
Abstract
Objective
Peer support for people with dementia and carers is routinely advocated in national strategies and policy as a post-diagnostic intervention. However there is limited evidence to demonstrate the value these groups offer. This study looked at three dementia peer support groups in South London to evaluate what outcomes they produce and how much social value they create in relation to the cost of investment.
Methods
A Social Return on Investment (SROI) analysis was undertaken, which involves collecting data on the inputs, outputs and outcomes of an intervention, which are put into a formula, the end result being a SROI ratio showing how much social value is created per £1 of investment.
Results
Findings showed the three groups created social value ranging from £1.17 to £5.18 for every pound (£) of investment, dependent on the design and structure of the group. Key outcomes for people with dementia were mental stimulation and a reduction in loneliness and isolation. Carers reported a reduction in stress and burden of care. Volunteers cited an increased knowledge of dementia.
Conclusions
This study has shown that peer groups for people with dementia produce a social value greater than the cost of investment which provides encouraging evidence for those looking to commission, invest, set up or evaluate peer support groups for people with dementia and carers. Beyond the SROI ratio, this study has shown these groups create beneficial outcomes not only for the group members but also more widely for their carers and the group volunteers.
Keywords
Background
Dementia is a national priority, particularly in the area of diagnosis and effective post-diagnostic support. The increasing numbers of people with dementia present challenges to the health and social sectors in how best to support people following diagnosis. Peer support is routinely advocated in national strategies and policy, such as the National Dementia Strategy (Department of Health, 2009), the Care Act (2014) and National Institute of Clinical Excellence (NICE) quality indicators (2013), and is recognised as a worthwhile community intervention for people with dementia and their carers. Several studies (Clarke et al., 2013; Keyes et al., 2016; Mason, Clare, & Pistrang, 2005) show that peer support can reduce isolation and loneliness associated with dementia and provide information and support on how to manage the condition to live well. People with dementia and their carers routinely say that they draw significant benefit from being able to talk to other people with dementia and their carers and to share practical advice and emotional support, which is shown to improve their overall wellbeing.
Scarcity of public resources means that value-for-money for interventions for people with dementia requires closer scrutiny (Knapp, Lemmi, & Romeo, 2013). Studies suggest that peer support may lead to direct healthcare savings by equipping people with coping mechanisms and providing emotional support, which can lessen the risk of crises and subsequent, potentially avoidable and expensive interventions by the statutory sector (Arksey, 2003; Banerjee & Whittenberg, 2009; Clarke et al., 2013; Hall Long, Moriarty, Mittleman, & Foldes, 2014; Spijker et al., 2009). Traditionally, cost-effectiveness and cost-benefit analyses have been used to assess value-for-money of health and social care interventions. However, the value produced by participating in peer support groups can be subtle and is difficult to measure (Knapp et al., 2013). As such there is a scarcity of research on the wider social, economic or environmental value they create.
Study aim
The aim of this study was to use the ‘Social Return on Investment’ (SROI) methodology to quantify the social value created by peer support groups for people with dementia and their carers.
Methods
Group characteristics.
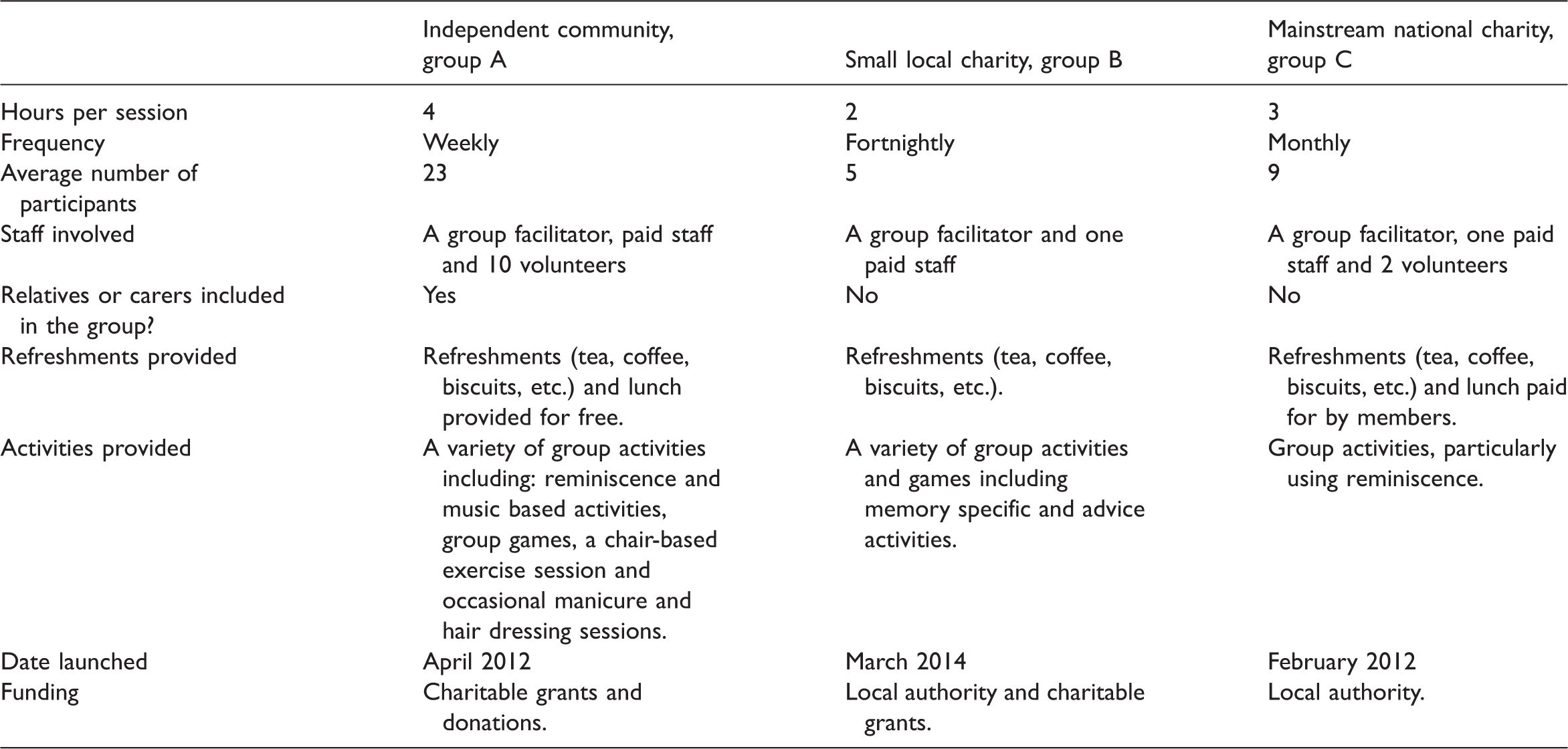
This study was a service evaluation and therefore did not require any ethical approval as deemed by the Kings College London ethics committee. Consent forms were obtained from participants prior to involvement.
SROI methodology
SROI has been previously described in detail in the literature (Millar & Hall, 2013). It is derived from better-known analytical methods such as cost-benefit analysis and social accounting and has become a recognised method of measuring impact, outcomes and value created by interventions or organisations. Briefly, through engaging stakeholders (people who it was thought would experience relevant and significant change from being involved with the group) SROI measures the value an intervention creates against the cost of enabling it to occur. It uses a concept of value that goes beyond what can be captured purely in financial terms by incorporating social, environmental and/or economic elements to calculate the total value, hereafter referred to as ‘social value’.
The authors closely followed established SROI methodology (Nicholls, Lawlor, Neitzert, & Goodspeed, 2009). The SROI method involves a mixed methods design. Qualitative methods are used to establish which outcomes (themes) were of most importance and impact on participant’s lives and ultimately combine to create social value, followed by a quantitative approach to create a monetary representation of these outcomes and their value.
Participant type and data collection method.
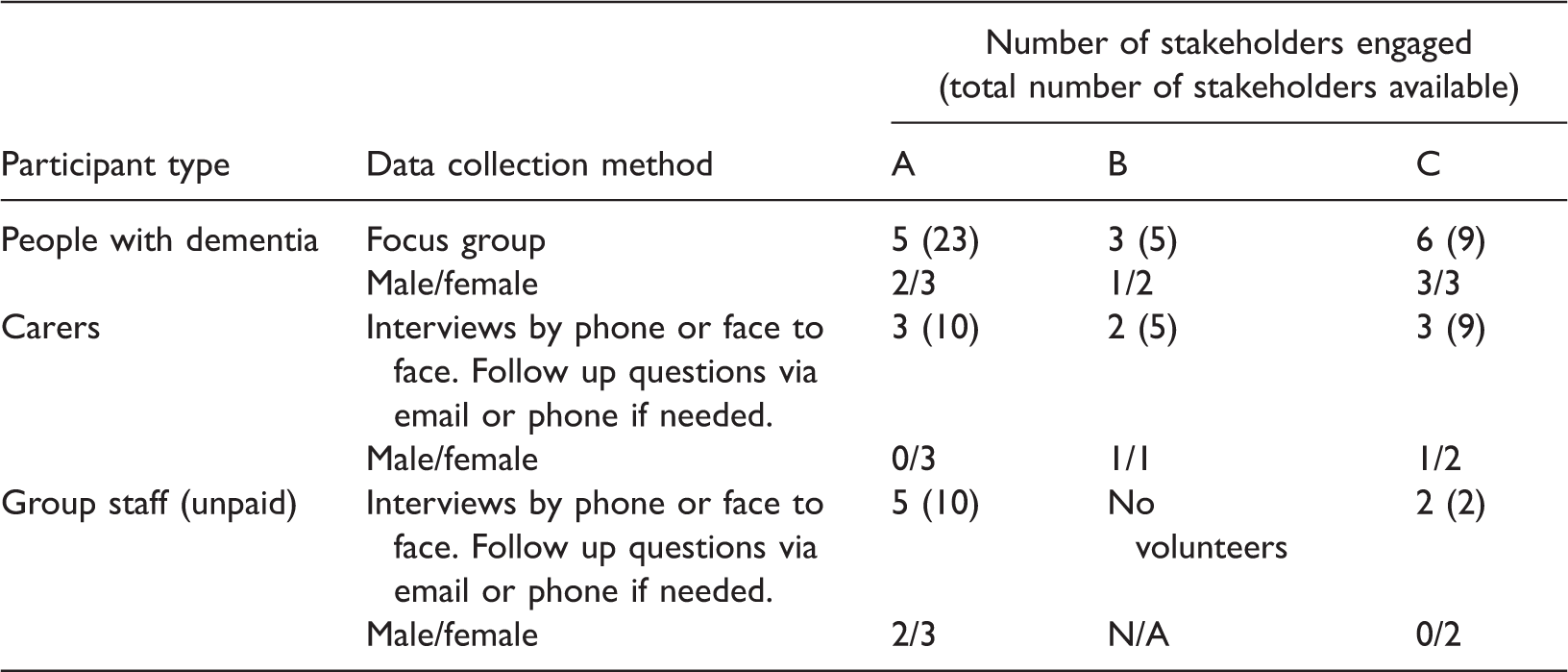
The expectation of sample sizes was modest given the stakeholder population sizes and it was acknowledged that some group members would not be able to be interviewed due to their level of cognitive impairment and that this would reduce the proportion of the member population that could potentially participate. Although a large sample size is not required for qualitative data collection, translation of the qualitative to quantitative data implies that larger sample sizes would have increased the validity of the outcomes for each stakeholder group.
With the help of the group facilitators participants were approached and invited to participate and despite small sample sizes it was felt a level of saturation was met with the themes reported. Group facilitators and volunteers were present at the focus groups for people with dementia to ensure a comfortable and familiar environment for participants. Sessions and interviews were recorded and transcribed verbatim. Transcripts were emailed to participants with email addresses to verify the transcriptions. Group facilitators verified focus group transcripts.
Thematic analysis akin to the ‘framework’ data analysis approach (Ritchie & Spencer, 1994) identified outcomes for each stakeholder through detecting the key themes in each transcript and charting the number of stakeholders who reported each theme.
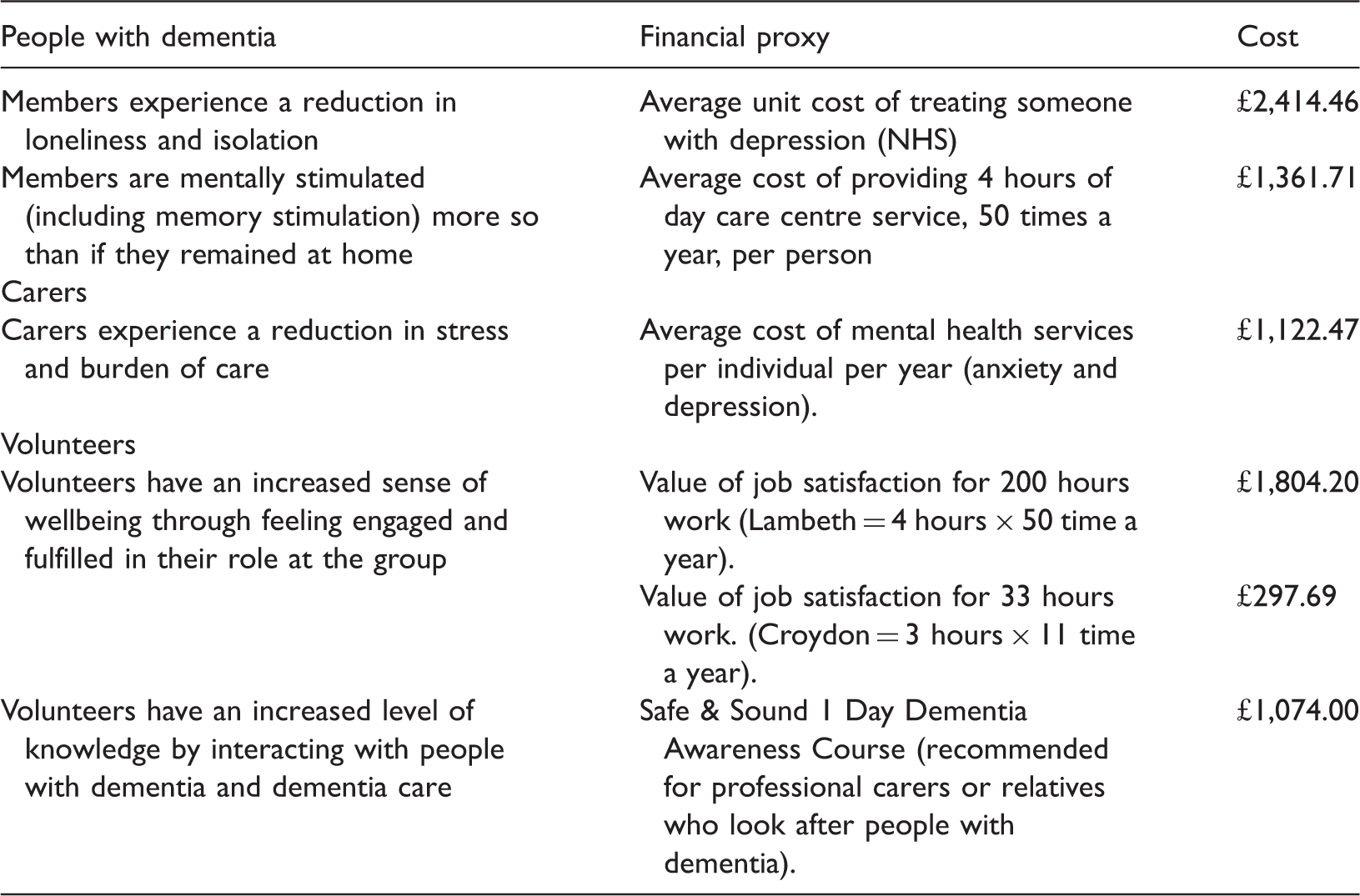
Financial proxy used to allocate a market price to identified theme.
Factors considered for calculating SROI impact ratio.

No previous published data to establish drop off rates therefore we allocated these rates based on knowledge of peer support groups and talking to group facilitators. These assumptions were validated by NEF Consulting.
The average used for the weighting factor was calculated based on frequency of groups delivered by a large charitable sector group provider. Groups run on average 2 hours once a month (a total of 24 hours a year).
In-kind contributions
The average UK wage (£14.80 per hour) was used to calculate the value of volunteers’ unpaid time with the exception of the accountant of group A, whose known hourly rate was £40 per hour (Office for National Statistics, 2011). The cost of free venue hire for each group was established by averaging the cost of renting out approximately 3–4 other similar venues in each borough.
Our approach
A separate SROI analysis was carried out on each group. By using the same researchers over the same time period, the approach to the method was the same and within this the same perspectives on discount factors, assumptions and financial proxies were used. This maximized the external validity of the three analyses and supported the comparisons then made between them.
The data methods, analysis and results were validated externally by NEF Consulting of the New Economics Foundation, which is the recognised expert organisation in the UK in using SROI analysis. Full results, calculations and impact maps for each peer support are available online (Health Innovation Network, 2015).
Results
Qualitative findings
Themes. a
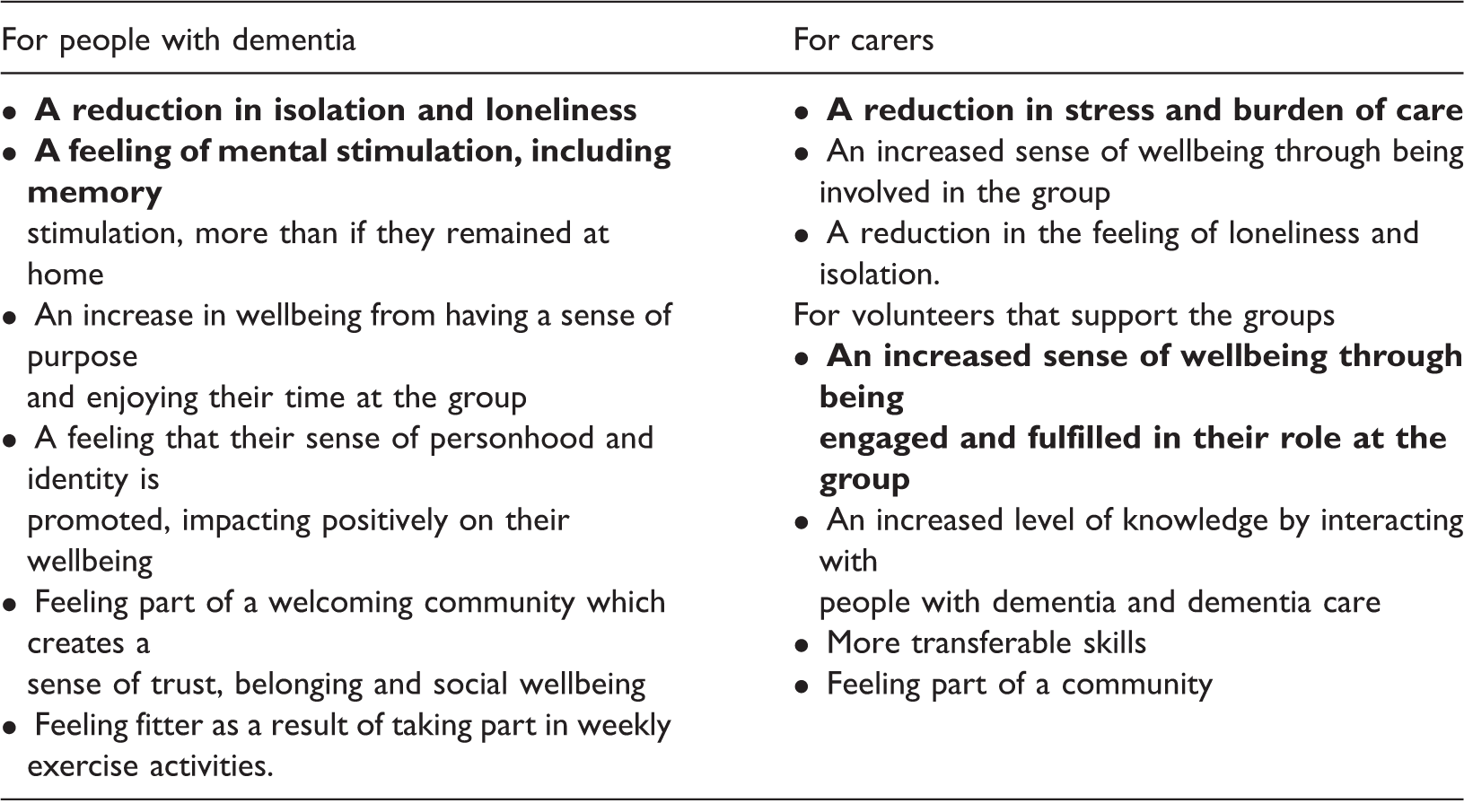
Themes in bold were evident across all three groups.
SROI analysis
Ratio by group.

Without the valued ‘cost’ of volunteers’ time or the venue hire, the ratios would have been much higher. For example, without the volunteer costs group A’s social value ratio would be £1: £12.99 and group C £1:1.40.
Discussion
This study has shown that peer support groups for people with dementia, regardless of size or structure, provided personal and social value to people with dementia, their carers and volunteers supporting the group, with a social value ranging from £1.17 to £5.18 for every pound (£) invested.
Common themes were identified across all three groups. A key finding across all groups is a reduction in isolation and loneliness, which is a common outcome seen in peer support generally and for people with dementia specifically (Clarke et al., 2013; Nesta & National Voices, 2015). Our findings show that peer support groups, or having the opportunity to meet others in a similar situation regularly can help people feel less lonely and less isolated and this experience is valued by people with dementia.
The carers of the group members reported observing that the members were mentally stimulated after attending the group, more so than if they had remained at home. Improving or maintaining cognitive stimulation is a recognised aim of some peer support interventions (Spagnolo et al., 2015; Woods, Aguirre, Spector, & Orrell, 2012) to maintain functional ability and quality of life. Studies have shown peer support for people with dementia has a beneficial impact in increasing wellbeing, self-esteem, quality of life and reducing depression (Banerjee et al., 2003; Leung, Orrell, & Orgeta, 2015), which may delay the need for more intensive support interventions or institutionalisation (Banerjee et al., 2003).
A reduced burden of care through improved coping skills and a reduction in stress has been associated with a reduction in carer depression and improvement in carer wellbeing in several studies (Black & Almeida, 2004; Brodaty, Green, & Koschera, 2003; McConaghy & Caltabiano, 2005). Our study supports these findings, with reduction in burden of care and stress a universal outcome across all groups, demonstrating the positive impact peer support groups have for carers. Findings from interviews with carers from groups B and C showed that these groups offered respite in terms of carers having some time for themselves and peace of mind that their relative is being stimulated and cared for in their absence, which reduced carer stress and the burden of care. Carers who attended group A also reported a sense of respite whilst participating in the group. Additionally, they reported enjoyment in sharing time together in a positive environment and meeting other carers with similar experiences, findings which are consistent with other studies (Greenwood, Habibi, Mackenzie, Dreenan, & Easton, 2013).
For both people with dementia and their carers, the overall sense of improved wellbeing and a reduction in negative risk factors to health such as loneliness, isolation and stress reinforces findings from previous studies (Banerjee et al., 2003; Clarke et al., 2013; Leung et al., 2015; Nesta & National Voices, 2015) that suggest peer support can reduce the risk of reaching a ‘crisis point’, with people either feeling more able to manage their situation or seek initial support and advice from peers or staff at the group before contacting the GP or emergency services.
Volunteers are not necessarily considered as beneficiaries of a peer support group, but the universal outcome, seen in Group A and C, of an increased sense of wellbeing amongst them is a noteworthy unintentional outcome of these groups. Also of interest is the fact that the volunteers reported an increase in understanding and knowledge of dementia. This outcome could be inadvertently recycled back into the group, potentially leading to improvements in the service being provided at no extra cost and positively influencing the social value produced over time.
All groups demonstrated a higher social value than the cost of investment. However, analysis of the largest group (A) indicates that a more intensive and frequently held group, involving volunteers and carers who also experience benefit, has a large impact on the overall social value produced by the group.
The two groups that had lower ratios show that smaller groups (in design or number of participants) still offer a gain in social value, relative to the cost of the service. People with dementia, like those without dementia, have a variety of preferences in terms of support and socialising and what is appealing to one person in terms of peer support will differ from the next. Our findings support the adoption of a mixed model approach to peer support, demonstrating that groups based on similar structure and design to those evaluated in this study are all a worthwhile investment. However, groups should consider ways to increase the value they create, relative to their investment. For instance, using volunteers as a free resource enables a higher number of people to be supported in the group and thus increases a group’s social value directly, as well as indirectly through the positive outcomes experienced by the volunteers. Identifying in-kind contributions such as free venue or activities was shown to increase a group’s social value. For example, group A used a communal room in an extra care housing home, with residents invited to participate as well.
Strengths and limitations
A strength of this study is the fact we evaluated three peer support groups of different designs and structures, using a mixed methods approach consistent with SROI methodology. Our methods and analysis were validated by NEF Consulting which is the expert organisation in SROI analysis. Limitations of the SROI process include the complexity of assigning financial proxies to soft themes, for example wellbeing and confidence and the availability of data to be used in robust calculations, for example displacement and attribution values. There is a risk in SROI analysis to focus solely on the ratio without examining the content behind it, which offers a richer insight to the value produced by groups (Nicholls et al., 2009).
Conclusion
The aim of this study was to understand and quantify the social value of peer support groups for people with dementia. A lack of robust economic evidence presents difficulties to commissioners or funders in investing in peer support as an intervention, as well as to groups to secure funding to set up and maintain their service. Findings from this study demonstrate peer support to be a worthwhile investment, both for people with dementia and their carers, but also for the volunteers who support the groups. It demonstrates that independent organisations and initiatives by smaller charities are able to produce a positive social return on investment, just as much or even more than groups run by large, more formal organisations. It provides guidance on how groups can increase their wider social value by using in-kind contributions such as volunteers and cost-free meeting space. We hope this study will aid decision making for those looking to commission, invest or set up peer support groups for people with dementia. Furthermore, we hope to have shown how to use SROI for similar community initiatives that are known to provide benefit but where a monetary value of the intervention is not yet known.
Footnotes
Acknowledgements
Thanks to the people with dementia, carers, volunteers and staff at the groups who participated in this study, Michael Weatherhead of NEF Consulting at the New Economics Foundation for validating our results, Dr AK Buttery, Innovation Fellow at the Health Innovation Network for reading and commentary on earlier drafts of this paper and Rebecca Jarvis, Programme Manager at the Health Innovation Network for suggesting SROI as a method to evaluate peer support groups.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project formed part of a wider project on peer support for people with dementia at the Health Innovation Network, the Academic Health Science Network for South London. NEF Consulting of the New Economics Foundation received payment from the Health Innovation Network to validate study methods, analysis and results.