
Abstract
Introduction:
Primary aldosteronism (PA) represents the most common cause of secondary hypertension. Beyond increased blood pressure, additional harmful effects of aldosterone excess including inappropriate left ventricle (LV) hypertrophy were found. We evaluated the effect of adrenalectomy and spironolactone on blood pressure and myocardial remodelling in a long-term follow-up study.
Methods:
Thirty-one patients with PA were recruited. Fifteen patients with confirmed aldosterone-producing adenoma underwent adrenalectomy; in the remaining 16 patients, treatment with spironolactone was initiated. Laboratory data, 24-hour ambulatory blood pressure monitoring (ABPM) and echocardiography parameters were evaluated at baseline and at a median follow-up of 64 months.
Results:
Both approaches reduced blood pressure (p = 0.001 vs. baseline). In both groups we observed a decrease in end-diastolic (p = 0.04, p = 0.01) and end-systolic LV cavity diameters (p = 0.03, p = 0.01). Interventricular septum and posterior wall thickness reduction was significant only after adrenalectomy (p = 0.01, p = 0.03) as was reduction of LV mass index (p = 0.004). A trend to lower LV mass on spironolactone was caused predominantly by diminution of the LV cavity, which was reflected in increased relative wall thickness (p = 0.05).
Conclusions:
Although both surgical and conservative treatment can induce a long-term decrease of blood pressure, adrenalectomy seems to be more effective in reduction of LV mass, as it reverses both wall thickening and enlargement of the LV cavity.
Introduction
Primary aldosteronism (PA) is the most common disorder causing secondary hypertension. Recent studies have shown that the prevalence of PA seems to be much higher than previously believed, and that this disease affects 5%–10% of the hypertensive population 1 and up to 20% of patients with moderate to severe hypertension. 2 This increase in the known prevalence rate is mainly related to more effective diagnostics using the aldosterone-to-renin ratio(ARR) as a screening test. 3
High aldosterone status was identified as an independent cardiovascular risk factor. 4 Patients with PA are threatened by stroke, ischaemic heart disease, atrial fibrillation or ventricular arrhythmias5,6 and also heart failure 7 to a higher degree than in essential hypertension of the same severity.
Considering its characteristic hormonal profile with autonomous aldosterone overproduction and suppressed plasma renin activity, PA gives us a unique opportunity to study the impact of high aldosterone levels on the cardiovascular system. Beyond the well-known role in homeostasis of minerals and body fluids and regulation of blood pressure, more recent studies have indicated additional harmful effects of aldosterone excess on the heart and blood vessels, including inflammation, collagen depositon, 8 myocardial fibrosis 9 and left ventricle (LV) remodelling. 10 These effects are independent of blood pressure levels and are related to high salt intake. 11 When compared with essential hypertension at the same blood pressure level, patients with PA have been shown to have increased arterial stiffness 12 and intima-media thickness. 13 Many echocardiographic studies reported a higher LV mass14–16 and more frequent LV hypertrophy, although these findings are not supported by all authors.17,18 Our recent results have also indicated an enlargement of the LV cavity and a higher prevalence of eccentric hypertrophy in PA 19 patients, suggesting the predominant effect of aldosterone-induced increase in plasma volume and therefore the preload of the LV. Nevertheless, the exact mechanisms of the development of myocardial remodelling caused by aldosterone remain unclear.
Several short-term studies have suggested that the changes in myocardial structure and function can be reversed by adrenalectomy due to aldosterone-producing adenoma.20,21 However, there are still a lack of data comparing the effects of specific treatment by surgery and spironolactone over a longer period. In this paper, we evaluated the impact of adrenalectomy or conservative treatment with aldosterone antagonists on myocardial alteration on long-term follow-up.
Methods
Participants
Thirty-one consecutive patients with PA were enrolled in our study. These individuals were recruited from the patients referred to our centre for the diagnosis of moderate to severe arterial hypertension, resistant hypertension (defined according to the European Society of Cardiology (ESC) guidelines 22 ), or hypertension with concurrent hypokalaemia.
The details on the recruitment and diagnostic criteria were described in our previous publication. 19
At least two weeks before admission, chronic antihypertensive treatment was switched to the combination of an α-blocker and slow-release verapamil, in order to compensate for hypertension and to minimise interactions between medication and laboratory hormonal examination. An absolute treatment withdrawal was not possible for ethical and safety reasons. Hypokalaemic patients were adequately treated with oral potassium supplements before running hormonal tests.
Patients with a high ARR (≥ 30 (ng/100 ml)/(ng/ml per hr) measured after two hours in the upright position) and elevated plasma aldosterone (≥150 ng/l) were considered highly suspicious for PA. The diagnosis of PA was then considered confirmed by plasma aldosterone levels over 80 ng/l after an intravenous saline load test. On the other hand, PA was considered highly unlikely in post-infusion plasma aldosterone levels under 50 ng/l. Patients in the ‘grey zone’ (indeterminate levels of 50–80 ng/l) were excluded from our study.23–25
To distinguish the definite subtypes of PA, we performed a computed tomography (CT) scan followed by selective adrenal vein sampling (AVS) in those patients who agreed with further invasive diagnostic methods and possible adrenalectomy. AVS was considered selective if the adrenal vein/inferior vena cava cortisol ratio exceeded 2:1. Lateralisation was then defined as an aldosterone-to-cortisol ratio in one adrenal vein at least four times higher than this ratio on the other side. 23
Patients with chronic diseases influencing heart anatomy (heart failure, valvular heart disease, known coronary artery disease, atrial fibrillation); a history of cardiovascular events (heart attack, stroke); or previous spironolactone treatment were not included in this study.
Eventually, 15 patients with diagnosed unilateral aldosterone-producing adenoma (APA) underwent adrenalectomy. Adenomas were histologically confirmed in all the cases. The effect of adrenalectomy was verified by normalisation of ARR, plasma potassium and a significant decrease or normalisation of blood pressure.
Conservative therapy with spironolactone was initiated in the 16 remaining patients (nine of them had idiopathic aldosteronism; seven patients had unsuccessful AVS or refused adrenalectomy). The initial dose of spironolactone was 50 mg per day.
Each participant provided written informed consent and the study was approved by the local ethics board.
Follow-up
All the participants were prospectively followed up. At three and 12 months after adrenalectomy or initiation of spironolactone treatment, their clinical status, blood pressure and laboratory tests were checked in our centre. In conservatively treated patients, we titrated the dose of spironolactone to maintain blood pressure under 140/90 mmHg (mean dose of spironolactone was 50 mg per day, in a range of 12.5–75 mg per day). Spironolactone was not tolerated even in small doses in three patients in the conservatively treated group. These patients were switched to eplerenone therapy and excluded from our study. In another three patients, dose reduction to 25 mg was sufficient to reduce negative side effects. Otherwise, spironolactone was tolerated well. Other antihypertensive therapy was adjusted according to the physician’s judgement in patients with persistent hypertension in both groups during regular 12-month check-ups at our centre.
At a median follow-up of 64 months (range 51–76 months), all the patients were finally examined in our clinic including clinical status assessment, laboratory tests, 24-hour blood pressure monitoring and echocardiography.
Blood pressure monitoring
We performed office blood pressure measurement in a sitting position with a standard mercury sphygmomanometer, following the European Society of Hypertension (ESH) recommendations. 22 All individuals also underwent 24-hour ambulatory blood pressure monitoring (ABPM) using a SpaceLabs device (SpaceLabs 90207; SpaceLabs, Richmond, WA, USA), which was set to measure blood pressure every 20 minutes during the day period (from 6 a.m. to 10 p.m.) and every 30 minutes during the night (from 10 p.m. to 6 a.m.).
Echocardiography
M-mode, two-dimensional and Doppler echocardiograms were recorded according to a standard protocol. With the patient lying down in the left lateral decubitus position, the LV end-diastolic (LVED) and LV end-systolic dimension (LVES), interventricular septum (IVS), and posterior wall thickness (PWT) were measured from the parasternal long axis (PLAX) projection using M-mode echocardiography, according to the recommendations of the American Society of Echocardiography. Relative wall thickness (RWT) was calculated as 2 × (PWT/LVED). We estimated the LV mass using the formula from Lang et al. 26
The LV mass was normalised to body surface area and, because of higher average values of the body mass index (BMI), also to the height2.7 index. LV hypertrophy was determined as the LV mass index (LVMI) ≥53 g/m2.7 (≥125 g/m2 – which is a cut-off value of LVMI normalised to body surface area). LV hypertrophy was further evaluated as either concentric in patients with RWT ≥0.42 or eccentric in the rest of the hypertrophy cases. Concentric remodelling was defined as RWT ≥0.42 in the absence of LV hypertrophy.26,27
Parameters of LV diastolic function were obtained using transmitral flow evaluation by Doppler echocardiography and tissue Doppler imaging of medial and lateral mitral annulus movement.
All the echocardiographic measurements were obtained by the same investigator.
Statistical analysis
Data were analysed using Statistica software (StatSoft, Tulsa, OK, USA). The results are expressed as the mean ± SD or, in the case of hormonal examination results, as the median with an interquartile range. Differences between the groups were tested by Student’s t test, variations within the groups during the follow-up by t test for dependent variables. The χ2 test was used for categorical data. All tests were considered statistically significant at the level of p < 0.05.
Results
A total of 15 patients with confirmed PA were diagnosed with aldosterone-producing adenoma and underwent adrenalectomy. In the other 16 PA patients, conservative treatment with spironolactone was initiated (nine of them had confirmed idiopathic aldosteronism; unsuccessful AVS, or refusal of further investigation did not allow to determine exact diagnosis in seven people).
At baseline, patients indicated for adrenalectomy and those indicated for conservative treatment had similar basic clinical characteristics including their age, height, weight, BMI and blood pressure levels, as shown in Table 1. The known duration of hypertension was slightly, although nonsignificantly, longer in the spironolactone group. Blood pressure levels were comparable between the two groups; however, patients indicated for adrenalectomy used a lower number of antihypertensives (p < 0.01). All details on antihypertensive treatment are shown in Table 2.
Baseline clinical characteristics.

24h: 24-hour; BP: blood pressure.
Antihypertensive treatment.

ACE: angiotensin-converting enzymes. ap < 0.05, bp < 0.01 vs. adrenalectomy.
Table 3 summarises the clinical and laboratory parameters in both groups at baseline and at the end of the follow-up period. Both the surgical and conservative approach significantly reduced blood pressure levels. Adrenalectomy cured hypertension (i.e. patients had normal blood pressure without any antihypertensive medication) in five cases (33%), and significantly improved blood pressure control in the others; only two patients did not achieve normal blood pressure with combined antihypertensive therapy in this period. In the conservative group, adding spironolactone to combined treatment led to blood pressure normalisation in 12 cases (75%) with a significant drop in blood pressure in the rest of the patients.
Clinical characteristics and laboratory data of study population.
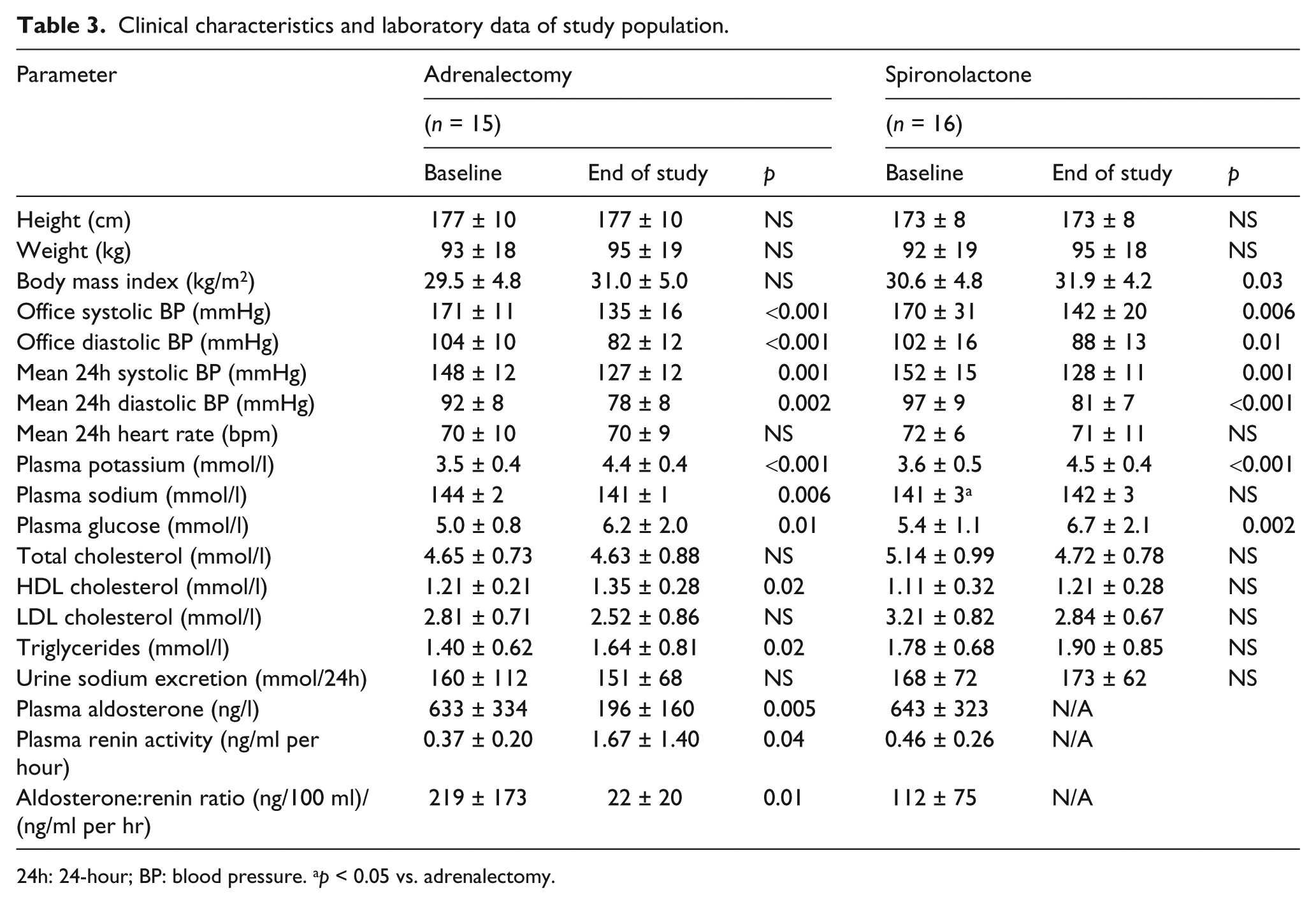
24h: 24-hour; BP: blood pressure. ap < 0.05 vs. adrenalectomy.
Both adrenalectomy and spironolactone treatment significantly increased plasma potassium levels (from 3.5 ± 0.4 to 4.4 ± 0.4 mmol/l and from 3.6 ± 0.5 to 4.5 ± 0.4 mmol/l, respectively, p < 0.001); patients after adrenalectomy also showed lower plasma sodium levels (144 ± 2 vs. 141 ± 1 mmol/l, p = 0.006). At the end of the follow-up, fasting plasma glucose increased in both groups (5.0 ± 0.8 vs. 6.2 ± 2.0 mmol/l, p = 0.01 and 5.4 ± 1.1 vs. 6.7 ± 2.1 mmol/l, p = 0.002) as two patients in each group had newly impaired glucose tolerance and one patient after adrenalectomy and two patients on spironolactone developed diabetes mellitus.
Table 4 shows the basic echocardiographic measurements obtained during the long-term follow-up. Both adrenalectomy and spironolactone treatment improved the E/e′ ratio as a parameter of LV diastolic filling, even though this ratio was significantly lower in patients indicated for adrenalectomy at baseline.
Echocardiographic findings.

LVED: left ventricle end-diastolic; LVEDi: left ventricle end-diastolic dimension index; LVES: left ventricle end-systolic dimension; LVESi: left ventricle end-systolic dimension index; IVSd: diastolic interventricular septum; PWd: posterior wall in diastole; RWT: relative wall thickness; ap<0.01 vs. adrenalectomy.
In both groups, specific treatment led to a significant decrease in both end-diastolic (from 53.7 ± 7.0 mm to 50.7 ± 5.6 mm after adrenalectomy and from 54.7 ± 4.0 mm to 51.3 ± 4.8 mm on spironolactone, p = 0.04, p = 0.01) and end-systolic LV cavity diameters (from 36.7 ± 7.5 mm to 32.0 ± 6.1 mm after adrenalectomy and from 34.6 ± 3.2 mm to 32.0 ± 4.8 mm on spironolactone, p = 0.03, p = 0.01). The reduction of IVS thickness was apparent only in patients after adrenalectomy (11.3 ± 1.1 mm vs. 10.1 ± 1.6 mm, p = 0.01), much like the drop in PWT (10.7 ± 1.5 mm vs. 9.4 ± 1.5 mm, p = 0.03) and LV mass index (50.2 ± 12.1 g/m2.7 vs. 39.0 ± 8.6 g/m2.7, p = 0.004). Despite a similar trend, the reduction of LV mass index was not significant in patients treated with spironolactone. A trend to lower LV mass after spironolactone treatment was caused predominantly by the diminution of the LV cavity, which was also reflected in the increase of RWTs (p = 0.05).
As shown in Figure 1, at baseline, LV hypertrophy was present in 47% of patients before adrenalectomy, and in 56% of patients on spironolactone therapy. The eccentric type of hypertrophy prevailed over the concentric one in both groups. Adrenalectomy successfully reversed LV hypertrophy in all patients except one case (p = 0.014). Spironolactone was less effective in the reduction of LV mass: LV hypertrophy persisted in 31% of medically treated patients (for details, see Figure 1). By reducing LV cavity diameters, the average RWT increased after the treatment with spironolactone (from 0.37±0.06 to 0.41±0.07, p = 0.05) and eccentric hypertrophy even transformed into the concentric type in two cases.

Prevalence of left ventricle (LV) hypertrophy.
Comparing the effect of both methods of treatment on LV remodelling, adrenalectomy was significantly more effective in reducing the thickness of the LV posterior wall (p = 0.03). A similar, borderline-significant trend was observed for IVS thickness and LV mass index (p = 0.07), while the influence on the diminution of the LV cavity was comparable in both groups (see Figure 2).

Comparison of effects of spironolactone or adrenalectomy on left ventricle (LV) parameters.
Discussion
In this study, we evaluated the long-term effects of specific treatment with adrenalectomy or spironolactone on basic echocardiographic parameters of the LV in patients with PA. Our results indicate that, even though both of these methods can manage the control of hypertension, the surgical approach is more effective in the reduction of LV hypertrophy. After adrenalectomy, the decrease in LV mass seems to be caused by the reduction of both wall thicknesses and LV cavity diameters, whereas conservative treatment with spironolactone leads only to a diminution of the LV cavity with no signs of wall attenuation. Nevertheless, both methods improved the diastolic function of the LV.
In the long-term follow-up, blood pressure markedly decreased both in the surgical and conservative treatment groups. In patients after adrenalectomy, this decrease occurred despite the reduction of antihypertensive treatment, which was even completely discontinued in 33% of these patients. Similarly to previous observations, 28 surgery did not cure hypertension in most patients, and two-thirds of them still required antihypertensives. 29 This can be explained by coexisting or newly developed essential hypertension during the long follow-up period; moreover, long-term excess of aldosterone could lead to vascular remodelling causing persistent hypertension even after normalisation of aldosterone concentrations. 30 A comparable blood pressure reduction was observed also after the initiation of spironolactone treatment, although the number of antihypertensive drugs needed to achieve blood pressure control did not change significantly despite a dose reduction in some of them.
A growing body of evidence connects aldosterone excess to the development and progression of cardiovascular disease, clearly independent of blood pressure levels. Hypertension caused by this frequent endocrine disorder has been shown to be associated with a higher LV mass compared to that in essential hypertension,14–16 although this finding has not been supported by all authors.17,18 These discrepancies can possibly be explained by the diversity of the studied cohorts with different severity and duration of hypertension, and different treatment or sex-related variations among the patients involved. Experimental animal studies have proposed that the excess of aldosterone can induce extracellular matrix and collagen deposition, 31 especially in the presence of high dietary salt intake. 32 Stimulation of fibroblast proliferation and collagen synthesis might be related to the activation of mineralocorticoid receptors in human cardiomyocytes, inducing inflammatory process and specific ionic movements, modulated also by the interaction with the angiotensin, bradykinin and endothelin systems.10,33 The demonstration of a regression of LV mass after specific treatment would provide additional evidence of the causal role of aldosterone-mediated excessive activation of mineralocorticoid receptors in the development of LV hypertrophy. Although several studies on limited cohorts showed a reduction in LV mass after adrenalectomy due to aldosterone-producing adenoma over short-term follow-up,15,21 there is still a lack of research comparing the cardiovascular effects of surgical and medical treatment of PA. The first report concerning both the pharmacologic treatment and surgery by Catena et al. 28 has put forward that both of these approaches can reduce LV mass in long-term follow-up; however, these changes occurred earlier after adrenalectomy than on spironolactone. In both groups, the reversal of LV hypertrophy was caused predominantly by LV wall attenuation. In contrast, the very recent long-term study by Rossi et al., 34 involving the as-yet largest cohort of patients with PA treated by adrenalectomy or spironolactone, reported that the LV mass index and the rate of LV hypertrophy decreased through LV inward remodelling and diminution of LV cavity diameters, with no observed effect of specific treatment on the wall thicknesses. The number of patients using angiotensin-converting enzyme inhibitors (ACEis) or angiotensin receptor blockers (ARBs) in both groups decreased at the end of the study in comparison with baseline (Table 2). It is questionable whether the lower rate of dual renin-angiotensin-aldosterone system (RAAS) blockade could explain the insufficient effect on regression of LV walls thickness. Grandi et al. 35 reported a better effect of dual RAAS blockade (ACEi + ARB vs. ACEi + Ca antagonist) in hypertensive patients with concentric hypertrophy. On the other hand, in the Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET), 36 the prevalence of LV hypertrophy was as similar to dual blockade as with monotherapy despite the lower blood pressure with dual RAAS blockade. Similarly, in the Aliskiren in Left Ventricular Hypertrophy (ALLAY) study, 37 the LV mass reduction with the combination of losartan + aliskiren was not significantly different from losartan monotherapy, independent of blood pressure lowering. Therefore, the benefits of dual RAAS blockade considering LV hypertrophy regression remain uncertain.
Our previous research indicates that patients with PA have significantly larger LV cavity diameters and more frequent eccentric subtype of hypertrophy than those with essential hypertension. 19 As we have suggested, these differences might result from the well-known aldosterone effect on sodium and water reabsorption in distal renal tubules and the increase in plasmatic volume resulting in the preload of the LV. This interpretation seems to be supported by studies of the LV pressure-volume curves in rats after aldosterone infusion 38 and also by human studies showing an increase in brain natriuretic peptide (BNP) levels in patients with PA. 39 Increased LV volumes compared with essential hypertension were confirmed also in a smaller group of patients with PA examined by magnetic resonance imaging (MRI) as a potentially more accurate method than commonly used echocardiography. 40
The present study shows that both adrenalectomy and mineralocorticoid receptor blockers can reverse the enlargement of the LV cavity during long-term follow-up, probably through the reduction of plasma volume and LV preload. In spite of the significant and similar blood pressure drop in both groups, however, only surgery led to a successful reduction in the thickness of LV walls. This suggests that the treatment with spironolactone was unable to induce a complete regression of the adverse effects of high aldosterone in PA patients. A possible explanation for this adverse effect is the fact that correctly indicated adrenalectomy leads to a normalisation of hormonal proportions in the renin-angiotensin-aldosterone axis, whereas in conservatively treated patients the levels of circulating aldosterone remain elevated with the possibility of escape phenomenon. Alternatively, as experimental studies have suggested, a possible involvement of nongenomic effects of aldosterone can contribute to myocardial damage.4,41 The finding of the insufficient effect of conservative treatment of PA is in agreement with the abovementioned extensive study by Rossi et al. 34 but in contradiction to previous observations. 28 One of the possible explanations for these divergent results is that the effect of spironolactone can be dependent on disease duration. Secondly, the dose of spironolactone needed to reverse myocardial thickening can be higher than the dose normalising blood pressure and volume overload. On the other hand, a regression of LV hypertrophy has been observed by Ori et al., 42 even after treatment with low doses of spironolactone, however, with the inclusion of patients with low renin hypertension. Further investigation will be needed to prove whether the effect on reversing myocardial damage can be improved by an earlier initiation of spironolactone treatment or a dose increase.
Considering the effects of spironolactone, we could not prove the expected reduction in the left atrial dimension to accompany the reduction in the LV cavity. Unfortunately, the left atrial diameter from PLAX projection was used as a single, and potentially inaccurate, parameter. The estimation of the left atrial volume would be more appropriate; however, this measurement was not available at baseline.
We are aware of several limitations of our study. First and most important is the limited number of patients involved. The statistical power of this study is not sufficient to prove a significant reduction of LV mass in the spironolactone group. However, even from the observed trends we can suggest that this – though nonsignificant – decrease in LV mass was caused by the diminution of the LV cavity, not by the attenuation of the LV walls. Secondly, we cannot be sure about the compliance with spironolactone therapy in all the patients, as it has been shown that compliance with antihypertensive treatment is rather poor. 43 On the other hand, we found a significant decrease in blood pressure and an increase in plasma potassium levels which can be explained only by the spironolactone effect.
Conclusions
This study was designed to compare the effects of adrenalectomy and spironolactone therapy in patients with PA. It revealed that although both methods can induce a long-term decrease in blood pressure and improve LV diastolic filling, adrenalectomy is more effective in LV hypertrophy reduction and reverses both LV wall thickening and LV cavity enlargement. Spironolactone treatment resulted in the reduction of the size of the LV cavity only. The mechanisms of the exact aldosterone effect on myocardial remodelling remain unclear and are worthy of further investigation.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by grant project NT/14155-3/2013 from the Ministry of Health of the Czech Republic.