
Abstract
In order to understand the words and deeds of dementia patients that we find very hard to explain or understand, we have paid attention to the self-awareness ability of dementia patients, the intellectual subject that integrates their own intellectual functions, and created ‘a model for interpreting puzzling words and deeds of dementia patients from the viewpoint of self-awareness’. The purpose of this study is to explain the reasons why dementia patients become unable to successfully perform activities of daily living (ADL) with advancement of dementia, using our model to present viewpoints understandable to caregivers. We classified dementia inpatients of a geriatric health services facility into four stages, using the model of self-awareness ability (consisting of ‘theory of mind’, ‘self-evaluation’ and ‘self-consciousness’) that was constructed by combining ‘theory of mind’ and Lewis’s developmental model of cognition and emotion. Furthermore, we observed and documented scenes from daily life, and we interpreted the reasons why patients become unable to seek assistance from others for ADL, based on the model. We came to understand why the patients could not seek assistance from others, because the patients who failed in the task of ‘theory of mind’ were unable to self-assess their own mind and the minds of others, and those having failed in the task of ‘self-evaluation’ could not evaluate their own situation.
Introduction
Approximately 2 million dementia patients live in Japan (Health and Welfare Statistic Association, 2008), but there are difficulties in caring for these people. Dementia patients account for nearly 80% of elderly abuse victims in a domestic setting (Institute for Health Economics and Policy, 2004). The major causes of abuse are triggered by behavior that puzzles caregivers, and an increase in the mental burden of caregivers due to an inability to communicate (Yosikawa, 2010). It has become an urgent issue to prevent abuse and to improve the quality of life (QOL) of dementia patients and their families. It can be said that caregivers’ understanding of the meaning of apparently puzzling words and deeds of dementia patients in daily life is a key to solving the issue.
Dementia is generally defined as a condition in which various cognitive functions, such as acquired memory, judgment, orientation, languages, and so on, have become impaired, causing varying degrees of inability to perform normal activities of daily living (ADL). Why do dementia patients turn out to be unable to perform normal ADL, once their cognitive functions have become disordered? It seems to be unreasonable to explain such constraint only through impairment of cognitive functions such as memory, judgment, and orientation. For instance, a patient, even if being able to recall his or her address and telephone number correctly, may lose his or her way in the streets to return home, but this cannot be explained only by impaired memory or orientation (Ozawa, 2002). This may be due to the impaired ability of the function of judgment. In the case of dementia, the impaired ability of judgment is said to be the inability to take an appropriate action suitable to an actual situation (Takeda, 2005), but the reasons for such failure have not been explained. In order for a dementia patient to become unable to get back home because he or she has got lost in the streets, it is necessary for him or her to have the self-awareness ability to recognize that they are indeed lost, the self-awareness ability to recognize the self-‘intention’ of wishing to return home and the self-awareness ability to recognize the self-‘desire’ to have someone contact their home for them. After all, dementia is not a mixture of impaired intellectual tools, such as impaired memory or orientation, but indicates a condition in which the intellectual core to coordinate these intellectual tools has been impaired (Ozawa, 2002), which will defy understanding of the whole picture of dementia, even if the intellectual functions are scrutinized piece by piece (Takenaka, 1996).
Accordingly, to understand the words and deeds of dementia patients that we find very hard to explain or understand, we have paid attention to the self-awareness ability of dementia patients, the intellectual subject that integrates their own intellectual functions, and created ‘a model for interpreting puzzling words and deeds of dementia patients from the viewpoint of self-awareness’ (Yokoi & Okamura, 2008).
Regarding the self-awareness ability (including ego, self-recognition, self-consciousness) of dementia patients, there are several published studies that explored anosognosia (Antoine, Antoine, Guermonprez, & Frigard, 2004; Banks & Weintraub, 2008; Barrett, Eslinger, Ballentine, & Heilman, 2005; Eslinger et al., 2005), the deficit of self-awareness accompanying frontotemporal dementia, Huntington disease, and Alzheimer disease (Derouesne et al., 1999; Snowden, Craufurd, Griffiths, & Neary, 1998; Sturm, Rosen, Allison, Miller, & Levenson, 2006), the relation between the deficit of self-awareness and performance of ADL or instrumental activities of daily living (IADL) (Cotrell & Wild, 1999; Cramer, Tuokko, Mateer, & Hultsch, 2004; Giovannetti, Libon, & Hart, 2002), the relation between cognitive function, such as memory, and the deficit of self-awareness (Gil et al. 2001; Ott et al., 1996; Vasterling, Seltzer, & Watrous, 1997). However, no published studies are currently available that have practically approached the analysis and the reasons of decline of living function from the point of self-awareness.
The purpose of this study is to explain the reasons why dementia patients become unable to successfully perform ADL with advancement of dementia, using our model to present viewpoints understandable to caregivers.
This model for interpreting puzzling words and deeds of dementia patients from the viewpoint of self-awareness consists of ‘a developmental model of cognition and emotion’ according to developmental psychologist Michael Lewis (Lewis, 1993; Lewis, Sullivan, Stanger, & Weiss, 1989) and the ‘theory of mind’ developed by psychologists Wimmer and Perner (1983) (Figure 1). According to Lewis, a human is born with emotions of ‘contentment’, ‘curiosity· interest’, and ‘distress’ and a baby in relation to others develops and differentiates emotions such as ‘joy’, ‘surprise’, ‘anger’, and the like. At around the age of 18 months, the baby begins to pay attention to the self, and the ‘self-consciousness’, differentiating the self from others, begins to sprout, developing the emotions of ‘Embarrassment’ and ‘Empathy’. And then from the age of two and a half to three, the infant starts to understand the rules and standards of the society in which the infant lives, while, by comparing him- or herself with these criteria, he or she obtains the function of ‘self- evaluation’ to judge whether the self-thinking, emotions, and actions are good or bad, thus developing the emotions of ‘Shame’ and ‘Guilt’. In addition, although it is usually assumed that the function of mind is as the background of other's behavior (Koyasu, 2000), Wimmer and Perner (1983) revealed that children can acquire the ‘theory of mind’, which is the ability to estimate psychological states (intention, thought, belief, desire, emotion, preference, etc.) that are in the background of the behavior of self and others and cannot be directly observed (Tager-Flusberg, Baron-Cohen, & Cohen, 1993), at between four and six years of age.
Interrelated development of cognition and emotion, and theory of mind (compiled from Lewis’s developmental model of cognition and emotion (Lewis, 1993; Lewis, Sullivan, Stanger, & Weiss, 1989), and Wimmer’s and Perner’s theory of mind (Wimmer and Perner, 1983)).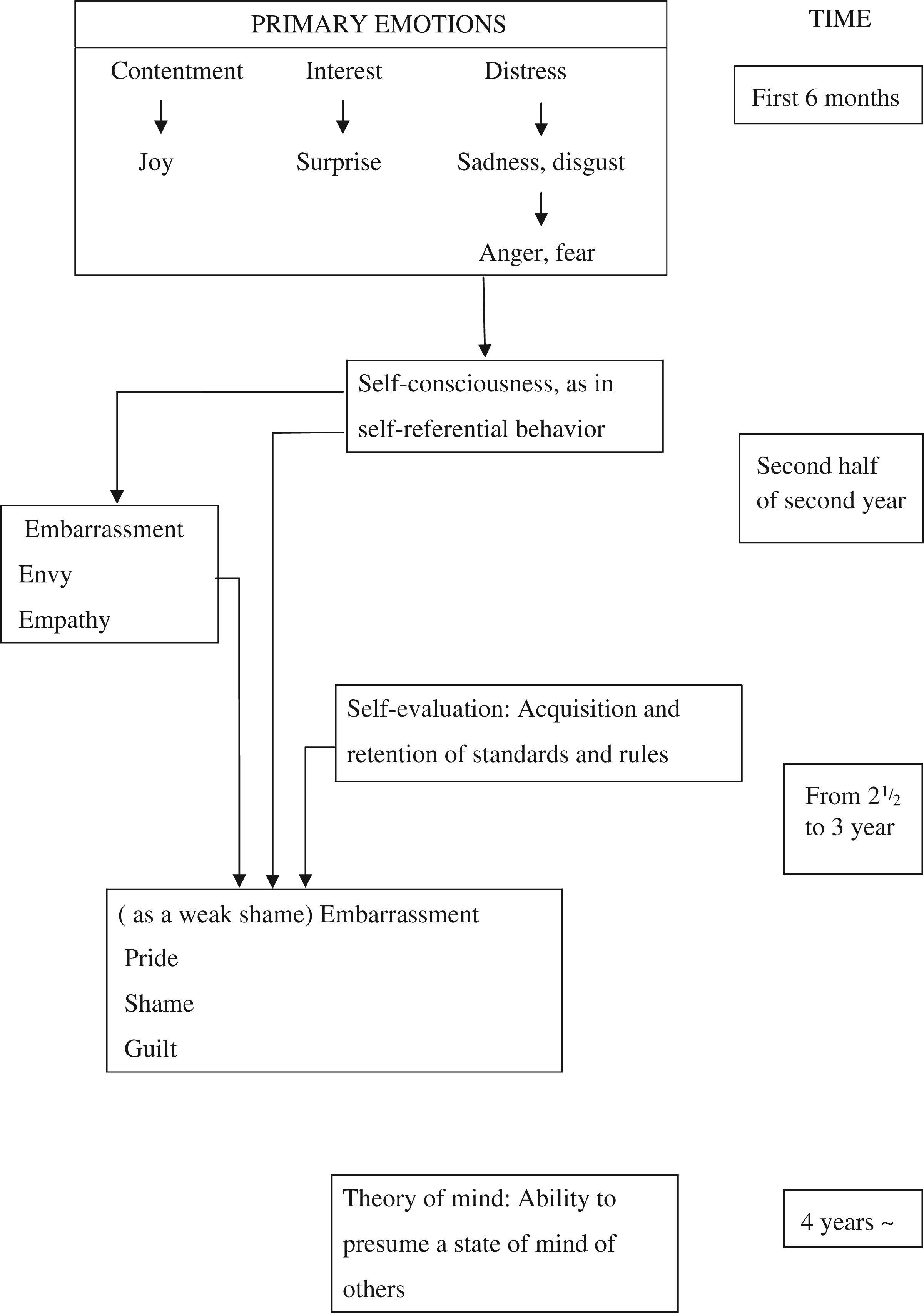
Self-awareness constitutes the basis of sociality (Kajita, 1989). In other words, it is suggested that the development of self-awareness forms the basis upon which infants adapt to the human relations, becoming conscious of their own existence at the awakening of ‘self-consciousness’ and distinguishing themselves from others, and further preparing for adapting to the social rules and standards in which they live, by making their ‘self-evaluation’, and becoming able to adapt to human relations with an unspecified large number of people, by presuming the other minds to be based on the ‘theory of mind’. Thus, the author has regarded the ‘self-consciousness’, the ‘self-evaluation’, and the ‘theory of mind’ in the present model as developmental stages of self-awareness for adapting to human relations.
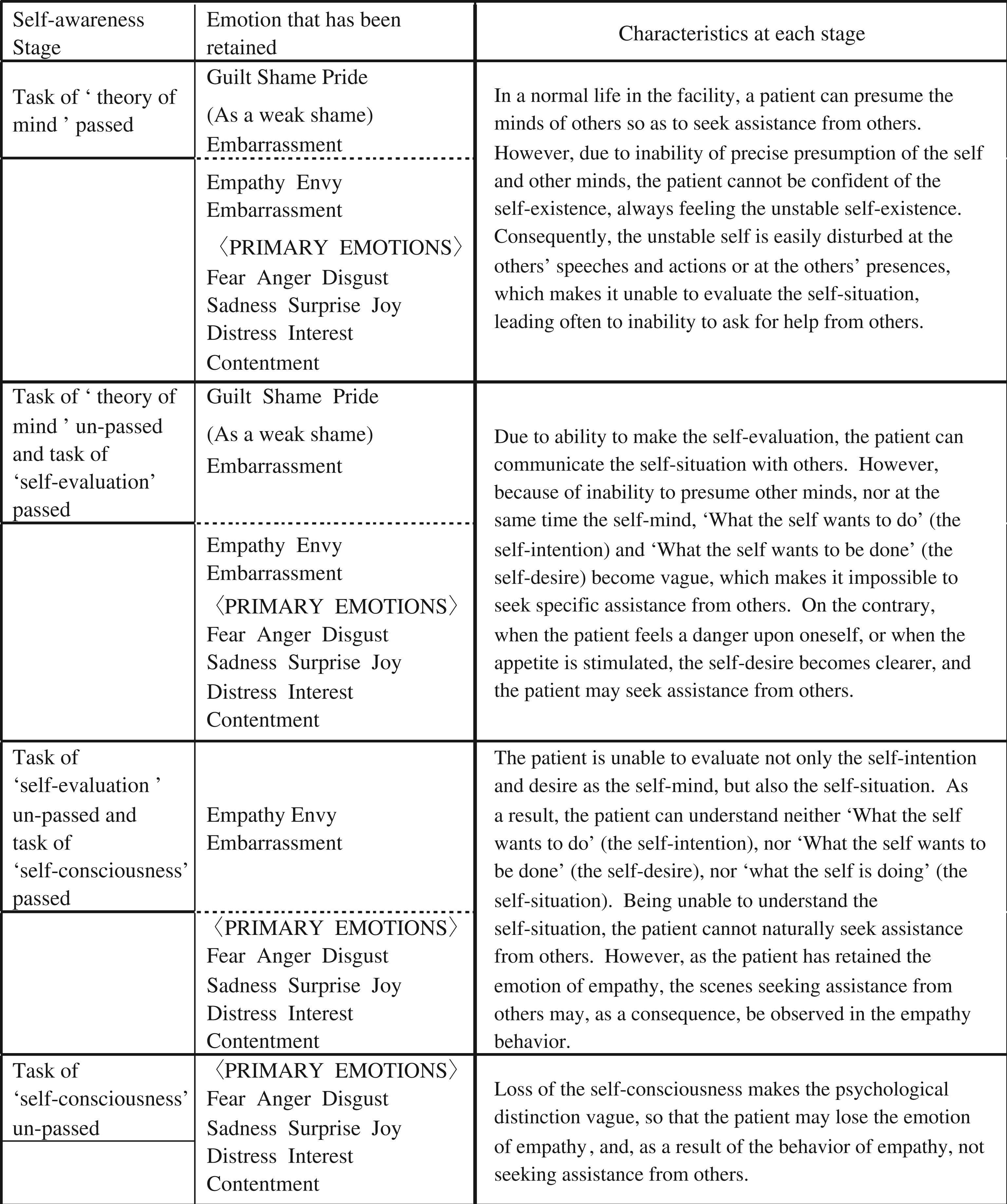
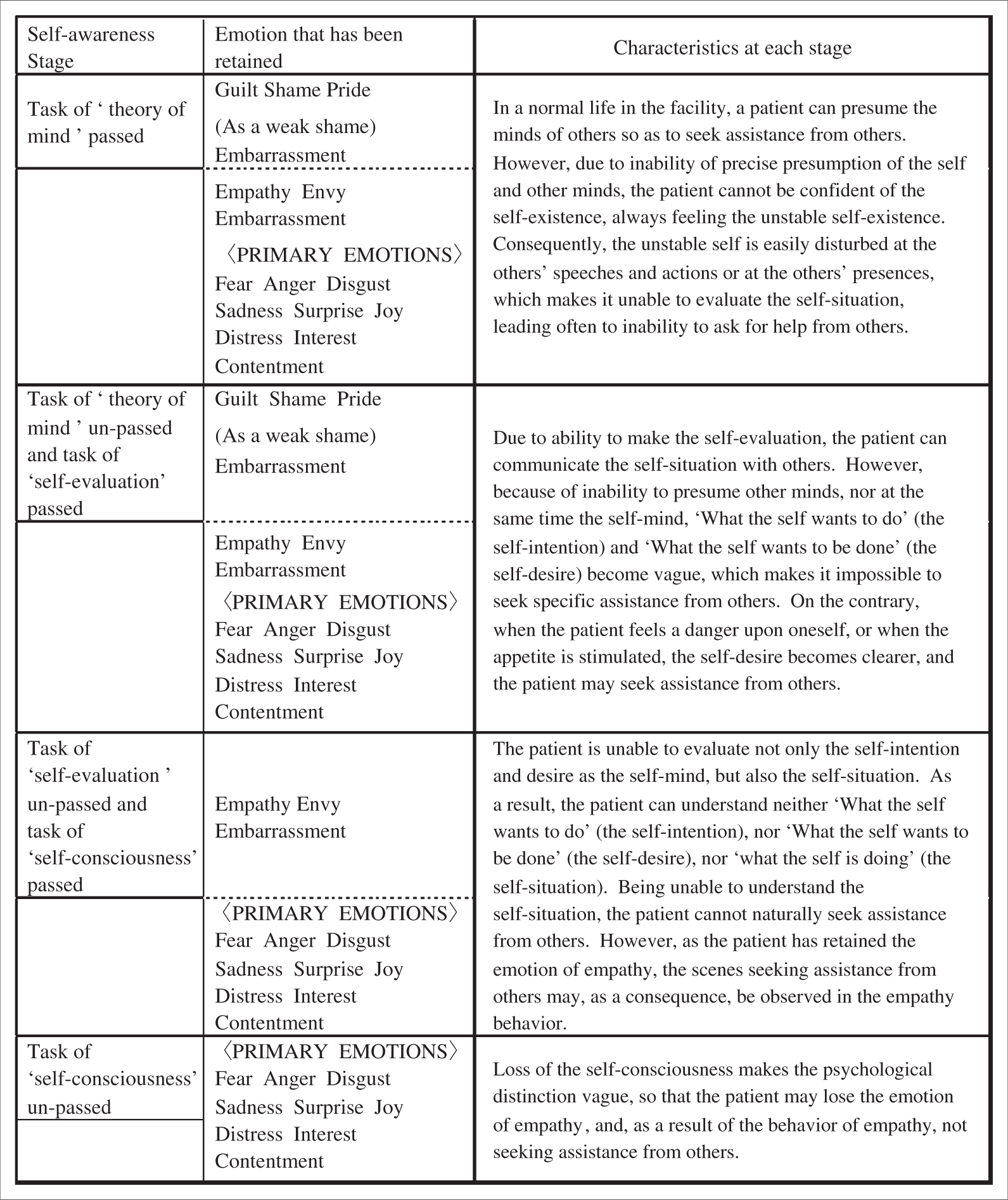
The ‘model for interpreting puzzling words and deeds of dementia patients from the viewpoint of self-awareness’ (Figure 2) views the above developmental model conversely. The loss of the function of ‘theory of mind’ (Tager-Flusberg et al., 1993), that is, the gradual inability to presume the psychological state (intention, thinking, belief, desire, emotion, preference, etc.) without the capability of direct observation (although it may be concealed in the background of the behavior of the self and others), will make it impossible to understand intention, thinking, belief, desire, and so on, of the self and others. The loss of the function of ‘self-evaluation’ will deprive the overall emotional gambit of ‘Shame’ and ‘Guilt’, making it impossible to evaluate the self-situation and to reduce resistance in taking actions that may be contrary to the social rules or standards. The functional loss of ‘self-consciousness’, that is, the psychological differentiation of the self from others, may lead to lose the emotion of ‘Embarrassment’, ‘Empathy’, etc., and as a result the behavior may be subject to only such primary emotions as ‘Contentment’, ‘Interest’, ‘Sadness’, or ‘Anger’.
A model for interpreting puzzling words and deeds of dementia patients from the viewpoint of self-awareness.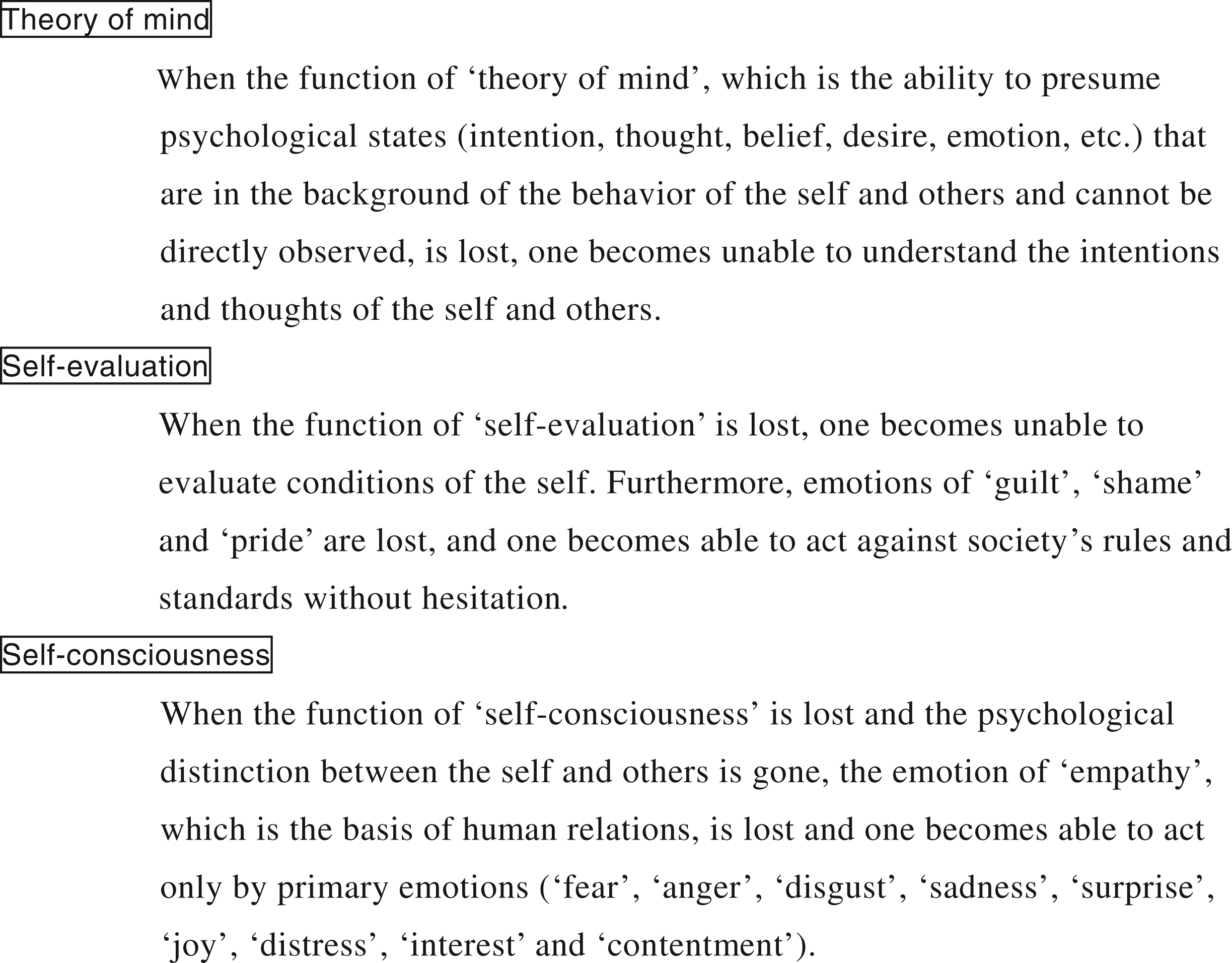
Methods
Subjects
The subjects were chosen from 44 patients who had been admitted to the designated ward for dementia in a geriatric health services facility, being diagnosed as having dementia by the diagnosis criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; American Psychiatric Association, 2000) (male 7, female 37, average age: 82.8 ± 8.1 years, Alzheimer disease: 22, Vascular dementia: 21, Pick’s disease: 1). Twenty-four patients (male 4, female 20) were finally selected whose families had been informed about the study purpose, and had consented to the study in writing. The average age was 83.4 ± 7.8, consisting of 11 patients with Alzheimer disease-related dementia, 12 with vascular dementia, and 1 with Pick’s disease. Taking into consideration the adaptation to a new environment, we excluded one patient who had stayed in the facility for less than 1 month and another two patients who were suspected of having mental illness as a complication other than dementia.
Evaluation of self-awareness ability
For evaluation of the self-awareness ability of ‘theory of mind’, ‘self-evaluation’, and ‘self-consciousness’, the author and the occupational therapist usually in charge of the subjects’ occupational therapy sessions made the evaluation with the subjects in a peaceful environment, taking into consideration the duration of attentiveness and the degree of any hearing disorder found in the subjects.
Evaluation methods of self-awareness ability in this model (Figure 2) are explained below.
Presence or absence of ‘theory of mind’
The author sat face to face to the subject across a table, showing much simplified adaptations of four picture cards that were originally in the version of Wimmer’s and Perner’s ‘Wrong Belief’ (1983) depicted by Muto (1995), and confirmed the presence or absence of the ‘theory of mind’ by pointing to the cards for each scene, while slowly reading out the description seen in Figure 3.
Four picture cards used to evaluate the presence and absence of the theory of mind. Scene 1. ‘There is a round box and a square box in front of Taro and Hanako. A bean-jam bun is contained in the round box.’ Scene 2. ‘Taro is leaving the room.’ Scene 3. ‘In the meantime, Hanako has transferred the bean-jam bun from the round box to the square box.’ Scene 4. ‘Taro has come back. In which box, the round box or the square box, does Taro think the bean-jam bun is?’.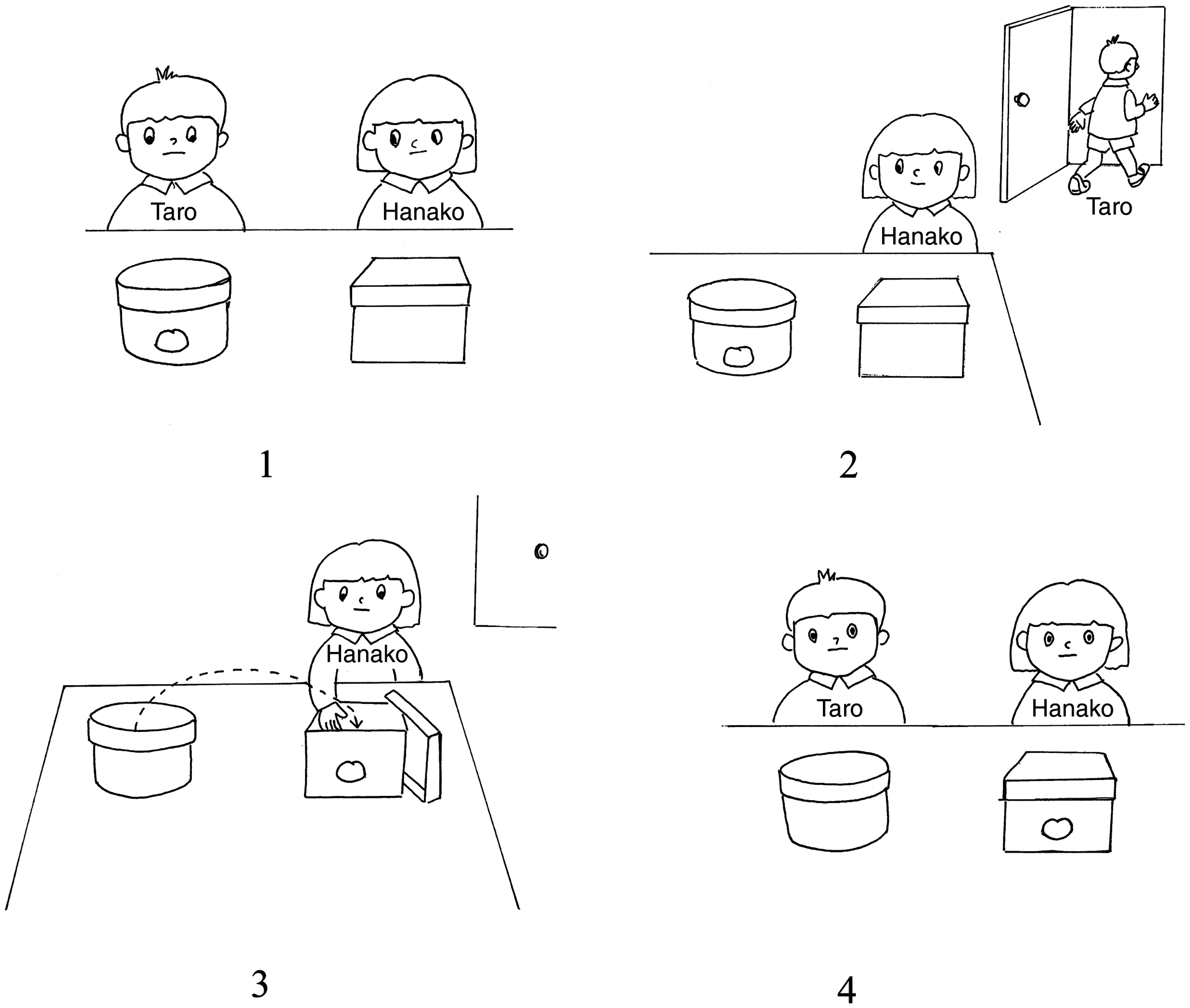
Presence and absence of ‘self-evaluation’
Lewis did not prepare a task to determine the presence or absence of ‘self-evaluation’. Consequently, the author devised and implemented four pairs of picture cards (Figure 4) to evaluate understanding of the fundamental rules and standards in Japanese society. First the author sat face to face with the test subject across a table, and confirmed that his or her attention was properly paid to the picture cards. Then, showing the cards pair by pair, the author read aloud slowly the narratives in the sequence given in Figure 4. In place of the ‘XXX’ seen in the captions, the subject’s name was used, and if the subject was a female, the author used the female version of the captions by changing the male characters into female ones. When the correct replies were given for all four tasks, the subject was regarded as being able to make a ‘self-evaluation’.
Four pairs of the picture cards used to evaluate the presence or absence of self- evaluation. Task 1. ‘Mr. XXX is washing his hands after use of the toilet.’ ‘Mr. XXX does not wash his hands after use of the toilet. Which is better?’ Task 2. ‘Mr. XXX is quarrelling with his friend.’ ‘Mr. XXX is getting on well with his friend. Which is better?’ Task 3. ‘Mr. XXX is wearing his clothes in public.’ ‘Mr. XXX has not put his clothes on, and is naked before everybody. Which is better?’ Task 4. ‘Mr. XXX is eating while standing.’ ‘Mr. XXX is eating while sitting. Which is better?’.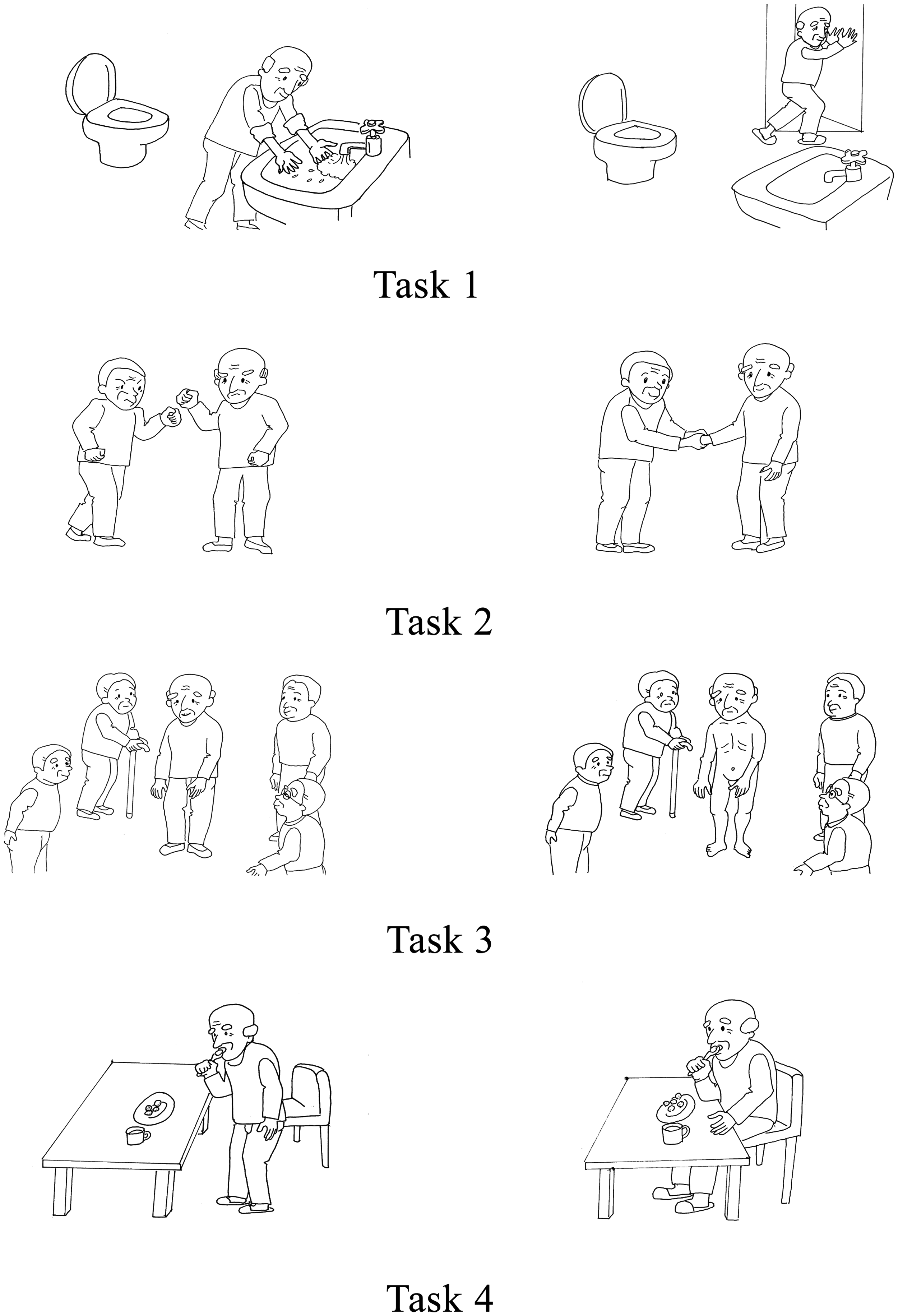
According to Lewis, the ‘self-evaluation’ ability develops from two and a half to three years old. In order to confirm if the above task was appropriate for the cognition ability in this age span, a child care worker in charge at a child care facility conducted a study in which the characters on the cards were changed into children. Twenty-eight children participated with the consent of their parents, with ages from 1 year 7 months to 3 years 11 months. The results confirmed that the age of 2 years 11 months in most of the children was appropriate for the development of ‘self-evaluation’.
Presence or absence of ‘self-consciousness’
Lewis et al. (1989) applied red lipstick on the tip of the nose of an infant without being noticed, and judged the presence or absence of his or her self-consciousness when the child touched the tip of his or her own nose when they saw their face in a mirror. However, a severe dementia patient does not have high interest as seen in the infant, nor is it possible to apply the lipstick technique due to impaired attentiveness.
Shoji (1989) reviewed all the preceding studies and suggested that the age at which an infant should be able to hearing their own name was from 18 months. As the age at which the above-mentioned lipstick task to evaluate the presence or absence of ‘self-consciousness’ used by Lewis was also from 18 months, the task of responding to one’s name is therefore considered to be an additional appropriate method for evaluation of ‘self-consciousness’. Thus, in accordance with the advice made by specialists studying ‘self-consciousness’, we adapted the previously reported method (Kajita, 1989) as follows. With the patient facing in any direction, either the patient’s name, both given and family names was spoken from behind the patient, or the name of another patient and a meaningless ‘ah…’ sound. The patient’s response, either turning round at the sound of their own name or not, was taken as constituting the core of recognition of the self or another stimulus, as well as a symbol representing the identity of each person.
Evaluation of ability to seek help from others
The author made a participation observation and documentation of the scenes where the subjects were asking for help from others, and where they did not seek help in those scenarios requiring help, by paying attention to the following.
Are the subjects who are embarrassed able to grasp their self-situations? From whom do they seek help?
Where do they seek help? At which point in time (when) do they seek help?
What kind of help do they seek?
How do they seek help?
The observations were made from 9:00 to 18:00 and from 13:00 to 18:00 twice weekly for 3 months, and each time the author wrote down in his pocket notebook the actual speeches and actions in the scenes in as much detail as possible. In addition, the author checked the records written by the respective subject’s caregivers and care nurses so as to extract such scenes as relating to the subject’s ability to seek help from others, the degree of reliability of these data being confirmed by the author from those who had recorded them.
Severity evaluation on general cognition function
The author and a caregiver made the evaluation with the Clinical Dementia Rating (CDR) (Hughes, Berg, & Danziger, 1982).
Analytical method
The author and the occupational therapist together classified the study subjects into four stages (the task of ‘theory of mind’ passed or failed; the task of ‘self-evaluation’ passed or failed; and the task of ‘self-consciousness’ passed or failed, which were divided by the presence and absence of ‘theory of mind’, ‘self-evaluation’, and ‘self-consciousness’). Then, for the scenario of the subject seeking help from others and that of a subject not seeking any required help from others, we interpreted why the subjects were unable to grasp their self-situations in embarrassment and why they were unable to seek help from others, by each of the four stages, based on the model of Figure 2.
Ethical consideration
For the present study we submitted the study protocol to the director of the study facility, and obtained the approval of the ethics review committee of the facility. As the study subjects manifested dementia, we informed their families in writing of the strict protection of the subjects’ privacy, and enrolled in the study only those subjects from whose families we received written consent to participate.
Results and discussion
To make it easy to understand the context of each stage, first we put together the characteristics that were seen through the cases in the scenes relating to the ability to seek help from others at each stage.
Then we showed the representative cases at each stage in the scenes relating to the ability to seek help from others. In our case reports, we have used the symbol < > for those scenarios where the subject sought help from others, and the symbol << >> for the scenario where help was not sought, although help was required.
On these scenes, based on the model of Figure 2, we interpreted on a stage-by-stage basis the reason why the subjects had become unable to grasp their self-situation that had caused them embarrassment, and why they had become unable to ask for help from others.
Six subjects who passed the task of ‘theory of mind’
Characteristic
In a normal life at the facility, we observed the scenes where the subjects grasped their self-situations and sought specific help from the staff. However, they did not precisely understand the minds of others, and were disturbed at the words or the presence of others, often making it impossible to seek help from others. [Case 1] A female in her 90s, Alzheimer disease, CDR: Mild (< >) One night, when an inmate with a severe degree of orientation disturbance came to her room, she exclaimed, ‘Help! Somebody!’ A staff member came quickly to the subject but the patient got angry, ‘What is wrong with this place? Why do you allow such a patient to hang around? This makes me feel much worse, although I have been already admitted in this hospital.’ The next day she barricaded the entrance door to her room with chairs. I asked, ‘What happened?’, and she explained, ‘At night someone had got into my room, hanging around. Someone is coming into this room, because there is a toilet in my room.’ [Case 2] A female in her 70s, Alzheimer disease, CDR: Mild The female inmate who often spoke meaninglessly, was sitting at the same table said, ‘I have toothache’, laying her face down on the table, and the subject sitting beside her explained to me, saying ‘When she visits a doctor, she has to pay the bill. She is worrying about it’, considering and assuming the other’s mind. On the other hand, (< >) the subject once put her handbag on the table, asking the unreliable inmate, ‘Will you watch over this?’, and returned to her room. Also, (<< >>) in the previous year the subject joined the Bon festival (a popular Japanese summer festival) dance of her own will, but this year, looking at so many strangers as inmate family members, she would not ask the staff member to let her join the dance, keeping the caregiver’s hand firmly held until the end of the dance. [Case 3] A male in his 80s, Alzheimer disease, CDR: Moderate The staff opened a coffee house twice weekly in a log hut adjacent to the facility. (<>) The subject forced me by hand to enter the coffee house again today. I explained that the coffee-house was not open today, but he was not persuaded, sitting down in front of the floor elevator of his ward, not trying to move. Also the subject was convinced that the inmate sitting on his right, who had said something the meaning of which was unclear, must have been begging for something, and shouted to the staff member who was sitting to his left, writing notes on the situation, ‘Don’t you feel sorry for her?’ Also one day, when I noticed that his front tooth was broken, I asked, ‘What happened?’, and the subject cooked up a story, saying, ‘My daughter took me for a ride in her car but she suddenly and unexpectedly braked very hard. That’s why my tooth is broken.’ [Case 4] A female in her 80s, Vascular dementia, CDR: Moderate (< >) When I was sitting slightly away from the subject, she called me to come to her, saying ‘Young man!’, and asked me to go and fetch a jacket, with a gesture that ‘it must be long enough’ (up to the wrist), as she claimed that the sleeves of a rather long undershirt are sticking out from the short-sleeved jacket. Also (< >) She said, ‘I cannot understand’ regarding the conversation from inmate, the meaning of which was unclear and she turned to me. ‘Listen carefully to his request’ she said, as I sat next to her. But (< >) she was once asked by a male inmate sitting at the same table to take care of the stuffed toy bear, Winnie-the-Pooh on the table. The subject became greatly upset and addressed a female inmate, whose understanding of spoken words was extremely poor, ‘Ma’am! What shall I do? I don’t know to whom this belongs. You are responsible for this! Take it away…’. She said this imploringly showing embarrassment. [Case 5] A female in her 80s, Alzheimer disease, CDR: Moderate (<< >>) On one occasion, an inmate who had no understanding of the spoken word was pounding on a table, quite near another female inmate. The female inmate shouted at the pounding inmate, ‘Why are you pounding? It’s noisy!’, without asking the staff member to caution the inmate. The staff member admonishingly explained about the situation to the female inmate who understood the problem, saying, ‘I did not know that’. [Case 6] A male in his 70s, Vascular dementia, CDR: Moderate This inmate was confined to a wheelchair, suffering from hemiplegia and a vision disorder. He was unable to stand up or maneuver his wheelchair. (< >) When his back was itchy, he called on staff members, asking them to scratch his back. On another occasion, when some other inmate tried to take his afternoon snack consisting of a bean jam-filled bun, he similarly called on the staff to stop this happening.
Discussion
For the subjects in this stage, when they asked for assistance from others, they first presumed the mind of the staff as shown in the phrase ‘I know well that I should not do this, but I cannot sleep’ (Case 1), and attracted the staff’s attention with such words as ‘Excuse me, excuse me’, ‘Young man’, and ‘Young lady’ (Cases 4–6). Afterwards the subjects asked for specific assistance, such as bringing them the cigarettes or their jacket, help with going to the toilet, back-scratching, and so on. In order to ask assistance from others, they have to be capable of making an accurate self-appraisal of their own situation, identifying such difficulties as going to sleep, going alone to fetch a jacket, going to the toilet, or requiring their back to be scratched, and it is essential to have an ability to assume knowledge of the other’s mind, such as the other’s intention, thought, or belief.
In normal daily life at the facility, even for the subjects that passed the task of ‘theory of mind’, enabling them to request assistance from others, it is impossible to assume precisely the mind of the others, as shown in the scenes in coping with the mind of the inmate with a severe orientation disorder (Case 1), the mind of other inmate family members at the Bon festival dance (Case 2), the mind of the inmate always saying something incomprehensible (Case 3), the mind of the male inmate asking for someone to look after his Winnie-the-Pooh (Case 4), the mind of the inmate pounding on the table with his fingers (Case 5), and so on. This is also well demonstrated in the use of a fiction or excuse that will easily reveal a lie to a listener (Case 3). Self-empathy is involved in assuming the mind-set of other people (Itakura, 2006). In the case of the inability to precisely understand the mind of others, it is safe to say that self-understanding of the subject’s own mind is at best faulty. The inability of a subject to precisely understand for themselves what is in/on their own mind indicates the inability to precisely assess self-intention and belief. With the inability of assessing self-intention or belief, it is impossible to have conviction regarding self-existence. This in turn makes the basis of the subject’s self-existence incessantly unstable, with the result that such an unstable self becomes susceptible to being easily disturbed by the words or presence of another. As a result of this, the entry of other inmates into a subject’s room disturbed her mind sufficiently to make her build up a barricade at the door; or the subject who was so as frightened by the minds of other inmate family members being strangers to her, that she was discouraged from participating in the Bon festival dance; or in the case of the subject who became disturbed at the mind of the inmate speaking nonsense, shouted at the staff member, or the subject who got embarrassed and confused at the inmate requesting disposal of the Winnie-the-Pooh, or the other subject who expressed her anger at the mind of the inmate pounding on the table. In short, due to the insufficient ability of a subject to assess their own mind-set, far less the mind-set of others, the subject’s mind at this stage becomes easily disturbed so that it becomes impossible for them to precisely evaluate the self-situation. Under this set of circumstances, the affected subject may thus become unable to seek suitable assistance from others.
Nine subjects who did not pass the task of ‘theory of mind’, but passed the task of ‘self-evaluation’
Characteristic
Scenarios were observed during which the subjects were capable of informing the staff of their self-situations, but scenarios in which the subjects sought specific assistance from the staff were scarcely seen, except when they felt threatened or in danger, or when their appetite was stimulated. [Case 7] A female in her 90s, Vascular dementia, CDR: Moderate (<< >>) This subject’s walking was unstable, but she often rose up from her seat and started to walk. I asked her, ‘What happened?’, and she replied, ‘I want to go to the washroom’, but she did not voluntarily ask to be taken there. Also (<< >>) she was found lying on her bedroom floor in the morning. She said that during the night she had fallen out of bed, ‘I tried to stand up, but fell down’, she said. She then said that she was sorry that she could not stand up, but she had not asked anybody to seek help to lift her up. [Case 8] A female in her 90s, Vascular dementia, CDR: Moderate During daytime this subject sat in a chair, often looking downward and drowsing. (<< >>) When she was subsequently made to visit the toilet, she looked into her diaper, found a stool, and was surprised at it, saying ‘Good Heavens!’ and in a sorrowful voice, repeated ‘Oh! My Goodness’. On the other hand, (< >) one early morning when she fell out of bed, she asked the staff to help her, saying, ‘Please help me’. [Case 9] A female in her 90s, Vascular dementia, CDR: Moderate (<< >>) When I went to see her once, she complained, ‘I feel giddy’. I laid her on a sofa, and she repeatedly complained, ‘I feel tightness and pressure in my chest’. I asked her, ‘Where?’, and she said, ‘Here’, placing her hand on her abdomen. When I said, ‘That’s your abdomen. I wonder if you are hungry’. Then she complained of her hunger, ‘I did not take breakfast or lunch. Please do something about it’. Usually she never sought any specific request asking for something to eat. On the other hand, (< >) when a country-style bean-jam bun was given to her during afternoon tea, she asked the staff member who was sitting beside her and supervising, ‘One more cup of tea, please’, holding the cup. [Case 10] A female in her 90s, Vascular dementia, CDR: Moderate (<< >>) This subject’s walking was unstable, and she often fell down. She occasionally stood up from a chair and started to walk holding onto a table. I asked, ‘What’s the matter?’, and she replied, ‘I’m going to the washroom: give me a car (she means her wheelchair)’, but she did not voluntarily call for the staff member to take her to the washroom. [Case 11] A female in her 80s, Alzheimer disease, CDR: Moderate (<< >>) The subject usually asked, ‘May I take this?’ when a meal was given to her, but did not ask for a rice bowl as a second helping. Even when her tea cup became empty, she did not ask for a refill saying ‘Please pour me some more tea’, unless someone else asked her, ‘Shall I pour the tea?’ However, (< >) one day at lunch when rice boiled with chestnuts was served, I sat beside her and observed that, after having eaten the first helping, she said, ‘Rice!’, holding the rice bowl up in her hand. [Case 12] A female in her 80s, Vascular dementia, CDR: Severe (<< >>) The subject was wandering slowly along, holding on the handrail and went into the guardroom, asking, ‘May I come in?’ After wandering around for some time, she approached a staff member who was talking with another inmate, and said, ‘I have a headache. I had better go to bed’. The staff member gave her black-sugar candy. While the subject was sucking it in her mouth, she remained sitting on a chair, saying, ‘I had better go back and sleep’. [Case 13] A female in her 80s, Alzheimer disease, CDR: Severe After fracturing her cervical femur, the subject underwent conservative treatment with observation, but felt pains persisting in her lower extremity. When the two staff members tried to assist her by lifting her onto the toilet seat, she refused, even before the transfer, saying, ‘No more help. Not for me’. But after she was transferred to the seat, she said, ‘What a pity!’ To the question, ‘Who?’, she expressionlessly replied, ‘It’s this wee-wee’. [Case 14] A female in her 80s, Vascular dementia, CDR: Severe This subject often went out from her room at night to the front of the lighted guardroom. (< >) On this particular day, she came out from her room as usual, trying to sit on the sofa in front of the guardroom, and asked the staff, ‘Can’t I? Can’t I?’ The staff replied, ‘No!’, and she seemed to give up sitting. The staff led her to a toilet, to change her incontinence-soiled clothes, and then took her into her room. She asked, ‘Do you take me here?’ The staff said, ‘Now go to bed’, and ‘Young lady, too’. Getting into the bed, she asked, ‘Is this O.K.?’ [Case 15] A female in her 70s, Dementia with Pick disease, CDR: Severe In a severe depressive condition, this subject hardly moved her body while sitting in a chair, and it was really seldom to observe the scenario where the subject talked to others. (< >) One night, a big cry, ‘Help! Somebody come quickly!’ was heard from her room. The staff hastened to the room, and found a roommate standing beside her bed, whereupon she exclaimed, ‘Please do something!’
Discussion
As the subjects at this stage are able to evaluate their self-situations, if not completely, they may be sometimes able to communicate their self-situations to others. In Case 7 the subject sat on the floor, but was unable to ask others to help her to her feet, and explained the situation by saying, ‘I tried to stand up, but fell down’, and, ‘I can’t stand up’. In Case 9, despite hunger, the subject was unable to ask for food, explaining her situation by saying, ‘I feel dizzy, have tightness in my chest, did not take breakfast or lunch’. In Case 10, despite the risk of fall, the subject did not ask for someone to help her get to the toilet, but stood up to start walking. When asked by the staff, ‘What’s the matter?’, she explained the situation, saying, ‘I’m going to the toilet’. In Case 13, despite pain, having been transferred to the toilet seat, the subject exclaimed, ‘What a pity!’. However, at this stage it is almost impossible for these subjects to ask for specific assistance. This may be attributed to the reasons that they are unable to assess what the minds of others are thinking, simultaneously with their own minds through which the self-intention and desire, namely ‘what the self wants to do and to be done’ become vague. In Case 12, the subject came into the guardroom with a vague idea of her ‘desire to do and to be done’, asking, ‘May I come in?’. In Case 14, her intention and desire became much weaker, and when she was led into her room, she asked, ‘Is this the way?’, ‘Is it O.K.?’.
However, in a dangerous situation or when one’s own life might be threatened (Cases 8, 15) or when the appetite is stimulated, the self-desire may become clearer, and the help of others is requested. When a life-threatening fear or physiological desire is strongly aroused, the learned and experienced intellect may appear.
Six subjects who did not pass the task of ‘self-evaluation’, but passed the task of ‘self-consciousness’
Characteristics
Among the six subjects, except for the two cases mentioned below, scenarios were not observed where the subjects sought the assistance of others. Even in the two exceptions, verbal expression became scarce, and scenarios where the staff’s assistance was asked for were rarely seen. Only in empathy behavior were scenarios observed where the help of others was requested. [Case 16] A female in her 70s, Alzheimer disease, CDR: Severe (<< >>) This subject was frightened by a nearby inmate talking loudly but not directed at her: she was standing, looking down. Usually she seldom actively talked to others, at best making appropriate responses to other’s talk, saying, ‘Ah! Is that so?’, but this time when I talked to her, she started to cry, looking down, while saying, ‘Everybody is speaking so proudly, but they are not supposed to do so’. Subsequently when I lightly patted her shoulder, she would not look back, stepped up to the tatami (straw mat) spread over the floor and sat upright on it. When stepping up onto the tatami mat, she took off her shoes and put them in order on the mat. [Case 17] A female in her 60s, Alzheimer disease, CDR: Severe Day and night this subject went out to wander, and hardly contacted others except for exchanging a few words. (< >) However, on one occasion she addressed herself in a half-sitting posture to her very old fellow inmate who was saying weakly, ‘I haven’t eaten anything’ in a depressive state. I was standing nearby, and shortly after she asked me for assistance, saying ‘Doctor! She is complaining of pains in her legs. I understand you are busy, but please’. Nevertheless, she did not intend to pull the author’s hand, and after having said, ‘I think you are busy, but…’, she returned to the inmate, saying tearfully, ‘A young man is coming soon for you. I, Granny, have a pain, too’. A few minutes later, however, she resumed her customary loitering around without even casting a look to this old woman.
Discussion
At this stage, the subjects are unable to evaluate not only the self-intention and desire as the self-mind, but also the self-situation. Consequently, they do not only understand ‘What they want to do’, and ‘What they want to be done’, but also ‘What they are doing’. As they cannot understand their own situation, they are naturally unable to seek other’s assistance. At this stage, the subjects scarcely expressed themselves. This may be attributed to not only to the consequences of atrophy of the brain, but also the result of a decrease in the necessity to communicate the self-intention, desire, or situations to others. This reduced requirement for communication may be attributed to a vicious circle causing loss of expressions in word and decrease of the opportunity to seek the assistance of others.
However, as the subjects who passed the task of ‘self-consciousness’ could retain empathetic behavior (Figure 2), it was sometimes observed that, among the empathetic behaviors, there were the scenes of seeking others’ help (Case 17). Also in Case 16, the expression of ‘Everybody is speaking proudly, and they are not supposed to speak in such a manner’ seemed to seek other’s help through the subject’s assessment of the minds of others; it should, however, be understood as a panic-stricken reaction to a shout made by some inmate not directed to her, and not as seeking assistance based on the belief of what a certain other person was thinking. After her insistence of, ‘They are not supposed to speak in such a manner’, the subject did not even look at me. Although the self is grasped from two aspects as the subject of consciousness and behavior (I), and as the object of the consciousness (me), it may be appropriate to understand her above words not as a request for assistance from the author being one of the others, but as the words of the self (I), who is a panic-stricken subject, empathizing the self (me), who is a crying object. It is presumed that this phenomenon occurred due to the vague differentiation between the self (I) as the subject and the self as the object (me), which were born together with a self-consciousness developing through relations with others during infancy.
Four subjects who did not pass the task of ‘self-consciousness’
Characteristics and discussion
For these final four subjects, no scenarios were observed where seeking another’s assistance occurred. The reason may be attributed to the psychological difference becoming unclear between the self and the others, and consequently leading to loss of the emotion of empathy and to suppressing the behavior of empathy on both the others and the self.
Conclusion
Summary of the reasons why dementia patients become unable to perform normal activities of daily living
With the advancement of the decrease of self-awareness ability, dementia patients become unable to understand ‘What the self wants to do’ (the self-intention) and ‘What the self wants to be done’ (the self-desire). Next they become unable to understand ‘What the self is doing’ (the self-situation). Finally being unable to make the psychological distinction between the self and others, they become unable to perform human relationships, and to carry out ADL as a result. In the case of the physically handicapped, even people with serious disorder can carry out ADL with seeking assistance from others. This is because they can establish human relationships by the psychological distinction between the self and others, and recognizing ‘What the self is doing’, ‘What the self wants to do’, and ‘What the self wants to be done’.
It can be said that human beings are able to live with adaptation to the complex field of human relations only after acquiring the function to distinguish between the self and others (‘self-consciousness’), the function to evaluate their thoughts and actions in comparison with the standards of the society in which they live (‘self-evaluation’) and, finally, the function to presume others’ minds (‘theory of mind’). In today’s primatology and theory of evolution, the evolution of ‘intellect’ is not caused by the fact that a human being makes tools; the Machiavellian intelligence hypothesis has become an established theory whereby it is purportedly necessary for a man to adapt to complicated human relations, such as cooperation or bargaining with other individuals within a group, and so on (Byrne & Whiten, 1997; Hasegawa, 2000; Humphrey, 1988). An approach from the direction of self-awareness ability, which is the adaptation ability to human relations, is considered to be an appropriate and powerful method (which also has evolutionary and primatological aspects) for dementia patients with declining ‘intelligence’ who become unable to successfully perform ADL.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
None declared.