
Abstract
Introduction:
Hypertension guidelines recommend fixed-dose combinations for enhanced blood pressure (BP) reduction and compliance. The objective of this study was to assess the effectiveness and safety of fixed-dose perindopril/amlodipine combination in reducing and controlling BP in Greek hypertensive patients, as well as the effect of baseline BP and added cardiovascular risk on BP reduction.
Methods:
This 6-month prospective observational study included male or female patients ⩾18 years with essential hypertension prescribed fixed-dose combination perindopril/amlodipine. BP was measured at baseline and 3 and 6 months. Baseline cardiovascular risk and treatment compliance were also assessed.
Results:
In 2231 per protocol patients, mean systolic BP decreased from 157.0±15.4 mm Hg to 129.0±7.9 mm Hg after 6 months, and diastolic BP from 91.5±10.1 to 78.8±6.7 mm Hg (both p < 0.001). BP control was achieved in 84.8% at 6 months. Patients with higher baseline added cardiovascular risk or BP had greater BP reduction (p < 0.001). Compliance was good (97.1% took treatment “every day” or “quite often”) and few (n = 27; 1.2%) discontinued treatment prematurely due to adverse events.
Conclusions:
Fixed-dose perindopril/amlodipine safely and effectively reduced high BP in real-life practice, achieving BP control in most patients. About half of Greek hypertensive patients have high/very high added cardiovascular risk.
Introduction
Arterial hypertension is a major global public health problem, both because of its incidence and its correlation with cardiovascular disease. 1 Forecasts for the burden caused by arterial hypertension predict an increase of up to 60% in patients with arterial hypertension by 2025. 1 Moreover, arterial hypertension has been identified as one of the major risk factors for cardiovascular disease and mortality, as it has been directly related to the development of chronic coronary artery disease, heart failure, peripheral artery disease and renal failure, in both men and women.2–5 Prevention, early detection, and treatment of arterial hypertension are thus crucial for global public health.6,7
Available data suggest that despite the wide availability of effective therapies, hypertension remains poorly controlled. 8 In patients with high added cardiovascular risk, it is important that target blood pressure (BP) values should be achieved within the shortest possible period. Antihypertensive monotherapy, however, rarely reduces high BP to target values.9,10 Combining different antihypertensive agents in fixed combinations is able to do this more effectively than increasing the dose of monotherapy, 11 while simplifying therapeutic regimens and improving patient compliance.6,7,12,13
The objectives of this observational study were to assess the safety and effectiveness of fixed-dose combination perindopril/amlodipine in hypertensive patients in real-life practice over a 6-month period. Other objectives included the evaluation of treatment compliance and the identification of total cardiovascular risk of patients and coexisting risk factors in hypertensive patients in Greece.
Patients and methods
Patients with essential hypertension from 230 private practices in Greece were enrolled in this multicenter, prospective, non-interventional study, coordinated by three Greek hospital cardiology departments. Physician recruitment mirrored the epidemiological distribution of physicians in Greece. 14 Evaluations were performed at inclusion, 3 months, and 6 months, and the duration of patient follow-up was 6 months. The first patient was enrolled on September 3, 2012, and the date of the last visit was September 7, 2013. Study design was based on recommendations of the current Helsinki Declaration, guidelines of good pharmacoepidemiology practice (ISPE GPP), and rules of good clinical practice (ICH-GCPs). Approval was obtained from ethics committees of all participating centers. All patients were informed and gave written consent, prior to inclusion.
Patients were ambulatory men or women ⩾18 years old, with diagnosed essential hypertension that was treated with daily fixed-dose combination perindopril arginine/amlodipine (available in dosages of 5/5, 5/10, 10/5, or 10/10 mg). The decision to administer perindopril/amlodipine had to be made before patient inclusion, and treatment was initiated a maximum of two weeks before enrollment. Exclusion criteria included secondary hypertension; serious end-stage diseases (cancer or serious liver, respiratory, heart, or renal insufficiency); severe neuropsychiatric diseases; cerebrovascular events with serious residual neurologic deficit; and pregnancy, lactation, or desire to become pregnant.
Demographic characteristics, cardiovascular parameters, coexisting risk factors for hypertension, comorbidities, and concomitant medication were identified at inclusion. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured according to usual practice by physicians at baseline, 3 months, and 6 months. Total cardiovascular risk was also assessed at inclusion, using baseline BP measurements in conjunction with information on risk factors, subclinical organ damage, and clinical disease (i.e. diabetes mellitus and established cardiovascular or renal disease). 13 The time and reason for treatment discontinuation and adverse events were recorded. Patient-reported compliance was assessed at 3 and 6 months using a five-point scale: (1) treatment taken daily since the previous visit; (2) taken often (only forgotten once or twice); (3) taken half the time; (4) not taken most of the time; and (5) never taken.
The primary endpoint was BP reduction over 6 months. BP control after 6 months was a secondary endpoint; it should be noted that as the original protocol was accepted prior to the publication of the 2013 European Society of Hypertension (ESH) guidelines, it initially included targets based on the 2007 ESH guidelines.6,13 However, BP control was eventually calculated based on the 2013 recommendations for better applicability with current medical practice. BP reduction according to baseline severity of hypertension and degree of added cardiovascular risk was also a secondary endpoint. BP reduction and control were assessed in the whole population and in two subgroups, one with high/very high added cardiovascular risk and another with diabetes mellitus (subgroup target BP <130/80 mm Hg). Safety and tolerability, and patient compliance, were also evaluated.
Statistical analysis
All study parameters were presented using descriptive statistics. For continuous variables (BP, age, etc.), mean value ± standard deviation were used; for ordered variables (e.g. patient compliance scale), mean value ± standard deviation, together with the median and frequency table was used; and for categorical/nominal variables (e.g. sex), numbers and percentages were used. Significance level for all tests (p-value) was set at p < 0.05. Patients in the per protocol set had a record of BP measurements at all three visits and good compliance (scored 1 or 2 at both post-baseline visits). To determine sample size, the bilateral 95% confidence interval of SBP was calculated as 1.5 mm Hg, i.e. ≈1% of expected mean target SBP (135 mm Hg; midway point of the range 130–139 mm Hg), based on an SBP standard deviation of ≈30 mm Hg after 3 or 6 months’ treatment with perindopril/amlodipine and on a sample size of 2000 patients. 15 Assuming the withdrawal of 15% to 20% of patients, final sample size was calculated as 2400 patients.
Repeated measures analysis of variance compared the values of SBP and DBP, between the three visits, while a t-test was performed on each pair of visits. A Friedman test was used to investigate change in BP classification over time. Multiple linear regression (stepwise method) was used to analyze the relation of cardiovascular risk stratification (“very high added risk” reference level) and first visit SBP values with SBP differences between the first and third visit (dependent variable). Statistically significant relationships were retested using analysis of variance for cardiovascular risk stratification and Pearson’s correlation coefficient for first visit SBP values. The same analyses were carried out for DBP. A Scheffe test was applied for pairwise comparisons between strata. The R statistical software suite (version 3) was used to perform statistical analysis.
Results
Of 2300 hypertensive patients in the study, 53.3% were male. Age at baseline was 64.3±11.3 years and mean body mass index was 28.5±4.2 kg/m2 (Table 1). Further baseline characteristics are presented in Table 1. Mean SBP and DBP were 157.0±15.4 and 91.5±10.1 mm Hg, respectively. Nearly 8 in 10 patients had either mild (grade 1) or moderate (grade 2) hypertension. Many patients (n = 1988; 86.4%) had moderate or greater added cardiovascular risk, and about half (n = 1047; 45.5%) had high/very high added cardiovascular risk (Table 1). Just over half (n = 1155; 50.2%) had dyslipidemia, and lipid-lowering therapy was used by 37.8% (n = 870). Most patients (97%; 2231/2300) completed the study (per protocol set).
Baseline characteristics, cardiovascular parameters, factors influencing prognosis in hypertension, and concomitant medication (n = 2300).
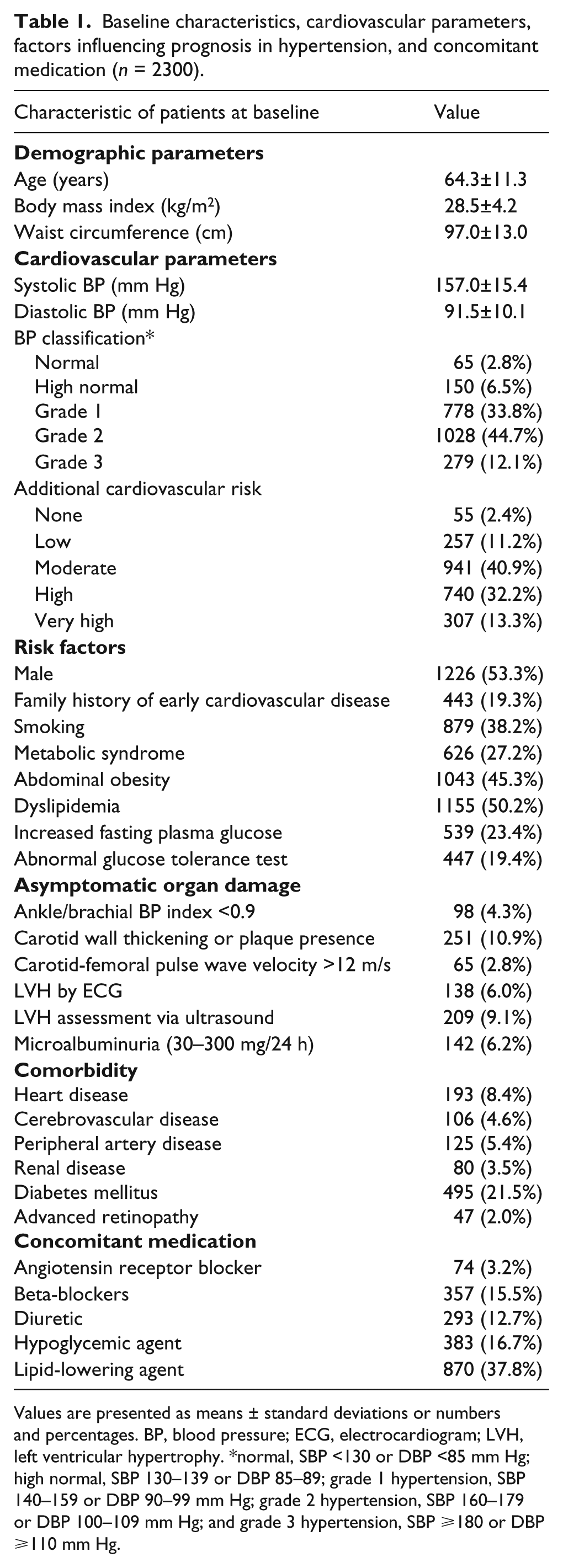
Values are presented as means ± standard deviations or numbers and percentages. BP, blood pressure; ECG, electrocardiogram; LVH, left ventricular hypertrophy. *normal, SBP <130 or DBP <85 mm Hg; high normal, SBP 130–139 or DBP 85–89; grade 1 hypertension, SBP 140–159 or DBP 90–99 mm Hg; grade 2 hypertension, SBP 160–179 or DBP 100–109 mm Hg; and grade 3 hypertension, SBP ⩾180 or DBP ⩾110 mm Hg.
SBP and DBP of patients who received perindopril/amlodipine decreased significantly versus baseline after 3 months and 6 months in the per protocol set (p < 0.001) (Figure 1). SBP decreased by 23.0 mm Hg to 134.0±10.1 mm Hg after 3 months and by 28.0 mm Hg to 129.0±7.9 mm Hg after 6 months. DBP decreased by 9.9 mm Hg to 81.6 ±7.5 mm Hg after 3 months and by 12.7 mm Hg to 78.8±6.7 mm Hg after 6 months (Figure 1). BP control (<140/90 mm Hg) was achieved in 84.8% (1893/2231) of the per protocol set.
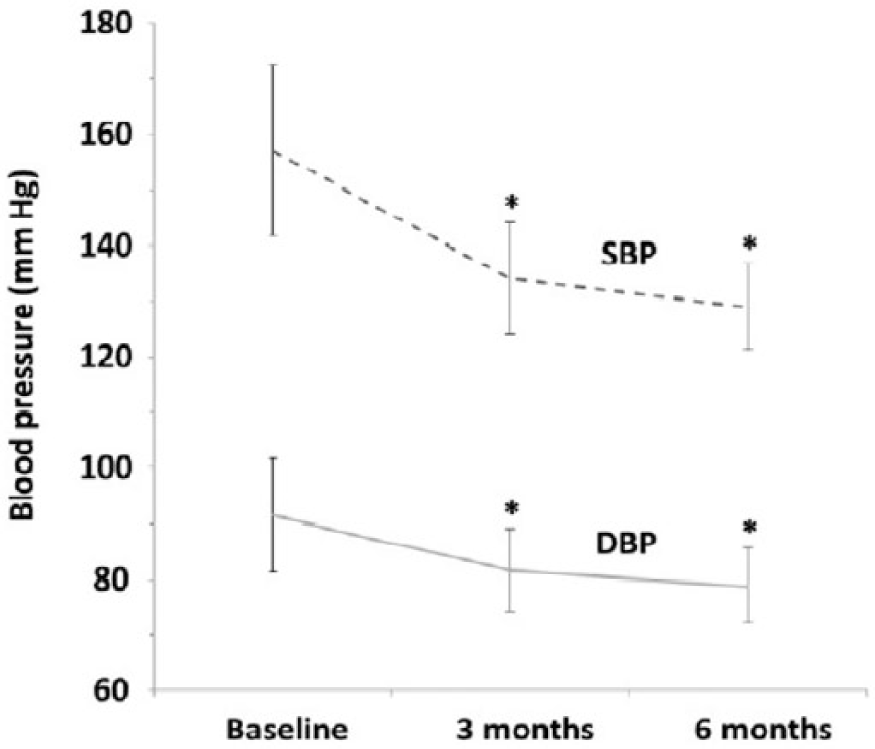
Mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) reductions after 3 and 6 months with fixed-dose combination perindopril/amlodipine in the per protocol set (n = 2231).
In 1009 patients in the per protocol set at high/very high added cardiovascular risk, mean SBP values decreased from 159.0±17.0 to 136.0±10.7 mm Hg after 3 months and to 130.4±7.8 mm Hg after 6 months (p < 0.001), while mean DBP values decreased from 91.9±10.8 to 82.0±7.8 mm Hg after 3 months and to 79.0±6.8 mm Hg after 6 months (p < 0.001). After 6 months, 83.1% of patients at high/very high added cardiovascular risk had controlled BP.
In 472 patients in the per protocol set with diabetes mellitus, the decrease in BP was similar: SBP fell from 156.0±17.0 to 134.5±11.4 mm Hg after 3 months and to 129.1±8.2 mm Hg after 6 months; and DBP fell from 91.2±11.1 to 81.8±8.3 mm Hg after 3 months and to 78.9±7.4 mm Hg after 6 months (p < 0.001). After 6 months, 67.6% of patients with type 2 diabetes had controlled BP (<140/85 mm Hg).
Patients with more severe hypertension at baseline had greater reductions in SBP and DBP after 6 months, which was confirmed by Pearson’s correlation coefficient (−0.863 for SBP and −0.756 for DBP; both p < 0.001) and analysis of variance (F-test for SBP and DBP; both p < 0.001) (Figure 2(a)). Further examination showed that patients with higher added cardiovascular risk at baseline had greater reductions in SBP and DBP after 6 months (F-test for SBP and DBP; both p < 0.001) (Figure 2(b)).

Blood pressure (BP) reduction with fixed-dose combination perindopril/amlodipine in the per protocol set according to severity of hypertension (A) and added cardiovascular (CV) risk stratification (B) at baseline (n = 2231).
Fifty-two patients (2.3%) prematurely discontinued treatment. Of these 52, 27 patients (1.2%) reported adverse events/reactions leading to treatment discontinuation: 21 patients reported minor adverse events (e.g. cough, ankle or lower limb edema), while 6 patients reported serious adverse events (one case (face edema) was suspected of being drug-related). Eighteen patients discontinued treatment because they did not attend scheduled visits and 8 due to other reasons.
Most patients (n = 2233; 97.1%) took perindopril/amlodipine “every day” or “quite often.” The dosage of perindopril/amlodipine did not change for the majority of patients (n = 1929; 83.9%). The perindopril/amlodipine fixed-dose combination dosages on each study visit are presented in Table 2.
Perindopril/amlodipine fixed combination dosage on each study visit.

P/A: perindopril/amlodipine fixed combination dosage.
Discussion
Real-life treatment of patients with essential hypertension and a wide range of risk (from low to high risk) using a fixed-dose combination of perindopril/amlodipine resulted in a significant reduction in BP after 3 and 6 months versus baseline. Hypertension was controlled in 85% of these patients. Perindopril/amlodipine was also effective at reducing and controlling BP in subgroups of hypertensive patients with high/very high added cardiovascular risk or diabetes mellitus. The greater the baseline severity of hypertension or degree of added cardiovascular risk, the greater the BP reduction. Treatment was safe and well-tolerated, with few reports of treatment discontinuation or adverse events.
Cardiovascular disease is one of the leading causes of morbidity and mortality worldwide, for which hypertension represents a major modifiable risk factor. 16 Few hypertensive patients (23%) present with elevated BP alone: 17 the majority present with multiple risk factors, 17 and current guidelines emphasize the importance of total cardiovascular risk assessment. 6 This was confirmed in our study, with the finding that about half of hypertensive patients in Greece had high or very high added cardiovascular risk.
The decrease of BP with fixed-dose perindopril/amlodipine was comparable to that observed in PEARL (PErindopril/Amlodipine Reducing blood pressure Level), 18 a 3-month prospective, observational trial in grade 1 or 2 hypertensive patients (mean age 61 years) with similar mean BP at baseline (158/92 mm Hg). In PEARL, perindopril/amlodipine decreased office BP by 26/12 mm Hg, 18 compared with 23/10 mm Hg after 3 months in our study. 6 PEARL also confirmed BP reduction with perindopril/amlodipine lasts a full 24 hours.
Current guidelines recommend the use of antihypertensive combination treatment over monotherapy when faster BP response, better BP control in patients with higher initial BP, and better patient adherence are needed. 6 Antihypertensive monotherapy decreases BP levels to a lesser degree, and patients on monotherapy have higher drop-out rates than those on combination therapy.6,11,19 A further advantage of antihypertensive combination therapy is the potential for pharmacological synergy between different classes of agents, which may lead to a reduction in the incidence of side-effects and provide a wider range of positive clinical effects than a single agent. 20
Early use of fixed-dose perindopril/amlodipine in the treatment of hypertensive patients appeared beneficial, as there was significant BP reduction in over half the population with low to moderate risk and treatment was well tolerated. The baseline-dependent BP reduction with perindopril/amlodipine may also allow this treatment to be administered safely in patients with low grade hypertension (patients with lower baseline SBP and DBP had lower reductions in SBP and DBP, and vice versa).
We also observed BP reduction and BP control in patients with high/very high added cardiovascular risk, for whom rapid cardiovascular risk reduction is essential, as well as in patients with diabetes mellitus, for whom BP control is usually harder to achieve. 6 Both SBP and DBP were reduced to a greater extent with perindopril/amlodipine in patients with more severe hypertension at baseline, and this was also the case for those at greater added cardiovascular risk at baseline. This more pronounced reduction in BP is especially beneficial in high-risk patients, since rapid achievement of therapeutic targets is reflected by a reduction in the risk of cardiovascular events.6,21 In ASCOT-BPLA (Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm), a combination of amlodipine ± perindopril reduced all-cause mortality by 11% and cardiovascular events and procedures by 16% versus atenolol ± bendroflumethiazide. 22
Despite the ready availability of effective therapies, hypertension remains poorly controlled. 8 The complexity of multidrug antihypertensive regimens, an under-appreciation of the long-term risks associated with hypertension, and a lack of compliance and adherence probably represent the main reasons. 6 The rapid achievement of target BP levels, as well as the low incidence of adverse events and the simplified antihypertensive drug regimen, may explain the levels of compliance observed in our study: nearly all reported taking treatment “every day” or “quite often”. In addition, indicative of the effectiveness and tolerability of treatment is the high percentage (83.9%; n = 1929) of patients who remained on the same dosage throughout the study. Half (51.3%) of these were initiated on the lowest dose (5/5 mg) of perindopril/amlodipine. Over a third (38.5%) received the maximum dose of perindopril (here 10 mg), the dose at which the greatest reduction in cardiovascular events is observed. 23
As this was an observational study, the efficacy and safety of perindopril/amlodipine were not assessed versus a comparator and there was no randomization. Nevertheless, participating patients and practices are representative of the daily clinical management of hypertensive patients in Greece, and our study included a sizeable population. Registry observations have been shown to be similar to those for general clinical practice.24,25 Although 2007 ESH/ESC guidelines were originally used to determine BP target levels, data have been presented to allow analysis and interpretation according to the latest 2013 ESH/ESC guidelines.6,12,13
Conclusions
Fixed-dose combination perindopril/amlodipine safely reduced and controlled elevated BP in patients with essential hypertension in a real-life clinical setting, with good patient compliance. The degree of BP reduction observed was associated with the severity of hypertension or with total cardiovascular risk at baseline. About half of hypertensive patients in Greece appear to have high or very high added cardiovascular risk.
Footnotes
Acknowledgements
Those who contributed to the “Prospective non-interventional study for the effectiveness of perindopril/amlodipine fixed dose combination and the compliance of hypertensive patients after a 6-month treatment” investigation are gratefully acknowledged.
Conflict of interest
A Manolis has received honoraria for lecturing and a research grand from Servier Hellas.
I Zarifis has received honoraria for an advisory board from Servier Hellas.
K Tsioufis has received honoraria for lecturing and an advisory board from Servier Hellas.
Two co-authors, V Grammatikou and M Kallistratos, are employed by the Medical Department of Servier Hellas.
Funding
This work was supported by Servier Hellas.