
Abstract
Introduction:
We measured the effects of azilsartan medoxomil co-administered with chlorthalidone 25 mg in stage 2 hypertension.
Methods:
Azilsartan medoxomil 40 or 80 mg plus chlorthalidone were compared with placebo plus chlorthalidone once daily in a randomized, double-blind, 6-week trial. The primary endpoint was change from baseline in 24-hour mean systolic blood pressure by ambulatory blood pressure monitoring.
Results:
Patients (N=551; mean age 59 years; 51.7% men) were randomly assigned to placebo plus chlorthalidone (n=184), azilsartan medoxomil 40 mg plus chlorthalidone (n=185), or azilsartan medoxomil 80 mg plus chlorthalidone (n=182). Baseline systolic blood pressures were similar among groups. After 6 weeks, least squares mean (standard error) reductions with azilsartan medoxomil 40 mg and 80 mg plus chlorthalidone were similar in magnitude (−31.7 (1.0) and −31.3 (1.0) mmHg, respectively), but greater than chlorthalidone alone (−15.9 (1.0) mmHg). Hypotension and serum creatinine elevations were more frequent with azilsartan medoxomil plus chlorthalidone than chlorthalidone alone (reversed with drug discontinuation). Notably, plasma potassium reduction of 0.43 meq/L with chlorthalidone was attenuated to 0.13 and 0.05 meq/L by azilsartan medoxomil 40 mg and 80 mg, respectively.
Conclusion:
Azilsartan medoxomil 40 mg or 80 mg plus chlorthalidone 25 mg was significantly more efficacious than chlorthalidone alone in reducing blood pressure and was well tolerated.
Clinicaltrial.gov, https://clinicaltrials.gov/ct2/show/NCT00591773, NCT00591773
Introduction
Despite the development and availability of several classes of antihypertensive drugs, the majority (⩾75%) of patients with hypertension do not achieve blood pressure (BP) goals with any single agent, indicating a need for combination therapy.1,2 The treatment guidelines that were in effect in the United States during the conduct of the study (e.g. JNC 7) recommend that patients with stage 2 hypertension, defined as clinic systolic BP (SBP) ≥160 mmHg or diastolic BP (DBP) ≥100 mmHg, begin initial treatment with combination therapy rather than monotherapy.2,3 Increasingly, combination therapy has also been suggested as first-line treatment for stage 1 hypertension.4,5
The combination of a thiazide-type diuretic with a blocker of the renin–angiotensin system (RAS), such as an angiotensin receptor blocker (ARB) or angiotensin-converting enzyme (ACE) inhibitor, is recommended by clinical guidelines based on efficacy and safety data from long-term trials.1–3 Hydrochlorothiazide, a thiazide-type diuretic, and chlorthalidone, a thiazide-like diuretic, are both used to treat hypertension, although several studies have found chlorthalidone provides greater BP reductions and has a longer duration of action.6–8 Therefore, chlorthalidone may be more efficacious than hydrochlorothiazide when used in combination with a RAS inhibitor. Data from an observational study of 3849 patients with arterial hypertension treated with either the ARB azilsartan medoxomil (AZL-M) or an ACE inhibitor showed that AZL-M was more effective in improving control of hypertension. 9 Data from phase 2 and 3 clinical trials have demonstrated that compared with the ARBs olmesartan and valsartan, AZL-M monotherapy had similar or better efficacy at 40 and 80 mg doses.10–13 Therefore AZL-M and chlorthalidone in combination may have more powerful antihypertensive effects compared with similar antihypertensive combination therapy. Indeed two phase 3 trials have shown that AZL-M combined with chlorthalidone showed superior antihypertensive efficacy compared with AZL-M and hydrochlorothiazide treatment as well as compared with the ARB olmesartan combined with hydrochlorothiazide.14,15 AZL-M is currently approved for use as a monotherapy at doses of 40 and 80 mg,16,17 and approved in a fixed dosed combination (FDC) with chlorthalidone (AZL-M 40 mg/chlorthalidone 12.5 mg and AZL-M 40 mg/chlorthalidone 25 mg) based, in part, on the data presented in this report as well as other studies in patients with essential hypertension such as the pivotal 8-week factorial design phase 3 trial (clinic SBP 160–190 mmHg) and a phase 3 study in patients who were non-responsive to AZL-M treatment alone (clinic SBP 160–190 mmHg and 24-hour SBP 140–175 mmHg by ambulatory BP monitoring (ABPM)).18–20
An additional major factor in the decision to select chlorthalidone as the thiazide-like diuretic to be combined with AZL-M was evidence showing that chlorthalidone has been utilized in major clinical outcomes trials in hypertension, and was associated with significantly superior stroke prevention than placebo (relative risk 0.64; P=0.0003), 21 and was found to have cardiovascular protective effects similar to those of an ACE inhibitor and a calcium antagonist. 22 It should be noted, however, that clinical outcomes studies with hard cardiovascular endpoints have not been conducted with the AZL-M/chlorthalidone combination.
This phase 3 clinical trial was designed as the first clinical trial of a potential FDC product to assess the additive BP reduction by AZL-M 40 and 80 mg in combination with chlorthalidone 25 mg, and served as the basis for the AZL-M/chlorthalidone FDC clinical development programme, that included, among others, the pivotal phase 3 trial, which led to US Food and Drug Administration approval of the AZL-M/chlorthalidone FDC. 20 Herein, we report the efficacy and safety of AZL-M co-administered in free combination with chlorthalidone in patients with stage 2 hypertension.
Methods
Study design and patient eligibility
This was a phase 3, multicenter, randomized, parallel-group, double-blind, placebo-controlled study to evaluate the efficacy and safety of AZL-M when combined with chlorthalidone 25 mg once daily in patients with stage 2 essential hypertension. Eligible patients were randomly assigned in a 1:1:1 ratio by an interactive voice response system to receive once daily AZL-M 40 mg with chlorthalidone 25 mg, AZL-M 80 mg with chlorthalidone 25 mg, or chlorthalidone 25 mg with placebo for 6 weeks. Treatment randomization was stratified by race: black and non-black. AZL-M was manufactured by Takeda Pharmaceutical Company (Osaka, Japan) and chlorthalidone 25 mg was manufactured by Mylan Pharmaceuticals Inc. (Morgantown, WV, USA). The protocol conformed to the Declaration of Helsinki and regional regulatory guidelines and the study was approved by regional institutional review boards. Each patient signed an institutional review board-approved consent form before any study procedures were initiated. The study medication blind was maintained using the interactive voice response system, which was accessed by the study sites for randomization number and study medication assignments.
To qualify for randomization, patients were required to be at least 18 years of age, to participate in a 3- to 4-week washout of previous antihypertensive therapy if treated previously (with all patients receiving single-blind placebo during the final 2 weeks of the washout), and to have stage 2 hypertension defined as a post-washout sitting trough clinic SBP ≥160 and ≤190 mmHg at day –1 (day prior to randomization) and 24-hour mean SBP ≥140 mmHg and ≤180 mmHg by ABPM at day 1. 23 Patients were also expected to have within the reference range clinical laboratory test results (including clinical chemistry, hematology and complete urinalysis) or abnormal results that were deemed not clinically significant for inclusion by the investigator.
Patients with any forms of secondary hypertension, known or suspected unilateral or bilateral renal artery stenosis, severe hypertension (seated clinic DBP >119 mmHg), those with a recent (within 6 months) history of major cardio-, or cerebrovascular event, clinically significant cardiac conduction defect, left ventricular outflow tract obstruction/aortic valvular disease, severe renal impairment (calculated glomerular filtration rate (cGFR) <30 mL/min/1.73 m2) were excluded. In addition, patients with hyper- or hypokalemia (defined as serum potassium outside of the normal reference range of the central laboratory), alanine aminotransferase level >2.5 times the upper limit of normal (ULN), type 1, or poorly controlled diabetes (glycosylated hemoglobin >8%), those with hypersensitivity to ARBs, thiazide-type diuretics, or other sulfonamide-derived compounds, or who were taking or expected to take an excluded medication, patients with an arm circumference <24 cm or >42 cm, night-shift workers, or those with baseline 24-hour ABPM reading of insufficient quality, and pregnant, or nursing women and those with childbearing potential not using approved means of contraception were also excluded.
Blood pressure assessments
ABPM was performed prior to randomization on day –1, and at week 6 (or early termination, if at least 4 weeks of double-blind therapy was completed) with a Spacelabs 90207 monitor (Spacelabs, Inc, Issaquah, WA, USA). The monitor was fitted in the morning immediately after trough clinic BP measurement and in-clinic dosing, and was programmed to measure BP every 15 minutes between 06.00 am and
Trough seated clinic BP measurements were taken at approximately 24 hours past the previous dose and prior to dosing or blood collection on days of clinic visits, with the patient sitting with feet on the floor in a quiet environment for at least 5 minutes. An appropriate sized cuff was applied to the non-dominant arm (supported at heart level), and three serial measurements were taken (with at least 2 minute intervals) with an automated, calibrated and certified device (Omron HEM 705CP, Omron Healthcare, Inc., Kyoto, Japan). The average of the three sitting BP levels was used to determine eligibility and at all visits (screening, baseline, weeks 2, 4, 6/early termination). A single pulse measurement was also taken manually.
Safety assessments
All patients who received at least one dose of study medication were included in the safety analysis set. Safety assessments included treatment-emergent adverse events (TEAEs; defined as adverse events that started after the first dose of double-blind study drug and ⩽14 days (or ⩽30 days for a serious adverse event) after the last dose of double-blind study drug), clinical laboratory data (including chemistry, hematology, lipid profile, fasting plasma glucose, and human chorionic gonadotropin (for female patients of childbearing potential)), weight, vital signs, physical examination, and 12-lead electrocardiograms. An additional safety variable, cGFR using the Modification of Diet in Renal Disease equation, was calculated and provided by the central laboratory (ICON Laboratories, Farmingdale, NY, USA). All TEAEs observed by the investigator or reported spontaneously by the patient were recorded and further characterized by the investigator for seriousness, and whether or not the event led to discontinuation of treatment. In addition, the protocol was amended to instruct investigators on the monitoring and management of patients with elevated serum creatinine >1.3 or >1.5 times above baseline and ULN, based on the National Kidney Foundation practice guideline. 24
Exploratory variables included high-sensitivity C-reactive protein (hs-CRP), adiponectin, insulin and plasminogen activator inhibitor type 1. Additional variables included homeostasis model assessment of insulin resistance and urine albumin-to-creatinine ratio, which were calculated and provided by the central laboratory.
Statistical analyses
Data analysis, tabulations of descriptive statistics, and inferential statistics were performed using SAS, version 8.02 (SAS Institute, Cary, NC, USA). All efficacy analyses were based on the full analysis set (FAS) and per protocol set (PPS). The FAS was defined as all randomly assigned patients who received at least one dose of double-blind study medication. The PPS was defined as all patients in the FAS except those subjects identified as having a major protocol violation. A patient was included in the analyses of a specific continuous variable only when there was both a baseline value and at least one value obtained during the double-blind treatment period. The last observation carried forward method was used to impute missing data. The data with the last observation carried forward method applied were used for the primary efficacy analysis.
The primary efficacy variable was change from baseline in the 24-hour mean SBP by ABPM, while the key secondary efficacy variable was change from baseline in trough clinic sitting SBP. ABPM SBP was chosen as the primary endpoint as several studies have shown that 24-hour SBP is the best predictor of cardiovascular risk, even after adjustment for risk factors including clinic BP.25–27 Treatment group comparisons (AZL-M plus chlorthalidone vs. placebo plus chlorthalidone) for the change from baseline in efficacy variables were carried out using an analysis of covariance (ANCOVA) with terms for treatment and baseline value (as a covariate) in the model. Model estimates, including P values, least squares (LS) means, and 95% confidence intervals (CIs) for treatment differences in the change from baseline were developed within the ANCOVA framework. Type 1 error was controlled for in the primary analysis by using the closed testing principle. An additional secondary analysis was performed on change from baseline in 24-hour mean ABPM DBP with treatment as fixed effect and baseline in 24-hour mean ABPM DBP as a covariate. These analyses were also performed on other ABPM parameters for SBP and DBP, including daytime mean (06.00 am to 10.00 pm), nighttime mean (12.00 am to 06.00 am), BP mean at 0–12 hours after dosing, and trough mean at 22–24 hours after dosing. Subgroup analyses such as age, sex, race and other important baseline factors were also performed for primary and secondary efficacy variables.
Sample size was estimated based on SBP by ABPM and clinical sitting SBP as it was a key secondary endpoint. Assuming a 13 mmHg standard deviation (SD) for the mean change from baseline in 24-hour mean SBP by ABPM for any treatment and a 15% dropout rate, a total of 540 patients (180 per treatment group) was determined to be sufficient to achieve at least 90% power to detect a difference of 5 mmHg between the AZL-M plus chlorthalidone treatment groups and placebo plus chlorthalidone group by a two-sample t-test of the mean change from baseline in 24-hour mean ABPM SBP with a two-sided significance level of 5%. Similarly, assuming a SD of 14 mmHg for the mean change from baseline in trough clinic sitting SBP, the sample size provided at least 85% power to detect a difference of 5 mmHg in trough clinic sitting SBP between the AZL-M plus chlorthalidone treatment groups and placebo plus chlorthalidone group with a two-sided significance level of 5%.
Results
Patient disposition and demographics
Patients were enrolled at 74 investigative sites in Argentina, Chile, Mexico, Peru and the United States from September 2007 to March 2009. The disposition of patients screened and enrolled in the study and the demographics of enrolled patients are shown in Figure 1 and Table 1, respectively. Patient demographics were comparable between groups. A total of 1786 patients were screened, and 1344 patients from 74 sites in the United States and Latin America entered the single-blind period. Of these patients, 551 were randomly assigned to treatment with placebo with chlorthalidone 25 mg (n=184), AZL-M 40 mg with chlorthalidone 25 mg (n=185), or AZL-M 80 mg with chlorthalidone 25 mg (n=182). All but four randomly assigned patients received at least one dose of double-blind study medication (three in the AZL-M 40 mg plus chlorthalidone 25 mg group and one in the placebo plus chlorthalidone 25 mg group). A total of 495 (89.8%) patients completed the study. The most common reasons for premature discontinuation included adverse events (4.4%) and voluntary withdrawal (1.8%). There was a higher withdrawal rate in the AZL-M 80 mg plus chlorthalidone 25 mg group (13%) versus the other groups (8.6–8.7%), primarily due to more patients who voluntarily withdrew or were lost to follow-up. Among the randomly assigned participants, the mean age was 58.7 years, with males and females similarly represented; the baseline mean 24-hour BP (151.4/89.7–153.2/90.5 mmHg) and mean clinic BP (165.6/93.4–166.4/94.8 mmHg) were similar across the groups. There were no major differences with respect to other demographic characteristics.

Disposition of patients.
Patient demographics.

Ethnicity was not collected at Latin American sites.
Patients who indicated more than one race category were included in each category indicated, and they were included in the multiracial category. Thus, the sum of the number of patients by racial category may be greater than the total number of patients in the treatment group.
Patients who self-identified as being Native American were predominantly from Latin America.
Drug class not available.
AZL-M: azilsartan medoxomil; CLD: chlorthalidone; RAAS: renin–angiotensin–aldosterone system; SD: standard deviation.
Change from baseline in SBP
At baseline, 24-hour LS mean (standard error (SE)) SBP by ABPM was similar among the chlorthalidone-alone (153.4 (0.8) mmHg) and the AZL-M 40 mg plus chlorthalidone (152.0 (0.8) mmHg) and AZL-M 80 mg plus chlorthalidone (151.9 (0.8) mmHg) groups. After the 6-week treatment period, the LS mean (SE) reductions in SBP by 24-hour ABPM observed in the AZL-M 40 mg plus chlorthalidone and AZL-M 80 mg plus chlorthalidone co-administration groups were similar in magnitude (−31.7 (1.0) and −31.3 (1.0) mmHg, respectively), but greater than that of the chlorthalidone-alone group (−15.9 (1.0) mmHg) (Figure 2). A statistically significant LS mean difference was observed for the change from baseline in 24-hour mean SBP between the chlorthalidone-alone and AZL-M 40 mg plus chlorthalidone groups (−15.9 (95% CI −18.5, −13.2) mmHg; P<0.001) and between the chlorthalidone-alone and AZL-M 80 mg plus chlorthalidone groups (−15.5 (95% CI −18.1, −12.8) mmHg; P<0.001). Overall, there was a significant change from baseline following 6 weeks of treatment between chlorthalidone alone and AZL-M plus chlorthalidone (P<0.001). Similar results were also observed for the analysis based on the PPS, in which the LS mean difference for AZL-M 40 mg plus chlorthalidone co-administration and AZL-M 80 mg plus chlorthalidone groups was −16.5 (95% CI −19.4, −13.6) and −15.5 (95% CI −18.3, −12.6), respectively, relative to chlorthalidone alone (P<0.001 for all comparisons).
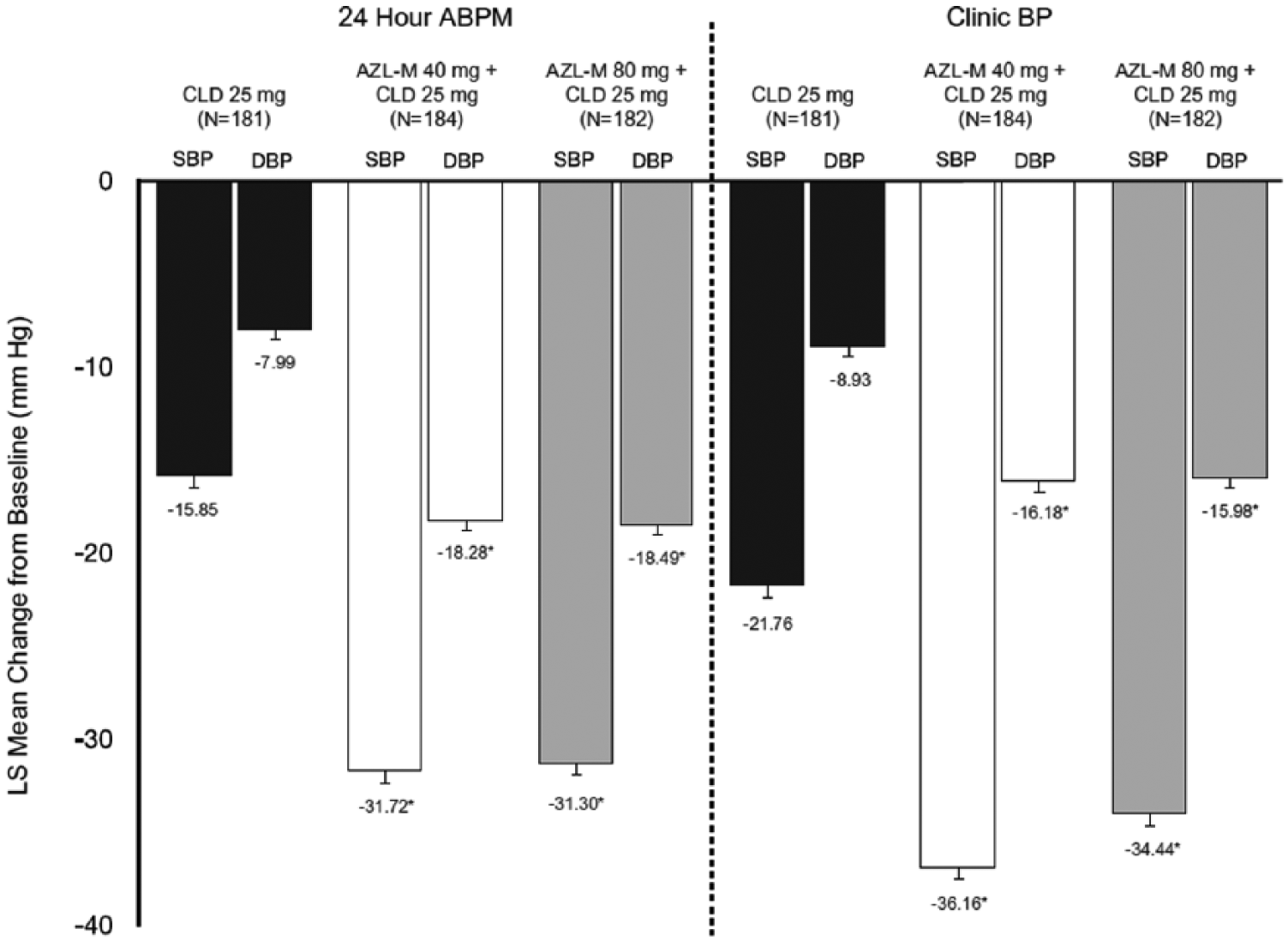
Clinic and ABPM results for both SBP and DBP.
Clinic SBP observations were similar to those observed with 24-hour ABPM. At baseline, LS mean (SE) clinic SBP was similar among the chlorthalidone-alone (165.6 (1.0) mmHg) and AZL-M 40 mg plus chlorthalidone (166.3 (1.0) mmHg) and AZL-M 80 mg plus chlorthalidone (166.3 (1.1) mmHg) groups. At week 6, LS mean (SE) reductions in clinic SBP in both the AZL-M 40 mg plus chlorthalidone and AZL-M 80 mg plus chlorthalidone co-administration groups were similar in magnitude (−36.2 (1.2) and −34.4 (1.2) mmHg, respectively), but greater than that observed in the chlorthalidone-alone group (−21.8 (1.2) mmHg) (Figure 2). AZL-M 40 mg plus chlorthalidone and AZL-M 80 mg plus chlorthalidone were associated with statistically significantly greater reductions of 14.4 mmHg (95% CI −17.81, −10.99) and 12.7 mmHg (95% CI −16.10, −9.25), respectively, relative to the chlorthalidone-alone group (P<0.001 for both individual comparisons).
Change from baseline in DBP
The baseline 24-hour LS mean (SE) DBP by ABPM was also similar between the chlorthalidone-alone (89.8 (0.9) mmHg) and both the AZL-M 40 mg plus chlorthalidone (90.5 (0.9) mmHg) and AZL-M 80 mg plus chlorthalidone (90.1 (0.9) mmHg) groups. After 6 weeks of treatment, reductions in ABPM DBP in both the AZL-M 40 mg plus chlorthalidone and AZL-M 80 mg plus chlorthalidone co-administration groups were similar in magnitude (−18.3 (0.6) mmHg, −18.5 (0.6) mmHg, respectively), but greater than that observed with chlorthalidone alone (−8.0 (0.6) mmHg) (Figure 2). The difference in the change from baseline was statistically significant across groups (P<0.001). Relative to chlorthalidone, the LS mean of the reduction from the baseline was significantly greater for AZL-M 40 mg plus chlorthalidone (the differences in the LS means are −10.3 mmHg (95% CI −12.0, −8.6)) and AZL-M 80 mg plus chlorthalidone (−10.5 mmHg (95% CI −12.2, −8.8)).
At baseline, LS mean (SE) clinic DBP measures were also similar among the chlorthalidone-alone (93.5 (0.9) mmHg) and the AZL-M 40 mg (94.7 (0.9) mmHg) and 80 mg (94.5 (0.9) mmHg) plus chlorthalidone groups. After 6 weeks of treatment, reductions in clinic DBP in both the AZL-M 40 mg plus chlorthalidone and AZL-M 80 mg plus chlorthalidone groups were similar in magnitude (−16.2 (0.7) mmHg and −16.0 (0.7) mmHg, respectively) but greater than that observed in the chlorthalidone-alone group (−8.9 (0.7) mmHg) (Figure 2). The differences in the LS means of the change from baseline (−7.3 mmHg (95% CI −9.3, −5.3) and −7.1 mmHg (95% CI −9.1, −5.1)) were statistically significant for the AZL-M 40 mg and 80 mg plus chlorthalidone co-administration groups, respectively, relative to the chlorthalidone-alone group (P<0.001 for both individual comparisons). Significantly greater reductions in mean clinic DBP were also observed in both AZL-M plus chlorthalidone groups relative to the chlorthalidone-alone group at week 2 and week 4.
At baseline, there were no statistically significant differences across treatment groups for any of the mean ABPM SBP or DBP parameters (trough, daytime, nighttime and 0–12 hours after dosing). At week 6, ABPM parameters for both SBP and DBP showed greater reductions in the nighttime and trough measures in the chlorthalidone-alone group compared with daytime measures, whereas the opposite was true for the co-administration therapy groups. However, co-administration therapy yielded incremental reductions in SBP/DBP for each measure, and there were statistically significantly greater reductions in favor of each AZL-M plus chlorthalidone group relative to chlorthalidone alone for all ABPM parameters (Table 2). Results were similar between the FAS analyses described above and the analyses based on the PPS (Supplemental Table 2). The mean SBP values observed at each hour of the week 6 ambulatory recording are shown in Figure 3. Both AZL-M plus chlorthalidone co-administration groups’ 24-hour and 12-hour trough to peak ratios for SBP and DBP were >0.5 (range 0.52–0.63) and slightly higher than those of the chlorthalidone-alone group (range 0.37–0.56). Patients aged ≥65 years tended to have a higher baseline 24-hour SBP compared with those aged <65 years; however, treatment responses were similar in both groups.
Baseline to week 6 for other ABPM parameters.

P<0.001.
ABPM: ambulatory blood pressure measurement; AZL-M: azilsartan medoxomil; CI: confidence interval; CLD: chlorthalidone; DBP: diastolic blood pressure; LS: least squares; SBP: systolic blood pressure; SE: standard error.
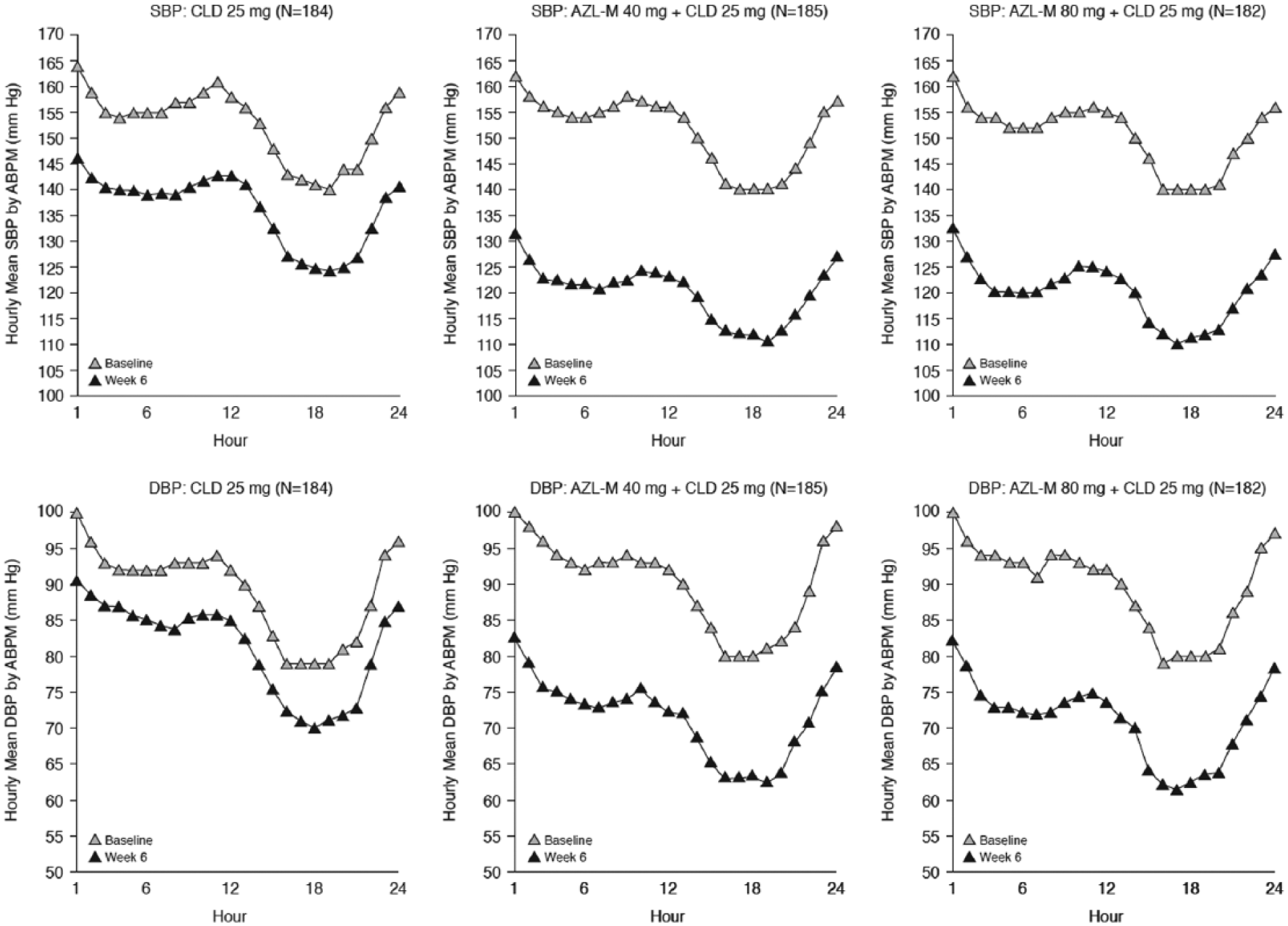
Hourly SBP and DBP ABPM data at baseline and week 6.
Subgroup analyses for heterogeneity of BP effects of AZL-M when co-administered with chlorthalidone relative to chlorthalidone alone were performed by age, gender, race, body mass index (BMI), baseline 24-hour mean SBP and cGFR for primary and secondary efficacy variables. Greater BP reductions were observed with AZL-M plus chlorthalidone therapy relative to chlorthalidone alone across all subgroups examined (Supplemental Table 3).
Achievement of response criteria
For each response criterion (defined as clinic SBP <140 mmHg and/or reduction of ⩾20 mmHg from baseline, clinic DBP <90 mmHg and/or reduction of ⩾10 mmHg from baseline, and joint SBP and DBP criteria), both co-administration groups had a statistically significantly higher proportion of responders than in the chlorthalidone-alone group (Figure 4). For both the SBP and combined SBP and DBP categories, there were over 20% more responders in the co-administration groups compared with the chlorthalidone-alone group. Likewise, improved response was also observed for the DBP category, with over 12% more responders in the co-administration groups compared with the chlorthalidone-alone group. Similar results were observed in the analysis based on the PPS.

Proportion of patients achieving BP target at final visit.
Safety
As summarized in Table 3, the overall frequency of TEAEs across groups was similar (chlorthalidone alone (51.9%) and AZL-M 40 mg and 80 mg co-administration groups (52.2%) and (51.6%), respectively); however, there were notable variations in the reporting rates of individual TEAEs. Commonly reported TEAEs (⩾2% of patients in any of the treatment groups), such as dizziness, hypotension, increased blood creatinine, diarrhea, urinary tract infection, hematuria, asthenia and muscle spasms were more frequent in the AZL-M with chlorthalidone groups, whereas headache and hypokalemia were reported more frequently in the chlorthalidone-alone group. Increased serum plasminogen activator inhibitor and elevated hs-CRP, which were exploratory variables, were also commonly reported and more frequent in the AZL-M plus chlorthalidone groups.
Treatment-emergent adverse events.

TEAEs were coded using the medical dictionary for regulatory activities, version 11.1.
Includes edema and edema peripheral.
Although blood potassium decrease was reported in <2% of patients, it is included because it is related to the preferred term hypokalemia.
AZL-M: azilsartan medoxomil; CLD: chlorthalidone; hs-CRP: high-sensitivity C-reactive protein; TEAE: treatment-emergent adverse event.
The percentage of patients with a TEAE that the investigator considered related (possibly, probably, or definitely) to the study drug was higher in the AZL-M plus chlorthalidone groups relative to chlorthalidone alone, primarily due to increased reports of dizziness in the co-administration arms. The majority of TEAEs were mild to moderate in severity. Reports of TEAEs that led to discontinuation and serious TEAEs were infrequent. The incidence of TEAEs that led to permanent discontinuation was slightly higher in the AZL-M plus chlorthalidone groups than with chlorthalidone alone. A total of seven patients across treatment groups reported serious TEAEs, including one death in the chlorthalidone-alone group (due to cardiogenic shock). There were two serious TEAEs of syncope, one in each AZL-M plus chlorthalidone group, but these events did not result in discontinuation. TEAEs related to signs and symptoms of hypotension (such as dizziness) were reported more frequently in the AZL-M plus chlorthalidone groups.
Among laboratory parameters, a mean increase from baseline in serum creatinine tended to be greater in the AZL-M plus chlorthalidone groups compared with chlorthalidone alone, whereas the mean decrease from baseline in serum potassium was greater in the chlorthalidone-alone group compared with AZL-M 40 mg and 80 mg plus chlorthalidone co-administration groups. Moderate increases of uric acid were observed in all groups, with slightly greater mean increases in the AZL-M plus chlorthalidone groups. Small increases of glucose and creatine kinase were observed proportionally in all groups. There were no significant mean changes from baseline in liver function parameters in any treatment group (Supplemental Table 4).
Creatinine elevations that met certain criteria (⩾30% and ⩾50% from baseline and >ULN) were reported by investigators as TEAEs of special interest, and patients with ≥50% ULN elevations were considered for discontinuation. All patients with creatinine elevations meeting either criteria were followed up until normalization or stabilization. An analysis of the relationship between creatinine elevations and BP reduction showed that patients with serum creatinine elevations had a higher mean SBP at baseline and also experienced greater reductions in SBP at week 6 than patients without serum creatinine elevations. Among patients with serum creatinine elevations who had available follow-up data, serum creatinine returned to or near baseline levels in all but one patient.
Discussion
In this study of patients with stage 2 hypertension, co-administration of AZL-M 40 mg/chlorthalidone 25 mg and AZL-M 80 mg/chlorthalidone 25 mg produced clinically meaningful and statistically significant reductions in 24-hour mean SBP and clinic trough SBP relative to chlorthalidone alone. In addition, both combination doses were more effective than chlorthalidone alone in achieving BP responses for clinic SBP, DBP, and joint SBP and DBP targets. Importantly, the treatment effect observed in the chlorthalidone 25-mg alone group (–21.8 mmHg) was consistent with previously reported reductions between 15 mmHg and 20 mmHg in patients with mild to moderate hypertension.28,29 Likewise, reductions in 24-hour mean SBP in the chlorthalidone-alone arm (–15.9 mmHg) were consistent with those observed in an ABPM study of chlorthalidone 25 mg (–12.4 mmHg), albeit in a small cohort of subjects with less severe hypertension (mean baseline clinic SBP 145 mmHg). 29
Previous studies have shown that as monotherapy, chlorthalidone was more effective in controlling hypertension than hydrochlorothiazide.6–8 Furthermore, AZL-M alone has been shown to be more efficacious compared to olmesartan and valsartan.10–13 Therefore, these two drugs were selected as combination therapy in this study as they represented the most effective antihypertensive agents in their respective classes. The current study was the first clinical trial of the AZL-M/chlorthalidone FDC clinical development programme and led to further clinical trials including a phase 3 trial composed of 1714 patients treated with AZL-M (20, 40, or 80 mg) and/or chlorthalidone (12.5 mg or 25 mg) for 8 weeks. 18 Patients treated with AZL-M and chlorthalidone in combination showed greater reductions in both clinic SBP and ABPM SBP when compared with AZL-M or chlorthalidone monotherapy. Compelling clinical interest led to the immediate drafting and publication of two other clinical trials of AZL-M/chlorthalidone FDCs immediately on study completion.14,15 In a study of 1071 patients with stage 2 hypertension, patients treated with fixed-dose AZL-M 40 mg with chlorthalidone 25 mg showed a greater reduction in both clinic SBP (5–7 mmHg) and ABPM SBP (7–9 mmHg) following 12 weeks of treatment compared with fixed-dose olmesartan plus hydrochlorothiazide combination therapy. 14 In another study of 609 patients with stage 2 hypertension, treatment with fixed-dose AZL-M 40 mg plus chlorthalidone 25 mg provided greater and clinically meaningful reductions in clinic SBP compared with co-administration of AZL-M 40 mg plus hydrochlorothiazide 25 mg treatment (35.1 mmHg vs. 29.5 mmHg; P<0.001). 15 The current study, although completed prior to Cushman et al. 14 and Bakris et al., 15 is clinically relevant as these data provided the basis for a full phase 3 clinical development programme resulting in the approval of FDC AZL-M/chlorthalidone in the United States and Mexico, and in other countries in South America, Europe and Asia. In keeping with the antihypertensive results observed in this study, we also note that azilsartan and azilsartan in fixed combination with chlorthalidone used in the SPRINT trial of 9351 patients with SBP ≥130 mmHg, in which patients achieved a mean SBP of 136.2 mmHg (n=4683; standard treatment group) or 121.4 mmHg (n=4678; intensive treatment group) following one year of treatment. 30 Taken together, AZL-M plus chlorthalidone combination therapy provides effective and additive BP reductions in patients with stage 2 hypertension.
Examination of BP reduction by subgroup, including age, race, sex and BMI, did not reveal evidence of heterogeneity in response to AZL-M plus chlorthalidone treatment. In particular, the response to AZL-M 40 mg or 80 mg plus chlorthalidone 25 mg therapy was comparable among black and white patients, with absolute reductions in 24-hour SBP ranging between 31.4 mmHg and 34.2 mmHg across both subgroups and doses. Decreases in 24-hour SBP with AZL-M plus chlorthalidone relative to chlorthalidone alone were not substantially different in either subgroup (range –14.9 to –16.6 mmHg), although interpretation of these data are limited by the relatively small number of black patients in the subgroup analyses.
Overall, AZL-M/chlorthalidone co-administration was well tolerated and the incidence of TEAEs was low among all three treatment groups. The majority of TEAEs were mild or moderate in severity. Patients in the chlorthalidone-alone group experienced higher rates of headache and hypokalemia, compared with combination therapy. In fact, the use of AZL-M largely mitigated the hypokalemic effect caused by the diuretic chlorthalidone, thus providing an approach for utilizing the antihypertensive efficacy of chlorthalidone while minimizing its adverse effect on potassium metabolism. A greater proportion of patients experienced dizziness in the combination therapy groups compared with chlorthalidone alone. The types of TEAEs and discontinuation rates in this study were similar to those reported in previous studies and confirm the safety and tolerability profile of azilsartan plus chlorthalidone.14,15
Limitations
Notably, while previous phase 3 trials examining the antihypertensive effects of AZL-M alone tended to display a consistent though modest pattern of dose differentiation between 40 mg and 80 mg,10,11 these trends were not observed in this study; however, this study did not formally evaluate differences in efficacy between AZL-M 40 mg and AZL-M 80 mg co-administered with chlorthalidone. A similar pattern of blunted dose–response has been observed with other ARB–diuretic combinations.31,32
Conclusion
Co-administration of AZL-M 40 mg and 80 mg with chlorthalidone 25 mg was associated with a positive benefit to risk and tolerability profile relative to chlorthalidone 25 mg alone. Co-administration was also significantly more efficacious than chlorthalidone 25 mg alone in reducing BP. This study confirms that combination therapy with AZL-M and chlorthalidone is an effective antihypertensive treatment in patients with stage 2 essential hypertension.
Supplemental Material
Supplement_Tables – Supplemental material for A randomized trial of the efficacy and safety of azilsartan medoxomil combined with chlorthalidone
Supplemental material, Supplement_Tables for A randomized trial of the efficacy and safety of azilsartan medoxomil combined with chlorthalidone by Michael A Weber, Peter Sever, Attila Juhasz, Andrew Roberts and Charlie Cao in Journal of the Renin-Angiotensin-Aldosterone System
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MAW is a consultant for Boehringer-Ingelheim, Daiichi Sankyo, Forest, Novartis, and Takeda; PS has received grant income from consultancies from Pfizer and Amgen and consultancy fees from Takeda; AJ and AR are no longer employees of Takeda, though, they were during the time the research was conducted; CC is an employee of Takeda.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Takeda Development Center Americas, Inc., Deerfield, IL, USA. High-resolution and color figures as well as drafting or formatting tables for this manuscript were produced by Sam Schmitt of Extenxion Media Group, LLC and Blue Momentum, an Ashfield Company, and were supported by Takeda Development Centers America, Inc.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.