
Abstract
Objective:
Increased circulating level of plasminogen activator inhibitor-1 (PAI-1) is associated with menopausal oestrogen deficiency. We therefore hypothesised that the combined oral contraceptive (COC) with spironolactone (SPL) improves insulin resistance (IR) in ovariectomised (OVX) rats by reducing circulating PAI-1.
Methods:
Twelve-week-old female Wistar rats were divided into sham-operated (SHM), OVX, OVX+SPL (0.25 mg/kg), COC (1.0 µg ethinylestradiol and 5.0 µg levonorgestrel) and OVX+COC+SPL rats treated with COC and SPL daily for eight weeks. IR was assessed by homeostatic model assessment of IR (HOMA-IR).
Results:
Data showed that OVX rats had a higher HOMA-IR value that is associated with increased visceral adiposity, triglycerides (TG), total cholesterol/high-density lipoprotein cholesterol (HDL-C), TG/HDL-C, plasma insulin, GSK-3, corticosterone and decreased 17β-oestradiol. However, these effects were attenuated in OVX+COC, OVX+SPL and OVX+COC+SPL rats compared to OVX rats. OVX rats had lower PAI-1 than SHM rats, whereas the beneficial effect on IR and other parameters by COC or SPL was accompanied with increased PAI-1. Improvement of IR and other parameters with combined COC and SPL in OVX rats was accompanied with reduced PAI-1.
Conclusion:
Taken together, COC or SPL improves IR independent of PAI-1, whereas a combination of COC and SPL in OVX rats ameliorates IR in a PAI-1-dependent manner.
Keywords
Introduction
The incidence of cardiovascular disease (CVD) among women is low before menopause and steadily increases after the onset of menopause or experimental ovariectomy. 1 Loss of ovarian function induced by menopause or ovariectomy is associated with cardiometabolic pathologies such as insulin resistance (IR), type 2 diabetes, chronic inflammation and atherosclerotic CVD.2,3
Plasminogen activator inhibitor-1 (PAI-1), a serine protease inhibitor, controls the fibrinolytic system by inhibiting tissue-type and urokinase plasminogen activators. 4 PAI-1 is also implicated in physiological and pathological conditions such as inflammation, thrombosis, vascular remodelling and wound healing through control of plasminogen cascade. 5 A link exists between oestrogen concentrations and PAI-1 in women. Menopausal oestrogen withdrawal is associated with increased circulating levels of PAI-1, while a decrease is found with hormonal therapy.6,7 These changes have been interpreted as potential reasons for the beneficial vascular effects of endogenous oestrogen in fertile women. 8 In addition, a link between PAI-1 and hormonal status has been identified in CVD in humans and animals.9,10
IR is a common metabolic link for a cluster of abnormalities such as hyperinsulinaemia, hypertriglyceridaemia and obesity which all contribute to CVD. 11 One of the possible mechanisms explaining the relationship between IR and CVD is an increase in plasma PAI-1. 12 The ability of PAI-1 to predict such sequelae disappear after adjustments for IR biomarkers, 13 the mechanism of which remains unclear.
Glycogen synthase kinase-3 (GSK-3) is a serine/threonine kinase, which phosphorylates and inactivates glycogen synthase. Numerous evidences support a role of elevated GSK-3 as a contributing factor in various pathophysiological states such as IR, obesity, diabetes, glucose intolerance and dyslipidaemia.14,15 Studies have suggested a role for glucocorticoids including corticosterone in the development of CVD as well to cause IR. 16
Spironolactone (SPL) is a non-selective mineralocorticoid receptor (MR) antagonist and has been in wide clinical use for several decades because of its potency over a newer and more selective MR antagonist, eplerenone. 17 Oral contraception remains one of the most effective reversible contraceptive methods commonly used worldwide by more than 100 million women. 18 Although the adverse contribution of combined oral contraceptives (COC) to the pathogenesis of cardiometabolic disorders remains unresolved,19,20 it has been shown to ameliorate conditions such as dysmenorrhea, fibroid-related symptoms, acne, premenstrual dysphoric disorder 21 and maternal mortality. 22 Although the use of a MR antagonist such as SPL during COC therapy may be controversial in certain conditions, 23 the clinical relevance of SPL cannot be overemphasised. 24
It has been shown that oestrogen depletion through ovariectomy has deleterious cardiometabolic effects, 3 and the beneficial effect of oestrogen therapy in such conditions has been conflicting. 25 Moreover, SPL use has been shown to be beneficial. 17 Hence, it will be interesting to know the effect of SPL use during hormonal therapy with COC in ovariectomised (OVX) rats. We therefore hypothesised that COC and/or SPL would improve IR in OVX rats through a reduction in circulating PAI-1.
Methods
Animals and surgical procedure
All experimental protocols were approved by the University of Ilorin Ethical Review Committee in accordance with guidelines of the National Institutes of Health Guide for the Care and Use of Laboratory Animals, and every effort was made to minimise both the number of animals used and their suffering. Twelve-week-old female Wistar rats were used for the study. After one week of acclimatisation, animals were anaesthetised (intraperitoneal (i.p.) injection of ketamine, 50 mg/kg) under aseptic conditions and underwent ovariectomy surgery (OVX groups) or sham surgery (SHM group). The surgical procedure was performed as reported before. 26 An antibiotic drug (amoxicillin) was used during the surgery and was also put into the drinking water of the rats after surgery for three days to prevent infection. After a one-week acclimatisation period, the animals were randomly assigned to five new groups (n=5 in each). Rats had unrestricted access to standard rat chow and tap water. Rats were maintained under standard environmental conditions of temperature, relative humidity and a 12-hour dark/light cycle.
Treatment
SHM and OVX groups received distilled water (vehicle; per os (p.o.)), the OVX+COC-treated group received a combination of 1.0 μg ethinylestradiol and 5.0 μg levonorgestrel p.o. (Wyeth-Ayerst, Inc., Montreal, Canada), the OVX+SPL-treated group received 0.25 mg/kg SPL (Pfizer Limited, Kent, UK) and the OVX+COC+SPL-treated group received a combination of COC and SPL p.o. The rats had their respective treatment daily, and this lasted for eight weeks.
Sample preparation
At the end of treatment, the rats were anaesthetised with pentobarbital sodium (50.0 mg/kg i.p.). Blood was collected by cardiac puncture into EDTA-coated and heparinised bottles accordingly. Blood collected into heparinised bottles was centrifuged at 1008 g for five minutes. Plasma was stored frozen until needed for biochemical assay.
IR and visceral adiposity
The IR was determined using the homeostasis model assessment for insulin resistance (HOMA-IR=fasting glucose (mmol/L)×fasting insulin (μIU/L)/22.5), whereas HOMA-β=20×fasting insulin (μIU/L)/fasting glucose–3.5. Visceral fat pads were collected by mid-line section of the rats after anaesthesia. The fat pads collected were peri-renal, abdominal and peri-uterine fats. The fat pads were weighed, and final visceral fat mass was adjusted for body weight. The quantification of the adiposity was determined in a blinded manner.
Biochemical assays
The plasma levels of PAI-1, GSK-3, 17β-oestradiol and corticosterone were estimated using enzyme-linked immunosorbent assay (ELISA) kits (Elabscience Biotechnology Co., Ltd., Wuhan, PR China). Insulin was also determined using an ELISA kit (Ray Biotechnology, Cruz, Canada). The biomarkers of dyslipidaemia including total cholesterol (TC), triglycerides (TG) and high-density lipoprotein-cholesterol (HDL-C) were estimated by standardised enzymatic colorimetric methods using an assay kit obtained from Fortress Diagnostics Ltd. (Antrim, UK), whereas low-density lipoprotein cholesterol (LDL-C) was estimated using Anandaraja’s formula. 27 The atherogenic indices (TC/HDL-C and TG/HDLC ratios) were estimated.
Statistical analysis
All experimental data are expressed as means±standard error of the mean. Statistical significance for measured variables was determined by one-way analysis of variance for the comparison of the mean values of variables among the groups. Bonferroni’s test was used to identify the significance of pair-wise comparison of mean values among the groups. Statistically significant differences were accepted at p<0.05. Statistical group analysis was performed with SPSS statistical software version 21, IBM Corp.
Results
COC and SPL treatment ameliorates visceral adiposity and IR in OVX rats
After eight weeks of experimentation, OVX rats had increased body weight and visceral adiposity compared to SHM rats, suggesting that OVX rats were obese. Treatment with SPL and/or COC significantly reduced the body weight and visceral adiposity (Table 1). OVX rats had hyperinsulinaemia with IR compared to SHM rats, but these were ameliorated in the groups treated with SPL and/or COC (Table 2).
Effect of combined COC and SPL treatment on body weight, visceral adiposity and lipid profile in OVX rats.
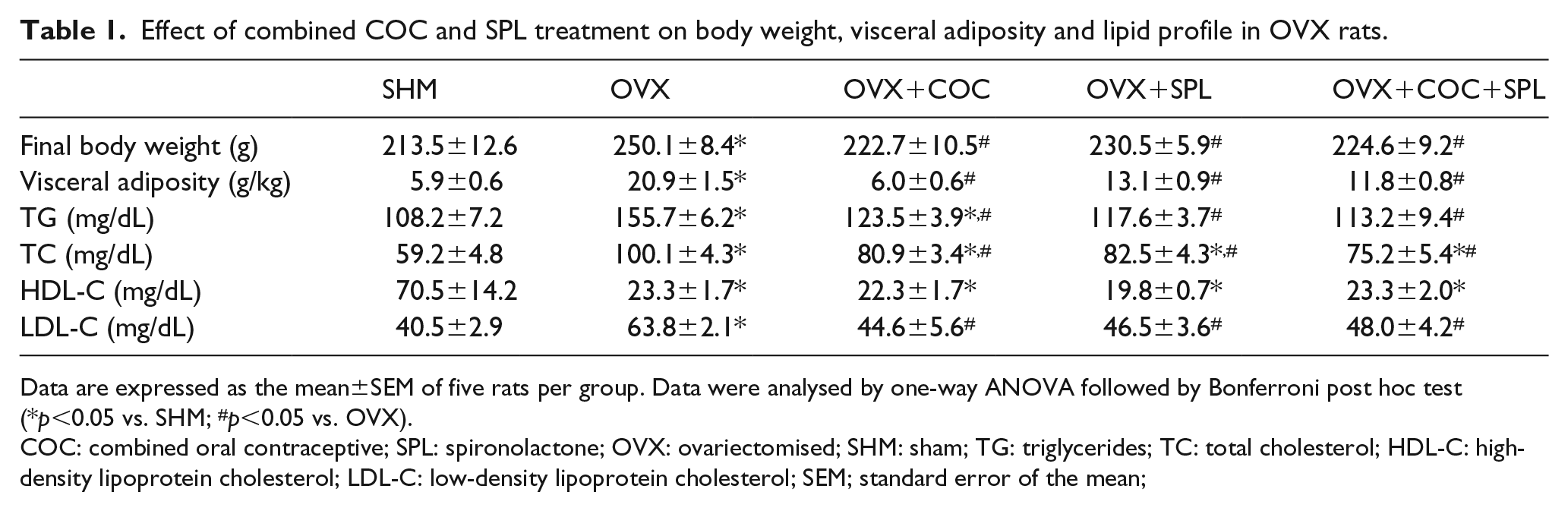
Data are expressed as the mean±SEM of five rats per group. Data were analysed by one-way ANOVA followed by Bonferroni post hoc test (*p<0.05 vs. SHM; #p<0.05 vs. OVX).
COC: combined oral contraceptive; SPL: spironolactone; OVX: ovariectomised; SHM: sham; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; SEM; standard error of the mean;
Effect of combined COC and SPL treatment on fasting blood glucose, insulin, insulin resistance and uric acid in OVX rats.

Data are expressed as the mean±SEM of five rats per group. Data were analysed by one-way ANOVA followed by Bonferroni post hoc test (*p<0.05 vs. SHM; #p<0.05 vs. OVX).
FBG: fasting blood glucose; HOMA-IR: homeostatic model assessment of insulin resistance.
COC and SPL treatment ameliorates atherogenic dyslipidaemia in OVX rats
TG, TC and LDL-C levels were elevated in OVX rats compared to SHM rats (Table 2), which were significantly attenuated in the rats treated with SPL and/or COC compared to OVX rats (Table 2). HDL-C was significantly lowered in all the experimental groups compared to SHM rats (Table 2). Atherogenic lipid indices (TG/HDL-C and TC/HDL-C) were elevated in OVX rats compared to SHM rats. These were significantly attenuated in the groups treated with SPL and/or COC (Figure 1).
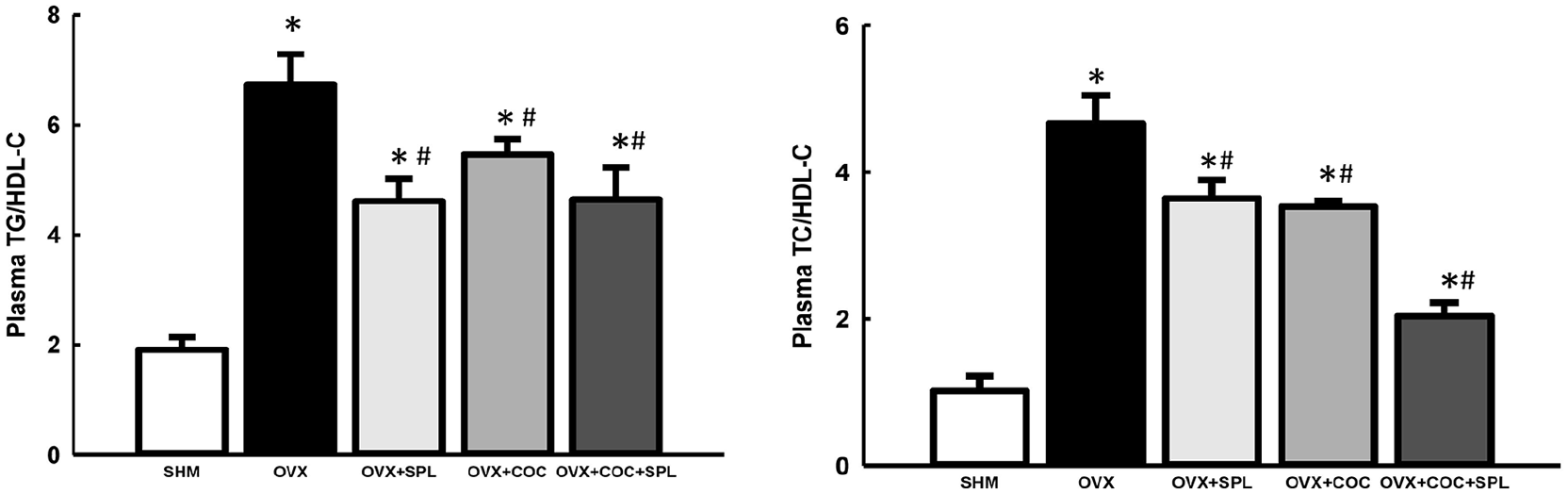
Effect of combined COC and SPL treatment on atherogenic lipid indices (TG/HDL-C (a) and TC/HDL-C (b)) in OVX rats. There was significant increase in TG/HDL-C and TC/HDL-C in OVX rats. However, COC and/or SPL treatment attenuated the atherogenic lipid indices in OVX rats. Data were analysed by one-way ANOVA followed by Bonferroni post hoc test. Values are expressed as the mean±SEM of five rats per group (*p<0.05 vs. SHM; #p<0.05 vs. OVX). COC: combined oral contraceptive; SPL: spironolactone; TG: triglycerides; HDL-C: high-density lipoprotein cholesterol; TC: total cholesterol; OVX: ovariectomised; ANOVA: analysis of variance; SEM: standard error of the mean.
COC and SPL treatment decreases circulating glucocorticoid in OVX rats
OVX rats had elevated corticosterone compared to SHM rats. SPL and/or COC treatment in OVX rats attenuated the corticosterone compared to OVX rats (Figure 2(a)).
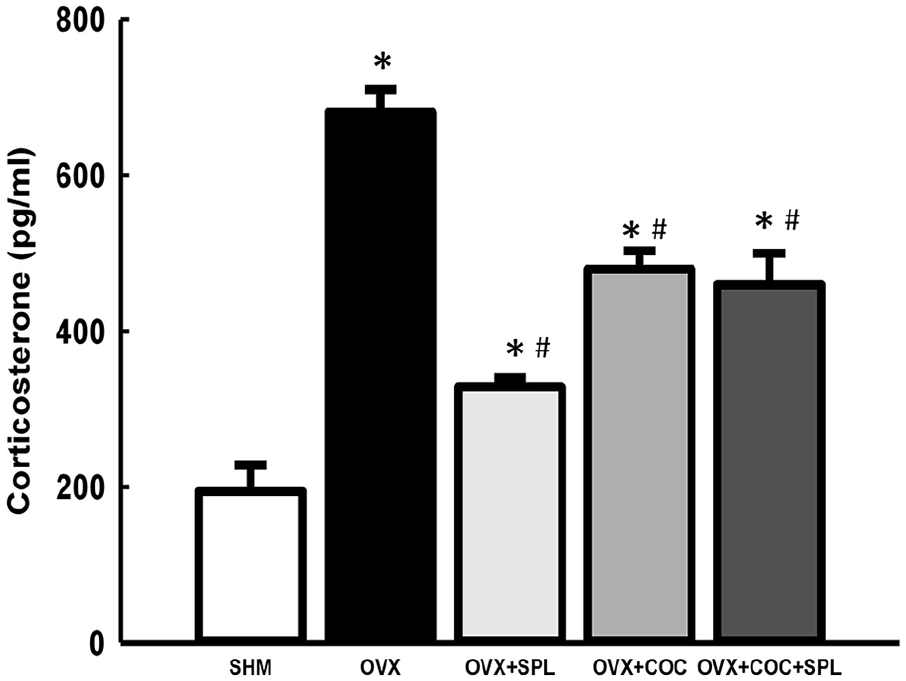
Effect of combined COC and SPL treatment on circulating glucocorticoid in OVX rats. There was significant increase in circulating corticosterone in OVX rats. However, COC and/or SPL treatment led to decreased circulating corticosterone in OVX rats. Data were analysed by one-way ANOVA followed by Bonferroni post hoc test. Values are expressed as the mean±SEM of five rats per group (*p<0.05 vs. SHM; #p<0.05 vs. OVX).
COC and SPL treatment increased circulating oestradiol but decreased circulating PAI-1 and GSK-3 in OVX rats
GSK-3 was elevated in OVX rats but was attenuated in the groups treated with SPL and/or COC (Figure 3). Plasma oestradiol was reduced in OVX rats compared to SHM rats. This was, however, significantly reversed in the groups treated with SPL and/or COC (Figure 4). PAI-1 was reduced in OVX rats compared to SHM rats. SPL or COC treatment led to increased PAI-1 levels compared to OVX rats. Treatment with both SPL and COC in OVX rats attenuated PAI-1 compared to OVX+SPL and OVX+COC rats, respectively (Figure 5).

Effect of combined COC and SPL treatment on circulating GSK-3 in OVX rats. OVX led to increased circulating GSK-3 which was attenuated in the OVX+SPL-, OVX+COC- and OVX+COC+SPL-treated rats. Data were analysed by one-way ANOVA followed by Bonferroni post hoc test. Values are expressed as the mean±SEM of five rats per group (*p<0.05 vs. SHM; #p<0.05 vs. OVX). GSK-3: glycogen synthase kinase-3.

Effect of combined COC and SPL treatment on circulating oestradiol in OVX rats. OVX led to decrease in circulating oestradiol which was increased in the OVX+SPL-, OVX+COC- and OVX+COC+SPL-treated rats. Data were analysed by one-way ANOVA followed by Bonferroni post hoc test. Values are expressed as the mean±SEM of five rats per group (*p<0.05 vs. SHM; #p<0.05 vs. OVX).

Effect of combined COC and SPL treatment on circulating PAI-1 in OVX rats. OVX led to decrease in circulating PAI-1 which was increased in OVX+SPL- and OVX+COC-treated rats. However, OVX+COC+SPL treatment caused a decrease in circulating PAI-1 compared to SHM, OVX+SPL and OVX+COC rats. Data were analysed by one-way ANOVA followed by Bonferroni post hoc test. Values are expressed as the mean±SEM of five rats per group (*p<0.05 vs. SHM; #p<0.05 vs. OVX). PAI-1: plasminogen activator inhibitor-1.
Discussion
The results of the current study demonstrate that OVX rats developed IR accompanied by hyperinsulinaemia, obesity, atherogenic dyslipidaemia, increased circulating GSK-3 and corticosterone and decreased PAI-1 (Figure 6). The results also show that the beneficial effect of SPL or COC is independent of the PAI-1 level in an oestrogen-deficient state. Furthermore, the study provides important findings that treatment with a combination of SPL plus COC improves all these dysfunctions, implying that MR antagonists such as SPL with oral ethinylestradiol/levonorgestrel therapy would be a better therapeutic intervention in the management of cardiometabolic disorders than a single administration. To the best of our knowledge, there has been no clinical or experimental study investigating the combined effects of SPL with ethinylestradiol/levonorgestrel therapy in terms of clinical and/or potential on cardiovascular risk factors in an oestrogen-deficient state.
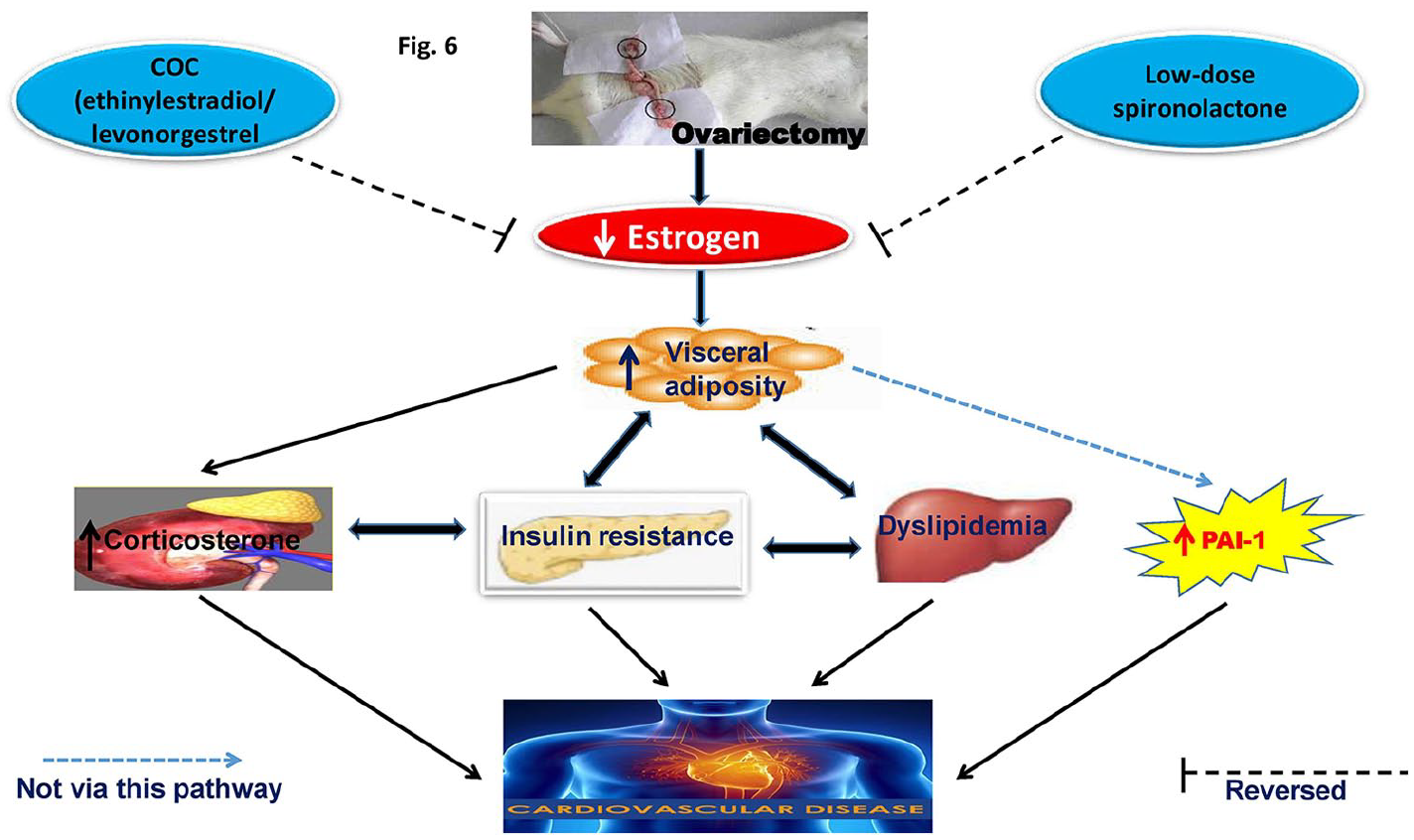
Schematic diagram of the possible mechanism by which oral hormonal therapy with COC and SPL reduce PAI-1 and improve insulin resistance.
IR is a critical metabolic factor that mediates CVDs, thereby making it an enormous global economic burden. 2 Postmenopausal oestrogen deficiency in human and experimental studies has been reported to enhance IR. 28 Moreover, ovariectomy in rats has been shown to lead to an increase in visceral fat,29,30 which is associated with IR.30,31 Use of SPL and/or COC, however, protected the OVX rats from IR and elevated visceral adiposity. Ethinylestradiol/levonorgestrel (COC) therapy was recently shown in our laboratory to be beneficial in OVX rats. 30 Yet, available evidence suggests that SPL with COC use is superior to COC monotherapy for the management of hirsutism and polycystic ovary syndrome.32,33 However, studies are lacking on the use of this combination for IR in clinical or experimental oestrogen deficiency, with our study revealing that SPL with COC use in an oestrogen-deficient state ameliorates IR and visceral adiposity. The protection of the OVX rats treated with SPL and/or COC may also be explained by the increase in oestradiol level (E2) which initially was depleted in OVX rats (Figure 4). Loss of ovarian function is associated with IR, 3 implying a connection between oestrogen deficiency and IR. Hence, SPL and/or COC can be used as alternative oral hormonal therapy.
Reports exist that in postmenopausal women, when the ovaries fail to produce E2, E2 does not function as a circulating hormone. Instead, it is synthesised in extragonadal sites such as the breast, brain, muscle, bone and adipose tissue where it acts locally as a paracrine or intracrine factor. 34 Therefore, the determinant of E2 action in postmenopausal women is not circulating oestrogen. To a certain extent, E2 function depends on oestrogen biosynthesis from a circulating source of androgen. Thus, a major driver of E2 action during menopause is the aromatisation of androgen to oestrogen, 34 which is why oestrogen is present in OVX rats, though significantly reduced compared to ovary-intact SHM rats and the oestrogen-replete OVX+COC, OVX+SPL and OVX+COC+SPL rats in the present study.
The finding that IR induced by OVX in rats is accompanied by increased atherogenic dyslipidaemia characterised by elevations of TC, TG and LDL-C concentrations, a decrease in HDL-C and increased TG/HDL-C ratio, which is a useful marker in identifying individuals at risk for developing atherosclerotic CVD, is noteworthy.35,36 These disturbances in OVX rats are consistent with previous studies in humans and animals.37,38 The observed abnormality in the lipid metabolism may be a consequence of IR and depleted E2 levels. 39 Treatment of OVX rats with SPL and/or COC ameliorated these dyslipidaemia except HDL-C.
Glucocorticoids (GCs) such as corticosterone mobilise glucose to the circulation from the liver, as well as by inhibiting the uptake and utilisation of glucose in the skeletal muscle and adipose tissue. Hence, IR and other CVD risk factors observed are concerns in conditions with elevated circulating GCs.16,40 GCs have been reported to cause impaired insulin action through the GSK-3-dependent pathway. 41 Oestrogen deprivation in menopausal and premenopausal women has also been shown to result in increased circulating corticosteroids. 42 The corticosteroid/GSK-3-dependent pathway has also been implicated in the development of IR. 43 Furthermore, oestrogen action has been shown to be modulated via the GSK-3-dependent pathway. 44 Visceral fat accumulation (and hence obesity) has also been linked to elevated GSK-3. 45 Taken together, the fact that oestrogen deprivation in OVX rats resulted in IR, inflammation, visceral fat accumulation, atherogenic dyslipidaemia accompanied by elevated corticosteroids and GSK-3 suggests that oestrogen deprivation–induced IR might be due to the corticosteroid-GSK-3 mediated pathway. However, treatment with SPL and/or COC ameliorated the circulating corticosterone and GSK-3, possibly via the corticosteroid/GSK-3 pathway and replenishment of oestrogen (Figures 3 and 4).
Increased plasma PAI-1 is suggested to represent a risk factor for CVD 46 but may have different relevance across sexes and hormonal status. 47 This is in line with previous findings in our laboratory where COC treatment induced cardiometabolic disorder that was accompanied by elevated circulating and cardiac PAI-1 levels. 48 The decrease and/or increase in PAI-1 level noticed in OVX rats and during hormone therapy with COC or SPL is in agreement with a previous study.48,49 Contrary to our finding that OVX rats had decreased levels of PAI-1, reports exist that oestrogen deficiency in postmenopausal women is associated with increased levels of PAI-1, while a decrease is found with the oestrogen therapy.6,7 In the same vein, oestrogen repletion with COC or SPL treatment in OVX rats in the present study led to increased PAI-1 levels, negating the general notion that oestrogen replacement therapy improves fibrinolytic balance by decreasing PAI-1. However, this observed increase in PAI-1 level was not associated with a detectable IR and other cardiovascular risk factors, although it has been shown that PAI-1 levels can be triggered or repressed, depending on the activation of the oestrogen receptor subtypes. 50 Moreover, the detrimental effect of PAI-1 seems not to rely solely on its plasma concentration in CVD state. 51
The fact that oestrogen repletion by COC or SPL in our study led to increased levels of PAI-1 further supported the finding that hormonal replacement therapy may also have its downsides, as despite the sufficient experimental evidence of vascular beneficial effects of oestrogen, clinical trials such as the Heart and Estrogen/progestin Replacement Study and Women’s Health Initiative have suggested that hormone replacement therapy in postmenopausal women may increase the risk of atherothrombotic CVD events, 25 accounting for the early increase in CVD mortality rates observed in the Heart and Estrogen/progestin Replacement Study. 52
Combined COC and SPL treatment is a promising alternative in the oestrogen-deficient state, as it causes oestrogen repletion and also decreased PAI-1 levels along with other cardiometabolic risk factors such as IR, hyperinsulinaemia and so on. It is less clear how our study fits with the large body of evidence that hormone therapy decreases PAI-1 levels, 7 but it does suggest that contrary to what was previously thought, 53 an oestrogen-dependent decrease in circulating PAI-1 is not explained by the endothelial effect alone but may rather rely on other phenomena such as modified metabolic clearance. However, this study proved that the combination of COC and SPL therapy in an oestrogen-deficient state is more beneficial than the independent use of COC or SPL in OVX rats.
Taken together, COC or SPL improves IR but increases circulating PAI-1, suggesting that factors other than decreased PAI-1 may account for the beneficial effects of COC or SPL use in an oestrogen-deficient state. Interestingly, a combination of COC and SPL in OVX rats ameliorated IR in a PAI-1-dependent manner.
Footnotes
Acknowledgements
The authors appreciate the technical support from the HOPE Cardiometabolic Research Team, Ilorin, Nigeria.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.