
Abstract
Introduction:
Angiotensin-converting enzyme 2 (ACE2) is a member of the renin–angiotensin system that degrades angiotensin (Ang) II to the seven-amino acid peptide fragment Ang-(1-7). We evaluated the changes in urinary ACE2 levels in response to treatment with the angiotensin II type 1 receptor blocker olmesartan in diabetes patients with nephropathy.
Materials and methods:
This prospective, open-label, interventional study was conducted with 31 type 2 diabetes patients with nephropathy. After initial evaluation, patients received 20 mg/day olmesartan, which was increased to 40 mg/day over a 24-week period.
Results:
In diabetes patients with chronic kidney disease, olmesartan significantly increased urinary ACE2 levels independently of blood pressure and plasma aldosterone levels and reduced albuminuria, urinary liver-type fatty acid binding protein (L-FABP), and plasma aldosterone levels. Multivariable regression analysis revealed that the change in urinary L-FABP levels was an independent predictor of increased urinary ACE2 levels.
Conclusion:
Olmesartan may have the unique effect of increasing urinary ACE2 levels. However, whether this contributes to olmesartan’s renoprotective effect must be examined further.
Keywords
Introduction
Angiotensin-converting enzyme 2 (ACE2) is a member of the renin–angiotensin system (RAS) that degrades angiotensin (Ang) II to the seven-amino acid peptide fragment Ang-(1-7).1,2 ACE2 is thought to function as a negative regulator of the RAS by degrading Ang II and producing Ang-(1-7) to counterbalance the Ang II-forming activity of ACE. Although ACE2 is reported to localize in renal glomeruli and tubules,3–6 the differences in ACE2 expression within the kidney seem to be not only tissue-specific but also cell-specific.6–9 Glomerular expression of ACE2 is reduced in diabetic mice, 6 and reduced ACE2 gene and protein expression has been confirmed in renal biopsies of patients with type 2 diabetes. 7 On the other hand, at the tubular level, increased ACE2 activity and protein expression have been found in diabetic mice.8,9 The renal RAS, specifically Ang II, plays a pivotal role in the pathogenesis of diabetic nephropathy. 10 Ang II and ACE are activated in type 2 diabetes 11 and are involved in the development of microvascular and macrovascular complications of diabetes such as nephropathy, retinopathy, and cardiovascular disease. 12 ACE 2 plays an integral role in protecting against renal damage and cardiovascular disease.8,13 It was reported that deletion of ACE2 leads to the development of Ang II-dependent renal damage, suggesting ACE2 as a renoprotective target in diabetes. 14 ACE2 is a homologue of ACE but is not blocked by ACE inhibitors. However, there are no clinical data showing whether Ang II type 1 receptor blockers (ARB) increase ACE2 activity. In this study, we evaluated the changes in urinary ACE2 levels resulting from ARB treatment in diabetes patients with chronic kidney disease (CKD).
Research design and methods
This prospective, open-label, interventional study was conducted with 31 outpatients after obtaining written informed consent and with the approval of the local ethics committee. The study was performed in accordance with the Declaration of Helsinki. Enrollment criteria were as follows: 1) type 2 diabetes with nephropathy under stable glycemic control, defined as a hemoglobin A1c (HbA1c) level <8.0% after administration of oral antidiabetic agents, insulin injection therapy, or diet therapy alone for 8 consecutive weeks; 2) albuminuria: urinary albumin/creatinine (Cr) ratio >30 mg/g (average of two consecutive measurements recorded during the 8-week pre-treatment period); 3) estimated glomerular filtration rate (eGFR) of 30–89 mL/min/1.73 m2; and 4) hypertension: systolic and diastolic blood pressure (BP) ≥130/80 mmHg treated with a fixed dose of antihypertensive agents other than RAS inhibitors for at least 8 weeks before the study. Exclusion criteria were as follows: 1) age <20 years or >80 years; 2) more than second-degree hypertension (BP >160/100 mmHg) 15 ; 3) eGFR ≥90 mL/min/1.73 m2 or <30 mL/min/1.73 m2; 4) severe heart failure, angina, myocardial infarction, or stroke occurring within 6 months before the trial; and 5) previous treatment with ARB for at least 8 weeks before the study.
After initial evaluation, patients received 20 mg/day olmesartan, which was increased to 40 mg/day over a 24-week period. Doses of other antihypertensive agents and statins were maintained during the study. BP measurements were performed at the outpatient clinic according to Japanese Society of Hypertension (JSH) 2009 guidelines at fixed times after the administration of medications. 15 Target BP was <130/80 mmHg. Measurements were made using a sphygmomanometer (Nippon Colin Co. Ltd, Tokyo, Japan) and performed twice with the patient seated after a 5-min rest.
At each patient visit, safety variables and patient compliance with treatment regimens were assessed. Plasma renin activity and aldosterone concentrations were measured by radioimmunoassay at a contract laboratory (SRL, Inc., Tokyo, Japan) at baseline and at week 24 with the patient in the supine position after a 20-min rest. Urinary albumin excretion was assessed by measuring urinary concentrations of albumin and Cr (albumin/Cr ratio) in the first morning urine sample. Urinary albumin levels were measured by the immunoturbidimetric assay. Urinary liver-type fatty acid binding protein (L-FABP) was measured in the same urine sample by a specific enzyme linked immunosorbent assay (ELISA; SRL, Inc.), and the results were expressed relative to the urinary Cr concentration. Urinary ACE2 concentration was measured at baseline and at week 24 by ELISA (Human ACE2 ELISA Kit, AdipoGen, Inc., Seoul, Korea) as described previously.16,17 The eGFR was calculated according to the following formula for Japanese patients 18 : eGFR (mL/min/1.73 m2) = 194 × sCr−1.094 × age−0.287(× 0.739 for women).
Data are expressed as means ± SEM. Changes in biochemical and urinalysis parameters were analyzed using the paired t-test. The relationships between variables were analyzed using Pearson’s correlation. Determinants of the factors associated with the changes in urinary ACE2 levels were assessed using multivariable linear regression. Age, sex, body mass index, changes in systolic and diastolic BP, urinary albumin/Cr ratio, and levels of eGFR, plasma glucose, HbA1c, plasma aldosterone, and urinary L-FABP were selected for the multivariate model. SAS 8.13 (SAS Institute, Cary, NC) was used for all analysis, and significance was set at p < 0.05.
Results
All enrolled patients (n = 31) remained in the study until the end of the trial. Baseline characteristics and concomitant medication use at baseline are shown in Table 1. Fifteen patients (48%) were using other antihypertensive agents at baseline. The final olmesartan dose was 26 ± 2 mg/day. As shown in Table 2, olmesartan treatment significantly decreased both systolic and diastolic BP values. No significant differences were seen in serum Cr levels or eGFR values during the study period. Furthermore, urinary L-FABP level was significantly decreased after olmesartan treatment. Figure 1 shows that the urinary albumin/Cr ratio was significantly decreased by olmesartan treatment from 720 ± 201 mg/gCr at baseline to 317 ± 91 mg/gCr at the end of the study (p < 0.01), whereas urinary ACE2 concentration was significantly increased from 27.8 ± 4.6 ng/mgCr at baseline to 42.9 ± 7.0 ng/mgCr at the end of the study (p < 0.05). Figure 2 shows that plasma renin activity was not significantly changed after 24 weeks of treatment, but plasma aldosterone levels were decreased from 97.6 ± 10.4 at baseline to 77.5 ± 6.7 pg/mL at the end of the study (p < 0.05).
Patient baseline characteristics and medication use.
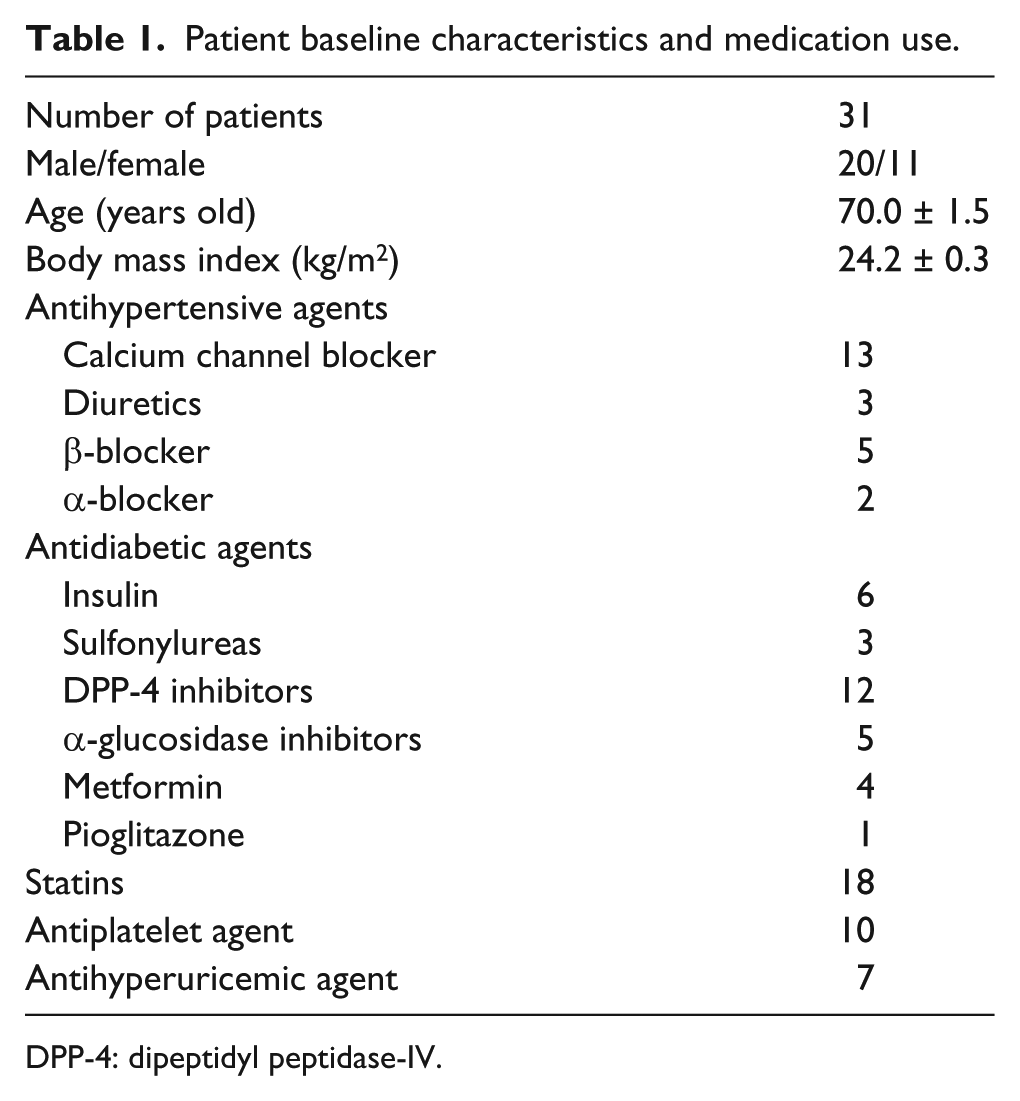
DPP-4: dipeptidyl peptidase-IV.
Changes in measured parameters.

BP: blood pressure; eGFR: estimated glomerular filtration rate; L-FABP: liver-type fatty acid binding protein.
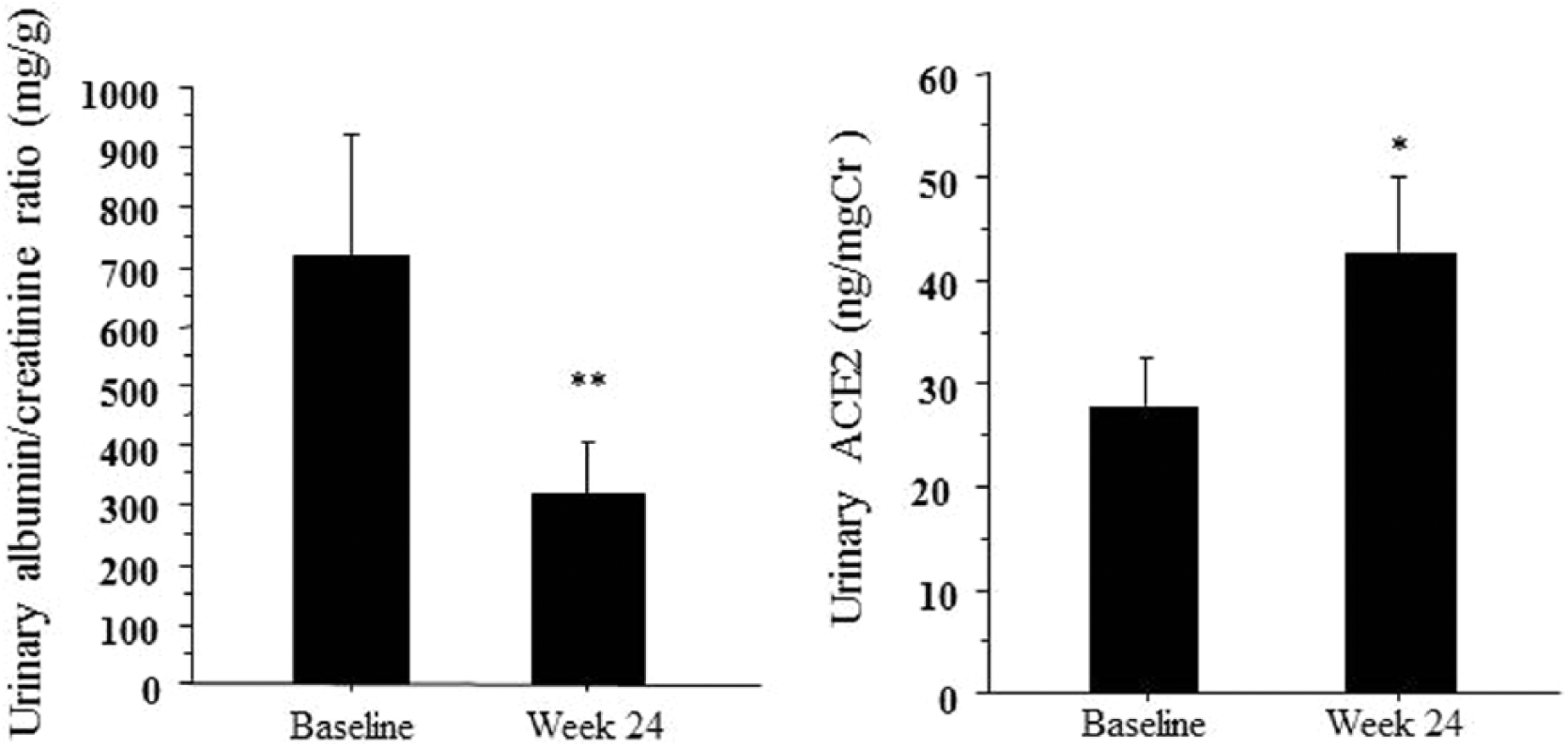
Changes in the urinary albumin excretion ratio and urinary angiotensin-converting enzyme 2 levels. *p < 0.05, **p < 0.01 vs. baseline.
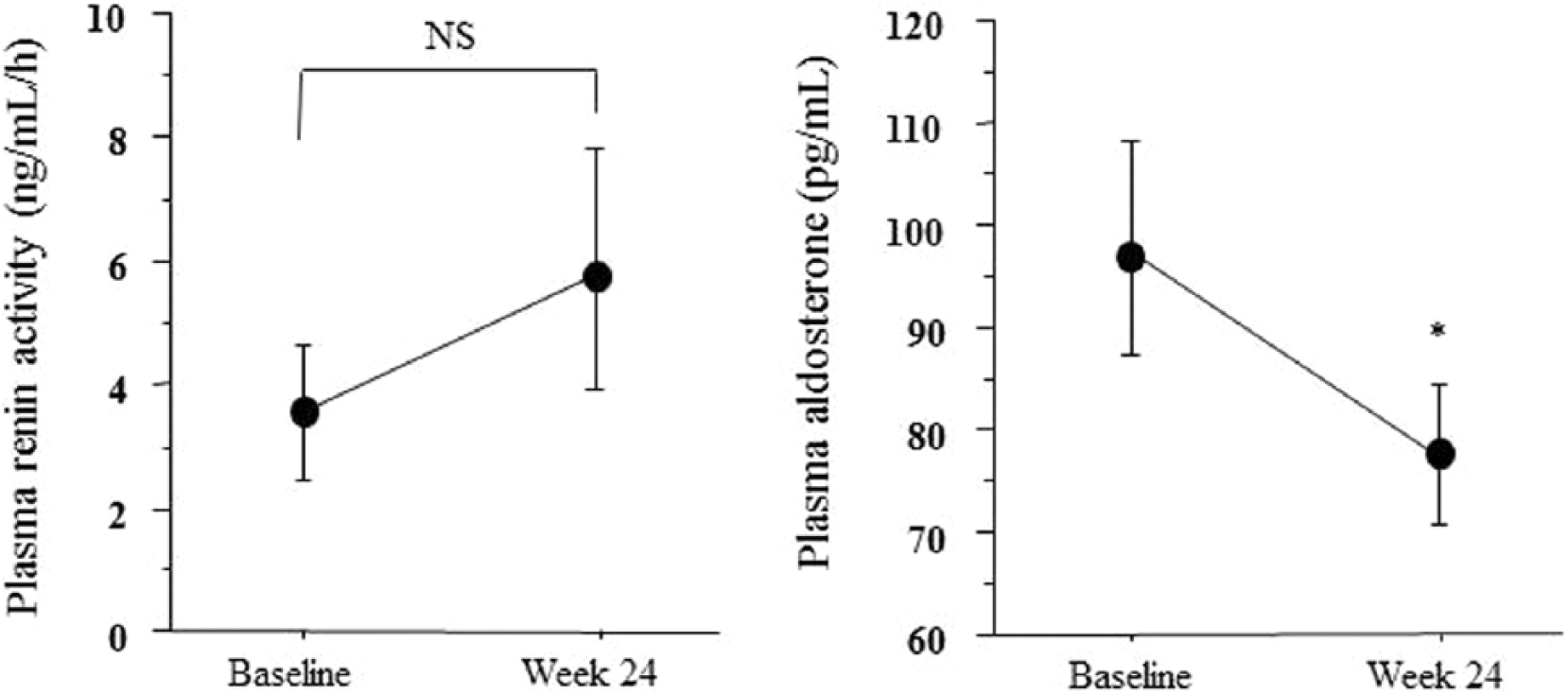
Changes in plasma renin activity and plasma aldosterone levels. *p < 0.05 vs. baseline.
In a simple regression analysis, changes in urinary ACE2 levels correlated significantly with changes in urinary L-FABP levels (r = 0.427, p = 0.016), but not with systolic and diastolic BP, urinary albumin/Cr ratio, or eGFR levels (Table 3). Multivariable regression analysis showed that urinary L-FABP levels were an independent predictor of changes in urinary ACE2 levels (R2 = 0.426) (Table 4).
Simple regression analysis of changes in urinary angiotensin-converting enzyme 2 levels.

eGFR: estimated glomerular filtration rate; L-FABP: liver-type fatty acid binding protein; UACR: urinary albumin to creatinine ratio.
Multivariable regression analysis of changes in urinary angiotensin-converting enzyme 2 levels.
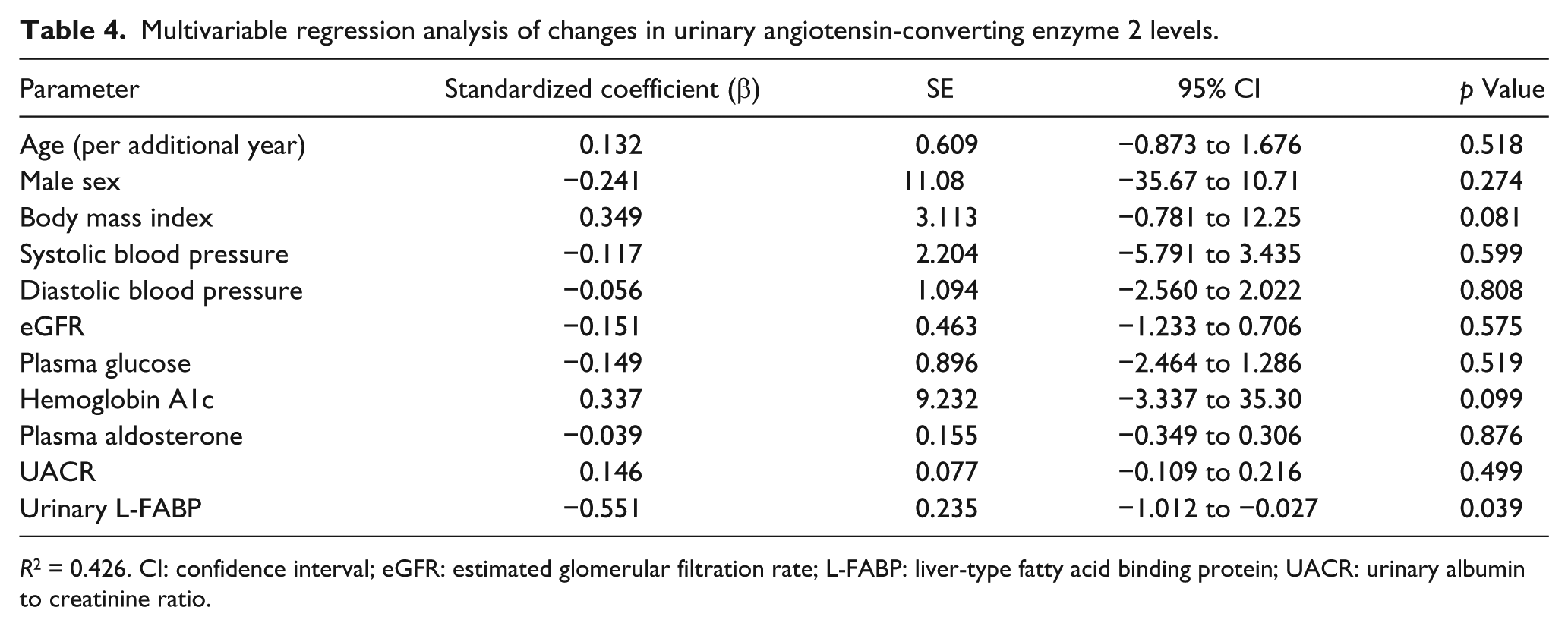
R2 = 0.426. CI: confidence interval; eGFR: estimated glomerular filtration rate; L-FABP: liver-type fatty acid binding protein; UACR: urinary albumin to creatinine ratio.
During the observation period, none of the patients exhibited a significant increase in the occurrence of adverse effects such as hypotension, and none required renal replacement therapy for hyperkalemia or progressive loss of kidney function.
Discussion
Ang-(1-7) is formed from Ang I and Ang II mainly by ACE2 and acts on the receptor protein Mas. 19 Based on these interactions, a new bioactive pathway in the RAS, referred to as the ACE2–Ang–(1-7)–Mas axis, has been proposed.20,21 This axis is antagonistic to the classical RAS pathway with ACE–Ang II–Ang II type 1 receptors.22,23 Deletion or inhibition of ACE2 has been associated with albuminuria in diabetic mice24,25 and with the development of Ang II-dependent renal damage. 14 Conversely, administration of human recombinant ACE2 was shown to reduce BP and attenuate glomerular injury in rodent models.26,27 Furthermore, ACE2 delivery by a recombinant protein or virus ameliorated the progression of diabetes-related complications, such as nephropathy and retinopathy.28–30 Thus, ACE2 may be an endogenous protector against the progression of CKD.
Chronic administration of either telmisartan or captopril did not change urinary ACE2 levels in mice. 31 Previous studies in humans have shown no significant effects of ARBs or ACE inhibitors on urinary ACE2 levels,17,32 although in these studies the effects were analyzed for ARBs in general, not for specific ARBs. Furthermore, urinary ACE2 levels in patients treated with olmesartan for >1 year were higher than in healthy controls, although other antihypertensive drugs, including calcium channel blockers and other RAS inhibitors, had no such effects on urinary ACE2 levels in an observational study. 33 However, the urine samples for ACE2 determination were collected only once, and thus the extent of changes in ACE2 levels due to antihypertensive agents could not be critically assessed. Taken together, no interventional studies have examined whether ARBs can definitely increase ACE2 activity in humans. Here, we demonstrated that the ARB olmesartan can increase urinary ACE2 levels and decrease plasma aldosterone levels in diabetic nephropathy patients with CKD. Many functional differences exist among ARBs that are not mediated by Ang II type 1 receptor blockade. 34 Long-term treatment of hypertensive patients with olmesartan reduces plasma Ang II levels, whereas several other types of ARBs have been reported to increase plasma Ang II levels in hypertensive patients.35–37 These findings suggest that the increased ACE2 activity due to olmesartan contributes to reduced plasma Ang II levels by upregulating Ang-(1-7) formation.
Urinary ACE2 levels are associated with hyperglycemia, and insulin treatment has been observed to reduce urinary ACE2 levels in mice. 31 However, no significant associations were observed in the present study between changes in urinary ACE2 levels and changes in glycemic indices, including plasma glucose and HbA1c levels, since only well-controlled patients were assessed. Although it has been reported that some calcium channel blockers, including benidipine, azelnidipine, and cilnidipine, reduced albuminuria in diabetic nephropathy,38–40 many of the patients in the present study had been treated with amlodipine for at least 8 weeks at baseline, suggesting only a slight effect of amlodipine on decreasing the urinary albumin/Cr ratio and increasing urinary ACE2 levels. However, the changes in urinary ACE2 levels correlated significantly with urinary L-FABP levels in the present study. Significant urinary ACE2 levels most likely reflect the state of the proximal tubules, and differences may exist in patients with CKD and tubular injury compared with healthy individuals. 41 In patients with diabetic nephropathy, the development of progressive diabetic kidney disease was associated with changes in proximal tubules, renal function, and prognosis and showed a higher correlation with structural lesions in the tubulointerstitium than with glomerular changes. 42 Various proximal tubule pathophysiological stresses, such as proteinuria, induce upregulation of human L-FABP gene expression, thereby resulting in increased proximal tubular L-FABP excretion and increased urinary L-FABP excretion. 43 Urinary L-FABP is an important marker of tubulointerstitial changes in diabetic nephropathy, while oxidative stress is a pathogenic factor underlying diabetic complications such as nephropathy.44–46 Because multivariate regression analysis showed that urinary L-FABP is an independent variable significantly associated with urinary ACE2 levels, olmesartan may have potential against the progression of tubulointerstitial damage due to increased urinary ACE2 levels. Nevertheless, further studies are needed to identify the factors associated with the increase in ACE2 levels, as ACE2 has the potential to be a marker of renal RAS activation in these patients.
Our study design was limited by the small sample size, short treatment duration, and lack of a control group since it was a preliminary investigation. Furthermore, we did not measure plasma levels of Ang-(1-7), Ang II, and ACE2, or urinary ACE2 activity, in this study, and thus the changes in ACE2 activity and their impact on the RAS may not have been fully characterized. Additional long-term studies are needed to accurately assess the renoprotective effects of olmesartan therapy in diabetes patients. Moreover, it should be clarified whether ARBs other than olmesartan have the same potential to increase urinary ACE2 levels.
In conclusion, olmesartan treatment leads to a reduction in albuminuria, urinary L-FABP, and plasma aldosterone levels in diabetes patients with CKD; however, it may have the unique effect of increasing urinary ACE2 levels. Some previous studies in mice and humans have shown that other RAS blockers do not increase urinary ACE2 levels. Whether this unique increase contributes to olmesartan’s renoprotective effect must be examined further in a future study.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.