
Abstract
Introduction:
Clinical studies demonstrated the benefits of eplerenone (EPL) in reduction of cardiovascular events in diabetic patients. Since acute myocardial infarction (AMI) and stroke are related to acute intravascular thrombosis, we postulate that the beneficial effects of EPL may result from its antithrombotic action.
Materials and methods:
Streptozotocin (STZ)-induced diabetic rats were treated with EPL (100 mg/kg/day) for 10 days. Thrombosis in the carotid artery was stimulated electrically.
Results:
Thrombosis development was enhanced in STZ-induced diabetic rats as compared to normoglycaemic controls. EPL caused prolongation of the time to artery occlusion, reduction in the incidence of occlusion and decrease in thrombus weight. Changes in the thrombi structure and the inhibition of hypertrophy of the tunica media in the artery wall were also observed. EPL caused reduction in tissue factor, plasminogen activator inhibitor type 1 and interleukin-1β plasma levels.
Conclusions:
Our study demonstrated the antithrombotic effect of EPL manifested by a decrease in the dynamics of thrombus formation and changes in its structure. The changes in thrombosis process were accompanied by antihaemostatic, profibrinolytic and anti-inflammatory effects. The aldosterone blockade with EPL seems to be an additional pharmacological strategy for the prevention and treatment of thrombotic disorders in diabetes.
Introduction
There is considerable evidence that aldosterone (ALDO) contributes to the development of cardiovascular disease (CVD) and renal diseases in diabetes. 1 It was revealed that diabetic patients with a small increase in plasma ALDO within the norm showed a 10% increase in CVD mortality in relation to diabetic patients with low-normal ALDO levels. 2 Additionally, it is suggested that ALDO and glucose high levels may modulate in return and potentiate their harmful effects in the cardiovascular system. 3 Some in vitro and clinical studies have provided evidence for a link between ALDO and haemostatic disturbances.1,4 We also showed that ALDO infusion enhanced experimental venous thrombosis in normoglycaemic rats and the mechanisms involved endothelial dysfunction, activation of coagulation and fibrinolysis impairment.5,6
An EPHESUS trial has shown strong effectiveness of selective mineralocorticoid receptor (MR) antagonist eplerenone (EPL) in the reduction of mortality in patients with heart failure. 7 The reduction in cardiovascular mortality was paralleled by the reduction in the risk of sudden death, acute myocardial infarction (AMI) and stroke. Moreover post-hoc analysis of the EPHESUS trial demonstrated a greater total risk reduction in diabetic patients compared with non-diabetics treated with EPL. 8
Taking into account both clinical and experimental data it has become obvious that the clinical benefit of EPL may be far greater than can be explained by its hypotensive action. Since AMI and stroke are related to acute intravascular thrombosis, we postulate that the effectiveness of EPL may result from its antithrombotic action. Hitherto, there are very few studies indicating that EPL influences haemostasis. Schafer et al. demonstrated that EPL improves endothelial function and reduces platelet activation in diabetic rats. 9 We have recently discovered the antithrombotic action of acute EPL administration in the stasis-induced model of venous thrombosis in normotensive rats. 6 However, there is still no data concerning the direct effect of EPL on arterial thrombosis in vivo. Therefore, in the present study we investigate the effect of EPL on the arterial thrombosis process and haemostatic parameters in streptozotocin-induced diabetic rats.
Materials and methods
Animals
Male Wistar rats weighing 250–350 g were used in this study. The animals were housed in a room with a 12 h light/dark cycle, and were given tap water and fed a standard rat chow. For 24 h before the experiment, the animals fasted but were allowed free access to water. The procedures involving the animals and their care were conducted in conformity with the institutional guidelines that are in compliance with national and international laws and Guidelines for the Use of Animals in Biomedical Research. 10
Chemicals
The following reagents were used in the study: EPL (Inspra, Pfizer, Poland), pentobarbitone sodium (Vetbutal, Biowet, Poland), heparin (Heparinum, Polfa, Poland), STZ (Sigma-Aldrich, Poland), buffered formalin, citric acid, eosin, gummi arabici, haematoxylin, natrium chloride, sodium citrate and trisodium citrate were provided by Polish Chemical Reagents (Poland).
Induction of diabetes
Diabetes was induced with a single injection of streptozotocin (STZ). STZ was freshly dissolved in sterile sodium citrate buffer (25 mmol/l, pH 4.5) and used within 5 min. The rats received a single 65 mg/kg intraperitoneal injection of STZ or citrate buffer in an equal volume of buffer per kg body weight (normoglycaemic; NORM). Diabetes developed over five weeks. Blood glucose was monitored using a one-touch blood glucose meter (CardioChek, Poland). Hyperglycaemia was defined as a random blood tail glucose level which exceeded > 200 mg/dl on the 3rd day, as well as the 5th week after STZ injection (on the day of experiment).
Drug administration
STZ-induced diabetic rats were randomised to eplerenone (EPL, 100 mg/kg per day, by gavage) or vehicle (VEH, 5% gummi arabici aq. sol.). EPL or VEH were administered for 10 days. Arterial thrombosis was induced on the 11th day.
Arterial thrombosis model
The rats were anaesthetised by an intraperitoneal injection of pentobarbitone sodium (45 mg/kg) and then fixed in the supine position on an operating table. Thrombosis was induced secondarily to electrical stimulation and injury of the endothelium with the current as previously described 11 in our modification. 12 Briefly, the left common carotid artery was separated from the surrounding tissue along a length of at least 20 mm. A stainless, hook shaped, steel electrode was inserted under the left carotid artery. A tiny piece of parafilm ‘M’ (5 mm × 20 mm) was inserted under the electrode for electrical isolation and the hook of electrode was in contact with the artery. The second electrode was inserted subcutaneously in the abdominal region. Both electrodes were connected to a circuit with a constant current generator. Thrombosis was induced by electrical stimulation (1 mA/10 min) of the left common carotid artery. A Doppler flow probe (1 mm diameter, Transonic Systems Inc., Ithaca, USA) was placed in contact with the exposed artery downstream of the electrode and connected to a blood flowmeter (HSE-TRANSONIC Transit Time Flowmeter, Germany). Blood flow was monitored continuously during the entire study. Total carotid blood flow over 55 min was calculated by the trapezoidal rule that measures the area under the carotid blood flow-time curve. The total blood flow was determined as an area under the curve (AUC) and normalised as percentage of baseline (0 min) flow over 55 min to provide a measure of integrated blood flow during thrombus formation. 13 Time to occlusion was defined as the time from application of the current (electrical stimulation) until the blood flow decreased to zero. If the vessel did not occlude by 55 min, the time to occlusion was assigned a 55 min value for data analysis. At the end of the experiment, a segment of the common carotid artery with the thrombus was clipped at both sides, dissected, opened lengthwise, and the thrombus was completely removed, air-dried in room temperature and weighed after 24 h.
Histological evaluation of the thrombus and the carotid artery
Occluded fragments (10 mm) of the carotid artery were collected from some of the NORM and STZ-induced diabetic rats (treated either with VEH or EPL). They were fixed in 4% buffered formalin for 24 h and processed routinely for embedding in paraffin. Thick sections (4 μm) were cut and stained by haematoxylin and eosin (H+E) for general histological evaluation and by May-Grünwald solution at 35°C for 20 min, then stained in diluted Giemza solution in 35°C for 40 min. Histological evaluation was performed by an experienced histologist in a blinded fashion. The obtained results of staining were submitted for evaluation in an Olympus BX50 microscope.
Haemodynamic parameters
The haemodynamic parameters were measured continuously throughout the study by an invasive method. The right carotid artery was isolated, a flow probe was gently placed and the carotid blood flow was continuously measured using the Ultrasonic Doppler Flowmeter (Transonic Systems Inc., Ithaca, USA). The systolic and diastolic blood pressures (SBP and DBP) were measured from the left carotid artery via a transducer (Hugo Sachs Elektronik – Harvard Apparatus GmbH, Germany). The heart rate (HR) was measured with electrodes for electrocardiography (ECG electrodes).
Haemostatic parameters and blood morphology
Blood samples had been drawn from the right ventricle of the heart before an arterial thrombus was removed. The blood was mixed with 3.13% sodium citrate in a volume ratio 9:1 and centrifuged for 20 min at 3500×g at 4°C. Tissue factor (TF), tissue plasminogen activator (t-PA) and plasminogen activator inhibitor type 1 (PAI-1) plasma levels were measured by enzyme immunoassays (Rabbit Monoclonal Antibody Anty Rat TF, ImmunoKontact AMS Biotechnology, Germany; Rat Active t-PA ELISA Kit and Rat Active PAI-1 ELISA Kit, Innovative Research, USA) in a microtitre plate using a Titertek Twin-Reader (Flow Laboratories, UK) according to the manufacturer’s directions. A blood morphology test was performed using haematological analyser ScilVet ABC Plus+ (HORIBA ABX, France). The counting of blood cells was based on the volumetric impedance method. Direct measurement of white blood cells (WBCs), red blood cells (RBCs), haemoglobin (HGB), platelet count (PLT) as well as automatic calculation of haematocrit (HCT) were performed.
Interleukin level
Interleukin-1β (IL-1β) and interleukin-10 (IL-10) plasma levels were determined by enzyme immunoassays using commercially available ELISA kits (Quantikine Rat IL-1 or Quantikine Rat IL-10; R&D Systems, Minneapolis, USA) according to manufacturer’s directions.
ALDO level
The ALDO serum level was determined by radioimmunoassay (Aldosterone CoatA-Count RIA Kit; DPC, Poland) according to manufacturer’s directions.
Statistical analysis
The data are expressed as mean±standard error of the mean (SEM) and percentage. The results and the incidence of occlusion were compared between the groups by means of the Mann-Whitney U test and the Fisher’s exact test, respectively. Values of p<0.05 were considered statistically significant.
Results
General parameters in control and diabetic rats
STZ-induced diabetes (STZ+VEH) caused elevation in blood glucose level (p<0.001) and reduction in body weight (p<0.001) as compared to non-diabetes rats (NORM). EPL significantly increased plasma ALDO level (p<0.001) in diabetic rats. The initial values of SBP and DBP were similar in all groups and they were not altered at the end of the study. EPL did not change SBP and DBP throughout the experiment. The initial and final values of HR were comparable in all groups. There were no differences in the survival rate between NORM, STZ+VEH and STZ+EPL groups (Table 1).
General parameters in normoglycaemic (NORM) and streptozotocin (STZ)-induced diabetic rats treated with placebo (VEH) or eplerenone (EPL); ap<0.001 vs NORM, bp<0.01 vs STZ+VEH.
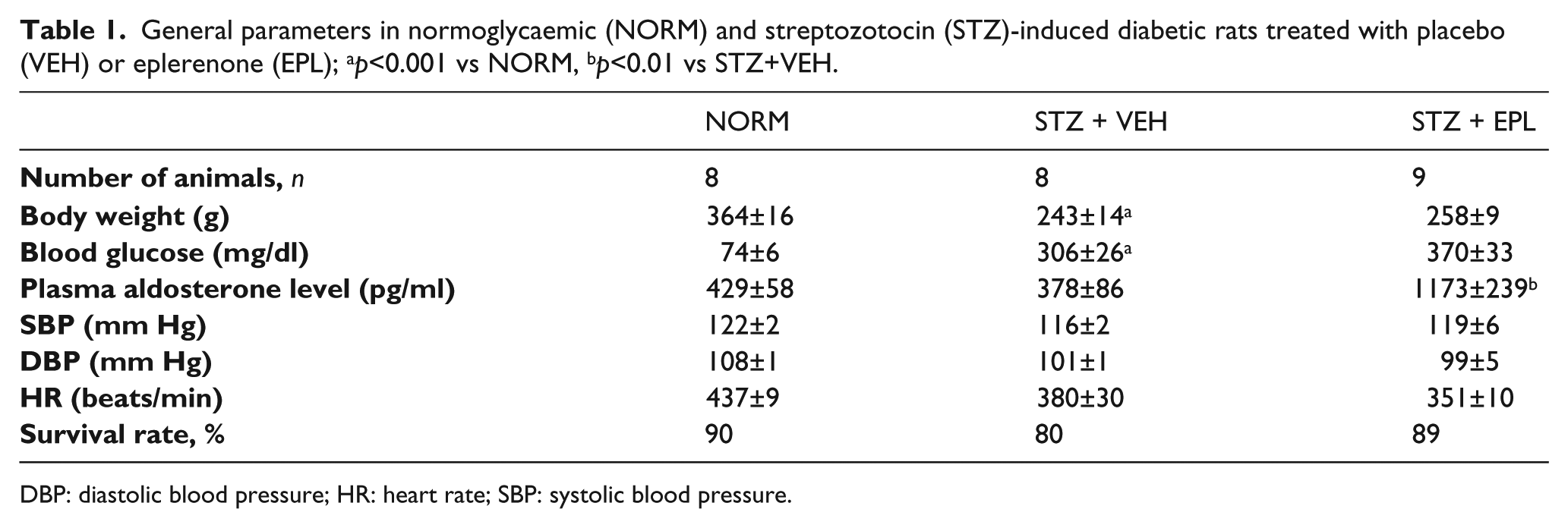
DBP: diastolic blood pressure; HR: heart rate; SBP: systolic blood pressure.
The patency status of the carotid artery
In all experiments the blood flow was measured downstream from the site of electrical stimulation and monitored continuously from the beginning of the study until its end. The initial blood flow (IBF) in the NORM rats was 6.0±0.6 ml/min. In the STZ+VEH group, IBF was reduced by about 40% (to 3.7±0.6 ml/min). EPL treatment did not change the initial carotid blood flow. In the NORM group, the blood flow decreased gradually after electrical stimulation, leading to a stable zero level, indicating occlusive thrombus formation, which occurred in 25% of animals (Figure 1). All STZ+VEH treated rats showed blood flow reduced to a stable zero level, indicating occlusive thrombus formation in 100% of animals (p<0.01) (Figure 1). EPL administration reduced incidences of occlusion by 22% and restored the blood flow as compared to the STZ+VEH group (Figure 1). The average blood flow significantly decreased in the STZ+VEH group compared with the NORM group (17.3±10.3% vs 50.4±5.2% of control; p<0.05). EPL administration significantly improved the average blood flow (35.4±9.4% of control; p<0.05), (Figure 2(a)). The total time to occlusion (TTO) in the NORM group was approximately 48 min (Figure 2(c)). All STZ+VEH treated rats showed shortened TTO in comparison to NORM group (15.0±1.0 vs 47.4±5.1; p< 0.001) (Figure 2(c)). EPL caused evident, but not significant prolongation of TTO as compared to the STZ+VEH group (Figure 2(c)).

Changes in the carotid blood flow determined in normoglycaemic (NORM), streptozotocin (STZ)-induced diabetes (STZ+vehicle (VEH)), and STZ+ eplerenone (EPL) rats subjected to electrical stimulation of the carotid artery. Significant differences relative to the NORM group were detected using Mann Whitney’s test and the Fisher exact test for vessel patency. Data are mean±standard error of the mean (SEM). *p<0.05; **p<0.01 compared with the NORM group (Mann Whitney test); ♦♦p<0.01 compared with the NORM group (Fisher test).
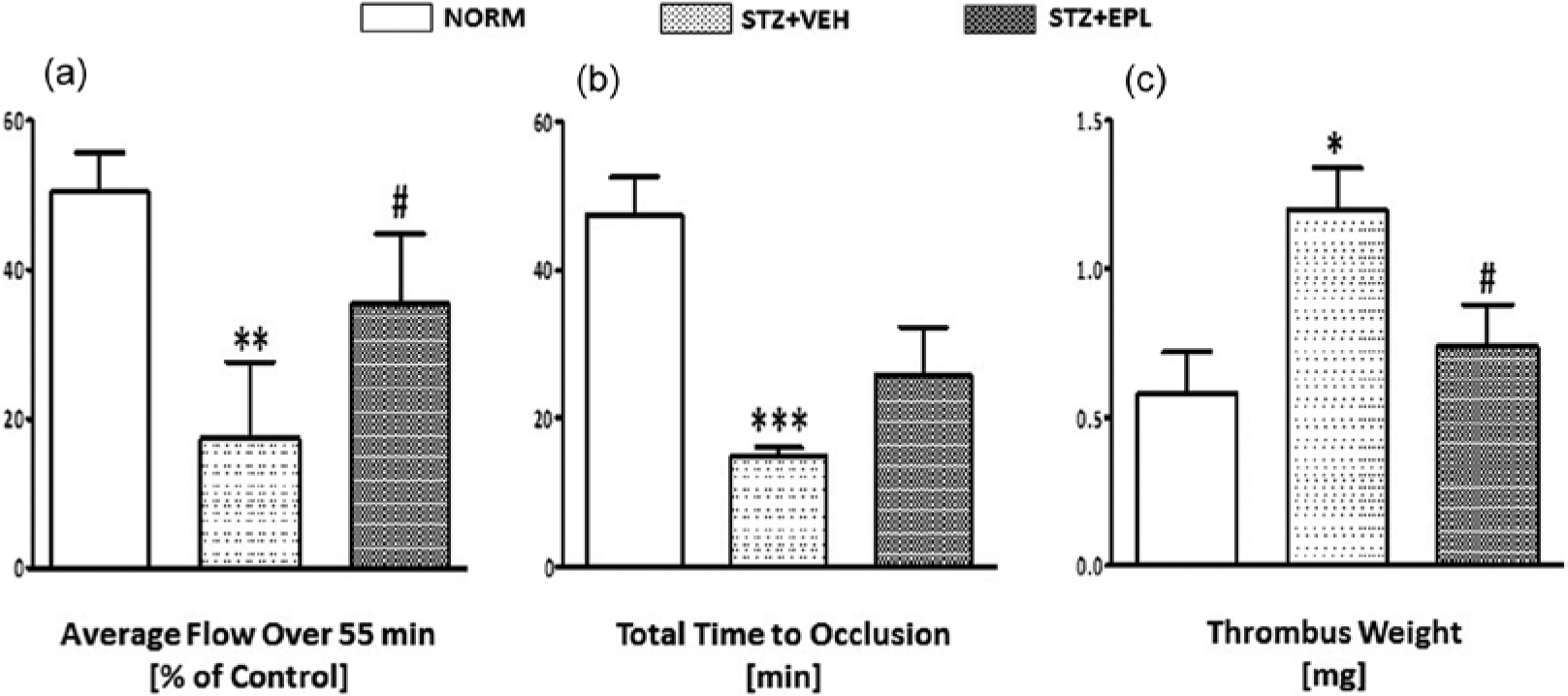
Effect of eplerenone (EPL) on (a) the integrated average blood flow (area under flow curve), (b) thrombus weight and (c) total time to occlusion in normoglycaemic (NORM) and streptozotocin (STZ)-induced diabetic rats. Data are mean±standard error of the mean (SEM). **p<0.01, ***p<0.001 compared with NORM, *p<0.05 compared with NORM group, #p<0.05 compared with STZ+vehicle (VEH) group.
Thrombus weight
As shown in Figure 2(b), a significant (p<0.05) rise in the arterial thrombus weight was observed in the STZ+VEH group (1.22±0.15 mg) compared to the NORM group (0.58±0.14 mg). The administration of eplerenone caused significant (0.74±0.14 mg; p<0.05) reduction in the arterial thrombus weight.
Thrombus morphology and wall of the carotid artery structure
Distinct differences between the study groups were observed in microscopic examination of thrombus and the carotid artery wall. Clots of the NORM group of rats were mainly composed of erythrocytes and platelets. There were no changes in the blood vessel wall (Figure 3(a)). A microscopic picture of thrombus in the diabetic STZ+VEH rats was different from the NORM group of animals: quite orderly arrangement of fibrous structures with densely packed platelets and numerous leukocytes was observed. There was also a distinct change in the artery wall. The thickness of the blood vessel wall was increased compared to the NORM rats. Moreover, the observed swelling of the muscle cells with light, not stained areas in the cytoplasm of these cells (Figure 3(b)). After eplerenone treatment (STZ+EPL), the structure of the thrombus was not so ordered, with loosely packed fibrin fibres. The number of leukocytes also diminished. The thickness of the carotid artery wall was reduced as compared to STZ+VEH rats. The observed swelling of the muscle cells and the light, not stained, areas were also reduced (Figure 3(c)).
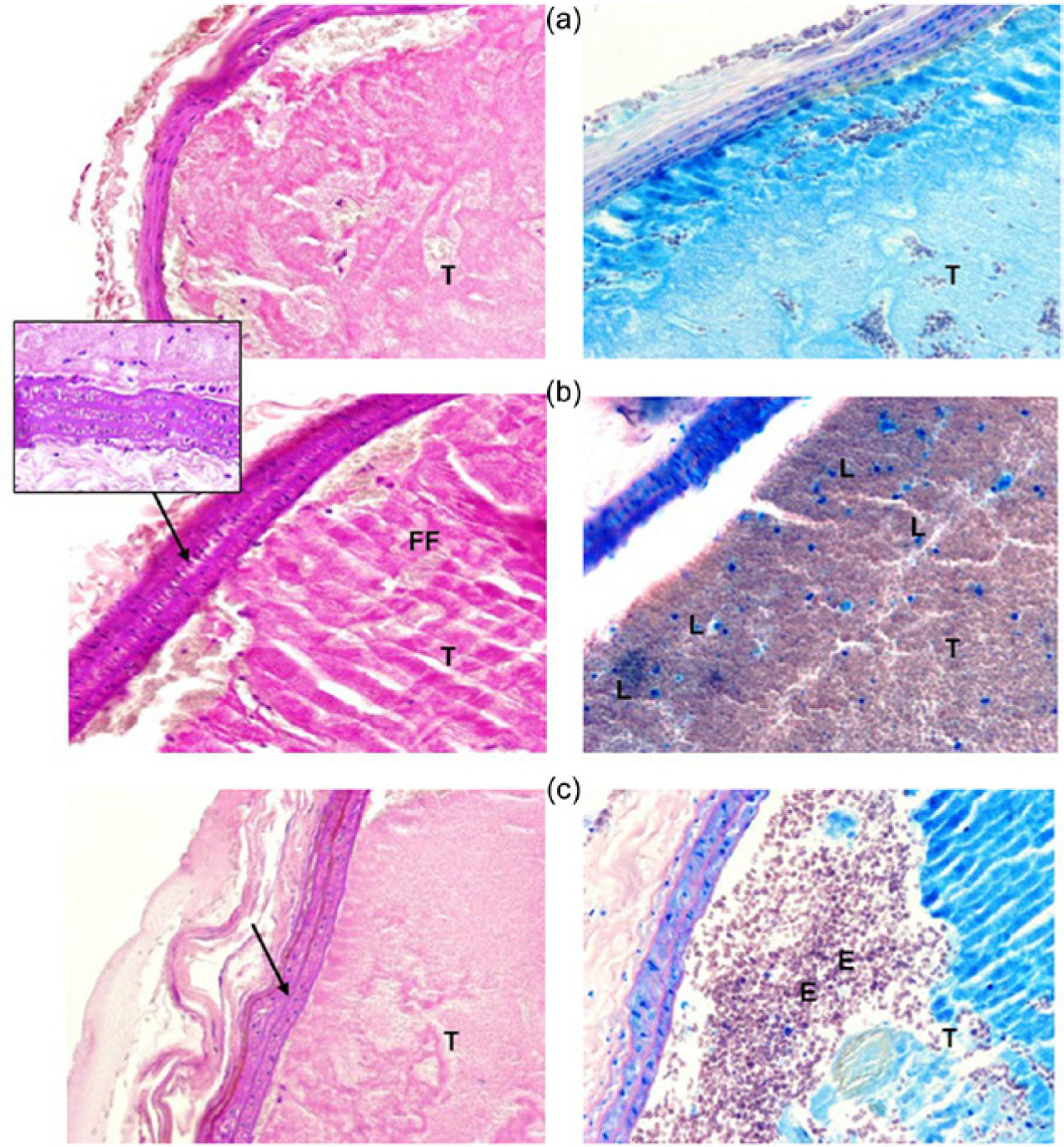
Photomicrographs of the thrombi and carotid artery wall in (a) normoglycaemic (NORM), (b) streptozotocin(STZ)-induced diabetic +vehicle (VEH) and (c) STZ+eplerenone (EPL) groups. Images on the left side were stained with haematoxylin and eosin (H+E), ×200; images on the right side were stained by May-Grünwald-Giemza, ×200. Arrows indicate tunica media in the artery wall. E: erythrocyte; FF: fibrin fibre; L: leukocyte; T: thrombus.
Haemostatic parameters and blood morphology
STZ+VEH rats showed a significant rise in the TF and t-PA plasma levels (p<0.05; p<0.01 vs NORM respectively) which were markedly reduced after EPL administration (p<0.001; p<0.01 vs STZ+VEH respectively). A significant increase in PAI-1 plasma level of STZ+VEH rats (p<0.001 vs NORM) was also observed. This effect was diminished in STZ+EPL group (p<0.001 vs STZ+VEH) (Table 2). A significant increase in haematocrit level and a decrease in platelet count of diabetic rats (p<0.05 vs NORM) were observed. Administration of EPL did not change the blood morphology (Table 2).
Haemostatic parameters, interleukin levels and blood morphology in normoglycaemic (NORM) and streptozotocin (STZ)-induced diabetic rats treated with placebo (VEH) or eplerenone (EPL), n=8–9; ap<0.05, bp<0.01, cp<0.001 vs NORM and STZ+VEH respectively.

HCT: haematocrit ; HGB: haemoglobin ; IL-1β: interleukin-1β; IL-10: interleukin-10; PAI-1: plasminogen activator inhibitor type 1; PLT: platelet count; RBC: red blood cell; TF: tissue factor; t-PA: tissue plasminogen activator; WBC: white blood cell.
Interleukin levels
In the STZ+VEH group, the level of IL-1β and IL-10 significantly increased compared to NORM (p<0.05; p<0.05 respectively) (Table 2). Eplerenone caused a significant decrease in the IL-1β level compared to the STZ+VEH group (p<0.05).
Discussion
In the present work we have demonstrated that EPL effectively reduced arterial thrombosis caused after electrolytic injury of the carotid artery in STZ-induced diabetic rats. We have also shown the changes in the thrombus structure and diminished vessel wall hypertrophy after EPL. The modification in thrombosis process was associated with reduced plasma levels of tissue factor, PAI-1 and IL-1β. Although, we did not investigate the mechanism involved, our data shows for the first time that EPL reduced arterial thrombosis process in STZ-induced diabetic rats, and that this effect seems to be independent of blood pressure and hypoglycaemia reduction.
Diabetes is associated with a hypercoagulable state that contributes to thrombotic disorders.14,15 Thus, the ability of EPL to decrease arterial thrombosis was studied in a widely used model of STZ-induced diabetes in rats. STZ injection selectively destroys insulin-producing cells in the pancreas leading to the typical complications of diabetes. 16 We have established that STZ-induced diabetes in rats contributes to haemostatic imbalance which leads to a hypercoagulable state rendering the carotid artery more susceptible to thrombosis. We have also observed a shortened time to artery occlusion, an increase in the incidence of the occlusion in the carotid artery and a significant rise in the arterial thrombus weight in STZ-induced diabetic rats in comparison to the NORM rats using an electrolytic injury model of the carotid artery. Similarly, the enhancement of thrombogenesis in the polyethylene tube-induced thrombosis in the carotid artery in STZ-induced diabetic rats was observed, though plasma haemostatic parameters were not measured. 17 We assume, therefore, that the increase in arterial thrombi formation in STZ-induced diabetic rats may be caused by the alterations in haemostatic parameters, inflammatory factors and disturbances in the blood flow. Since this had not been previously studied, we attempted to characterise the changes in the plasma haemostatic parameters as well as the thrombus and vessel wall structures in the arterial thrombosis model in STZ-induced diabetic rats.
We have also observed an increase in the plasma TF activity. It is necessary to mention that TF is recognised as an essential initiator of thrombin generation and coagulation which may be involved in thrombus propagation at the site of vascular injury.18,19 The mechanism of TF increase in diabetes may be related to the formation of advanced glycation end products and reactive oxygen species, which activate NFκB leading to TF production. 20
Hyperglycaemia impairs fibrinolytic activity on the surface of endothelial cells and decreases plasma fibrinolytic potential.21,22 Consequently, the acceleration of arterial thrombus growth may be also caused by fibrinolysis inhibition. The fibrinolytic system is controlled by a critical balance between plasminogen activators and plasminogen activator inhibitors. The actions of t-PA are inhibited predominantly through local release of PAI-1 from activated platelets in the growing thrombus. Few studies have demonstrated markedly increased mRNA and protein expression of PAI-1 in STZ-induced diabetic rats.23,24 Additionally to what had been previously found, we have observed a slight but significant increase in the PAI-1 plasma level.
It is known that diabetes is the state which is associated with an increased level of pro-inflammatory cytokines which may essentially influence the prothrombotic potential by their adverse effect on coagulation, fibrinolysis and the endothelium. 19 It could also be the case in our model, since a marked increased level of IL-1β in STZ-induced diabetic rats was observed.
Quantitative changes in coagulation factors can affect the final organisation of the thrombus. We observed that the arterial thrombus in STZ-induced diabetic rats showed an inflammatory nature expressed as an orderly arranged fibrous structure with densely packed platelets and numerous leukocytes. It could be that a high TF level is associated with a more compact clot structure due to intensive local thrombin dependent fibrin production. Cellular composition of the thrombus may also reflect an inflammatory state secondary to hyperglycaemia while elevated PAI-1 may impair the lysis of fibrin fibres. Similarly, clots formed in diabetes patients had a more compact structure characterised by smaller pore size, increased fibre thickness and a number of branch points compared with normoglycaemic controls.25,26 It is worth mentioning that high glucose has been shown to increase glycation of fibrinogen 27 and clots formed from glycated fibrinogen despite a more compact structure being resistant to lysis.
One of the most important modulators of thrombus formation and propagation in diabetes is vascular dysfunction that disturbs the blood flow. It was shown that the combination of increased vascular thrombogenicity and a reduction in the blood flow of >75% promoted occlusive thrombosis in rabbit femoral arteries. 28 Also in our model, alterations in the systemic blood flow occurred, expressed as a significant reduction (>40%) of the initial carotid blood flow. As it had been previously shown, the carotid blood flow reduction depends on limited nitric oxide bioavailability and up-regulation of ET-1 biosynthesis in the vessel wall in STZ-induced diabetic rats.9,29
We also found vascular hypertrophy of the carotid artery in STZ-induced diabetic rats. Subcellular alterations in smooth muscle cells manifested by increased volume and enhancement in non-stained areas in the cytoplasm were noticed. Correspondingly, an increase in the endothelial and adventitial cell proliferation and an increase in the total collagen content within the media were observed in the mesenteric vessel of diabetic rats. 30 These alternations could be associated with the increased vessel wall endothelin (ET) level and with overexpression of transforming growth factor-β (TGF-β), epidermal growth factor (EGF) and an increased level of pro-inflammatory cytokines in STZ-induced diabetic rats.31,32
In our study, the platelet count was also significantly diminished in STZ-induced diabetic rats. In diabetes, the low number of platelets could be connected with shortened survival time and increased platelet turnover, resulting from the impairment of platelet membrane permeability, due to glycation of proteins and lipid disorders. 33
Summing up, in this part of the study, we showed for the first time in the electrolytic injury model of carotid artery thrombosis that STZ-induced diabetes leads to enhancement of thrombus formation with the mechanisms involving TF activation, PAI-1 inhibition and inflammation.
An important finding of the current research is that EPL effectively reduces arterial thrombosis caused by electrolytic injury of the carotid artery in STZ-induced diabetic rats. This model of vascular injury produces significant endothelial damage leading to exposure of subendothelial matrix that induces highly reproducible arterial thrombi. Although thrombus formation was initiated by a stimulus that is unrelated to clinical thrombosis, the thrombus structure (rich in platelets and fibrin, with piles of red cells trapped in the fibrin network) proves that growth of thrombotic material is clinically relevant. 11 Importantly, this model allows for the possibility to continuously monitor the dynamics of thrombus formation and its lysis. 34 Using this model, we and others have demonstrated the antithrombotic/prothrombotic activity of many compounds and biological substances.11–13,35–39
EPL effectively prevented or delayed the time to artery occlusion, promoted sustained vessel patency and reduced thrombus weight in diabetic animals. To explain the low rate of arterial thrombus formation we assumed that the drug action on coagulation and fibrinolysis may be responsible. The time to occlusion reflecting the amount of time it takes for a thrombus to completely block the blood flow also reflects the amount of thrombin generation (or inhibition of generation) taking place while the drug is acting on the thrombus. 40 We found a marked reduction in TF plasma level in STZ+EPL rats. So far the increased TF activity in diabetes has been well documented, although the mechanism of this has remained unknown. We had previously shown, that acute ALDO infusion increased TF plasma level five-fold in normotensive rats. 5 It could be postulated that EPL-decreased TF level in STZ-induced diabetic rats is related to tumor necrosis factor (TNF)-α downregulation. Satoh et al. (2006) demonstrated that EPL downregulated TNF-α converting enzyme and TNF-α concentration in cultured monocytes from patients with congestive heart failure. 41 Since TNF-α is known for inducing the expression of TF in cardiovascular cells, decreased TNF-α may lead to reduced expression of TF. 42 Thus, the present data indicate that inhibition by EPL of the TF/thrombin dependent pathway could have a particular importance in the mechanism of the antithrombotic action of the drug. Moreover, thrombin plays a key role also in platelet activation and fibrinolytic potential regulation.
The results of our study indicate that the antithrombotic effect of EPL in diabetes involves fibrinolysis activation. We observed a slight but significant reduction in PAI-1 plasma level in EPL-treated diabetic animals which is likely to promote endogenous thrombolysis and inhibition of thrombus extension. 43 Furthermore, we observed an increasing tendency in elevating the ratio of t-PA/PAI-1 in STZ+EPL rats in comparison to STZ-induced diabetic rats (data not shown). Our results are the first which indicate the increase of plasma fibrinolytic activity after EPL administration in STZ-induced diabetic rats. We had previously shown that ALDO infusion in normoglycaemic rats markedly increased the PAI-1 plasma level and mRNA PAI-1 level in the aorta.5,6 Another study revealed that chronic EPL administration decreased the expression of PAI-1 renal cortical tissue in type 2 diabetes animal models. 44
We found considerable changes in the architecture of the thrombus formed in the carotid artery of STZ+EPL rats. It showed a weakly organised fibrin structure with low amounts of leukocytes. Reduced thrombin generation, secondary to a decrease in TF, may account for the formation of less compact and more lysable fibrin. It was shown that accessibility of the clot to fibrinolytic proteins and alternations in binding of t-PA and plasminogen were both regulated by the fibrin structure. 45 Moreover fibrinolysis proceeds rapidly in platelet-poor areas of the clot, whereas platelets-rich areas remain relatively unlysed. 46 Thus, on the basis of our observations, the reasons for alterations in the thrombus structure and its mass may be a complex process consisting of antithrombin, profibrinolytic and anti-inflammatory action of EPL.
The anti-inflammatory effect of EPL could also contribute to the suppression of the wall hypertrophy in diabetic arteries. Nagata et al. (2006) showed that EPL in a non-antihypertensive dose inhibits coronary vascular inflammation in Dahl salt-sensitive hypertensive rats. 47 In our study, EPL reduced vessel wall hypertrophy, attenuated muscle cell swelling and non-stained areas in these cells. However, we cannot determine whether the suppression of hypertrophy originates via limited cellular hyperplasia or hypertrophy of smooth muscle cells or a decrease in collagen content. The mechanism of the suppression of arterial hypertrophy by EPL needs to be addressed in further studies.
It is worth adding that in vitro and in vivo studies in rodent models indicate an important role of ALDO and MR activation in the induction of inflammation and reactive oxygen species formation leading to endothelial dysfunction, decreased nitric oxide bioavailability, monocyte and macrophage infiltration of the vascular wall and vascular remodelling, factors that contribute to atherosclerosis. 48 There is strong evidence that EPL reduces the effects of ALDO on atherosclerosis in animal models.49,50 Importantly, the association of plasma ALDO with carotid plaque progression in patients with symptomatic vascular disease was recently found. 51 Consequently there are reasonable expectations that MR antagonists should affect plaque volume. Therefore, the antihaemostatic effect of EPL, revealed in our studies and despite its antiatherosclerotic action, may account for preventing atherothrombosis.
With regard to its effect on blood coagulation and thrombosis, hyperglycaemia is known to be associated with enhanced platelet reactivity. Bearing in mind that arterial thrombosis is a process in which platelets play the crucial role we cannot exclude antiplatelet mechanisms in the antithrombotic action of EPL. We had previously observed ex vivo reduction of platelet adhesion to fibrillar collagen in STZ-induced diabetic rats after long-term EPL treatment. 39 In another study, two weeks treatment of STZ-induced diabetic rats by EPL at dose 100 mg/kg attenuated platelet reactivity by a decrease in GPIIb/IIIa activation and surface-expression of P-selectin. 9 In our work, EPL treatment does not influence the blood cell count. In view of the above changes, the reactivity of platelets and other blood cells rather than their quantity should be taken under consideration with regard to EPL’s influence on the process of arterial thrombosis. Moreover, activated platelets also release PAI-1 that contributes to impaired fibrin degradation and the role of PAI-1 in clot lysis depends on the number of the platelets. 52
We did not observed changes in the values of the blood pressure, HR and glucose level in STZ-induced diabetic rats after EPL treatment. Similarly, any modifications in hemodynamic parameters in normotensive rats and diabetic mice53–55 as well as glucose level in STZ-induced diabetic rats 9 were not observed after chronic EPL administration. Thus our results suggest that the ability of EPL to inhibit arterial thrombosis is independent of its hypotensive and hypoglycaemic activities.
Summing up, we demonstrate here for the first time the antithrombotic action of EPL in STZ-induced diabetic rats. EPL diminished the dynamics of arterial thrombus formation with changes in thrombus morphology and in the arterial wall structure. The changes in the arterial thrombosis process were accompanied by antihaemostatic, profibrinolytic and anti-inflammatory effects of the drug. Our results also confirm the role of ALDO in haemostatic disorders in diabetes rats.
Perspectives
This report describes evaluation of EPL in a model with intravascular thrombi where the drug was tested to assess its possible utility for prevention of arterial thrombosis in diabetes. Although the mechanisms of antithrombotic and antihaemostatic actions of EPL have not been explained, our findings of novel pleiotropic activities of EPL may have important therapeutic implications. Moreover, basic and clinical studies have demonstrated that elevated plasma ALDO levels predict the development of insulin resistance and that ALDO directly interferes with insulin signalling in vascular tissues. 56 Thus, prevention or restoration of these changes via a blockade of ALDO action in the vessels may account for the clinical benefit of EPL in diabetic patients with cardiovascular disease. In the light of our data, we can assume that hypoglycaemic therapy regarded as a method limiting vascular diseases 57 may be potentiated by the beneficial antithrombotic effects of EPL.
Footnotes
Conflicts of interest
The authors declare that they have no conflicts of interest.
Funding
This work was supported by the Ministry of Science and Higher Education (grant number NN405 627938); the Polish Cardiac Society (ADAMED grant).