
Abstract
Introduction:
Adrenergic receptors (AR) play important roles in regulating lung function. However, there are few reports concerning AR expression and the protective effect of angiotensin II receptor blockers (ARB) on the lung in chronic heart failure (CHF). In this study, we aimed to investigate the protective effects of the ARB olmesartan on the lung in CHF.
Materials and methods:
Wistar rats were randomly divided into four groups: normal control, sham-operated rats, rats with CHF induced by ligating the left anterior descending coronary arteries, and rats with CHF treated with olmesartan (1 mg/kg) once daily for 8 weeks. Heart function, plasma renin activity (PRA) and angiotensin II (Ang II) levels, lung microscopic structure inspection and mRNA and protein expressions of α1A-, β1- and β2-AR in lung were tested.
Results:
Compared with the CHF group, PRA and Ang II levels were decreased while heart function and mRNA and protein expression of α1A-AR, β1-AR and β2-AR were up-regulated in the olmesartan group (p<0.05 or p<0.01). The inflammation and cell proliferation in CHF lung tissue were reduced in the olmesartan group.
Conclusion:
Olmesartan may play a beneficial role in protecting lung in CHF by up-regulating AR and decreasing levels of PRA and Ang II.
Introduction
Chronic heart failure (CHF) is characterized by activation of the sympathetic nervous system (SNS) and the renin–angiotensin system (RAS). It is already well known that there are interactions between the SNS and the RAS. A local RAS exists in the lung, and the pulmonary vascular endothelium is the predominant site for the angiotensin-converting enzyme which produces angiotensin II (Ang II). As a highly selective angiotensin II receptor blocker (ARB), olmesartan can not only block the combination between Ang II and the Ang II type 1 receptor (AT1R), but can also reduce the level of Ang II. 1 Olmesartan can reduce the activity of the RAS in CHF. In contrast, α1A-adrenoceptor (AR) and β2-AR are the main adrenergic receptor subtypes in the lung and play important roles in smooth muscle contraction and relaxation, as well as alveolar fluid clearance.2–6 The enhanced SNS activation in CHF can lead to down-regulation of cardiac β-AR expression. 7 However, there is little research to show that AR expression changes correspondingly under the condition of CHF, or whether olmesartan has an impact on lung AR through interactions between the RAS and the SNS. This study was designed to investigate the effect of olmesartan on heart function, levels of plasma renin activity (PRA) and Ang II, and α1A-AR, β1-AR and β2-AR expression in the lungs of rats with CHF.
Materials and methods
The study protocol was approved by the Committee on the Ethics of Animal Experiments of Capital Medical University (Permit Number: SCXK2007-004). All animal work was done according to the standards for laboratory animals established by the People’s Republic of China (GB14925-2001).
Animals
Adult male Wistar rats weighing 250–280 g were purchased from the Military Medical Science Academy of the Chinese People’s Liberation Army (Beijing, China). All the animals were barrier housed in a clean, air-conditioned animal room at the Beijing Anzhen Hospital (Beijing, China) with a 12-hour light–dark cycle, and were provided with standardized rat food and water.
Medicine and reagents
Olmesartan (20 mg/pill) was purchased from the Shanghai Sankyo Pharmaceutical, Co. Ltd. (Shanghai, China). Radioimmunoassay kits for PRA and Ang II were purchased from the Radioimmunoassay Institute Technology Development Center of the People’s Liberation Army General Hospital (Beijing, China). Trizol reagent was obtained from Invitrogen (Carlsbad, CA, USA) and the reverse transcription polymerase chain reaction kit (A5000) was obtained from Promega (Madison, WI, USA). All primers were synthesized by Invitrogen (Shanghai, China). The SYBR Green Real-Time PCR kits were purchased from Takara Bio (Shiga, Nagano, Japan). Rabbit anti-rat α1A-AR, β1-AR and β2-AR antibodies were purchased from Santa Cruz Biotechnology, Inc. (Santa Cruz, CA, USA).
Experiment protocol
The CHF model was established by ligation of the left anterior descending artery (LAD) as previously described. 8 In brief, Wistar rats were anesthetized by intra-abdominal injection of 1% phenobarbital sodium on a volume-cycled ventilator for small animals. A high frequency and low tidal volume ventilation method (VT 10 ml/kg, respiratory rate 80 per minute, I/E ratio 1:2) was used. The rats were orotracheally intubated and the ventilation sustained from the rats anesthetized to the surgery completed. The trachea cannulas were unplugged after the rats were awake. Anterior myocardial infarction was created by ligation of the LAD. During surgery, the presence of a myocardial infarction was assessed using a 12-lead electrocardiogram. Only rats with electrical evidence of myocardial infarction were kept in the study. Four weeks later, left ventricular ejection fraction (LVEF) was evaluated by echocardiography. Rats with LVEF ≤45% were used as CHF models. 9
Rats were randomly assigned to a normal control group (normal, n = 10), or a sham-operated group (sham, n = 10). The sham group was subjected to the same procedure except for the ligation of the LAD. Rats with CHF (LVEF ≤45%) were randomly assigned to one of two groups: a CHF saline control group (CHF, n = 10) or an olmesartan group (Olm, n = 10). Rats in the normal, sham and CHF groups received an intragastric administration of saline once daily; the Olm group received an intragastric administration of olmesartan (1 mg/kg in 2 ml) saline once daily. The olmesartan dose was established according to the ratio between animal and human body surface area. The treatment lasted for 8 weeks. Ten rats from the normal and sham groups were randomly chosen to match the number of rats in the CHF and Olm groups for quantitative real-time PCR and western blotting. All surviving rats were assessed by echocardiography before and after treatment, while PRA and Ang II levels were detected by radioimmunoassay.
Echocardiography
After being anesthetized by an intra-abdominal injection of 1% pentobarbitol sodium (30 mg/kg), the rats were assessed using a 10-MHz phased-array transducer (Siemens, Germany) at a left 30° decubitus position. Two-dimensional parasternal long- and short-axis views were obtained at the papillary muscle level. Left ventricular ejection fraction, left ventricular end diastolic dimension (LVEDD), and left ventricular end systolic dimension (LVESD) were measured. All measurements, performed by an experienced technician who did not know the treatments, were averaged over three consecutive cardiac cycles.
Radioimmunoassay and tissue preparation
After rats had been anesthetized as described above, 2 ml of blood were obtained from the abdominal aorta, collected into ice-cooled anticoagulant tubes (containing 20 µl ethylene-diaminetetraacidic acid (EDTA), 10 µl 2-mercaptoethanol, and 20 µl 8-hydroxy quinoline), centrifuged at 20000× g for 10 min at 4°C and stored at −80°C. After extraction, plasma samples were directly tested by homogeneous competition radioimmunoassay using the radioimmunoassay kits for PRA and Ang II mentioned above, and then measured using a γ-radioimmunoassay counter after being centrifuged at 3000× g for 15 min at 4°C.
After taking blood samples from the abdominal aorta, the thorax was opened. Lung tissue for quantitative real-time PCR and western blotting was snap-frozen in liquid nitrogen and stored at −80°C until analysis.
Microscopic structure inspection
The lungs were filled with 10% formalin for at least 24 h before paraffin embedding and sectioning (4 μm). Sections were stained with hematoxylin-eosin. The tissues were examined using an Olympus DP70 microscope (Olympus, Tokyo, Japan). Forty histological fields (×40 magnification) were analyzed from at least four separate samples. A strict protocol for blinding and randomization was adhered to, including randomly choosing 10 sections from each mouse and selecting the most typical images to present in the results.
RNA preparation, reverse transcription, and quantitative real-time PCR
Total RNA extraction, reverse transcription-PCR and quantitative real-time PCR were performed as previously described, 9 using Trizol reagent, an RT-PCR kit and a SYBR Green Real-Time PCR kit. The PCR primer sequences are described in Table 1. The housekeeping gene GAPDH was used as a control. Each sample was tested in triplicate. The results were normalized against GAPDH and expressed as fold change using the 2−ΔΔCT method. 10
Primer sequences used in quantitative real-time PCR reactions for α1A-AR and β-AR subtypes.
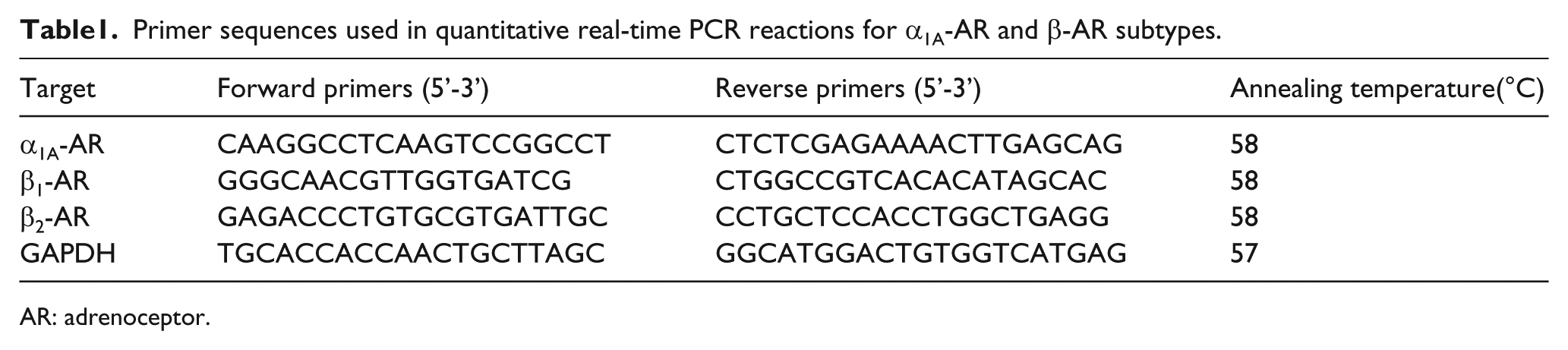
AR: adrenoceptor.
Protein preparation and western blotting
Samples were homogenized in RIPA buffer (50 mM Tris/HCl pH 7.4, 150 mM NaCl, 2 mM EDTA, 1% NP-40, 0.1% SDS) and total protein was extracted from the homogenates. The protein concentration of the lung was quantified using the Bradford protein assay. Proteins were resolved on a 10% sodium dodecyl sulfate polyacrylamide gel (SDS-PAGE), transferred to a nitrocellulose filter membrane using a semi-dry electrophoretic graphite electrode with constant electric current of 1 mA/cm2 gel for 2 h. Membranes were blocked with 5% nonfat dry milk in Tris-buffered saline-Tween (TBST) (20 mM Tris, 500 mM NaCl, pH 7.5, 0.1% Tween 20) at room temperature for 2 h, then incubated overnight at 4°C with diluted primary antibodies in 5% nonfat milk in TBST. The dilutions of the specific antibodies for receptor subtypes were as follows: α1A-AR, 1:200; β1-AR, 1:200; β2-AR, 1:100. The membranes were washed three times with TBST at room temperature and then incubated with horseradish peroxidase-conjugated secondary antibody (β-actin was used as an internal standard). AB chromogenic agent (Santa Cruz Biotechnology, Inc.) was applied to the membrane for development of the film, and a scanner was used for imaging. Densitometry was applied to the analysis of protein level. The results of western blot analysis were quantified by measuring the relative intensity compared with the control using Quantity One 4.6 (Bio-Rad, Hercules, CA, USA). Ratio of signal intensity of objective strips together with intra-reference strips (β-actin) represented expressed levels of objective receptors in tissues.
Statistical analysis
SPSS 17.0 was used for statistical analysis. Data are presented as mean ± standard deviation (SD) for all assays. Statistical significance was estimated by one-way analysis of variance (ANOVA) followed by a Newman–Keuls test for comparison. A value of p < 0.05 was considered statistically significant.
Results
Apart from early death within the first 24 h after operation, one rat in CHF group died during the treatment period.
Effects of olmesartan on heart function
There was no statistically significant difference in the LVEF between the normal and sham groups before therapy (p > 0.05). Compared with the sham group, LVEF of the CHF and Olm groups was dramatically decreased (p < 0.01, p < 0.05,), whereas LVEDD and LVESD were significantly increased (p < 0.01, p < 0.05). After therapy, compared with the CHF group, LVEF of the Olm group was clearly increased (p < 0.05), while LVEDD and LVESD were decreased (p < 0.05; Table 2).
Results of heart function detected by ultrasonic cardiogram before and after therapies (mean±SD).

BT: before therapy; AT: after therapy; LVEF: left ventricular ejection fractions; LVEDD: left ventricular end diastolic dimension; LVESD: left ventricular end systolic dimension.
p < 0.01 vs. Sham group.
p < 0.05 vs. Sham group.
p < 0.05 vs. CHF group.
Effects of olmesartan on serum PRA and Ang II levels
There were no differences in PRA or Ang II between the normal and sham groups. Compared with the sham group, PRA and Ang II of rats in the CHF group were significantly increased (p < 0.01), but PRA and Ang II in the Olm group were lower than in the CHF group (p < 0.05; Table 3).
Results of PRA and Ang II levels detected by radioimmunoassay (mean±SD).

PRA: plasma renin activity; Ang II: angiotensin II.
p < 0.01 vs. Sham group.
p < 0.05 vs. CHF group.
Effects of olmesartan on pulmonary structure
In comparison with the sham group, the pulmonary structure was remodeled in rats in the CHF group: thickening of the alveolar septa, cellular proliferation and infiltration of inflammatory cells were all observed. The pulmonary structure remodeling was improved in the Olm group (Figure 1).

Lung histopathology in different groups. The lung tissues of rats were obtained from normal rats (a), sham-operated rats (b), chronic heart failure rats (c) and olmesartan-treated chronic heart failure rats (d) prior to staining with hematoxylin and eosin (H & E). All sections are shown at 40× magnification.
Effects of olmesartan on α1A-AR, β1-AR and β2-AR mRNA levels
Expression of α1A-AR, β1-AR and β2-AR mRNA in the normal and sham groups showed no difference (p > 0.05). Compared with the sham group, the expression of α1A-AR and β1-AR mRNA was markedly decreased in the CHF group (p < 0.05); while β2-AR mRNA expression did not change (p > 0.05). After administration of olmesartan, mRNA expression of all three AR subtypes was significantly increased (p < 0.05; Figure 2).

The mRNA expressions of α1A-adrenoreceptor (AR), β1-AR and β2-AR in lung tissue of rats. The results are expressed as the mean values ±SD. *p < 0.05 vs. sham group; **p < 0.05 vs. CHF group.
Effects of olmesartan on α1A-AR, β1-AR and β2-AR protein levels
Compared with the sham group, the protein expression of α1A-AR and β1-AR was markedly decreased in the CHF group (p < 0.05). The protein expressions of α1A-AR, β1-AR and β2-AR were significantly increased in the Olm group compared with the CHF group (p < 0.05) (Figure 3).

Western blotting for detection of α1A-adrenoreceptor (AR), β1-AR, β2-AR and β -actin expressions in lung tissue of rats. The results are expressed as a percentage of the given band/ β-actin band, and as the mean values ±SD. *p < 0.05 vs. sham group; **p < 0.05 vs. CHF group.
Discussion
The main findings of our study are: (1) Olmesartan can improve heart function and pulmonary remodeling in rats with CHF; (2) CHF was associated with increased PRA and Ang II levels, which can be inhibited by olmesartan; and (3) the levels of α1A-AR and β1-AR mRNA and protein expression in the lung were down-regulated in CHF, while the mRNA and protein expressions of α1A-AR, β1-AR and β2-AR were enhanced by olmesartan. These results indicate that olmesartan may play a beneficial role in the protection of lung in CHF by up-regulating the expression of AR and decreasing levels of PRA and Ang II.
Activation of the SNS and the RAS are pathophysiological consequences of CHF. PRA and Ang II levels would be elevated after RAS activation, and Ang II could promote lung injury by stimulating the release of inflammatory cytokines, generating reactive oxygen species and accelerating fibrosis. 11 Furthermore, the lungs are very sensitive to the vasoconstrictive and proliferative effects of Ang II. A previous study reported the protective effect of irbesartan on lung remodeling in rats with CHF. 12 However, most ARBs increase PRA and Ang II levels because of the lack of negative feedback on renin activity. Some studies have reported that long-term treatment with olmesartan in hypertension resulted in decreased plasma levels of Ang II.1,13 However, there are very few studies concerning the effect of olmesartan on Ang II in CHF. AR also participates in the regulation of lung function, and α1A-AR and β2-AR are the main AR subtypes in rat lung. α1A-AR mediates contraction of lung vessels and hyperplasia of vascular smooth muscles, while β2-AR mediates bronchial smooth muscle relaxation and alveolar fluid clearance, and has anti-inflammatory action.2–6 Notably, β2-AR plays a very important role in regulating lung function in CHF, and in other diseases.14,15
In our study, there was a decrease in PRA and Ang II levels and an improvement of heart function after administration of olmesartan, which is consistent with some previous studies.1,13,16,17 One possible mechanism is that olmesartan activation of angiotensin-converting enzyme 2 (ACE2) can hydrolyze Ang II to Ang1–7. Increased Ang1–7 and decreased Ang II showed a beneficial effect on ventricular remodeling and improve heart function. 18 In the present study, we found that pulmonary structure remodeling and inflammation were improved after administration of olmesartan. This is entirely consistent with a report by Jasmin et al. 12 We speculate that this result is associated with the down-regulation of Ang II by olmesartan. Furthermore, the protective effect of olmesartan on heart function might help to reduce lung injury.
Our previous study showed that expression of α1-AR and β-AR subtypes was altered in the heart of rats with CHF. 19 In this study, we also found changes in the lung, with α1A-AR being down-regulated in the lung tissue of rats with CHF. When CHF occurs, the development of pressure or volume overload of the lung microcirculation elicits adaptions. It increases the resistance of gas transfer, disorders of fluid filtration and reabsorption, and alveolar membrane remodeling. 20 Down-regulation of α1A-AR can relax the pulmonary artery and inhibit the proliferation of vascular smooth muscle, which may delay the development of pulmonary hypertension and protect the function of the right ventricle. The expression level of β2-AR was not down-regulated in the lungs of rats with CHF, which could be helpful for the relaxation of vascular and bronchial smooth muscles, and promotion of clearance of pulmonary edema fluid through regulation of sodium ion channels and release of inflammatory factors.20,21 Therefore, it had a beneficial effect in reducing pulmonary edema and improving pulmonary micro vascular permeability in CHF.14,22 These changes may therefore be adaptive reactions. The SNS would be activated in CHF and the elevated catecholamine could down-regulate β-AR by activating β-adrenergic receptor kinase and phosphorylating β-AR. 23 Therefore, the down-regulation of β1-AR may be a compensatory reaction to high levels of catecholamine in CHF.
It is generally accepted that there are extensive interactions between the SNS and the RAS. Our results showed that α1A-AR, β1-AR and β2-AR protein expression was up-regulated after administration of olmesartan. Some data suggest that Ang II can modify the expression of α1-AR.24,25 α1-AR tends to become more sensitive to agonists owing to an elevated Ang II level, which promotes alpha-adrenergic vasoconstriction. 26 The down-regulation of α1A-AR in CHF lung might be associated with the elevated Ang II level. While olmesartan reduced the Ang II level, α1A-AR expression returned to normal levels. β1-AR expression was down-regulated in CHF lung. This is in good agreement with some studies, which reported that Ang II can decrease the expression level of β1-AR by acting on AT1R and then inhibiting adenylate cyclase activity; this effect could be inhibited by AT1R antagonists or adenylate cyclase inhibitors.27,28 After the Ang II level was decreased, β1-AR expression levels also returned to normal. However, β2-AR expression was not down-regulated in the current study. Similar data have been reported, in which β2-AR expression had not fundamentally changed in the heart of rats with CHF; β2-AR function had been desensitized in CHF to protect the organ.15,19 After treatment with olmesartan, the expression of β2-AR was up-regulated, which could better protect the lung function of rats with CHF. These mechanisms require further research.
Conclusion
Olmesartan can decrease levels of PRA and Ang II and regulate the expression of α1A-AR, β1-AR and β2-AR, which may improve heart function and protect the lung.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported in part by the Chinese Integrated TCM-WM Scientific Research Foundation (No. 2011-01).