
Abstract
Introduction:
To determine if the serum prorenin level is useful for detecting ocular disease in a non-diabetic population.
Materials and methods:
We enrolled non-diabetic men (n = 402) and women (n = 349) in our study. We used the antibody-activating direct enzyme kinetic assay of human prorenin to determine serum prorenin levels. We performed multiple regression analysis to determine the factors that affect serum prorenin levels, such as: age, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol, fasting blood sugar, and HbA1c or estimated glomerular filtration rate. Our study subjects were divided into groups by their ophthalmologic diagnosis. One-way analysis of variance (ANOVA) was performed to detect a significant difference in the serum prorenin levels among the groups.
Results:
There were no significant differences in serum prorenin levels among the ocular diseases and disorders. The DBP was negatively correlated with serum prorenin levels in men (r = − 0.1992; p = 0.021) and in women (r = − 0.2067; p = 0.031).
Conclusion:
Considering the current results and those of previous studies together, we found that the prorenin value is useful solely for predicting development of diabetic retinopathy in adults.
Keywords
Introduction
Ocular diseases such as glaucoma, diabetic retinopathy (DR) and age-related macular degeneration (AMD) threaten visual function by causing irreversible neuro-vascular degeneration. To minimize the chances of blindness, predictors are needed to enable more opportunities for early intervention. Previous studies report that higher serum levels of prorenin, a precursor of renin, are associated with the subsequent development of DR.1–3
Prorenin undergoes proteolytic activation with cleavage to renin, by cathepsin B and renin processes that form a rate-limiting step of the renin-angiotensin system (RAS) in the circulation. Prorenin was shown to exhibit renin-like enzymatic activity, via non-proteolytic activation in the local RAS. The mechanism underlying the non-proteolytic activation of prorenin is that prorenin binds to the (pro)renin receptor and undergoes a conformational structural change, to expose its active site.4,5 This is referred to as the receptor-associated prorenin system (RAPS). Previous studies report that the RAPS plays an important role in DR.2,3,6–8 Moreover, the results of studies that used rodent models of ocular diseases clearly suggest that the RAPS is critically involved in the generation of choroidal neovascularization (CNV), 9 uveitis 10 and retinopathy of prematurity 11 ; indicating that the RAPS also might be associated with development of ocular diseases other than DR. Thus, we designed the current study to assess whether serum prorenin levels are valuable for detecting eye diseases other than DR in non-diabetic adults.
Materials and methods
We enrolled 751 non-diabetic Japanese subjects (402 men and 349 women) who visited our hospital, for the current study. Non-diabetic subjects were defined as those without a history of diabetes nor abnormalities indicating the presence of diabetes. After the subjects were informed of the purpose of the current study, they provided informed consent. We collected blood samples from all participants in the morning, to measure biochemical parameters that included total cholesterol, high-density lipoprotein (HDL) cholesterol, aminotransferase (AST), alanine aminotransferase (ALT), uric acid, fasting glucose and hemoglobin A1c (HbA1c), plus the serum levels of prorenin and serum creatinine. We calculated the estimated glomerular filtration rate (eGFR) using the serum creatinine to evaluate renal function that might affect the circulatory prorenin levels. 12 Our study adhered to the Declaration of Helsinki. The Research Ethics Committee of Asahikawa Medical University approved the study.
We measured the serum prorenin levels using the antibody-activating direct enzyme kinetic assay of human prorenin (AAD-PR assay), as previously described. 13 That previous study shows clearly that the AAD-PR assay has a higher sensitivity (up to 1.5-fold) for detecting prorenin levels, compared with conventional methods. 13
In addition to using the prorenin measurement, we measured blood pressure (BP) twice, consecutively, while the subjects were seated, using an automatic device (EP-88Si, Colin, Tokyo, Japan). The mean of both measured values was used for our analysis.
We performed an ophthalmic examination that included the slit lamp test, retinal photography and visual field testing using frequency-doubling technology (FDT) perimetry (Carl Zeiss Meditec, Dublin, CA) with the C20-1 program. We obtained a fundus photograph with a 50° angle of view, to include the optic disc and the macula. Well-trained ophthalmologists examined the retinal photographs, to identify any signs of ocular diseases. We diagnosed glaucoma in the subjects with visual field abnormalities that corresponded well with the glaucomatous appearance of the optic disc. We performed the slit lamp examination to detect cataracts. We defined as normal subjects those with no abnormalities detected during any examination and those without a history of both systemic and ocular diseases.
The study data are given as mean ± SD. We performed the unpaired t-test to compare the characteristics between men and women. We performed multiple regression analyses to determine the variables that affect serum prorenin levels in men and women. We performed multiple comparisons to detect differences in serum prorenin levels among the patients who were divided into groups, by ocular disorders and diseases. A p value of 0.05 or less was considered statistically significant.
Results
Table 1 shows the differences between men and women for the studied parameters (age, BMI, SBP, DBP, triglycerides, HDL cholesterol, AST, ALT, uric acid, fasting blood sugar, HbA1c and eGFR).
Subject characteristics.

ALT: alanine aminotransferase; AST: aminotransferase; BMI: body mass index; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; HbA1c: hemoglobin A, Type 1C; HDL: high-density lipoprotein; IU: international units; mmHg: millimeters of mercury, a measure of pressure; SBP: systolic blood pressure; SD: standard deviation
To eliminate any gender difference, multiple regression analysis was performed in men and women (Table 2 and Table 3, respectively). Only DBP was correlated negatively with serum prorenin levels, in both genders, as seen in Figure 1 (men, standardized partial regression coefficient (r) = − 0.1992; p = 0.021 and women, r = − 0.2067; p = 0.031); while the SBP was not correlated significantly with serum prorenin levels. We found that eGFR was not correlated with serum prorenin levels in non-diabetic men nor women.
Factors correlated with the serum prorenin levels in non-diabetic men.

ALT: alanine aminotransferase; AST: aminotransferase; BMI: body mass index; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; HbA1c: hemoglobin A, Type 1C; HDL: high-density lipoprotein; IU: international units; mmHg: millimeters of mercury, a measure of pressure; r: standardized partial regression coefficient; SBP: systolic blood pressure; SD: standard deviation
Factors correlated with the serum prorenin levels in non-diabetic women.

ALT: alanine aminotransferase; AST: aminotransferase; BMI: body mass index; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; HbA1c: hemoglobin A, Type 1C; HDL: high-density lipoprotein; IU: international units; mmHg: millimeters of mercury, a measure of pressure; SBP: systolic blood pressure
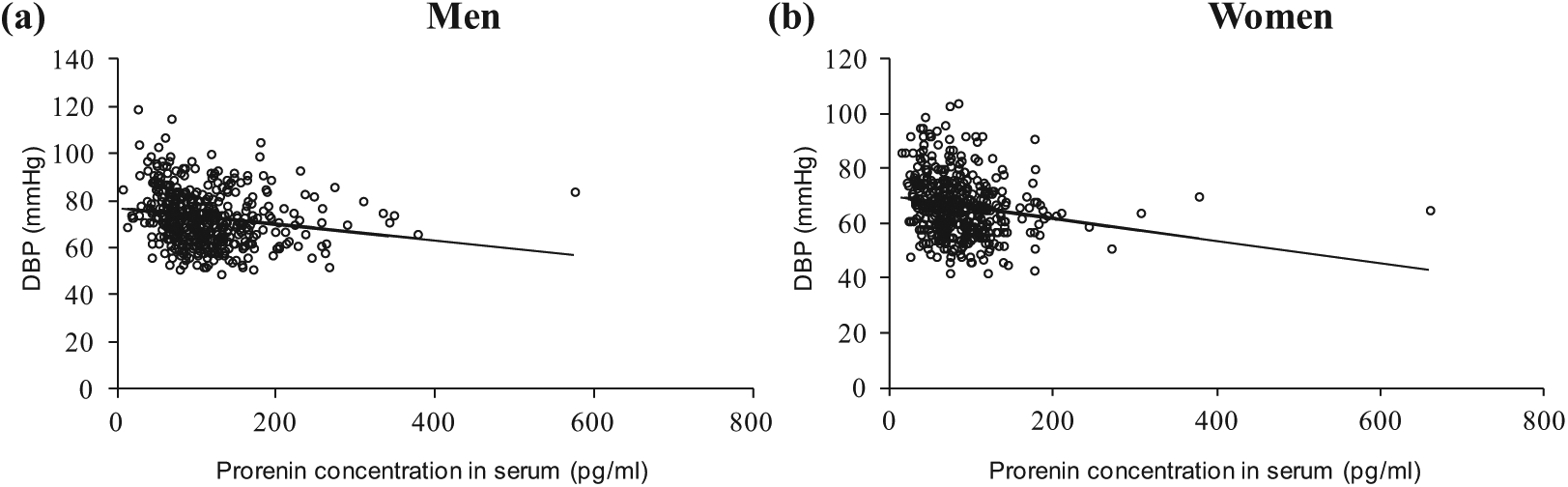
Correlation between serum prorenin levels and DBP in healthy men and women. Serum prorenin levels were negatively correlated with DBP in (a) men (r = – 0.1992; p = 0.021) and (b) women (r = − 0.2067; p = 0.031).
Our study subjects were grouped by ocular disorders (Table 4). To perform statistical analyses to see if there was a difference in serum prorenin levels among these ocular diseases, we chose to exclude some groups in which the number of participants was few (the nonhighlighted groups in Table 4).
Ocular diseases and disorders in men and women. The highlighted data were used for the multiple comparison analysis in Figure 2.

As is shown in Figure 2, we made comparisons using the data of cataract (prorenin concentration = 102 ± 17.1 pg/ml), conus (136 ± 64.4 pg/ml), glaucoma (77.9 ± 29.1 pg/ml), optic disc cupping (119.4 ± 44.0 pg/ml), retinal arteriolar sclerosis (108.3 ± 65.6 pg/ml) and healthy control (107.0 ± 56.6 pg/ml) groups in men; with the conus (59.8 ± 26.6 pg/ml), glaucoma (75.2 ± 35.9 pg/ml), retinal arteriolar sclerosis (62.7 ± 22.5 pg/ml) and healthy control (87.0 ± 51.9 pg/ml) groups in women: There was no statistically significant difference found in the multiple comparisons in men (p = 0.08) and women (p = 0.16).

Comparison of the serum prorenin levels between the patients with ocular disorders and normal subjects (control subjects) in men and women. There was no statistically significant difference found in men (p = 0.08) nor women (p = 0.16).
Discussion
In the present study, we measured the serum prorenin levels in non-diabetic subjects to determine if any non-diabetic factors were associated with RAPS. Our study showed that serum prorenin levels were correlated negatively with DBP, but not with SBP, in non-diabetic subjects; and that no ocular disorders were correlated with serum prorenin levels in those non-diabetic subjects.
Although it is unknown whether prorenin itself can modulate BP as angiotensin II does, a previous clinical study reports that serum prorenin levels are correlated negatively with DBP and SBP. 14 Higher BP was suggested to cause negative feedback of the RAS, resulting in a decreased serum prorenin level when BP is high. In contrast, studies using transgenic animals with extremely high prorenin levels compared to wild type animals fail to show a definite effect of prorenin on BP, because of having the opposite results.15,16 The current study showed that the serum prorenin level was correlated negatively with the DBP, but not with SBP, in a non-diabetic human population; thus, the negative feedback system of the RAS might be dominant, especially in a non-diabetic population.
The goal of the current study was to determine for the first time if any ocular disorders were associated with changes in serum prorenin levels in non-diabetic adults. The current data did not show any differences in serum prorenin levels among patients with ocular disorders such as conus, cataracts, glaucoma nor retinal arteriolar sclerosis. In fact, we speculated that the serum prorenin levels might increase in subjects with certain ocular diseases in which inflammation plays a role. Satofuka et al.9,6 previously reported that inhibition of non-proteolytic activation of prorenin reduces the expression of pro-inflammatory cytokine in an experimental CNV model 9 and storeptozotocin-induced diabetes model. 6 In the present study, no patient had CNV associated with exudative AMD. A further study is needed to compare the serum prorenin levels between subjects with and without exudative AMD.
A limitation of the current study was that a direct role of circulatory prorenin in the pathogenesis of ocular diseases has not yet been proven. The circulatory prorenin levels declined by 50% after bilateral nephrectomies, substantiating the presence of extra-renal sources of prorenin. 17 Regarding the retina, immunohistochemical studies show clearly that prorenin is produced in the retinal endothelial cells and ganglion cells6,18; however, it cannot be concluded that the retina is definitely the major source of prorenin in the circulation, because no study has determined whether ocular enucleation results in reduced circulatory prorenin levels. Therefore, a consideration is that changes in the serum prorenin levels result from activation of the RAPS in the eye, as well as other organs, such as the lungs, kidney, brain and ovaries. 4
In conclusion, we found that serum prorenin levels were correlated negatively with DBP in non-diabetic subjects. In addition, no ocular disorders were found to be correlated with serum prorenin levels in non-diabetic subjects. Taken together with previous works that suggest higher prorenin levels reflect the pathogenesis of diabetic microvascular complications, the measurement of serum prorenin may be valuable for predicting the development and progression of DR.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by the Japanese Ministry of Education, Science and Culture in Tokyo (Grant-in-aid for Young Scientists (B) number 23791955 (to author HY)).