
Abstract
Hypothesis / introduction:
Prior studies have denoted gender differences in the expression and therapeutic benefits of hypertension treatment and clinical outcomes. This study documents for the first time gender differences in the expression of blood and urine angiotensin peptides in normotensive Afro-Caribbean Barbadians (25 males; 26 females).
Materials and methods:
Participants provided clinical anthropometric measurements, 24h ambulatory blood pressure and urine collections, and a blood sample for measurements of angiotensin peptides.
Results:
Plasma renin activity ranged between 0.00 and 3.00 ng/ml/h. Plasma and urinary Ang II were comparable in both genders, while urinary Ang-(1-7) was greater in females (p<0.05). Urinary Ang-(1-7) and office systolic blood pressure correlated significantly in females only (p<0.01), while plasma Ang-(1-7) and Ang II correlated significantly in both genders (p>0.05).
Conclusions:
A shift in the balance between Ang II and Ang-(1-7) and their respective pressor and depressor axes might be markers of the cardio-renal protective mechanisms that may be present in females of Afro-Caribbean descent.
Introduction
Cardiovascular disease (CVD) increases with age, but males and females differ substantially in the manifestation of these conditions. 1 Males suffer from more life-threatening diseases such as heart disease, while females suffer from more non-fatal chronic conditions. Also, ethnic disparities in cardiovascular health are in part influenced by the interplay between genetics and environmental factors. 2
A higher prevalence of hypertension exists in persons of African descent compared with other ethnic groups.3,4 Afro-Caribbean populations in the United Kingdom have a higher incidence of strokes and end-stage renal failure compared with Caucasians. 5 There is a real void of mechanistic studies to explain the increased susceptibility of populations of African descent to the development of hypertension. Studies have demonstrated reduced angiotensin converting enzyme 2 (ACE2) activity in pre-hypertensive subjects and similarly reduced ACE2 activity in diabetic and renal disease patients.6–8 Furthermore, low plasma renin activity (PRA) is more prevalent in persons of African descent than in persons of European descent. 9 In addition, a strong sex-driven blood pressure dimorphism has been documented in rats with increased tissue renin gene expression.10–12 In males, renal injury increases in parallel with increased activation of the renin–angiotensin–aldosterone system (RAAS) while the same is not readily found in females. 13 No previous study has characterized any gender differences in RAAS biomarkers in an Afro-Caribbean population. Therefore, we investigated the characteristics of RAAS biomarkers between genders in a normotensive Afro-Caribbean population that is genetically less diluted than other populations of African descent in Europe and North America. 14
Materials and methods
In total, 25 males and 26 females (age range of 21–55 years) of Afro-Caribbean origin were recruited from The University of the West Indies, Cave Hill Campus and the staff of the Hilton Resort. Subjects were asked to attend the clinic on two separate occasions. The Institutional Review Board of the University of the West Indies/Ministry of Health approved the study. Participants were asked to sign a consent form and fill out a pre-screening questionnaire. Upon the first visit, participants were provided with an ambulatory blood pressure monitor and a container to collect a 24h urine sample. During the second visit, anthropometric measurements and clinical blood pressure (BP) measurements were recorded, supine venous blood samples were collected, and urine samples were returned for analysis. Subjects with at least one of the following criteria were excluded from the study: high alcohol consumption [>14 unit’s females, 21 units males per week (1 unit = 8 g of alcohol)] and recreational drug use; smokers >1 year; Diabetes (diagnosed on fasting blood glucose); hypertension (on medication); clinically evident vascular disease or a body mass index (BMI) <18 kg/m2 or > 36 kg/m2.
The ambulatory blood pressure monitor (ABPM) (SpaceLabs Medical 90217-IQ, SpaceLabs Inc., USA) and automated blood pressure monitor [OMRON 705IT (HEM-759-E) Omron Corporation, Kyoto, Japan] were used to record 24 h ambulatory and office BP, respectively. Upon giving consent to participate in the study, subjects wore an ABPM for 24 h and underwent standard BP measurements in both seated and supine positions with the use of the OMRON 705IT. On day one, participants were given a demonstration of the accurate technique of applying the ABPM, after which the participant was instructed to wear the ABPM for 24 h. They were also given an activity sheet on which they documented their activities for the 24 h. ABPM was set in wake mode from 06:00–22:00 hours, with a reading taken every 30 minutes, and in sleep mode from 22:00–06:00 hours with a measurement taken every hour. On day two, a registered nurse or physician took office seated and supine BP measurements. Participants were instructed to sit quietly for 30 minutes, then 3–5 consecutive BP readings were recorded at 5-minute intervals. Participants were then required to lie in a supine position for 30 minutes. This was followed by 3–5 consecutive BP measurements every 5 minutes. Average BP readings were calculated and expressed in the form of mean ± standard deviation (SD).
All volumes of urine and blood samples were recorded. Samples were submitted to the Hypertension and Vascular Disease Center, Wake Forest University Health Sciences, for analysis of the RAAS peptides in plasma and urine. The 24 h urine samples were collected to measure volume, creatinine, electrolytes, and urinary content of angiotensin II (Ang II) and angiotensin-(1-7) (Ang-(1-7)). Plasma and urinary concentrations of angiotensin peptides and PRA were processed in duplicates for radioimmunoassay, as previously described in detail elsewhere.15,16 Briefly, venous blood was collected in EDTA tubes containing a cocktail of protease inhibitors including 0.44 mM 1,20 ortho-phenanthroline monohydrate (Sigma, St. Louis MO.), 0.12 mM pepstatin (Peninsula Labs, Belmont CA), and 1 mM Na p-hydroxymercuribenzoate (Sigma, St. Louis MO), as described by us elsewhere.15,16 Recoveries of radiolabeled angiotensins added to the sample and followed through the extraction were 92% (n=23). The minimum detectable levels of the assays were 0.9 fmol (0.8 pg)/tube. The intra-assay coefficient of variation is 12% for Ang II and 8% for Ang-(1-7). Collection of the urine specimens was accomplished in a plastic container to which 20 ml of 6N HCl had been added as a preservative. Subjects were instructed to gently agitate the container after each urine void and to keep the container throughout the 24 h collection period inside a plastic ice chest. Urine was extracted using Sep-Pak columns (Waters Associates, Watford, Hertfordshire, England) activated with 5 ml sequential washes of a mixture of ethanol:water:4% acetic acid (83:13:4), methanol, ultra pure water, and 4% acetic acid. The sample was applied to the column, washed with ultrapure water an acetone, and eluted with two 1 ml and one 1.5 ml washes of a mixture of ethanol:water:4% acetic acid. The weight of the eluate was recorded, and from the total eluate two 2 ml aliquots were transferred into conical bottom polystyrene tubes and dried. The eluted sample was reconstituted into a Tris buffer with 0.1% bovine serum albumin. Ang-(1-7) was measured using the antibody described by us previously.17,18 Samples were corrected for recoveries as described by us elsewhere.17,18
The number of participants used in this study was based on a sample size calculation from a previously reported study describing changes in Ang-(1-7) in plasma and urine of normotensive and hypertensive patients. 17 The sample size calculation was done at a power of 80% and a confidence level of 95% with the noted effect size from the cited study. SPSS version 19 and Microsoft Excel 2007 were used to analyze the data to make inferences. Student’s t-test was used to identify statistical differences of the mean values at the 95% confidence level after verifying if the data were normally distributed by frequency distribution. Multiple regression analysis was used to determine correlations between the RAAS biomarker, urinary electrolytes and other variables.
Results
Demographics
There were 51 participants in the study (25 males; 26 females). Table 1 documents the demographic characteristics and BP variables of the 51 Afro-Caribbean subjects. Participants were relatively young with a tendency for females to be leaner compared with males. There were no differences in either the office or 24 h ambulatory BP averages in both males and females; in both genders, systolic and diastolic BPs were within the normal range of the JNC-7 guidelines (Table 1). The average 24 h ambulatory systolic BP % dip reading showed that female participants tended to have a marginally lower value compared with their male counterparts (Table 1).
Main characteristics of subjects included in the study.

SP: Systolic pressure; DP: Diastolic pressure. Values are means ± SD obtained from 26 female and 25 male normotensive subjects.
Angiotensin peptide analysis
Table 2 documents the values of RAAS variables obtained in the subjects. PRA, in 49 of the 51 participants, was within the range reported by others. 5 Outliers from the analysis of the RAAS variables in both genders were values outside of the range reported previously. 17 There was no effect of gender in the values of supine PRA. While plasma Ang II concentrations were 59% lower in male participants compared with females, the difference was not statistically significant (Table 2). Likewise, plasma concentrations of Ang-(1-7) and the plasma Ang-(1-7)/Ang II ratio (females: 0.52 ± 0.31; males: 0.72 ± 1.10, p>0.05) were comparable in both males and females (Table 2).
Renin–angiotensin system values in Afro-Caribbean Caribbean subjects.

Values are means ± SD of plasma and urinary markers of renin–angiotensin system activity and excretory function. Values for plasma Ang II and Ang-(1-7) concentrations are from 40 (20 females) and 42 (21 females) subjects, respectively. Other variables were obtained in all 51 subjects.
Urinary concentrations of Ang II were almost half the urinary Ang-(1-7) values recorded in the overall patient population (Table 2). In addition, plasma Ang II concentrations correlated significantly with plasma Ang-(1-7) concentrations in both females and males (Figure 1(a) and (b)). While gender does not impose any significant differences in BP levels and plasma content of RAAS biomarkers, urinary Ang-(1-7) concentrations in males were 19% below the values found in females (Table 2). These differences in urinary Ang-(1-7) content were associated with lower 24 h creatinine excretion rates in females. Urinary sodium and potassium concentrations are equivalent in both females and males (Table 2).

Scattergram of the relationship between plasma Ang II and Ang-(1-7) in females (a) and males (b). Ang II: Angiotensin II; Ang-(1-7): Angiotensin-(1-7). Note that the plotted data were derived after sorting plasma renin activity of the participants by increments of 0.1 ng/ml/h to compensate for intrinsic variability.
The comparatively lower Ang-(1-7) levels in the females’ urine prompted a further examination of additional differences in the relationship among measured variables. In order to compensate for intrinsic variability, data were sorted as a function of 0.1 ng/ml/h increments in PRA (range: 0.00–3.00 ng/ml/h). Table 3 summarizes the output of the multiple regression analysis for both genders. Significant correlations (p<0.05) are denoted in bold figures. The regression analysis shows the existence of differences between the genders in measured variables which correlated significantly. Most of the significant associations were present in female subjects, whereas in males significant correlations were limited to plasma Ang-(1-7) and plasma Ang II (r=0.62, Table 3), plasma Ang-(1-7) and ambulatory systolic BP (r=0.50, Table 3), urinary levels of Ang-(1-7) and creatinine (r=0.66, Table 3), and urinary potassium concentrations and systolic BP dip (r=-0.53, Table 3). In females, PRA is strongly correlated with BMI, waist circumference, office diastolic BP, plasma Ang II and urinary Ang-(1-7) concentrations as well as urinary creatinine content. Plasma Ang-(1-7) and plasma Ang II also correlated in the female participants (r=0.52, Table 3). Of interest is the strong correlation between plasma Ang II and the systolic pressure dip (r=0.90, Table 3) as well as the correlations between urinary Ang-(1-7) content and both office systolic (Figure 2(a) and (b)) and diastolic BPs.
Regression analysis of RAAS biomarkers and other variables in Afro-Caribbean Caribbean subjects.

BMI: Body mass index; WC: waist circumference; SBP: office systolic blood pressure; DBP: office diastolic blood pressure; ASP and ADP: ambulatory systolic and diastolic blood pressure, respectively; SPd: systolic blood pressure dip; Ang II: angiotensin II; Ang-(1-7): angiotensin-(1-7); UC: urinary creatinine. Regression coefficients depicting significant correlations at the 95% confidence level (p<0.05) are highlighted by
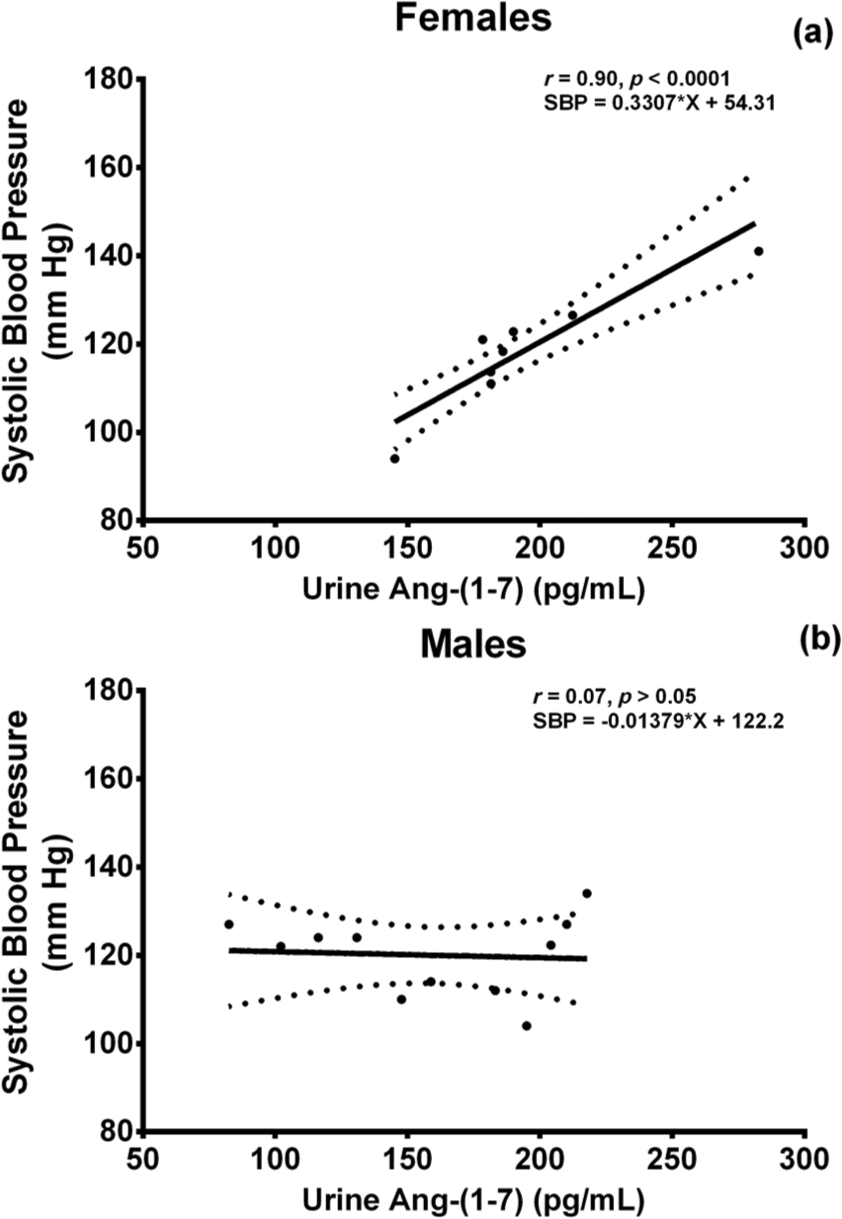
Office systolic blood pressure correlates with urinary Ang-(1-7) content in females (a) but not in male (b) normotensive subjects. Ang-(1-7): Angiotensin-(1-7). Note that the plotted data were derived after sorting plasma renin activity of the participants by increments of 0.1 ng/ml/h to compensate for intrinsic variability.
Discussion
The data generated from this study document important gender differences in the profile of RAAS peptides in normotensive Afro-Caribbean participants. Young black females of Afro-Caribbean descent showed lower urinary excretion rates of Ang-(1-7) and a higher urinary excretion rate of creatinine when compared with male participants. It must be noted however that the Ang-(1-7)/creatinine ratio in both genders were similar. This outlines a possible interplay between renal RAAS biomarker synthesis, regulation and gender phenotypes. In addition, females showed significant associations among office BP and urinary Ang-(1-7) as well as strong correlations of PRA with BMI, plasma Ang II and urinary Ang-(1-7). The demonstration of significant correlations in females but not males among urinary sodium excretion, waist circumference, urinary potassium excretion, and systolic BP suggests that young Afro-Caribbean women may be more prone to display phenotypes related to increased salt sensitivity of the BP.
It is well documented that hypertension, more prevalent in persons of African descent than persons of European descent, is disproportionally severe and associated with a higher rate of clinical complications. Although this excess disease burden has been attributed to external factors, such as access to care and higher social stress, both genotypic and phenotypic differences have been described between the ethnic groups, especially through the interactions between the RAAS and sodium handling. While race, a key component of ethnicity, is not herein considered an intermediate phenotype, the data obtained in this study show significant differences in RAAS biomarkers among normotensive male and females within the relatively pure genetic background of a population of African descent. Since the ethnicity of the whole study sample was Afro-Caribbean, any considerations of ethnicity related differences in either gender are nullified. For both males and females, the BMI was in the normal range, and there were no differences in either age or BMI between genders.
Normotension was assessed in this study by monitoring 24 h ambulatory systolic BP and the nocturnal dipping phenomenon associated with reduced pressures during rest periods. Although males and females had similar office systolic BPs, males tended to express higher ABPM systolic BP and less systolic BP dipping during periods of rest. The measured BP variables, whether in terms of office BP or ABPM, reinforced the conclusion that the study population was normotensive. There were no significant differences in BP between genders despite the fact that females tended to have a higher waist circumference when compared with males. The Afro-Caribbean sample characterized in this study had relatively low PRA values compared with previously reported data. 5 These data suggest that they may be tending towards a fluid-overloaded salt-sensitive state.19,20 This interpretation is also strengthened by the finding of a tendency for a reduced systolic BP dip in both males and females, since others have shown that non-dipping is associated with a fluid-overloaded state evidenced by the fact that it can be reversed with a salt-restrictive diet or diuretics. 21
After compensating for intrinsic variability by sorting the data by PRA, at increments of 0.1 ng/ml/h, likely inferences were drawn. In agreement with past studies, we now show in Afro-Caribbean subjects that urinary Ang-(1-7) levels were almost twice as high as the urinary Ang II levels. 17 Females had significantly higher levels of urinary Ang-(1-7) than males. Interestingly, females showed an unusual significant association between clinical systolic and diastolic BP with urinary Ang-(1-7). Since the kidney is the major source for the Ang-(1-7) found in urine, the correlation between BP and urinary Ang-(1-7) content strengthens the previous suggestion that the level of the heptapeptide in the urine is a marker of hypertension.17,22-26 This interpretation is based on studies where urinary Ang-(1-7) concentrations were significantly reduced in untreated essential hypertensive subjects. 17 Although we did not investigate the mechanism associated with the higher urinary Ang-(1-7) expression in females, this finding may reflect a gender difference in the contribution of the enzymatic mechanisms accounting for the formation of the peptide in the kidney. This interpretation is supported by experimental studies showing that estrogen up-regulates the expression of renal ACE2 while reducing plasma ACE activity, in part through a direct effect on the expression of ACE mRNA.26,27 The absence of a gender difference in urinary Ang II content is further evidence that processing of both peptides by the kidney is differentially regulated. This finding may be due to increased neprilysin activity, more so in the females, as the likely source of higher urinary Ang-(1-7) from Ang I catabolism along with renal ACE catabolism reaction of Ang II. 28 Urinary Ang-(1-7) correlated with urinary Ang II levels in females, thus emphasizing linearity in the regulation, production and catabolism of the peptide by the respective catalytic enzymes in the females more so than males. 28 The significant correlation between waist circumference and urinary Ang II in females further justified the associated increase in cardiovascular risk of both parameters.
Contrasting with the findings in urine, plasma Ang-(1-7) levels were equivalent in males and females. However, plasma Ang-(1-7) correlated with waist circumference, ambulatory diastolic BP, and nocturnal systolic BP dipping in females and a significant correlation with ambulatory systolic BP was observed in both genders. While the correlations with the BP readings were unexpected, the correlation with the nocturnal BP dipping observed in the females was consistent with a protective effect of Ang-(1-7). A noteworthy observation was that plasma Ang II levels were significantly correlated with plasma Ang-(1-7) levels in the whole group, thus emphasizing linearity in the regulation, production and catabolism of these peptides by their respective catalytic enzymes. 28 Also, the plasma Ang-(1-7)/Ang II ratio was comparable in both males and females. The congruence of these findings of the RAAS biomarkers in plasma confirms the identification of outliers of the RAAS variables from the data in comparison with previously reported data, and validates the inferences from the analytical approaches applied to the data. 17 Noticeable large standard deviations in the concentration of these parameters would therefore be due to the intra-assay coefficient of variation for Ang II and Ang-(1-7). In the females, PRA correlated with BMI, waist circumference, office diastolic BPs, plasma Ang II and urinary Ang-(1-7). The significant correlations found in females between PRA and biomarkers of hypertension traits suggest a more sensitive estrogen-dependent regulation of arterial pressure. Indeed, the inverse correlation in females between PRA and urinary Ang-(1-7) is in keeping with the concept that the ACE2/Ang-(1-7)/Mas receptor axis confers a protective effect in the regulation of BP. The demonstration that these correlations are absent in normotensive males suggests a relative suppression of the functional mechanisms tilting the vasodepressor pathway towards a vasopressor mechanism.
As it relates to the other urinary parameters, the apparent inverse correlation between urinary potassium and systolic BP dip in the males is consistent with the literature, as lower plasma potassium levels would cause higher and more sustained BPs and hence lower BP dip percentages. 29 This inference is also supportive of the significant correlations of urinary potassium with clinical and ambulatory systolic BPs in the female participants. Urinary sodium significantly correlated with waist circumference and plasma Ang II. These findings are consistent with expected findings in risk profiling and sodium homeostasis. Differences in the urinary creatinine levels and associations with the respective urinary RAAS peptides are mainly due to the apparent difference in muscle mass between genders.
The protective role of estrogen is mainstream in distinguishing the biological differences between genders. Its role in cardiovascular health is well established in its ability to down-regulate ACE and AT1 receptor as well as increase the expression of ACE2 and the AT2 receptor, which may further attenuate the actions of the Ang II/AT1 receptor axis and enhance the actions of the counterprotective Ang-(1-7)/Mas receptor axis. 15 The mean age of the participants, especially the females, would suggest the likely contribution of this protective effect in female participants. Estrogen depletion, similarly to what would be observed during and after menopause, has been shown to increase ACE activity, thus increasing Ang II levels. 20 More so, epidemiological studies and clinical trials have denoted sex differences in the therapeutic benefits attributed to RAAS inhibition via ACE inhibitor or an ARB. 13
The data generated from this study indicate significant gender differences in the profile of RAAS biomarkers in normotensive Afro-Caribbean participants. The observation that plasma angiotensin levels are similar in males and females contrasts with a previous study in which plasma Ang-(1-7) concentrations were found to be higher in young normotensive white male compared with females. 15 Whether this difference is related to genetics or environmental factors remains to be established. Nevertheless, the study described here provides the first characterization of hemodynamic and hormonal characteristics of normotensive male and female subjects of Afro-Caribbean descent.
It may be argued that inter-individual differences in the plasma and urinary angiotensin peptide values among the participants may be a limitation of the study. This is unlikely, as variability of hormone measurements is a consistent finding of studies in human subjects. We acknowledge the theoretical possibility that the infrequency of significant correlations in the males from the multivariate analysis may indicate that the study may have been underpowered to identify the associations. Nevertheless, this study was exploratory and a first in a genetically native sample of persons of African descent. The role of ethnicity and how it affects the role of RAAS peptides in the modulation of CVD seems a likely area for future investigations in the development of ethnicity and gender-related treatment of CVDs. It may also assist in the understanding of the pitfalls of the beneficial effects of hormone replacement therapies and RAAS-blocking therapies in this ethnicity.
Conclusions
The study provides the first characterization of hemodynamics and angiotensins of normotensive male and female subjects of Afro-Caribbean descent. It also indicates significant gender differences in the profile of RAAS biomarkers in normotensive Afro-Caribbean participants. The findings show that a shift in the balance between Ang II and Ang-(1-7) and their respective axes might be markers of the cardio-renal protective mechanisms that may be present in females of Afro-Caribbean descent. Further studies are required to determine the role of ethnicity and how it affects the role of RAAS peptides in the modulation of CVD, and also for the development of ethnicity and gender-related treatment of CVDs.
Footnotes
Acknowledgements
We thank Dr. K.B. Brosnihan, Director of the Peptide Core at the Hypertension and Vascular Research Center for her valuable assistance in the processing of the samples. We are also appreciative of the funding support provided by the Venture Fund, The Wake Forest University Health Sciences Office of Research and Campus Research Awards Committee, The University of the West Indies, Cave Hill Campus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the University of West Indies (D Cohall, 2009 & 2010); a Venture Fund grant by the Wake Forest University School of Medicine (CM Ferrario, 2011); and PO1 grant from the NHLBI of the NIH [grant number - HL-051952].
Supplementary research material
Supplementary research materials for this article can be retrieved by contacting the corresponding author, Damian Cohall.