
Abstract
Background:
Previous studies have shown that angiotensin II AT1 receptor gene (AT1R) polymorphisms are associated with the risk for hypertension. However, the results remain controversial. In the present study, we performed a meta-analysis to systematically summarize the association between AT1R genetic polymorphisms and the risk for hypertension.
Methods:
We searched the literature in PubMed, EMBASE, ISI Web of Science, Wanfang, and Chinese National Knowledge Infrastructure databases (CNKI) to find case-control studies on the associations of AT1R genetic polymorphisms with the risk for hypertension. The meta-analysis was performed by using RevMan 5.0 software. The association of hypertension risk with AT1R genetic polymorphism was estimated by pooled odds ratios (ORs) and 95% confidence intervals (95% CIs).
Results:
Fifty-six studies involving 28,952 subjects were included in the present meta-analysis. Our results suggest that the polymorphism (A1166C) of AT1R gene is associated with a statistically increased hypertension risk, not only in Asian populations but also in Caucasian populations. We did not find any association in African populations.
Conclusions:
This meta-analysis suggests that A1166C polymorphism in the AT1R gene is associated with the risk of hypertension in Asian and Caucasian populations.
Introduction
Hypertension is a major public health problem throughout the world. 1 However, the pathogenesis of hypertension remains unclear. It is considered that hypertension is a complex disease resulting from the interaction between genetic polymorphisms and environmental factors. 2 Recently, many genes have been identified as candidates for contribution to hypertension. 3 Of these, the angiotensin II AT1 receptor (AT1R) plays an important role in normal blood pressure regulation and in the pathophysiological progression of hypertension.4 –6 The polymorphisms of the AT1R gene have been reported to be associated with the pathogenesis of hypertension.7–9 In particular, a single nucleotide polymorphism (SNP), A1166C, is the most studied variant being located in the 3′ untranslated region of the AT1R gene. 10
Several studies have indicated that A1166C polymorphism is associated with hypertension.11,12 However, this association has not been confirmed in other reports.13,14 In 2010, Wang et al. conducted a meta-analysis assessing the association of the AT1R gene A1166C polymorphism with hypertension in the Chinese population; this indicated that the AT1R C allele carriers have a higher risk for hypertension. 15 Niu and Qi also performed a meta-analysis and found that the AT1R C allele conferred an increased risk of hypertension. 16 However, in these two meta-analyses, the number of the included studies was rather small. In recent years, many new large-sample-size case-control studies have been conducted.11–14 Therefore, to further assess the relation between AT1R gene polymorphism and hypertension, we performed a carefully designed meta-analysis including 56 studies involving 28,952 subjects.
Methods
Selection of studies
We conducted a systematic computerized literature search for studies published before 1 December 2014. We searched the literature in PubMed, EMBASE, ISI Web of Science, Wanfang database in China, and Chinese National Knowledge Infrastructure (CNKI) database with the following search terms: “hypertension” and “angiotensin II type 1 receptor” or “AT1R” and “polymorphism” or “SNP”, or “mutation” or “variant”, by two independent investigators. The publication date and language were not restricted in the present study. All studies which met to the inclusion criteria were retrieved for further examination and data extraction.
Selection criteria
Studies satisfying the following criteria were included: 1) reported the relation between the AT1R genetic polymorphism and susceptibility to hypertension; 2) definition of hypertension as systolic (or diastolic) blood pressure ⩾140 mmHg (or 90 mmHg) or treatment with antihypertensive medication; 3) in a case-control using either a hospital-based or a population-based design; 4) detailed genotype data were provided for the calculation of odds ratio (OR) and 95% confidence interval (95% CI). Studies that focused on juvenile hypertension or secondary forms of hypertension such as pregnancy-induced hypertension were excluded from this study.
Data extraction
Two researchers performed the data extraction independently. The following information from all eligible studies were obtained: first author’s last name, year of publication, ethnicity of the population studied, study design, number of subjects in each category, baseline characteristics of the study population, and the number of persons with different genotypes in cases and controls and the genotyping methods.
Statistical analysis
The RevMan 5.0 software was employed for the present meta-analysis. The Hardy–Weinberg equilibrium was estimated by the χ2-test. We performed analyses under the dominant model (CC+AC vs. AA), recessive model (CC vs. AC+AA), and additive model (C vs. A). We utilized Q-test and I2 test to examine the heterogeneity between each study. By heterogeneity test, if I2 < 50%, we select the fixed effect model to merge OR. If I2 > 50%, we selected the random effect model to merge OR. Sensitivity analysis and publication bias analysis were tested using RevMan 5.0 statistical software. The statistical significance of the pooled OR was determined with the Z test, and a p value of <0.05 was considered significant.
Results
Baseline characteristics
A total of 447 articles concerning the AT1R A1166C polymorphism and hypertension were retrieved after first search in PubMed, EMBASE, ISI Web of Science, Wanfang in China, and CNKI databases. As shown in Figure 1, after excluding duplicated publications or those that did not meet the inclusion criteria, we included 56 case-control studies for the final analysis.11–14,17–68 The characteristics of each study are summarized in Table 1. These 56 studies involved 28,952 subjects (14,708 hypertensive patients and 14,290 healthy control subjects). There were 39 studies carried out in Asian populations,19–22,24–53,57,58,61,63,65 while 15 studies were performed in Caucasian populations.11–13,18,23,54–56,59,60,62,64,66–68 Only two studies involved an African population.17,18

Flow diagram of study identification.
Characteristics of participants.

Meta-analysis
As shown in Table 2. we found the polymorphism (A1166C) of AT1R gene was associated with a statistically increased hypertension risk ((AC+CC) vs. AA: OR = 1.44 (95% CI: 1.24–1.66, p < 0.001); (AA+AC) vs. CC: OR = 0.61 (95% CI: 0.46–0.81, p < 0.001); C allele vs. A allele: OR = 1.35 (95% CI: 1.18–1.55, p < 0.001)) in the total population (Figures 2 to 4). In the subgroup analyses, the association was also significant among studies using Asian populations in all genetic models ((AC+CC) vs. AA: OR = 1.41 (95% CI: 1.19–1.66, p < 0.001; (AA+AC) vs. CC: OR = 0.50 (95% CI: 0.38–0.65, p < 0.001); C allele vs. A allele: OR= 1.40 (95% CI: 1.21–1.63, p < 0.001)). However, we only found an association in a dominant model ((AC+CC) vs. AA: OR = 1.37 (95% CI: 0.99–1.89, p = 0.05)), but not in a recessive model ((AA+AC) vs. CC: OR = 0.81 (95% CI: 0.53–1.22, p = 0.32)) or an additive model (C allele vs. A allele: OR = 1.09 (95% CI: 0.79–1.51, p = 0.58)) in Caucasian populations. We did not found any association in African populations ((AC+CC) vs. AA: OR = 2.53 (95% CI: 0.66–9.70, p = 0.18); C allele vs. A allele: OR = 2.16 (95% CI: 0.93–5.01, p = 0.18)).
Meta-analysis of A1166C polymorphism of the AT1R gene and hypertension.

OR: odds ratio, CI: confidence interval.
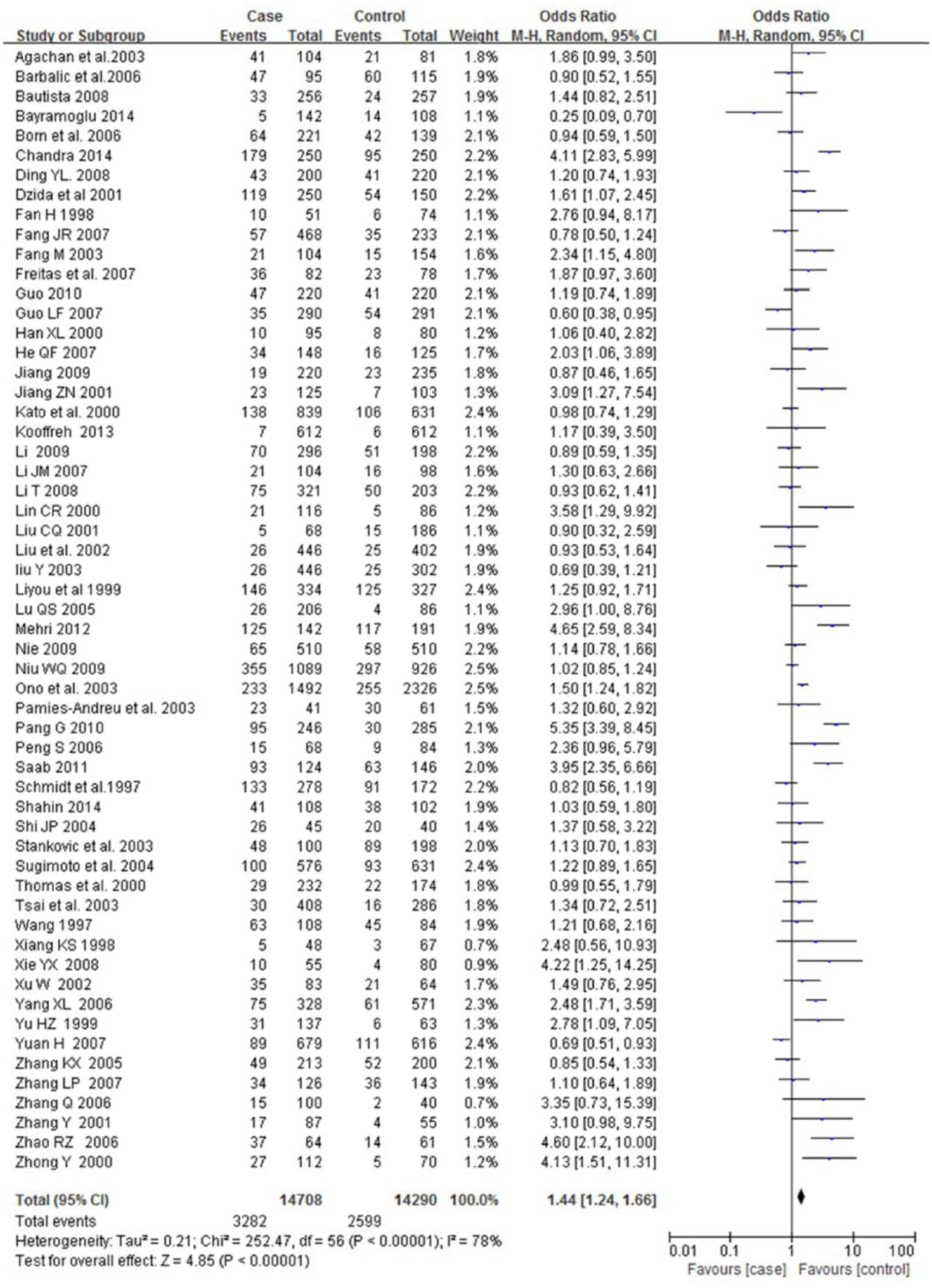
Forest plot of hypertension associated with AT1R genetic polymorphism in a dominant model ((AC+CC) vs. AA). The squares and horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95% CI.
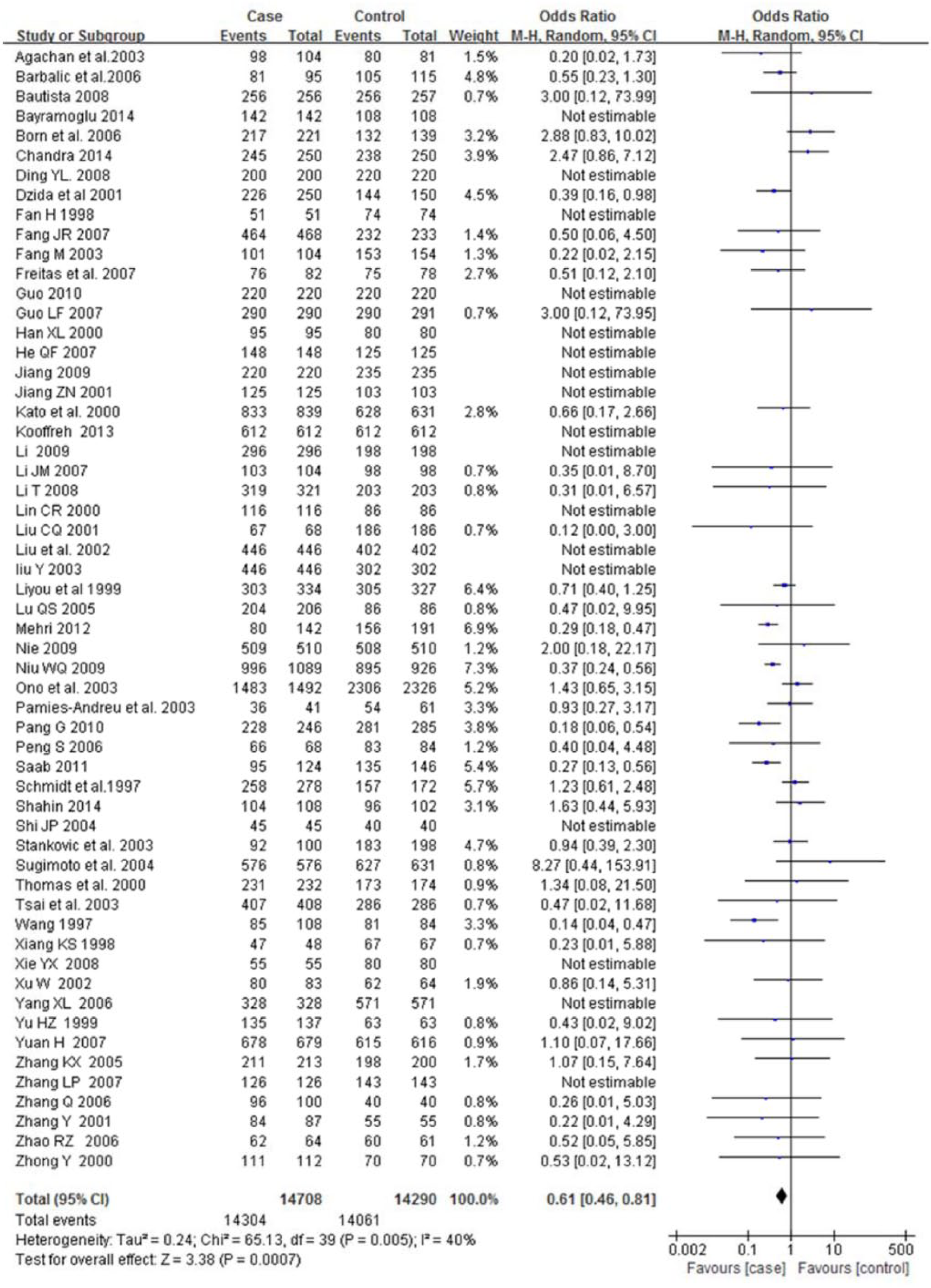
Forest plot of hypertension associated with AT1R genetic polymorphism in a recessive model ((AA+AC) vs. CC). The squares and horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95% CI.

Forest plot of hypertension associated with AT1R genetic polymorphism in an additive model (C vs. A). The squares and horizontal lines correspond to the study-specific OR and 95% CI, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95% CI.
Publication bias
The publication bias test of the literature was conducted using a funnel plot and Egger’s test. Symmetrical funnel plots were obtained in the SNP tested in all of the models, which displayed no publication bias (Figure 5). Egger’s test further confirmed the absence of publication bias in this meta-analysis (all p > 0.05, data not shown).

Funnel plot for publication bias test. Each circle denotes an independent study for the indicated association.
Sensitivity analysis
We removed one single study from the overall pooled analysis each time to check the influence of the removed data set to the overall ORs. The pooled ORs and 95% CIs were not significantly altered when any part of the study was omitted, which indicated that any single study had little impact on the overall ORs and the results of this meta-analysis were stable.
Discussion
The present study aimed to explore the association of the AT1R gene A1166C polymorphism with hypertension among a total of 28,952 subjects via a meta-analysis. We demonstrated that the AT1R gene 1166C allele carriers have higher risk for hypertension in Asian and Caucasian population, but not in African population.
Meta-analysis is a powerful tool for summarizing results from different studies by producing a single evaluation of the major effect. Genetic association studies have a tendency to lack the power to detect a statistically significant association with complex diseases, especially studies with small sample sizes. To achieve a satisfactory power, meta-analysis of multiple studies clearly has a role in offering an association study with such potentials. In the present study, we collected 56 case-control studies involving 28,952 subjects in this meta-analysis to clarify the relation between AT1R genetic polymorphism and hypertension. We found a significant association between C allele and the increased risk of essential hypertension. In the stratified analysis, we divided these studies into different subgroups by race of the participants. Significant association between hypertension and the A1166C polymorphism was observed in both Asian and Caucasian populations, but not in African populations. Our results were in line with a previous meta-analysis in a Chinese population. However, the mechanism responsible for the association of hypertension risk with A1166C polymorphism remains unclear. A1166C polymorphism is in a non-coding region of AT1R gene, and therefore the amino acid sequence of the AT1 receptor is not altered. The lack of a functional role of the A1166C polymorphism makes this SNP somewhat unappealing as a “true” influence of hypertension susceptibility. However, the A1166C polymorphism might affect mRNA stability and transcription, or alternatively be in linkage disequilibrium with other functional polymorphisms. Therefore, the functional study of this variant was expected in the future.
Furthermore, we did not find the publication bias. Sensitivity analysis also showed that omission of any single study did not have significant impact on the combined ORs. This made the results of this meta-study more reliable to some extent. However, we found significant heterogeneity among all the included studies. This heterogeneity may result from study design of included studies. Two kinds control sources-hospital-based controls and population-based controls were used in the studies. The hospital-based controls might have selection biases and might not be representative of the general population. In addition, three races including Asian, Caucasian, and African populations were involved in the present study. This fact may be another source of heterogeneity.
There were also some limitations in this meta-analysis. Firstly, some clinical factors such as age, sex may affect the hypertension risk. In the present study, we did not adjust these confounders. Determining whether or not these factors influence the results of this meta-analysis would need further investigation. Secondly, this meta-analysis only focused on papers published in the English and Chinese language. Thirdly, the cross-sectional nature of our included studies precludes comments on causality. Finally, in this study, we only focused on the AT1R gene A1166 C polymorphism and did not evaluate other polymorphisms in the AT1R gene, leading to the possibility that the potential role of the A1166 C polymorphism is diluted or masked by other gene–gene or gene–environment interactions.
Conclusion
In conclusion, this meta-analysis clarified the association of A1166C polymorphism in AT1R gene of the risk of hypertension. The presence of AT1R gene 1166C allele is associated with an increased risk of hypertension in Asian and Caucasian populations.
Footnotes
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by Shandong Province medical and health science and technology development projects (grant number 2013WS0107).