
Abstract
Objective:
This study aims to determine whether genetic variants in ACE I/D and AGT M235T are associated with overweight-obesity and body mass index (BMI) in a Tunisian population.
Methods:
We designed an age- and sex-matched case-control study. The height and weight were measured and BMI was calculated. A total of 259 overweight-obese patients and 369 healthy controls were genotyped for the ACE I/D and AGT M235T genes using polymerase chain reaction and restriction fragment length polymorphism.
Results:
ACE I/D and AGT M235T genes were associated with BMI, waist circumference and overweight-obesity (p⩽0.001). In an additive model, the I and the M alleles in ACE and AGT variants, respectively, were associated with a lower BMI: –1.45 and −2.29 units, respectively. ACE I/D genotypes were associated with dyslipidemia; AGT M235T genotypes with dyslipidemia and total cholesterol.
Conclusion:
These data suggest that variations in ACE I/D and AGT M235T affect the risk of overweight-obesity, BMI and dyslipidemia, and could point to a key molecular pathway of metabolic syndrome and its related comorbidities.
Introduction
In recent years, obesity has become one of the major health challenges worldwide. 1 Recent data from the World Health Organization showed that obesity almost tripled between 1975 and 2016. 2 It is linked to multiple medical complications, affecting quality of life. 3 Obesity is a multifactorial disease resulting from complex interactions between genetic (interactions of several genes with each other) and environmental factors. 4
Polymorphisms in several obesity candidate genes have been the subject of intensive research as obesity is highly influenced by genetics, but a limited number of studies have investigated a possible link between obesity and the renin–angiotensin system (RAS).
The ACE gene, mapped on chromosome 17q23, is highly polymorphic in the promoter and coding regions, but because of the strong linkage disequilibrium in this region, the functional variant of this gene has not yet bee of the strong linkage disequilibrium in this region, the functional variant of this gene has not yet been determined. 5 The most studied ACE gene polymorphism, the 278-bp insertion (allele I) or deletion (allele D) variant in intron 16, is associated with plasma and cellular ACE levels. 6 The polymorphism results in two homozygous genotypes (DD with 190 bp and II with 490 bp) and one heterozygous genotype (ID with 490 bp as well as 190 bp). Cellular and plasma ACE levels are higher in homozygous DD than in homozygous II subjects, with intermediate levels among heterozygous ID subjects. 6 Unfortunately, data concerning the role of the I/D polymorphism in coronary artery disease risk in different populations are conflicting.7–10
The AGT gene, localized on chromosome 1q41-qter, encodes AGT. There is only one haplotype block at the AGT locus, and all common single nucleotide polymorphisms (SNPs) identified appear to be in complete linkage disequilibrium with the most intensively studied M235T polymorphism. 11 Although the functional variant has not yet been definitively identified, 12 the T235 allele has been consistently associated with cardiovascular disease.11,13,14
Recent genome-wide association studies have discovered several loci associated with obesity-related traits. 15 Most of these studies have been performed in European, Asian or Caucasian populations. However, information about the genetic background of obesity in North African populations is scanty.
Our main aim was to determine the effects of the angiotensin-converting enzyme insertion/deletion (ACE I/D) and the angiotensinogen (AGT M235T) gene polymorphisms on the risk of overweight-obesity and its associations with body mass index (BMI) in a Tunisian population.
Subjects and methods
Design and subjects
An age- and sex-matched case-control study was designed. Cases were individuals with overweight or obesity recruited from the department of endocrinology from Fattouma Bourguiba University Hospital (Monastir, Tunisia). All these patients were prospectively invited to participate in this study. Controls were normal-weight individuals, and were also prospectively selected and invited to participate among those attending a routine checkup as part of annual physical examination. Controls were living in the same geographic area as cases and without any history of hypertension or diabetes. Samples were collected during the period from January 2018 to April 2019.
Patients were individuals who had essential hypertension and were treated with selective antihypertensive medication (diuretics, beta blockers, calcium channel blockers) for about 3 years or more than that in monotherapy or combination therapy.
Anthropometric variables
Weight (kg), height (cm) and waist circumference (WC, cm) were determined according to a standard protocol in the Nutrition Center by trained nurses. BMI was calculated as weight (kg)/(height)(height)m2. Participants were categorized as normal body weight: 18.5–24.9 kg/m2, overweight BMI: 25–29.9 kg/m2 or obese BMI: >30 kg/m2 (National Heart, Lung, and Blood Institute in cooperation with the National Institute of Diabetes and Digestive and Kidney Diseases, 1998). 16
Sample collection and biochemical Markers
After an overnight fasting, from each of the recruited participants, 5 ml peripheral blood sample was withdrawn by venipuncture of the upper limbs and placed into tubes containing EDTA (for DNA extraction and lipid profiling).
Serum was separated for the analysis of total cholesterol (TC), high-density lipoprotein cholesterol (HDLC) and triglyceride (TG) analysis. Fasting blood glucose was measured at the time of blood collection. Biochemical analysis of TC, TG, HDLC was done using Randox kits (spectrophotometer). Low-density lipoprotein cholesterol was calculated using the Friedewald equation. 17
Genotyping
DNA was extracted from blood samples according to the Miller et al. 1988 protocol. 18 Allele-specific polymerase chain reaction (PCR) of ACE I/D polymorphism (specific primer sequences, forward oligo: 5′CTGGAGACCACTCCCATCCTTTCT3′ and reverse oligo: 5′GATGTGGCCATCACATTCGTCAGAT3′) was done following a standardized protocol. 19 DD homozygotes were re-amplified using specific primers (forward oligo: 5′TGGGACCACAGCGCCCGCCACTAC3′ and reverse oligo: 5′TCGCCAGCCCTCCCATGCCCATAA3′) in order to avoid misclassification of heterozygotes as homozygotes. 20 The AGT M235T genotype was determined by PCR amplification (specific primer sequences, forward oligo: 5′CAGGGTGCTGTCCACACTGGACCCC3′ and reverse oligo: 5′CCGTTTGTGCAGGGCCTGGCTCTC3′) followed by digestion with restriction enzyme Tth111I according to the described method. 21
Ethical considerations
This study was reviewed and approved by our hospital ethical committee. Participants were informed that participation is voluntary, and written consent was obtained from each participant after discussing the objective of the study and before being subjected to the questionnaire. No names were recorded on the questionnaires.
Statistical analysis
Hardy–Weinberg expectation for the genotypic distributions of SNPs was investigated with a Chi Square goodness of fit test with one degree of freedom.
Continuous variables are presented as mean (standard deviation) and categorical as frequency (percentage). We used ANOVA and Chi Square to compare continuous and categorical variables distribution between groups, respectively. Those variables associated with the genetic variants of interest and with BMI or overweight-obesity were considered as potential confounders. We used multivariate logistic regression analysis and multivariate linear regression analysis to evaluate the association between genetic variants and overweight-obesity and BMI, respectively. These multivariate models were adjusted for all the confounder variables. To correct for multiple comparisons we used the Bonferroni correction to establish the statistical significance threshold (p-value=0.05/3 genetic variants=0.017).
A multi-locus genetic risk score (GRS) was computed for each individual as the sum of the number of risk alleles across the variants that were associated with overweight-obesity or BMI.
The statistical analyses were carried out using SPSS 22.0 statistical software package for social sciences (SPSS, Chicago, IL, USA).
Results
The characteristics of the participants in this study are shown in Table 1. Finally, 259 overweight-obese and 302 normal-weight Tunisian subjects were included. The mean age of the participants was 48.88 ±14.69 years for patients and 48.27 ±13.70 years for the control group. The characteristics of the two groups were similar in terms of age, sex, smoking, diabetes and TG. Overweight-obese individuals presented with a higher proportion of hypertension, dyslipidemia, and with higher levels of TC, LDL and HDL cholesterol, BMI and WC.
Demographic and biochemical characteristics of the participants in the study stratified by the presence of overweight-obesity.

Mean (Standard Deviation).
HDL: high density lipoprotein; LDL: low density lipoprotein; BMI: body mass index.
Genotype distributions of all studied polymorphisms were compatible with Hardy–Weinberg expectation in cases and controls. The distribution of the AGT M235T and ACE I/D polymorphisms is shown in Table 2.
The distribution of the AGT M235T and ACE ID polymorphisms in cases and controls.
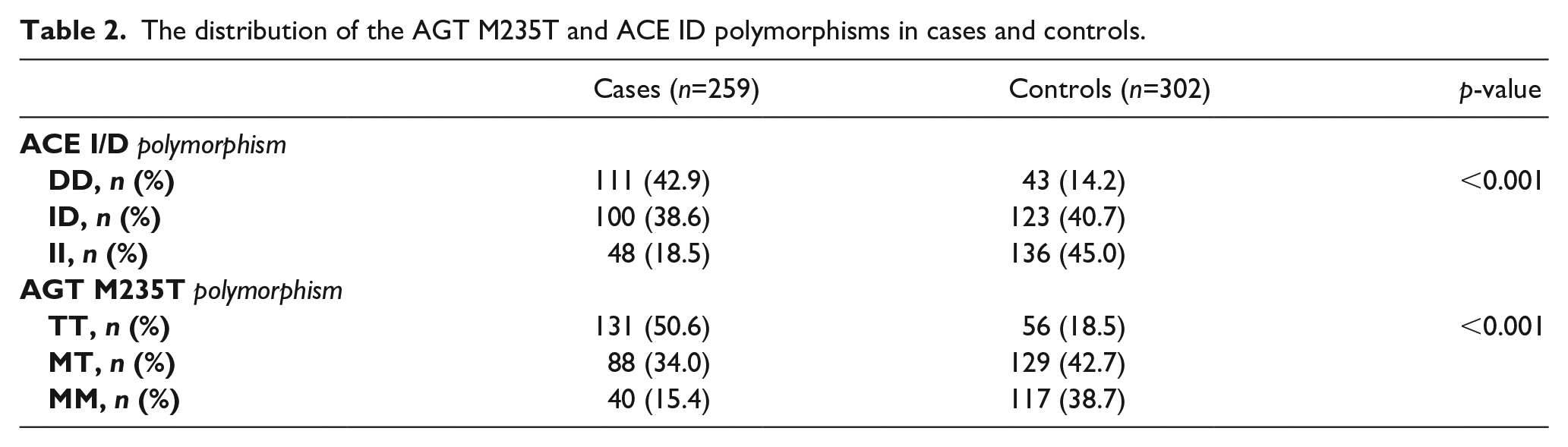
The frequencies of the polymorphic variants of AGT and ACE genes were significantly different between the 259 patients and the 302 controls included in the analyses, respectively (AGT, p<0.001 and ACE, p<0.001).
Furthermore, the frequencies of AGT and ACE genes were significantly different between overweight and obese patients, respectively (AGT MM/MT/TT, 11.7/35.9/52.4% vs. 18.5/32.5/49%, p=0.308 and ACE II/ID/DD, 16.5/36.9/46.6% vs. 20.4/39.5/40.1%, p=0.302).
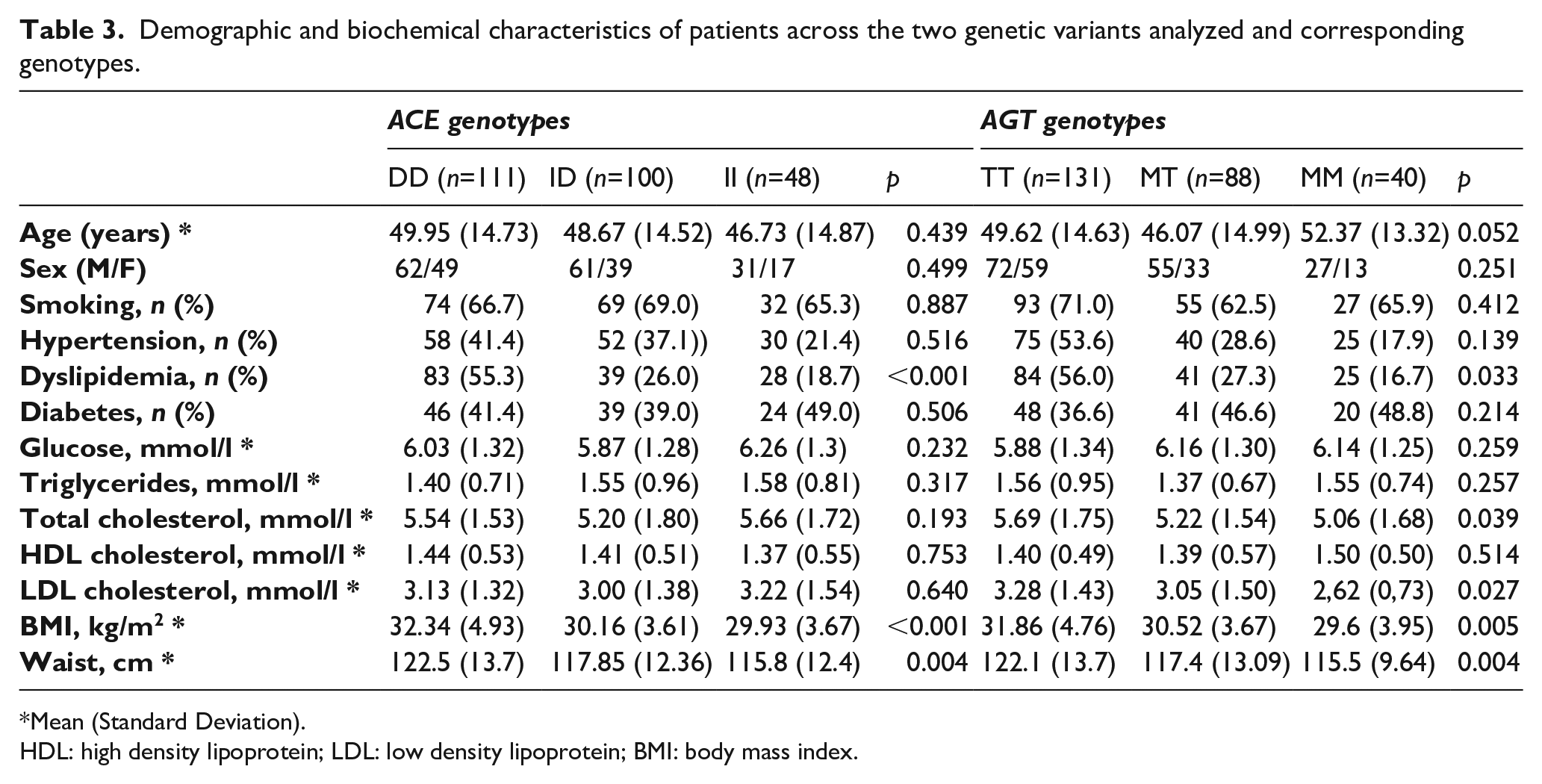
The characteristics of patients across genotypes are shown in Table 3. ACE and AGT genotypes were both associated with dyslipidemia, BMI, WC and overweight-obesity. AGT M235T genotype was associated with TC.
Demographic and biochemical characteristics of patients across the two genetic variants analyzed and corresponding genotypes.
Mean (Standard Deviation).
HDL: high density lipoprotein; LDL: low density lipoprotein; BMI: body mass index.
The DD genotype and TT genotype, for ACE and AGT respectively, were related to higher proportion of hypertension, smoking, diabetes and odds of being overweight-obese. No significant correlation was found between smoking and hypertension in patients (r=0.89; p=0.163).
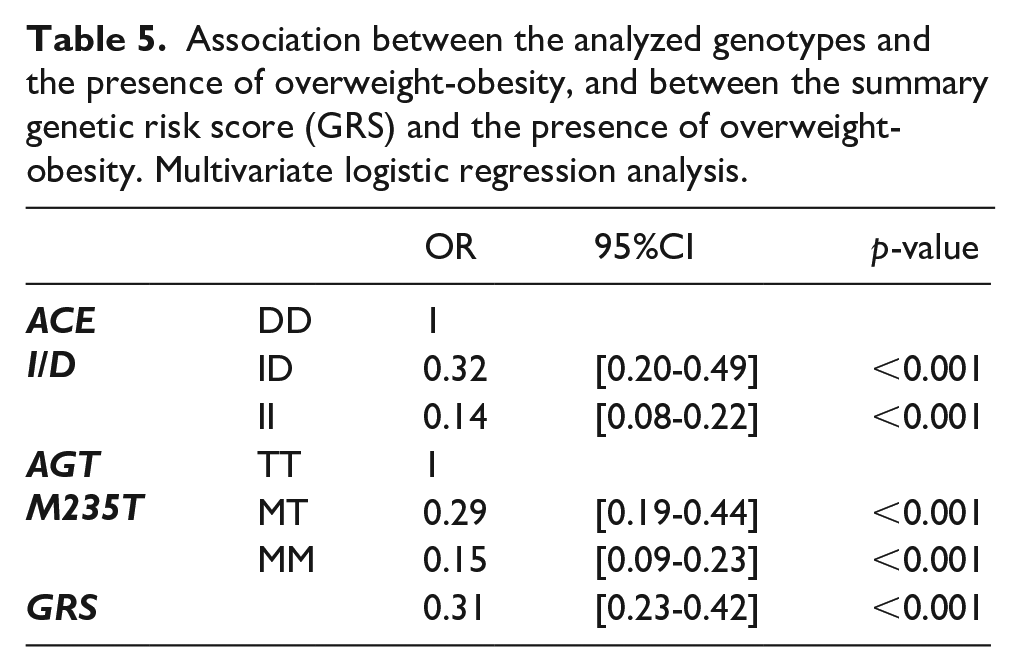
In Table 4, we present the univariate and multivariate effect size on BMI per each of the I and M alleles carried by an individual across genetic variants and in the multi-locus GRS. The results of the multivariate logistic regression analyses are shown in Table 5. The presence of the I and M alleles was also associated with lower odds of being overweight-obese.
Univariate and multivariate linear regression analysis between the analyzed genotypes and BMI, and between the summary genetic risk score (GRS) and BMI.
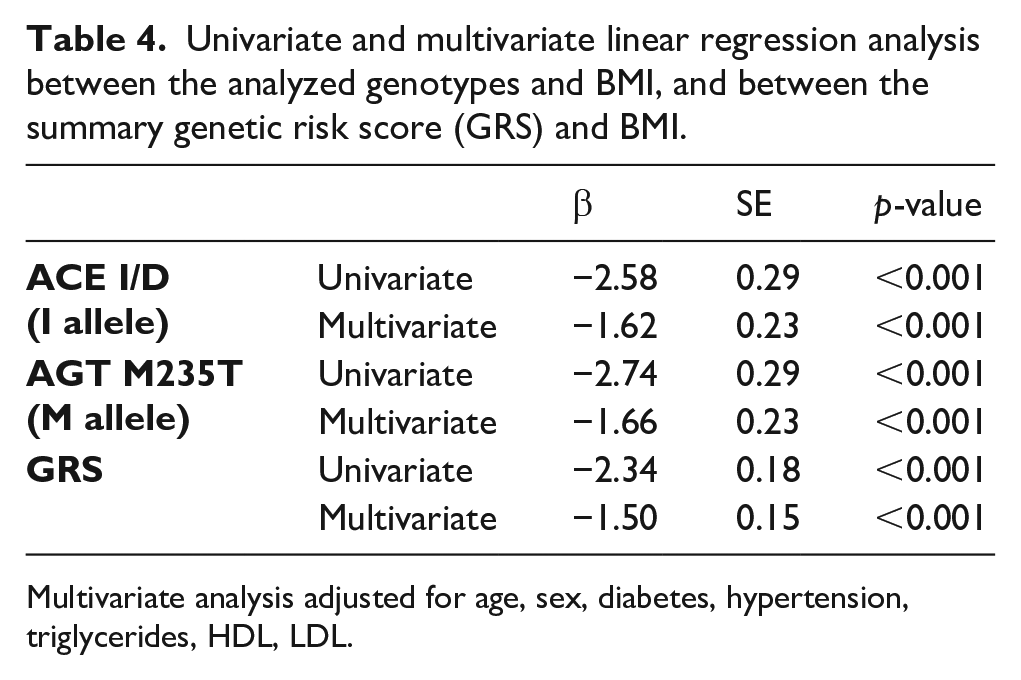
Multivariate analysis adjusted for age, sex, diabetes, hypertension, triglycerides, HDL, LDL.
Association between the analyzed genotypes and the presence of overweight-obesity, and between the summary genetic risk score (GRS) and the presence of overweight-obesity. Multivariate logistic regression analysis.
Discussion
A number of important research papers have extensively searched the link of ACE I/D and AGT M235T with several diseases, mainly hypertension22,10 and diabetes,23–25 often with highly inconsistent findings throughout various ethnic populations worldwide; associations with overweight and obesity, an important risk factor for cardiovascular diseases, have also been reported.9,26,27 In this context, ACE I/D and AGT M235T polymorphisms association studies in the Tunisian population are very limited, with reports linking them to obesity. 28
In the current study on this North African population, we report an association between ACE I/D and AGT M235T genes, and BMI and overweight-obesity.
Several studies have investigated the association between ACE I/D and AGT M235T and overweight-obesity in Asian,26,29–31 Caucasian32,33 and African populations.27,28 Our results are in part consistent with these previous findings, and confirm the relevance of these loci in overweight-obesity also in a North African population.
A number of investigations in this sense have generated mixed results. A study performed by Akin et al. evaluated the ACE polymorphism’s association among obese patients with insulin resistance (IR) and reported that the DD genotype was significantly higher in IR obese individuals than those without IR. 29 Mehri et al. reported an association of BMI with ACE gene polymorphism. 28 These findings were consistent with those found by El-Hazmi and Warsy, who reported an increased DD genotype frequency in overweight and obese Saudi individuals. 26 Mao et al. in the same way found a significant association was observed between DD genotype and overweight/obesity risk in overall populations (Africans, Caucasians and Asians, together) and Africans. 9 Although some studies have reported significant association between ACE polymorphism and obesity, others have found no associations. For instance, Pan et al. found no close relationship between ACE and obesity. 34 Motawi et al. published similar findings in a study of Egyptian women in which ACE polymorphism was not associated with obesity. 35 Rizvi et al. showed that ACE gene polymorphisms were not associated with BMI. 36 Similar, Pacholczyk et al. reported no significant associations between ACE gene polymorphisms and extreme obesity. 37 Moreover, Lelis et al. found no associations between BMI and WC (overweight/obesity) and ACE. 27
Data from literature regarding AGT polymorphisms association with obesity were scanty. We have investigated AGT polymorphism’s influence on overweight and obesity. In our study, a significant association between AGT genotypes and BMI, WC and the odds of being overweight-obese was observed, confirming previous findings. 31 Giacchetti et al. reported a correlation between AGT expression in adipose tissue of obese patients and BMI in visceral adipose tissue. 38 Similarly, Umemura et al. published a close relationship of increased plasma AGT levels with BMI and blood pressure in obese individuals. 39 However, Lelis et al. were not able to find association between BMI and WC and AGT. 27 Moreover, Prat-Larquemin et al. reported no association between the AGT variants and fat mass. 40
The present study has to be interpreted within the context of its limitations. Herein, only the association between the genetic polymorphisms of ACE and AGT with overweight-obesity was studied and we did not address the functionality of the variants. There are no measurements of markers of RAS activation available to correlate directly with the genetic polymorphisms investigated here. Among the limitations we have also to mention the limited number of SNPs analyzed in this study. In addition, the sample size of our study population is modest, hampering our statistical power. Therefore, extending the investigation of the studied associations on a larger sample set is warranted to confirm that the present findings would replicate in other groups. However, we did observe and replicate some associations previously reported in other ethnic groups.
Conclusion
In conclusion, this preliminary case-control study indicates that angiotensin-converting enzyme insertion/deletion and angiotensinogen polymorphisms were significantly associated with overweight-obesity, BMI and dyslipidemia in this sample of the Tunisian population.
Further confirmatory studies with a larger sample number would be necessary to support or contradict our results. Moreover, biological investigation including measurement of ACE and AGT levels and activity could be beneficial to understand the influences of these genes on the development of this cluster of events.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Ministry of Higher Education, Scientific Research and Information and Communication Technologies, Tunisia.