
Abstract
Introduction:
The role of angiotensin (Ang) (1–7) on the vasoconstrictor effect induced by angiotensins could be different in the presence of an ACE inhibitor or an ARB because Ang II is formed through several pathways. Therefore, the role of Ang (1–7) in Ang I and Ang II contraction was evaluated in aortas from Wistar rats after 48-hour coronary occlusion treated with captopril or losartan.
Methods:
Concentration-response curves to Ang I or Ang II were conducted in the absence or presence of Ang (1–7) and A779: a) sham group; b) 48-hour coronary occlusion; c) treated with captopril or d) losartan (3.1 mg/kg, i.m.).
Results:
Captopril caused a significant increase in the contractile effect of Ang I and Ang II, while losartan reduced it. The presence of Ang (1–7) in the captopril group showed a reduction of the contraction compared to the sham group, while the treatment with losartan did not show a significant difference. Ang (1–7) presents effects different from Ang I or Ang II.
Conclusion:
Ang (1–7) showed a modulatory role, suggesting Ang I did as well after treatment with an ACE inhibitor but not with an AT1 receptor antagonist.
Introduction
AT1 receptor blockers (ARBs) and angiotensin-converting enzyme inhibitors (ACEis) have been shown to improve the survival of patients both in the acute and long-term phase of myocardial infarction (MI). 1 ACEis have shown to improve hemodynamic parameters and the functional capacity in patients who have chronic infarct,2,3 but when the renin angiotensin system (RAS) is active the recommended doses of ACEi do not inhibit the enzyme completely. 4 In case of the antagonist of the AT1 receptors, although angiotensin II (Ang II) may be formed by different routes, the benefits are caused by avoiding the Ang II effect of interacting with AT1 receptors, a process that ACEi does not. 5 ACE contributes to the formation of Ang II. 6 The effect of Ang II depends on its biosynthesis from Ang I through the catalysis of circulating and endothelial ACE. 2 Inhibition of ACE also affects the formation of other components of the RAS. 7 It has been reported that ACEis are directly related to Ang (1–7) because these drugs prevent the metabolism of Ang (1–7) on the inactive peptide Ang (1–5) 8 and inhibits the metabolism of bradykinin, which is a vasodilator potentiated by Ang (1–7). 9 Ang (1–7) has central and peripheral actions. 10 For example, it generates vasodilation of the feline mesenteric artery, and dog and pig coronary artery. Also, the heptapeptide potentiates the vasodilator effect of bradykinin in the conscious rat. 11 Additionally, it has been described that Ang (1–7) plasma levels are increased in rats, dogs and humans treated with captopril or losartan. 12 To date it is unknown whether Ang (1–7) has a role in the vascular contractility of Ang I and Ang II in the aorta of infarcted Wistar rats previously treated with an ACEi or ARB. Therefore, the purpose of this study was to evaluate the role of the Ang (1–7) on the vasoconstrictor effect induced by Ang I or Ang II in aorta from rats treated with an ACE inhibitor or an Ang antagonist after 48 hours of coronary occlusion.
Methods
Animals
Wistar male rats (300–400 g) were used and obtained from CINVESTAV-IPN (Sede Sur). Rats were placed in individual boxes with light-dark cycles of 12 × 12 hours with free access to food and water. Rats were grouped as follows: a) sham group with vehicle; b) 48-hour coronary occlusion with vehicle; c) treated with captopril; d) treated with losartan. Animals were euthanized 48 hours after coronary occlusion, and aortic rings of all experimental groups were incubated in the absence or presence of Ang (1–7) 10−5 M 13 and/or A779 10−5 M. Captopril or losartan were administered at a dose of 3.1 mg/kg intramuscularly (i.m.) 30 minutes before the occlusion and 24 hours after. The experimental protocols were designed according to the Federal Regulation for Animals Experimentation and Care (SAGARPA NOM-062ZOO-1999, Mexico.).
Reagents
Captopril, losartan, Ang I, Ang II, Ang (1–7), ketamine and xylaxine were obtained from Sigma-Aldrich Inc. Physiological saline solution (0.1 ml) was administered as vehicle. Ang I, Ang II and Ang (1–7) were dissolved in Krebs-Heinselet solution.
Induction of MI
To induce MI, the left anterior descending coronary artery was ligated between the pulmonary outflow tract and the left atrium using 5-0 silk suture under aseptic conditions in anesthetized rats (ketamine HCl/xylazine, 80/12 mg/kg intraperitoneally (i.p.); 150 mg/kg of ampicillin subcutaneously (s.c.)). Onset of ventricular arrhythmias and the presence of myocardial blanching distal to the occlusion confirmed successful ligation of the artery. Organs were returned to the thorax cavity and sutured using 2-0 silk suture. Sham-operated animals were intervened in the same manner but suture was not placed around the coronary artery. The infarcted area was determined using blue tetrazolium, which stains healthy tissue blue. The staining made it possible to measure the infarcted area by planimetry.
Isolated organ bath experiments
The thoracic aorta was excised and placed in fresh Krebs-Henseleit solution containing 118 mM NaCl, 4.7 mM KCl, 1.2 mM KH2PO4, 1.2 mM MgSO4·7H2O, 2.5 mM CaCl2·2H2O, 25 mM NaHCO3, 11.7 mM dextrose, and 0.026 mM calcium disodium ethylenediaminetetraacetic acid (EDTA) aerated with 95% O2/5% CO2 at 37°C. The aortas were cleaned of surrounding tissue and cut into rings that were 4–5 mm long. The aortic rings were mounted in 10 ml chamber tissue baths filled with Krebs-Henseleit solution at 37°C (pH 7.4) and they were continuously aerated with 95% O2/5% CO2. To record the semi-isometric force development, the rings were suspended on two wire hooks (NUBRYTE wire) and fixed to the bottom of the chamber and a force transducer (BIOPAC TSD105) connected to a BIOPAC MP100WSW system (from BIOPAC Systems Inc, Santa Barbara, CA, USA). The ring segments were adjusted to a tension of 3 g. The integrity of the endothelium was evaluated by the vasodilator response after the administration of 10−5 M acetylcholine to aortic rings that had been pre-treated with 10−6 M phenylephrine.
The vasoconstrictor effect of Ang I and Ang II
Concentration-response curves to Ang I (10−12 to 10−6 M) and Ang II (10−12 to 10−6 M) in the absence or presence of Ang (1–7) 10−5 M 10 minutes before generating the curves 9 were obtained using rat aortic rings with endothelium from the sham group and the infarcted previously treated with the vehicle, losartan or captopril (1 mg/kg i.m.) 30 minutes before occlusion was made and 24 hours later.
Ang (1–7) antagonism
Concentration-response curves to Ang I (10−12 to 10−6 M) and Ang II (10−12 to 10−6 M) in the absence or presence of Ang (1–7) 10−5 M and A779 10−6 M 10 minutes before generating the curves 10 were obtained using rat aortic rings with endothelium from the sham group and the infarcted previously treated with the vehicle, losartan or captopril (1 mg/kg i.m.) 30 minutes before occlusion was made and 24 hours later.
Calculation of maximal response and ED50
The calculation of both parameters was made by WinNonlin professional 2.1 software from raw data of each curve (n = 9) for all experimental groups.
Statistical analysis
The concentration-response graphs were developed with the GraphPadPrism5 software. To compare the infarcted area, a one-way analysis of variance (ANOVA) was carried out. The data obtained in the concentration-response curves were analyzed through a two-way ANOVA, establishing a value less than p < 0.05 to report a significant difference.
Results
Determination of the percentage of the infarcted area
Table 1 shows the results of the infarcted area 48 hours after the coronary occlusion was performed in all experimental groups. The magnitude of the infarcted area was significantly less in case of that observed with captopril or losartan groups (p < 0.05).
Percentage of infarcted area obtained through the technique of blue tetrazolium in hearts from rats treated with captopril or losartan at 1 mg/kg, 48 hours after coronary occlusion.

Each value represents the mean ± SEM of nine hearts. ap < 0.05 vs IM. One-way analysis of variance (ANOVA) was performed. MI: myocardial infarction.
Effect of Ang (1–7) on the contraction induced by Ang I and Ang II after captopril or losartan treatments.
Figure 1 shows the effect of Ang (1–7) on the concentration-response curves of Ang I or Ang II in the aortic rings from rats treated with captopril or losartan (both at 3.1 mg/kg i.m.). The figure shows that both angiotensins induced a concentration-dependent contraction and, compared with the sham group, the contractile effect in the aortic rings with 48-hour coronary occlusion shows no significant difference, while those obtained under captopril treatment provoked a significant increase in the contractility (p < 0.01 in both angiotensins). Such an increase is related to an augment in the maximal effect (Emax) value (Table 2, p < 0.05) but not in the EC50 values (Table 3). The presence of Ang (1-7) in the aortic rings from rats treated with captopril significantly reduced the Ang II contractile effect to control values but not in the case of Ang I (Figure 1(a) and (b)); such a reduction is related to an Emax value reduction (Table 2). The Ang (1–7) induced an increased PD2 value (Table 3). On the other hand, the treatment with losartan provoked a significant reduction of the contraction and Emax value and an increase in the EC50 generated by Ang I and Ang II compared with the sham group (p < 0.05 for all cases). However, the incubation with Ang (1–7) did not show a significant change (Figure 1(c) and (d)). The presence of A779 and Ang (1–7) generated an increase in the vasoconstrictor effect of Ang II with both treatments. In the case of Ang I, the presence of A779 and Ang (1–7) showed a vasodilator effect with captopril treatment and no effect with treatment of an AT1 antagonist.
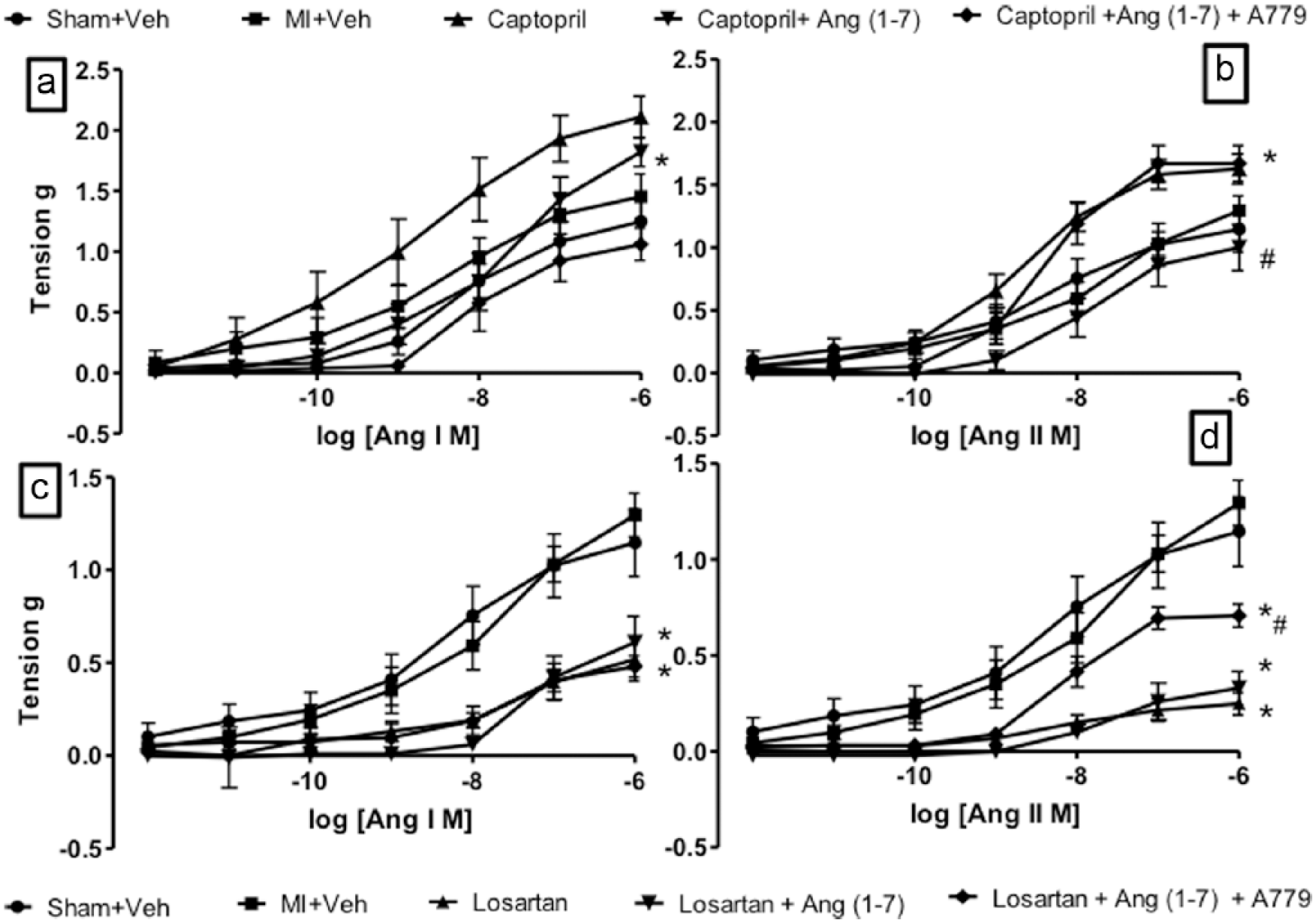
Concentration-response curves of Ang I and Ang II on aortic rings in the presence and absence of Ang (1–7) 10−5 mol/l and A779 10−6 mol/l from rats with 48 hours of coronary occlusion. The values are expressed as the mean ± SEM (n = 9). Figure (a) and (c) show that Ang (1–7) generates a modulator effect that leads to vasoconstriction related with captopril treatment and when losartan is administered it does not participate. Figure (b) and (d) show the presence of A779 confirms the participation of Ang (1–7) as vasodilator in the curves to Ang II. n = 9 for all experimental groups; *p < 0.05 vs control; #p < 0.05 vs treatment alone. Ang: angiotensin; MI: myocardial infarction; Veh: vehicle.
Maximal effect values of control, infarcted and treated groups.

Each value represents the mean ± SEM of nine aortas. ap < 0.05 vs sham; bp < 0.05 vs MI. cp < 0.05 vs treatment alone. One-way analysis of variance (ANOVA) was performed. MI: myocardial infarction; Ang: angiotensin.
EC50 mM values of control, infarcted and treated groups.

Each value represents the mean ± SEM of nine aortas. ap < 0.05 vs sham; bp < 0.05 vs MI; cp < 0.05 vs treatment alone. One-way analysis of variance (ANOVA) was performed. MI: myocardial infarction; Ang: angiotensin.
Discussion
The present work demonstrated that Ang (1–7) showed a biphasic role in the contractility induced by Ang I and Ang II in the aortic rings of infarcted rats treated with captopril or losartan. Although Ang (1–7) showed a modulatory effect present when the ACE is inhibited, possibly by a synergistic effect between the ACE inhibitor and Ang (1–7), in the case of losartan it does not. Also, we found that Ang I generates contractile effects different from Ang II with captopril or losartan treatments.
The result of the infarcted area by the treatment with captopril or losartan agrees with other studies14–16 that found that ACEis do not reduce the infarcted area; it participates in a process that limits the growth of the necrosed area due to the interaction of bradykinin with B2 receptors. This effect disappears with the administration of the antagonist of these receptors, HOE140. 15 Regarding the reduction caused by losartan, it was published that ARBs stop the ischemia process owing to the activation of AT2 receptors, bradykinin and prostaglandins in pigs (likewise, the effect is reversed by the administration of HOE140, indomethacin or PD123319, respectively).15–17 Even when the sham and MI groups showed no statistical differences to both angiotensins, the MI group generated bigger maximal effect values. This can be explained by the fact that the ability of nitric oxide (NO) to relax the vascular tone is altered during MI. This effect is the result of the reduction in the vascular response to NO, more than the reduction of the liberation of NO. 18 It is also known that during MI the levels of Ang II are increased with a vasoconstrictive effect, and that this is the most important determinant for the generation of cardiac remodeling. 19 As observed with captopril treatment, the contractile effect to both angiotensins increased, which shows that the drug does not inhibit the enzyme completely. 20 It also might exacerbate the activity of other enzymes present in the system we know of: Chymase, elastase and cathepsin G hydrolyze Ang I to Ang II5,21 and to act under hypoxic conditions as in MI or even in Ang (1–12) discovered by Nagata. 22 Therefore the gradual increased in the contraction is due to the hydrolysis of Ang I to become Ang II.
In contrast, the treatment with losartan generates a reduction in the contractile effects after 48 hours, suggesting it can be due to the blockade of the AT1 receptors. It has also been reported that AT1 receptor blockade stimulates the production of Ang (1–7) due to the increase in the concentration of Ang II (main precursor).23,24 It is important to mention that Ang (1–7) generated a reduction in the vasoconstriction of Ang II with the captopril treatment. Several researchers have suggested that Ang (1–7) might act as an endogenous ACEi and obtain a synergic effect with captopril,25,26 preventing bradykinin hydrolysis in addition that Ang (1–7) increases the vasodilating actions of it.8,9 Other results obtained from our laboratory support it because, when the rings were incubated with L-arginine methyl ester (L-NAME), the vasodilating effect were reversed, proving that this is due to the liberation of NO (not reported). None effect between losartan and Ang (1–7) was found as expected because other authors found that this interaction is associated with the increase in the bradykinin plasma levels.9,27,28 The presence of A779 also demonstrated that Ang (1–7) might be activated by another modulator that is up Ang II. We propose Ang I to be this modulator because depending on the presence of an ACE inhibitor or an ARB, it leads Ang (1–7) to generate vasoconstriction or vasodilation, possibly by the participation of unknown peptides or enzymes. Even though it is reported that Ang I has no effects by itself because it just provides the substrate for the vasoactive peptides Ang II and Ang (1–7), we might be mistaken.
Footnotes
Acknowledgements
The authors thank C. Ramon Martinez-Gomez and Juan Martinez-Parente from CINVESTAV Instituto Politecnico Nacional for the experimental animals.
Conflict of interest
None declared.
Funding
This work was supported by grants from DGAPA PAPIIT IN224310-3, IN 212213-3 UNAM CATEDRA CONS-26 FES Cuautitilán, Universidad Nacional Autónoma de México and the “Secretaría de Investigación y Posgrado” (SIP: