
Abstract
Objective:
We analyzed the efficacy and safety of combination therapy of high-dose losartan (100 mg/day) and hydrochlorothiazide (HCTZ, 12.5 mg/day) compared with those of the combination of high-dose telmisartan (80 mg/day) and HCTZ (12.5 mg/day).
Methods:
Forty hypertensive patients who received a combination of high-dose telmisartan and HCTZ were enrolled. We applied a changeover strategy with switching from a combination of high-dose telmisartan and HCTZ to high-dose losartan and HCTZ. We divided the patients into two groups; those who achieved the target blood pressure (controlled group) and those who did not reach the target blood pressure (uncontrolled group) before the changeover and performed further analysis.
Results:
The uncontrolled group showed a significant decrease in systolic blood pressure (SBP) (143±12 mmHg to 126±11 mmHg at three months). In addition, serum uric acid significantly decreased in all subjects, and in each of the controlled and uncontrolled groups. There were no significant changes in other biochemical parameters, such as potassium and hemoglobin A1c, at three months after the changeover in all subjects.
Conclusion:
Combination therapy with high-dose losartan and HCTZ was superior to the combination of telmisartan and HCTZ with respect to significant decreases in systolic blood pressure and serum uric acid in hypertensive patients.
Introduction
Combinations of angiotensin II type 1 receptor blockers (ARBs) and thiazide diuretics are recommended by various guidelines for the treatment of high blood pressure.1,2 Most patients with hypertension require two or more drugs to achieve their target blood pressure (BP). 3 In fact, large-scale clinical trials have shown that thiazide diuretics and/or calcium channel blockers are frequently added to ARBs to achieve adequate BP control. 4 Nine kinds of single-pill fixed-dose combinations of ARBs and diuretics are available for clinical use in Japan (Table 1). The combination of high-dose telmisartan (80 mg/day) and hydrochlorothiazide (HCTZ, 12.5 mg/day) (Micombi®BP) has the strongest BP-lowering effect. 5 We previously used a changeover design in which the patients were switched from high-dose ARBs or a combination of medium-dose losartan (50 mg/day) and HCTZ to high-dose telmisartan and HCTZ. 6 Although we found that high-dose telmisartan and HCTZ induced a significant reduction of BP at three months after changeover, the combination therapy resulted in a significant increase in serum uric acid (UA). In particular, an elevation of serum UA was observed in patients who were switched from a combination of medium-dose losartan and HCTZ to high-dose telmisartan and HCTZ.
Nine kinds of single-pill, fixed-dose combination of angiotensin II receptor blockers (ARBs) and diuretics in Japan.

It is still controversial whether a higher level of serum UA is a risk factor for arteriosclerosis and coronary artery disease. Although a relationship between serum UA and cardiovascular events was not observed in the Framingham study, 7 such relationships have been demonstrated in some studies.8,9 Moreover, in a subanalysis of data from the Japanese Coronary Artery Disease Study, a high level of UA was shown to be an independent predictor of all events, including cardiovascular events and all-cause mortality. 10 In a prospective, randomized trial, allopurinol was shown to decrease C-reactive protein and reduce cardiovascular and hospitalization risk in patients with estimated GFR (eGFR) <60 ml/min. 11 Among ARBs, although both losartan and telmisartan significantly blocked urate transporter 1 (URAT1) in in vitro experiments,12,13 only losartan showed uricosuric action through the inhibition of URAT1 in humans. 14
We hypothesized that a combination of high-dose losartan and HCTZ could produce similar reduction in BP and significant decrease in serum UA compared with a combination of high-dose telmisartan and HCTZ. Therefore, we analyzed whether a changeover with switching from a combination of high-dose telmisartan and HCTZ to high-dose losartan (100 mg/day) and HCTZ would be more efficacious and safe for hypertensive patients.
Methods
Study design
Forty hypertensive patients who received a combination of high-dose telmisartan and HCTZ were enrolled. We applied a changeover strategy with switching from Micombi®BP (a single-pill fixed-dose combination of telmisartan (80 mg/day) and HCTZ (12.5 mg/day)) to Preminent® (a single-pill fixed-dose combination of losartan (50 mg/day) and HCTZ (12.5 mg/day)) + losartan (50 mg/day). Twenty-four patients (60%) received Micombi®BP in the morning and the rest of patients (40%) received it in the evening. After changeover, we did not change the administration time in all patients.
We divided the patients into two groups: those who achieved the target BP (controlled group) and those who did not reach the target BP (uncontrolled group) before the changeover, and performed further analysis according to the Japanese Society of Hypertension Guidelines 2009. 1 We excluded patients with secondary hypertension, heart failure of NYHA grade III or IV, moderate to severe liver dysfunction (defined as aspartate aminotransferase and alanine aminotransferase levels of more than three-fold the normal ranges), renal dysfunction (defined as a serum creatinine (Cr) level of more than 2.0 mg/dl), pregnancy, or a history of allergy to losartan. The protocol in this study was approved by the ethics committee of Fukuoka University Hospital, and all subjects gave their informed consent to participate.
Evaluation of clinical parameters
We analyzed seated office systolic BP (SBP), diastolic BP (DBP) and pulse rate (PR), body weight (BW), and blood and urinary levels of biochemical parameters at baseline and at three months after changeover. BP was determined as the mean of two measurements obtained in an office setting by the conventional cuff method using a mercury sphygmomanometer after at least 5 min of rest. All of the blood and urinary samples were collected in the morning after the patients had fasted overnight. Data regarding serum levels of biochemical parameters, such as high-density lipoprotein-cholesterol (HDL-C), low-density lipoprotein-cholesterol (LDL-C), triglycerides (TG), UA, Cr, eGFR, brain natriuretic peptide (BNP), fasting blood glucose (FBS), hemoglobin A1c (HbA1c), sodium (Na), potassium (K), albumin (Alb), urinary (U)-UA, U-Cr, the ratio of U-UA to U-Cr (U-UA/U-Cr), and the fractional excretion of UA (FEUA, U-UA × serum Cr/serum UA × U-Cr) were collected in all patients. Body mass index (BMI) was calculated as weight (kg)/height (m)2.
The characteristics of the patients, with regard to history of dyslipidemia (DL), diabetes mellitus (DM), hyperuricemia (HU), smoking status and medication use, were obtained from medical records. Patients who had a current SBP/DBP ≥ 140/90mmHg or who were receiving antihypertensive therapy were considered to have hypertension. Patients with LDL-C ≥ 140 mg/dl, TG ≥ 150 mg/dl and/or HDL-C < 40 mg/dl, or who were receiving lipid-lowering therapy were considered to have DL. DM was defined using the American Diabetes Association criteria or the use of a glucose-lowering drug. HU was defined as a serum UA level of ≥ 7.0 mg/dl. Chronic kidney disease (CKD) was defined as an eGFR level of < 60 ml/min per 1.73 m2.
Statistical analysis
Statistical analysis was performed using the StatView statistical software package (StatView 5; SAS Institute Inc., Cary, NC, USA). Data are shown as the mean ± standard deviation (SD). Categorical variables were compared between groups by a chi-square analysis. The significance of differences between mean values was evaluated by paired and unpaired t-tests or one-way analysis of variance followed by Fisher’s protected-least-significant-difference test, as appropriate.
Results
Patient characteristics
Table 2 shows the characteristics of the 40 patients, who included nine (23%) males. No patients withdrew from the study. The prevalence of DL, DM, HU and CKD was 63%, 13%, 35% and 40%, respectively. In addition, the percentage use of calcium channel blocker (CCB), β-blocker and α-blocker was 98%, 35% and 10%, respectively. There were no significant differences in the baseline patient characteristics between the controlled and uncontrolled groups. We did not change these medications throughout the study period.
Baseline patient characteristics.
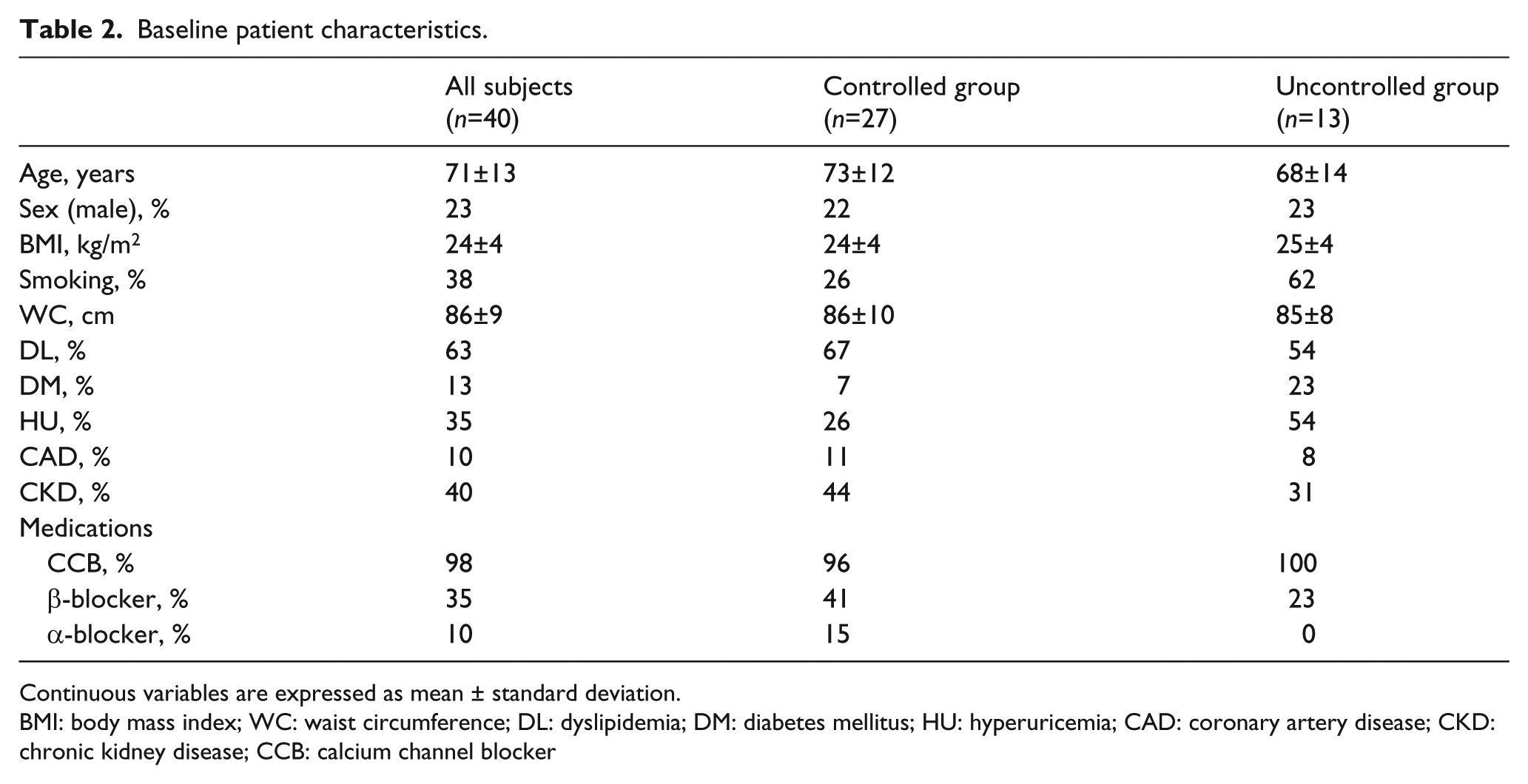
Continuous variables are expressed as mean ± standard deviation.
BMI: body mass index; WC: waist circumference; DL: dyslipidemia; DM: diabetes mellitus; HU: hyperuricemia; CAD: coronary artery disease; CKD: chronic kidney disease; CCB: calcium channel blocker
Changes in BP and PR
In all patients, SBP/DBP and PR at baseline were 126±17/69±11 mmHg and 69±9 beats/min, respectively (Figure 1). SBP significantly decreased from 126±17 mmHg at baseline to 119±13 at three months after changeover in all subjects. In particular, the uncontrolled group showed a significant decrease in SBP (143±12 mmHg to 126±11 mmHg at three months). There were no significant changes in DBP or PR during the study period.

Changes in systolic blood pressure (SBP)/diastolic blood pressure (DBP) and pulse rate (PR) in all subjects (n=40), and in the controlled (n=27) and uncontrolled groups (n=13) at zero and three months.
Changes in biochemical parameters
As shown in Table 3, there were no significant changes in biochemical parameters such as serum blood urea nitrogen (BUN), Cr, K, HbA1c, BNP and lipid profile in all subjects, or in the controlled and uncontrolled groups.
Change in biochemical parameters in all subjects, controlled and uncontrolled groups.

BUN: blood urea nitrogen; Cr: creatinine; eGFR: estimated glomerular filtration rate; Na: sodium; K: potassium; TG: triglyceride; LDL-C: low density lipoprotein cholesterol; HDL-C: high density lipoprotein cholesterol; FPG: fast plasma glucose; HbA1c: hemoglobin A1c; BNP: brain natriuretic peptide; U-Alb: urinary albumin; UA: uric acid; FEUA: fractional excretion of UA.
Changes in serum UA, U-UA/U-Cr and FEUA in all subjects, and in the controlled and uncontrolled groups
The combination of high-dose losartan and HTCZ significantly decreased serum UA after three months in all subjects, and in the controlled and uncontrolled groups (Figure 2), whereas there were no changes in U-UA/U-Cr or FEUA in all subjects, or in the controlled and uncontrolled groups (Table 3).

Changes in serum uric acid (UA) in all subjects (n=40), and in the controlled (n=27) and uncontrolled groups (n=13) at zero and three months.
Changes in serum UA, K and HbA1c between sub-groups
The normal UA, K and HbA1c values at our University Hospital are 5.0–7.0 mg/dl, 3.5–5.0 mEq/l and 4.6–5.6%, respectively. Therefore, we divided all of the patients into two groups according to each normal range described as previously. 6 Our ‘relatively high UA group’ was defined as UA > 6.0 mg/dl, and the ‘relatively low UA group’ was defined as 6.0 mg/dl ≥ UA. Our ‘relatively high K group’ was defined as K > 4.3 mEq/l, and the ‘relatively low K group’ was defined as 4.3 mEq/l ≥ K. Our ‘relatively high HbA1c group’ was defined as HbA1c > 5.1%, and the ‘relatively low HbA1c group’ was defined as 5.1% ≥ HbA1c. In the relatively low and high UA groups, their values at three months were significantly less than those at baseline (Figure 3). In the relatively high K group, although the level of K at three months was significantly less than that at baseline, the average value was still within the normal range (K=4.3 mEq/l at three months). Moreover, there were no significant changes after three months in either the relatively low K group or the low and high HbA1c groups.

Changes in uric acid (UA) (a) (UA > 6.0 mg/dl vs. 6.0 mg/dl ≥ UA), potassium (K) (b) (K > 4.3 mEq/l vs. 4.3 mEq/l ≥ K) and hemoglobin A1c (HbA1c) (c) (HbA1c > 5.1% vs. 5.1% ≥ HbA1c).
Discussion
In the present study, the combination of high-dose losartan and HTCZ significantly reduced SBP and serum UA after the switch from high-dose telmisartan and HTCZ. Moreover, there were no serious adverse effects in any of the patients.
High-dose losartan and HTCZ significantly reduced SBP. BP control is the best strategy for achieving remarkable clinical benefits with regard to cardiovascular and renal protection. Since the change in SBP using high-dose losartan and HTCZ was −7 mmHg in all subjects, SBP reduction should provide tremendous clinical benefits. For example, a 2 mmHg reduction in SBP should provide a 10% lower incidence of stroke mortality and about a 7% lower incidence of mortality from coronary artery disease or other vascular causes in middle age. 15
The synergistic effect of the combination of high-dose losartan and HTCZ may be stronger than that with high-dose telmisartan and HTCZ. In a previous study, 12.5 mg/day of HCTZ significantly increased plasma renin activity (PRA). 16 In this case, the blockade of the activation of PRA induced by HTCZ with high-dose losartan may be stronger than that with high-dose telmisartan. Since the combination of medium-dose losartan (50 mg/day) and HTCZ had the same depressor effect as that of medium-dose telmisartan (40 mg/day) and HCTZ, 17 we did not expect that a changeover from high-dose telmisartan and HTCZ to high-dose losartan and HTCZ would be a useful strategy for inducing a more significant reduction in SBP.
In this study, high-dose losartan and HTCZ significantly decreased serum UA after a switch from high-dose telmisartan and HCTZ. Losartan has been shown to have uricosuric action via URAT1 in hypertensive patients. 14 Hamada et al. reported that losartan and HCTZ increased the ratio of UA clearance to creatinine clearance (CUA/Ccr) in patients with a serum UA above 5.5 mg/dl, whereas telmisartan and HCTZ significantly reduced CUA/Ccr. 17 Unexpectedly, U-UA/U-Cr and FEUA did not change after the changeover to high-dose losartan and HTCZ. The classification of HU into one of two types (i.e. the overproduction of UA or a decrease in the urinary excretion of UA) based on a 60-min spot urine or 24-h urine collection in outpatients is important for determining the treatment strategy, 18 but there are no standardized methods available. Thus, further studies will be needed to resolve this issue.
Benson et al. indicated that telmisartan activated peroxisome proliferator-activated receptor (PPAR)-γ, which may improve insulin sensitivity, 19 whereas losartan did not activate PPAR-γ. 20 Telmisartan may be useful in hypertensive patients with insulin resistance or DM. 21 Nonetheless, in this study, the levels of HbA1c and FBS did not change at three months after a changeover from high-dose telmisartan and HTCZ to high-dose losartan and HTCZ. Telmisartan-induced activation of PPAR-γ may not be clinically important in this study, and this result was consistent with a previous report. 22
Zillich et al. reported that the treatment of thiazide-induced hypokalemia might reverse glucose intolerance. 23 Although the level of K at three months after changeover was significantly decreased in the relatively high K group, the average value (K=4.3 mEq/l at three months) was still within the normal range and was clinically ignorable. Therefore, the level of K may not influence glucose intolerance.
Study limitations
This study has three important limitations. First, the sample size is relatively small, which limits our ability to determine significance. Second, we applied a changeover with switching from high-dose telmisartan and HTCZ to high-dose losartan and HTCZ. However, a crossover study would be preferable. Third, we applied a changeover strategy with switching from one tablet (Micombi®BP) to two tablets (Preminent® + losartan). Twenty-four patients received Micombi®BP in the morning and the rest of patients received it in the evening before changeover, whereas we did not change the administration time in all patients after changeover. The numbers of tablets and administration time may affect drug adherence and BP lowering effects.
Conclusions
The combination of high-dose losartan and HTCZ significantly reduced SBP and decreased serum UA after three months. In addition, there were no serious adverse effects in any of the patients.
Footnotes
Conflict of interest
KS, SM and YU have received grants and lecture honoraria from MSD, Co. Ltd. KS is a Chief Director and SM is a Director of NPO Clinical and Applied Science, Fukuoka, Japan. KS has an Endowed Department of ‘Department of Molecular Cardiovascular Therapeutics’ supported by MSD, Co. Ltd. SM and YU belong to the Department of Molecular Cardiovascular Therapeutics supported by MSD, Co. Ltd.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.