreational activities.
It may also be viable for managers to create a ‘home’ COG-D that portrays the percentage of residents who are impaired in each cognitive function. This information would be valuable to care home providers with an interest in comparing the severity of cognitive impairment across homes within their organisation in order to guide decisions on resources and highlighting staff training needs.
It is noteworthy that training of the concept and deployment of COG-D markedly improved the knowledge of care staff of cognitive dysfunction in dementia. When asked to name specific cognitive problems associated with dementia in the pre-training phase, care staff stated more behavioural (e.g. wandering, agitation, undressing, aggression, etc.) and psychological problems (e.g. frustration, anxiety, depression, etc.) than cognitive deficits. Following the intervention, a significantly greater number of cognitive problems were named. Implementation of the COG-D appears therefore to have influenced care staff to give greater consideration to background cognitive factors (e.g. inhibitory control) which have the potential to lead to needs-driven dementia-compromised behaviours given the presence of proximal triggers.
This pilot investigation has provided unequivocal support for both the practicality and usefulness of the COG-D in residential care homes. The application of the COG-D is not exclusive to dementia. The cognitive profile of any neurological (e.g. brain injury, stroke, Parkinson’s disease, motor neurone disease, etc.) or developmental disorder (e.g. autistic spectrum disorders, attention deficit hyperactivity disorder, learning difficulties, etc.) might be usefully depicted by the COG-D following assessment with an appropriate test battery. Notwithstanding these strengths, we acknowledge that the COG-D is still at an early stage of development. Despite Cronbach’s alpha coefficient for the total COG-D test battery indicating a high degree of internal consistency, additional psychometric properties including the construct validity and test-retest reliability for the assessment battery await investigation. Furthermore, only a small proportion of residents and care staff at each home participated in this phase of the study and the pilot ran for only two weeks. To examine the generality of the findings reported here and to test the feasibility of the COG-D larger scale studies are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.